
Abstract
Nonmelanoma skin cancer (NMSC) is the most common malignancy in the world, with over 5.4 million new cases diagnosed in the United States annually. Basal cell carcinoma (BCC) comprises 70–75% of these cases, and up to 85% occur in the head and neck region. Basal cell carcinoma is thus the most common cancer in the world and is reaching epidemic proportions, with an ever-rising incidence. This can be observed most strikingly in Australia, which has the highest prevalence of skin cancer in the world. BCCs less commonly cause death, but if left alone can invade locally and cause significant functional loss and morbidity.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Basal cell carcinoma
- Nevoid basal cell carcinoma syndrome
- Head and neck surgery
- Vismodegib
- Sonidegib
- Staging
- Surgical excision
Introduction and Epidemiology
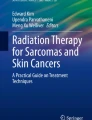
Nonmelanoma skin cancer (NMSC) is the most common malignancy in the world, with over 5.4 million new cases diagnosed in the USA annually [1]. Basal cell carcinoma (BCC) comprises 70–75% of these cases, and up to 85% occur in the head and neck region [2]. Basal cell carcinoma is thus the most common cancer in the world and is reaching epidemic proportions, with an ever-rising incidence. This can be observed most strikingly in Australia, which has the highest prevalence of skin cancer in the world [2]. BCCs less commonly cause death, but if left alone can invade locally and cause significant functional loss and morbidity (Fig. 8.1).

A large invasive, disfiguring basal cell carcinoma, with extension into the nasal cavity, maxillary sinus, and orbit
Given its potential for causing local destruction, treatment of BCC is indicated. To date, there are numerous treatment strategies including electrodesiccation and curettage, surgical excision, Mohs micrographic surgery, topical and intralesional agents, radiation therapy, and photodynamic therapy. BCCs can be categorized by their potential for recurrence based on location, pathologic features, and patient factors. In addition to these factors, resource availability and costs of treatment may best guide the clinician in selecting the most appropriate therapy for reducing the likelihood of local recurrence as well as obtaining the best functional outcome. The focus of our chapter will be on the role of surgery for this disease entity in the head and neck.
In starting to understand the surgical treatment of BCCs of the head and neck, it is incumbent upon clinicians to have a thorough understanding of the predisposing factors of BCC, biology of the disease, and the extent of surgical excision necessary to obtain cure.
Risk Factors and Pathogenesis
Basal cell carcinomas arise from the basal layer of the epidermis. Both environmental and genetic factors have been implicated as risk factors in the development of BCC. Exposure to ultraviolet (UV) radiation in sunlight is the most important, followed by other environmental exposures including arsenic, radiation, immunosuppression, and genetic factors.
Environmental Risk Factors
The significance of sun exposure as a risk factor was initially proposed in the 1920s and has since been confirmed by a myriad studies [3]. Established tenets of risk stratification predict that BCC occurs more frequently in light-skinned sun-sensitive people, those with benign sun-related skin conditions, and occurs mainly on sun-exposed body sites [3, 4]. Multiple epidemiologic observations have shed light onto the association between sun exposure and the development of BCC, including the striking geographic variation (with states closer to the equator having twice the incidence of BCC compared with that of the Midwest United States) [5].
There remains considerable dispute regarding the exact nature of sun exposure that is required to cause pathogenic change. Some authors argue that the cumulative dose of ultraviolet UV radiation is the culprit, whereas Kricker and colleagues posited that frequent, intense periods of sun exposure significantly increase the risk of the development of BCC [6]. Some authors suggest that the intermittent versus continuous nature of sun exposure is irrelevant; rather, that sun exposure during childhood and adolescence predisposes these individuals to NMSC [7].
UV light exposure as a risk factor for BCC has also been described in relation to indoor tanning. A case control study from Yale revealed a 69% increased risk of early-onset BCC associated with tanning beds, especially among women, in a dose-dependent fashion [8]. Certain photosensitizing agents have been shown to increase the risk of NMSC, potentiating the carcinogenic effect of UV light. Robinson and colleagues showed a significantly increased risk of BCC, specifically early-onset BCC, in patients who have ever used photosensitizing antimicrobials such as tetracyclines [9]. The most common indications for tetracycline use in young patients include skin rashes and acne. These findings offer a word of caution to the use of these medications in younger patients. The authors also found a significant association between squamous cell carcinoma and ever use of thiazide diuretics, but this association could not be replicated in BCC [9].
A history of prior NMSC also significantly increases the risk of future BCC. There is a reported 45% 5-year risk of new BCC among patients with previous BCC, as opposed to 5% in the general population [10, 11]. This may be in part due to “field cancerization,” a topic that has rapidly gained interest in head and neck oncology. Kanjilal and colleagues found multiple and distinct p53 mutations via DNA sequence analysis in tumor and adjacent nonmalignant skin samples in a cohort of patients with NMSC of the head and neck, confirming that field cancerization may play a role in the development of BCC [12].
Several other notable risk factors have been linked to the development of BCC. A recent prospective study revealed an almost twofold increase in the incidence of BCC in patients with a history of ionizing radiation compared to control patients [13]. Certain environmental exposures such as arsenic have also been linked to the development of BCC [14].
Immune modulation and suppression have been shown to be potent risk factors, which can be seen most strikingly in transplant patients. NMSC has been shown to develop at an alarming rate in this cohort; the cumulative incidence of NMSC in transplant patients was shown to be as high as 50% [15]. The risk of BCC in particular is increased tenfold in transplant recipients [16]. Figure 8.2 shows a transplant patient with multiple primary BCC of the head and neck, highlighting the scope of the problem in this patient population.

Transplant patient with multifocal basal cell carcinoma of the head and neck. This is a common but difficult problem to manage in this patient cohort
Interestingly, the incidence of NMSC increases in a linear fashion with the duration of immunosuppressive therapy. An Australian study reported an increase in skin cancer incidence from 7% at 1 year of immunosuppressive therapy to 82% at 20 years [17]. However, duration is not the only causative factor: the immunosuppressive regimen implemented also plays a significant role. For example, transplant patients who were placed on cyclosporine, azathioprine, and prednisolone were almost three times more likely to develop skin cancer when compared to patients on azathioprine and prednisolone alone [18]. Cyclosporine is a robust T-cell modulator. Transplant patients treated with cyclosporine have been shown to have significantly lower CD4 counts compared to age-matched controls [19]. Similarly, HIV patients have been shown to have a significantly increased risk of BCC and SCC [20]. The significance of CD4 lymphocytopenia is discussed further below. Table 8.1 summarizes the known risk factors for BCC.
Molecular Pathogenesis
The prevailing molecular theory for BCC involves the hedgehog pathway. It was first described in the context of nevoid basal cell carcinoma syndrome (NBCCS), an autosomal dominant disorder associated with multiple BCC, medulloblastoma, mandibular cysts, developmental disability, prominent forehead with broad nasal bridge, and pits on the soles of hands and feet [21]. The causative genetic alteration has previously been mapped to chromosome 9q22 [22]. Loss of heterozygosity at this locus was later confirmed to be an independent factor, found to be in 68% of BCC [23]. The locus codes for the protein Patched (PTCH), which is inhibited by sonic hedgehog (SHH) [24]. Loss of function PTCH mutations lead to downstream activation of smoothened (smo), B-cell lymphoma (bcl) 2, as well as glioma-associated oncogenes (gli) 1, 2, and 3 which have been found to be overexpressed in BCC mouse models and human cell lines, leading to oncogenesis [25, 26]. This pathway has provided several molecular targets for potential drug applications. Figure 8.3 summarizes the SHH pathway.

A schematic of the hedgehog pathway. Hedgehog pathway inhibitors vismodegib and sonidegib inhibit the smoothened of the hedgehog pathway. SHH, sonic hedgehog; PTCH, patched; SMO, smoothened; GL1, glioma-associated oncogene; BCL-2, B-cell lymphoma 2
The p53 pathway has been extensively studied in cancer biology as a well-known tumor suppressor and more recently in BCC as well. In a study of 11 patients with BCC, DNA sequencing revealed a p53 mutation (or multiple p53 mutations) in every single sample studied [27]. Normal epithelium studied from these patients showed wild-type p53 in all but one sample [27]. Larger studies have revealed ultraviolet light-induced point mutations in p53 in over half of all BCC, suggesting a correlation between the two [23].
Immune dysfunction has been shown to play a role in skin cancer as well, as evidenced by the NMSC epidemic in transplant and HIV patients. Significant dysregulation in the T-cell response has been shown in numerous studies. A 2017 study revealed a significant increase in the proportion of a subset of CD4+ cells, Treg cells, in BCC compared to control [28]. The author suggested that the crosstalk between T reg cells and basal keratinocytes may not only directly lead to carcinoma formation but also creates a microenvironment in which the tumor is allowed to flourish. The precise interplay between these factors has yet to be completely elucidated.
Presentation and Work-Up
BCC usually presents as insidiously growing skin lesion, often with pearly appearance with potential ulceration, bleeding, or telangiectasias. There are various types of BCC such as nodular, cystic, superficial, micronodular, or pigmented [29]. As seen in Table 8.2, nodular, cystic, and superficial are low-risk subtypes, whereas morpheaform, micronodular, and basosquamous are high-risk subtypes [29].
Staging of BCC is performed according to the AJCC eighth edition TNM classification (Table 8.3) [30] and mirrors that used for cutaneous SCC. In stage 1 tumors, the tumor is smaller than 2 cm and does not invade any underlying structures. In stage 2, the tumor is larger than 2 cm and has likely invaded into the dermis, possibly surrounding neural structures. In stage 3 tumors, the cancer has spread to structures below the skin, such as the muscle, bone, cartilages, or lymph nodes. Lastly, in stage 4, the tumor may have spread toward the skull base or toward distant organs such as the lungs or brain [30].
A biopsy is necessary for diagnosis, but wide local excision is often performed for small, suspicious lesions for diagnostic and therapeutic reasons.
For small lesions of the head and neck, imaging is not usually necessary. For extensive BCC of the head and neck, computed tomography (CT) is frequently the imaging modality of choice. CT allows evaluation of the extent of bony erosion (i.e., temporal bone, maxilla, zygoma, orbit, etc.) and also allows reasonable visualization of nodal basins. Figure 8.4 shows a representative example of bony erosion caused by BCC, which is optimally appreciated on CT scan. If clinical suspicion is high, magnetic resonance imaging (MRI) may be used to assess the extent of perineural invasion [29]. Due to the low rate of distant metastasis from BCC, positron emission tomography-CT (PET-CT) is generally not implemented, though may be of use to assess response to systemic therapy in locally advanced or metastatic BCC [29].

Coronal CT depicting bony erosion of the zygoma caused by locally invasive BCC
Treatment
Largely due to the high incidence of BCC, clinicians of various subspecialties are involved in managing BCC. With more advanced BCCs , there is an increased need for a multidisciplinary evaluation. Head and neck surgeons, dermatologists, Mohs surgeons, and sometimes radiation oncologists and medical oncologists are involved in the care of patients with BCC. There are a variety of treatment options for BCC of the head and neck. The primary goal in treatment of BCC is always eradication of the disease. However in the head and neck, respect of anatomy and oncologic control must be balanced with the ablative defect and the form and function of the underlying structures. Locally invasive head and neck BCC can have debilitating effects on form and function, necessitating a thoughtful and thorough approach to treatment. The current standard of care and decision-making with regard to treatment is heavily influenced by the risk stratification put forth by the National Comprehensive Cancer Network (NCCN) [31], as seen in Table 8.2. Determining the character of the BCC as low or high risk for recurrence is critical. The NCCN has identified features of head and neck BCC with lower likelihood for recurrence after treatment including BCC with less than 6 mm in diameter in high-risk areas (H-zone: central face, nose, lips, eyelids, eyebrows, periorbital), less than 10 mm in other areas of the head and neck, a nodular or superficial histopathologic growth pattern, lack of perineural invasion, primary lesion, well-defined clinical borders, lack of prior radiation, and immunocompetent patients [31].
In low-risk head and neck BCC, the treatment modalities of surgical excision, Mohs surgery, cryosurgery, curettage and electrodessication, radiation, and topical or intralesional agents can be utilized with various advantages and disadvantages. For the purposes of this chapter, we will focus on the role of surgery. In the head and neck, surgical excision offers significant advantages: allowing for margin-control, more precise control over tissues removed and preserved, and more deliberate preservation of critical structures. Generally accepted margins for surgical excision are established at 4–6 mm for small tumors, as excisions of lesions 2 cm or less in diameter have previously resulted in negative margins in more than 95% of cases [32–33].
Mohs micrographic surgery has also been shown to be a favorable treatment option in the appropriate tumors. In a randomized control trial of high-risk primary and recurrent facial BCC, 10-year recurrence rates were greater following surgical excision than Mohs micrographic surgery (12.2% vs. 4.4%, respectively), although at the time of the study, recommended margins were limited to 3 mm [34]. Importantly, Mohs micrographic surgery has been shown to create a median defect size 1.6 times smaller than that of surgical excision [35], which is ideal for lesions of the face and neck. Mohs micrographic surgery is relatively more costly a procedure and time intensive and therefore may not be feasible for all patients.
Head and neck BCC with high risk for recurrence after treatment include tumors greater or equal to 6 mm in high-risk areas, greater than 10 mm in diameter in other areas of the head and neck, aggressive histopathological subtypes (sclerosing, micronodular, basosquamous), recurrence, prior radiation, poorly defined borders, immunosuppression, or perineural invasion [31].
Within the head and neck, the basis for high-risk sites (so called H-zone) is defined embryologically. These locations represent embryological cleavage planes that offer little resistance to deeper tumor invasion. BCC arising in the H-zone displays a disproportionately high recurrence rate [36]. Given the density of critical structures and cosmetically sensitive areas within the head and neck, complete tumor removal without cosmetic or functional impairment becomes more difficult. In these settings, Mohs micrographic surgery, surgical excision, and radiation are the most effective treatments.
For locally advanced BCC of the head and neck, careful surgical planning is of utmost importance. Preoperative evaluation and imaging dictates the extent of surgery that is necessary. For extensive scalp BCC, neurosurgery involvement may be necessary for complete extirpation of disease. Similarly, for advanced orbit BCC, ophthalmology or oculoplastic surgery can be helpful for complex orbit-sparing procedures. For extensive BCC involving the maxilla, oral oncology support may be helpful for potential dental extractions, radiation molds, and obturator placement for anticipated oral antral fistula. Pre- and postauricular lesions may dictate the need for parotidectomy and/or lateral temporal bone resection, necessitating a neuro-otologist. If the anticipated surgical defect is large or particularly complex, a microvascular reconstruction is often an ideal choice, especially if postoperative radiation is likely.
The incidence of metastasis of BCC is extremely low, approximately 0.003 percent to 0.1 percent of cases [37]. However, the presence of multiple primary tumors in the head and neck has been cited as a risk for the occurrence of metastasis. In fact, of the reported metastatic BCC cases, 85–90% were attributed to primary tumors in the head and neck [38, 39]. Thus, there is very little literature regarding the utility of sentinel lymph node biopsy and elective neck dissection in advanced BCC. While the potential utility of lymph node dissection is very low even in advanced head and neck BCC, there have been reports of sentinel lymph node biopsy in certain high-risk types of BCC, including basosquamous carcinoma [40].
Radiation therapy has been studied extensively in BCC. As a single modality, radiation therapy is effective for BCC not amenable to surgery, including BCC that if excised would lead to significant cosmetic deformity, or in patients too frail to undergo surgical excision [41]. Tumor size and location often dictate the course of radiation to be given. Doses and number of fractions are variable, but most head and neck BCC can be treated to a total of 40–50 Gy over 10–20 fractions [41]. Larger tumors often receive higher dose/fractions, whereas elderly, ill patients may be treated more palliatively with a lower dose over a shorter period of time [41]. Radiation as a single modality provides acceptable cure rates for small head and neck BCC, but is less efficacious with larger cancers. Head and neck BCC less than 2 cm treated with radiation alone have been shown to have 98% local control rate at 10 years. Conversely, BCC greater than 5 cm had only 53% local control at 8 years [42]. Further, advanced BCCs treated with radiation alone have an unacceptably high and cause-specific mortality [43], highlighting the need for multimodality therapy in this high-risk group of patients.
In the postoperative setting, radiation has been shown to be of benefit in select cases. Adjuvant radiation should be considered in patients with multiply recurrent disease, positive margins after multiple resections, perineural invasion, T4 disease with extensive soft tissue or bony invasion, or lymph node metastasis [44, 45].
Historically, there has been little use for systemic therapy in the treatment of BCC. However, in recent years, the Hedgehog pathway inhibitors for the treatment of BCC have emerged as a treatment option in the locally advanced or metastatic setting. Vismodegib and sonidegib are smoothened (smo) inhibitors (see Fig. 8.3), which have shown safety and efficacy in treating advanced BCC. Vismodegib was initially FDA approved for use in 2012, when a prospective study revealed a 30% response rate in patients with metastatic BCC and a 43% response rate in patients with locally advanced BCC [46]. Complete response was observed in 21% of patients with locally advanced BCC [46]. Sonidegib was introduced in 2015 following a phase II randomized double-blinded study demonstrating a 12-month objective response rate of 57.6% in locally advanced BCC and 7.7% in metastatic BCC [47,48,49]. A recent meta-analysis of studies using vismodegib and sonidegib in advanced BCC confirmed these findings, showing similar overall response rates in locally advanced disease (69% vs. 57%, respectively), but significant complete response rates in only vismodegib (31% vs. 3%) [50]. However, such a comparison may be misleading. Although there has not been a cross-trial comparison, sonidegib and vismodegib were compared using a matching-adjusted indirect comparison to reduce confounding of treatment effects which could have occurred in an unadjusted indirect comparison. Patients from the sonidegib trial had an objective response rate (ORR) of 56.7% and progression-free survival (PFS) of 22.1 months, whereas patients from the vismodegib trial displayed an ORR of 47.6% and PFS of 9.5 months, thus indicating a slightly greater benefit with sonidegib therapy [51].
Vismodegib has been used in the neoadjuvant setting in locally advanced head and neck BCC, where early reports have shown very promising results in tumor reduction, allowing for more modest organ-sparing surgical excision or radiation treatment [52]. A dramatic example is shown in Fig. 8.5. Vismodegib may also have some applications in a concurrent treatment setting: a recent study revealed that vismodegib treated cell lines were more radiosensitive than control [53]. Thus, future applications of targeted systemic therapies will likely yield further evolution in the multidisciplinary management of advanced BCC.

Axial T1 MRI sequence depicting a dramatic response of locally invasive BCC (with temporal bone and intracranial extension) before (a) and after (b) 3 months of neoadjuvant vismodegib. The patient had an excellent response to treatment and went on to definitive surgical resection
Conclusion
BCC is a ubiquitous disease entity with excellent treatment options. A variety of clinical subspecialties are involved in the care of patients with BCC of the head and neck, and understanding the populations at risk, molecular pathogenesis, and workup is key to managing BCC appropriately. Surgery is a cornerstone of BCC treatment and generally provides optimal outcomes with acceptable function and cosmesis. With the elucidation of the molecular pathogenesis of BCC, exciting novel therapies are now available and appear to be primed to change the paradigm of treating locally advanced and metastatic BCC. Most importantly, a multidisciplinary approach is crucial in patients with locally advanced or metastatic BCC of the head and neck.
References
Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. population, 2012. JAMA Dermatol. 2015;151(10):1081–6.
Staples MP, Elwood M, Burton RC, et al. Non-melanoma skin cancer in Australia: the 2002 national survey and trends since 1985. Med J Aust. 2006;184:6–10.
Marzuka AG, Book SE. Basal cell carcinoma: pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management. Yale J Biol Med. 2015;88(2):167–79.
Armstrong BK, Kricker A, English DR. Sun exposure and skin cancer. Australas J Dematol. 1997;38:1): 1–6.
Chuang TY, Popescu A, Su WP, Chute CG. Basal cell carcinoma. A population-based incidence study in Rochester, Minnesota. J Am Acad Dermatol. 1990;22(3):413–7.
Kricker A, Armstrong BK, English DR, Heenan PJ. Does intermittent sun exposure cause basal cell carcinoma? A case-control study in Western Australia. Int J Cancer. 1995;60(4):489–94.
Iannacone MR, Wang W, Stockwell HG, O’Rourke K, Giuliano AR, Sondak VK, Messina JL, Roetzheim RG, Cherpelis BS, Fenske NA, Rollison DE. Patterns and timing of sunlight exposure and risk of basal cell and squamous cell carcinomas of the skin—a case control study. BMC Cancer. 2012;12:417.
Ferrucci LM, Cartmel B, Molinaro AM, Leffell DJ, Bale AE, Mayne ST. Indoor tanning and risk of early-onset basal cell carcinoma. J Am Acad Dermatol. 2011;67(4):552–62.
Robinson SN, Zens MS, Perry AE, Spencer SK, Duell EJ, Karagas MR. Photosensitizing agents and the risk of non-melanoma skin cancer: a population-based case-control study. J Invest Dermatol. 2013;133(8):1950–5.
Karagas MR, Stukel TA, Greenberg ER, Baron JA, Mott LA, Stern RS. Risk of subsequent basal cell carcinoma and squamous cell carcinoma of the skin among patients with prior skin cancer. Skin Cancer Prevention Study Group. JAMA. 1992;267(24):3305–10.
Marghoob A, Kopf AW, Bart RS, Sanfilippo L, Silverman MK, Lee P. Risk of another basal cell carcinoma developing after treatment of a basal cell carcinoma. J Am Acad Dermatol. 1998;28(1):22–8.
Kanjilal S, Strom SS, Clayman GL, Weber RS, el-Naggar AK, Kapur V, Cummings KK, Hill LA, Spitz MR, Kripke ML, et al. P53 mutations in nonmelanoma skin cancer of the head and neck: molecular evidence for field cancerization. Cancer Res. 1995;55(16):3604–9.
Karagas MR, McDonald JA, Greenberg ER, Stukel TA, Weiss JE, Baron JA, Stevens MM. Risk of basal cell and squamous cell skin cancers after ionizing radiation therapy. For the Skin Cancer Prevention Study Group. J Natl Cancer Inst. 1996;88(24):1848–53.
Boonchai W, Green A, Ng J, Dicker A, Chenevix-Trench G. Basal cell carcinoma in chronic arsenicism occurring in Queensland, Australia, after ingestion of an asthma medication. J Am Acad Dermatol. 2000;43(4):664–9.
Webb MC, Compton F, Andrews PA, Koffman CG. Skin tumors post transplantation: a retrospective analysis at a single center. Transplant Proc. 1997;29:828–30.
Hartevelt MM, Bavinck JN, Kootte AMM, Vermeer BJ, Vandenbroucke JP. Incidence of skin cancer after renal transplantation in the Netherlands. Transplantation. 1990;49:506–9.
Ramsay HM, Fryer AA, Hawley CM, Smith AG, Harden PN. Non-melanoma skin cancer risk in the Queensland renal transplant population. Br J Dermatol. 2002;147:950–6.
Jensen P, Hansen S, Moller B, Leivestad T, Pfeffer P, Geiran O, Fauchald P, Simonsen S. Skin cancer in kidney and heart transplant recipients and different long-term immunosuppressive therapy regimens. J Am Acad Dermatol. 1999;40(2):177–86.
Ducloux D, Carron PL, Rebibou JM, Aubin F, Fournier V, Bresson-Vautrin C, Blanc D, Humbert P, Chalopin JM. CD4 lymphocytopenia as a risk factor for skin cancers in renal transplant patients. Transplantation. 1998;65(9):1270–2.
Omland SH, Ahlstrom MG, Gerstoft J, Pedersen G, Mohey R, Pedersen C, Kronborg G, Larsen CS, Kvinesdal B, Gniadecki R, Obel N, Omland LH. Risk of skin cancer in HIV-infected patients: a Danish nationwide cohort study. J Am Acad Dermatol. 2018;18:30475, epub ahead of print.
Gorlin RJ, Goltz RW. Multiple nevoid basal-cell epithelioma, jaw cysts, and bifid rib. A syndrome. N Engl J Med. 1960;262:908–12.
Farndon PA, Del Mastro RG, Evans DG, Kilpatrick MW. Location of gene for Gorlin syndrome. Lancet. 1992;339(8793):581–2.
Gailani MR, Leffell DJ, Ziegler A, Gross EG, Brash DE, Bale AE. Relationship between sunlight exposure and a key genetic alteration in basal cell carcinoma. J Natl Cancer Inst. 1996;88(6):349–54.
Stone DM, Hynes M, Armanini M, Swanson TA, Gu Q, Johnson RL, et al. The tumour-suppressor gene patched encodes a candidate receptor for Sonic Hedgehog. Nature. 1996;384(6605):129–34.
Fan H, Oro AE, Scott MP, Khavari PA. Induction of basal cell carcinoma features in transgenic human skin expressing Sonic Hedgehog. Nat Med. 1997;3(7):788–92.
De Zwaan SE, Haass NK. Genetics of basal cell carcinoma. Australas J Dermatol. 2010;51(2):81–92.
Ponten F, Berg C, Ahmadian A, et al. Molecular pathology in basal cell cancer with p53 as a genetic marker. Oncogene. 1997;15(9):1059–67.
Omland SH. Local immune response in cutaneous basal cell carcinoma. Dan Med J. 2017;64(10):5412.
Bichakjian CK, Olencki T, Aasi SZ, et al. Basal cell skin cancer, version 1.2016, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2016;14(5):574–97.
Amin MB, Edge S, Greene F, et al., editors. AJCC cancer staging manual. 8th ed. New York: Springer; 2017.
Miller SJ, Alam M, Andersen J, Berg D, Bichakjian CK, Bowen G, et al. Basal cell and squamous cell skin cancers. J Natl Compr Cancer Netw. 2010;8(8):836–64.
Wolf DJ, Zitelli JA. Surgical margins for basal cell carcinoma. Arch Dermatol. 1987;123(3):340–4.
Jerant AF, Johnson JT, Sheridan CD, Caffrey TJ. Early detection and treatment of skin cancer. Am Fam Physician. 2000;62(2):357–82.
van Loo E, Mosterd K, Krekels GA, Roozeboom MH, Ostertag JU, Dirksen CD, Steijlen PM, Neumann HA, Nelemans PJ, Kelleners-Smeets NW. Surgical excision versus Mohs micrographic surgery for basal cell carcinoma of the face: a randomized clinical trial with 10 years follow-up. Eur J Cancer. 2014;50(17):3011–20.
Muller FM, Dawe RS, Moseley H, Fleming CJ. Randomized comparison of Mohs micrographic surgery and surgical excision for small nodular basal cell carcinoma: tissue-sparing outcome. Dermatol Surg. 2009;35(9):1349–54.
Yalcin O, Sezer E, Kabukcuoglu F, Kilic AI, Sari AG, Cerman AA, Altunay IK. Presence of ulceration, but not high risk zone location, correlates with unfavorable histopathological subtype in facial basal cell carcinoma. Int J Clin Exp Pathol. 2015;8(11):15448–53.
Von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. Report of five cases and review of 170 cases in the literature. J Am Acad Dermatol. 1984;10(6):1043–60.
Ozgediz D, Smith EB, Zheng J, Otero J, Tabatabai ZL, Corvera CU. Basal cell carcinoma does metastasize. Dermatol Online J. 2008;14(8):5.
Wadhera A, Fazio M, Bricca G, Stanton O. Metastatic basal cell carcinoma: a case report and literature review. How accurate is our incidence data? Dermatol Online J. 2006;12(5):7.
Jankovic I, Kovacevic P, Visnjic M, et al. Application of sentinel lymph node biopsy in cutaneous basosquamous carcinoma. Ann Dermatol. 2011;23(1):123–6.
McGovern S, Ballo M. Radiation oncology in skin cancer treatment. In: MacFarlane D, editor. Skin Cancer management. New York: Springer; 2010. p. 259–71.
Petrovich Z, Kuisk H, Langholz B, et al. Treatment results and patterns of failure in 646 patients with carcinoma of the eyelids, pinna, and nose. Am J Surg. 1987;154(4):447–50.
Kwan W, Wilson D, Moravan V. Radiotherapy for locally advanced basal cell and squamous cell carcinomas of the skin. Int J Radiat Oncol Biol Phys. 2004;60(2):406–11.
Jackson JE, Dickie GJ, Wiltshire KL, et al. Radiotherapy for perineural invasion in cutaneous head and neck carcinomas: toward a risk-adapted treatment approach. Head Neck. 2009;31(5):604–10.
Lott DG, Manz R, Koch C, Lorenz RR. Aggressive behavior of nonmelanotic skin cancers in solid organ transplant recipients. Transplantation. 2010;90(6):683–7.
Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal cell carcinoma. N Engl J Med. 2012;366(23):2171–9.
Jain S, Song R, Xie J. Sonidegib: mechanism of action, pharmacology, and clinical utility for advanced basal cell carcinomas. Onco Targets Ther. 2017;10:1645–53.
Dummer R, Guminski A, Gutzmer R, et al. The 12-month analysis from basal cell carcinoma outcomes with LDE225 treatment (BOLT): a phase II, randomized, double-blind study of sonidegib in patients with advanced basal cell carcinoma. J Am Acad Dermatol. 2016;75(1):113–25.
Midgen MR, Guminski A, Gutzmer R, et al. Treatment with two different doses of sonidegib in patients with locally advanced or metastatic basal cell carcinoma (BOLT): a multicentre, randomised, double-blind phase 2 trial. Lancet Oncol. 2015;16(6):716–28.
Xie P, Lefrançois P. Efficacy, safety, and comparison of sonic hedgehog inhibitors in basal cell carcinomas: a systematic review and meta-analysis. J Am Acad Dermatol. 2018;79:1089. https://doi.org/10.1016/j.jaad.2018.07.004.
Odom D, Mladsi D, Purser M, et al. A matching-adjusted indirect comparison of sonidegib and vismodegib in advanced basal cell carcinoma. J Skin Cancer. 2017;2017:ePub 6121760.
Block AM, Alite F, Diaz AD. Combination trimodality therapy using vismodegib for basal cell carcinoma of the face. Case Rep Oncol Med. 2015;2015:1. https://doi.org/10.1155/2015/827608.
Hehlgans S, Booms P, Gullulu O, et al. Radiation sensitization of basal cell and head and neck squamous cell carcinoma by the hedgehog pathway inhibitor vismodegib. Int J Mol Sci. 2018;19(9):E2485.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kansara, S., Yao, C.M.K.L., Gross, N.D. (2020). Surgical Treatment for Basal Cell Carcinoma of the Head and Neck. In: Migden, M., Chen, L., Silapunt, S. (eds) Basal Cell Carcinoma. Springer, Cham. https://doi.org/10.1007/978-3-030-26887-9_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-26887-9_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-26886-2
Online ISBN: 978-3-030-26887-9
eBook Packages: MedicineMedicine (R0)