
Abstract
Basal cell carcinoma (BCC) is the most common skin cancer in Caucasians, Hispanics, and Asians. While it is far more prevalent in Caucasians, it nevertheless presents in all skin types. Unfortunately, false perceptions regarding inherent photoprotection from melanin lead to delays in diagnosis and treatment in darker skin types. The classic presentation, a translucent solitary nodule on sun-exposed sites such as the head and neck, is common across various skin types. Treatment options, including destruction, surgery, radiation, and topical chemotherapy, are similar across races. This chapter will review the epidemiology, pathophysiology, clinical presentations, differential diagnoses, histopathology, and treatment of basal cell carcinoma.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Basal cell carcinoma is a slow-growing skin cancer typically found on the head and neck that is induced by ultraviolet radiation. Individuals with darker skin types have inherent protection from ultraviolet light due to an increase in epidermal melanin causing sun-induced skin cancer to be less prevalent [1]. Although diagnosis and management are similar across different skin types, delays in diagnosis and treatment exist in darker skin types as there are false perceptions regarding inherent photoprotection and the ability to develop skin cancer.
2 Epidemiology
BCC is the most common skin cancer in Caucasians, Hispanics, Chinese, and Japanese and the second most common skin cancer in Blacks and Asian Indians. However, because melanin is photoprotective, BCC is 19 times more common in Caucasians than in Blacks [2]. BCC comprises 65–75 % of skin cancer in Caucasians, compared to 30 % in Indians, 12–35 % in American Blacks, and 2–8 % in African Blacks. Considering the diversity of skin color with different concentrations of melanin in the epidermis, inherent sun protection varies widely in skin color leading to variable prevalence rates [3].
3 Etiology
Basal cell carcinoma is associated with long-term cumulative ultraviolet radiation (UVR) exposure, particularly UVB. UVB directly damages DNA and RNA causing a transition mutation in the nucleic acid sequence [2]. Although UVR plays a significant role in the development of BCC, it is not the only risk factor, as BCC can also occur in non-sun-exposed skin. Other factors predisposing to BCC are ingestion of arsenic, radiation, scars, ulcers, albinism, nevus sebaceous, immunosuppression, and genetic conditions such as Gorlin’s syndrome and xeroderma pigmentosum.
4 Clinical Features
In skin of color patients, similar to Caucasians, BCC most commonly occurs in patients over age 50. Seventy to ninety percent of BCCs develop on the head and neck region, followed by the trunk, then extremities. The clinical presentation and histologic features of BCC are somewhat different in people of color than Caucasians [1, 4]. The most common clinical presentation across skin types is nodular BCC, which typically presents as a solitary asymptomatic papule or nodule with telangiectasias and a rolled border. As lesions progress, they may develop ulceration (Figs. 42.1, 42.2, and 42.3). The classic findings of telangiectasias and a pearly rolled border may be challenging to appreciate in darker skin types [5]. BCCs in Asians often appear brown to glossy black and are described as having a “pearly black” appearance. Pigmented BCC, a variant of nodular BCC, is much more common in darker-skinned patients and represents more than 50 % of BCCs in Blacks, Hispanics, and Asians, compared to 6 % in Caucasians (Figs. 42.4 and 42.5) [1, 5]. Superficial BCC presents as an erythematous scaly plaque most commonly on the trunk or extremity (Fig. 42.6). Morpheaform BCC is less common in Blacks than Caucasians and presents with a porcelain-colored plaque with smooth indistinct borders that may be atrophic or indurated (Fig. 42.7).

Nodular BCC presenting as a pearly papule with telangiectasias on the lower eyelid of a Hispanic female

Large nodular BCC with prominent telangiectasias, a translucent rolled border, and early central ulceration on the lower eyelid of a Hispanic female

Large nodular BCC on the scalp of an elderly Hispanic female

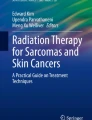
Pigmented BCC with glossy black or pearly black appearance on the upper cutaneous lip of a Hispanic male

Pigmented BCC with rolled border and central ulceration on the cheek of a Hispanic male

Superficial BCC presenting as erythematous scaly plaque on the arm of a Hispanic male

Morpheaform BCC with features of pearliness and porcelain-white areas on the arm of a Hispanic female
5 Natural History and Prognosis
Although BCCs are slow-growing neoplasms that rarely metastasize, they can be locally invasive and can cause significant morbidity and cosmetic disfigurement. Metastatic rates range from 0.0028 to 0.1 % and do not vary based on skin type.
6 Histopathology
BCC is classified into five main histologic and clinical subtypes. The most common subtype, nodular BCC, is characterized by basophilic aggregates with peripheral palisading and retraction artifact in the papillary and reticular dermis. Pigmented BCC also has melanin and melanocytes within the tumor. Superficial BCC has similar basophilic aggregates with peripheral palisading and clefting arising from the epidermis. Micronodular BCC is similar to nodular BCC, with smaller tumor islands that are widely dispersed. Infiltrative BCC presents with cords and strands of neoplastic cells infiltrating through collagen fibers often deep in the dermis. A fibrotic stroma and frequent mitoses are observed. Morpheaform BCC is marked by strands of basaloid neoplastic cells embedded in a characteristic heavily fibrotic stroma.
7 Diagnosis and Differential Diagnosis
The diagnosis of BCC is made on clinical examination and histology. Physical examination should focus on identifying tumor size, palpating clinical margins, and lymph node exam. Diagnosis is confirmed with a skin biopsy of a suspicious lesion. The differential diagnosis for a BCC includes squamous cell carcinoma, actinic keratosis, seborrheic keratosis, melanoma, nevi, angiofibroma, and sebaceous hyperplasia. Pigmented BCC can be particularly challenging to differentiate from seborrheic keratoses, blue nevi, lentigines, or melanoma.
8 Treatment
A variety of treatment options exist for BCC. Clinical and histologic traits such as tumor size, location, and histology determine whether the tumor is low risk or high risk. The goal is complete removal of the tumor with maximal preservation of function and cosmetic appearance. The treatment modality should be tailored to the individual patient with consideration for the location and size of the cancer and the patient’s preferences, age, and general health.
Surgery is the most common treatment modality for basal cell carcinoma. The three modalities used are electrodessication and curettage, wide local excision, and Mohs micrographic surgery. In electrodessication and curettage, the tumor is removed by curettage followed by electrodessication of the lesion with a 2–3 mm margin. This method is indicated for smaller superficial or nodular BCCs on the trunk and extremity. A wide local excision with 4–6 mm is considered for well-defined larger skin cancers on the trunk and extremity. Mohs micrographic surgery can offer superior histologic margin control and maximum tissue conservation. Indications for Mohs micrographic surgery in individuals with BCC include location on central face, ear or lip, tumors >2 cm on the trunk, recurrent lesions, incompletely excised lesions, tumors with morpheaform or infiltrative histology, poorly defined lesions, lesions with perineural invasion, lesions arising in scar/radiation sites, immunosuppression, and history of genetic conditions such as Gorlin’s syndrome and xeroderma pigmentosum.
Topical treatments can be employed for low-risk patients with primary superficial BCC who cannot undergo surgery or radiation or in patients with multiple primary tumors even though the cure rate is lower than surgical excision. Both imiquimod and topical 5-fluorouracil are approved by the US Food and Drug Administration for the treatment of superficial BCC <2 cm on the trunk and extremity.
Vismodegib is a novel therapeutic agent that targets the Hedgehog signaling pathway and was recently approved by the FDA in 2012 for the treatment of metastatic BCC.
References
Gloster Jr HM, Neal K. Skin cancer in skin of color. J Am Acad Dermatol. 2006;55(5):741–60; quiz 61–4. PubMed PMID: 17052479. Epub 2006/10/21. eng.
Roewert-Huber J, Lange-Asschenfeldt B, Stockfleth E, Kerl H. Epidemiology and aetiology of basal cell carcinoma. Br J Dermatol. 2007;157 Suppl 2:47–51. PubMed PMID: 18067632. Epub 2007/12/11. eng.
Battie C, Gohara M, Verschoore M, Roberts W. Skin cancer in skin of color: an update on current facts, trends, and misconceptions. J Drugs Dermatol. 2013;12(2):194–8. PubMed PMID: 23377393. Epub 2013/02/05. eng.
Kim GK, Del Rosso JQ, Bellew S. Skin cancer in Asians: part 1: nonmelanoma skin cancer. J Clin Aesthet Dermatol. 2009;2(8):39–42. PubMed PMID: 20729955. Pubmed Central PMCID: 2923966. Epub 2010/08/24. eng.
Ahluwalia J, Hadjicharalambous E, Mehregan D. Basal cell carcinoma in skin of color. J Drugs Dermatol. 2012;11(4):484–6. PubMed PMID: 22453586. Epub 2012/03/29. eng.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Duong, T., Srivastava, D. (2014). Basal Cell Carcinoma. In: Jackson-Richards, D., Pandya, A. (eds) Dermatology Atlas for Skin of Color. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-54446-0_42
Download citation
DOI: https://doi.org/10.1007/978-3-642-54446-0_42
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-54445-3
Online ISBN: 978-3-642-54446-0
eBook Packages: MedicineMedicine (R0)