
Abstract
The cryopreservation of mammalian embryos has expanded over the past 20 yr by encompassing a range of sophisticated methods to deal with different developmental stages and different sensitivities to low-temperature exposure. We have described a method for slow, controlled-rate freezing of early stage embryos based on exposure to 1,2-propanediol and sucrose, while the method for late-stage (blastocyst) embryos employs mixtures of glycerol and sucrose. Both methods have been used for animal and human embryos. A third rapid cooling or “vitrification” technique is described, which depends on brief but controlled exposure of multicellular embryos to mixtures of glycerol and 1,2-propanediol at high concentrations. This technique is used for successful animal embryo cryopreservation but is not yet widely applied in the clinic.
Access provided by Autonomous University of Puebla. Download protocol PDF
Similar content being viewed by others

Key Words
1 Introduction
The development of cryopreservation techniques for preimplantation-stage mammalian embryos has progressed hand in hand with, and largely driven by, advances in their in vitro manipulation and culture. Important early work included the in vitro culture of eight-cell mouse embryos to the blastocyst stage (1), the demonstration that mouse embryos cultured in vitro could be transferred to host mothers and yield live offspring (2), the growth of human embryos to the blastocyst stage in culture (3), and the birth of a calf after in vitro fertilization and embryo culture (4).
Throughout this period, it was becoming obvious that embryo cryopreservation would too become centrally important in reproductive technologies by allowing optimal utilization of resources in the development of breeding programs in animals (5) by permitting genetic banking (for example, of rare or economically important mouse strains [6]), and by enhancing the clinical approach to infertility treatment, where often more embryos are produced in vitro than can be safely implanted in the mother (7).
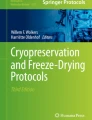
The first mammalian species to have embryos successfully cryopreserved was the mouse in the early 1970s (8,9), and over the next three decades this has been extended to embryos of most species, including rat, rabbit, cow, goat, sheep, pig, horse, canine and feline species, primates, and man. Across all these different species, the protocols applied to embryo cryopreservation tend to fall into one of two broad categories, (1) slow controlled-rate cooling and (2) ultrarapid cooling or vitrification (see Chapter 3). The choice of protocol is most often dictated by logistical or regulatory concerns, and may be affected by additional factors such as species peculiarities and the stage of embryonic development. These will be highlighted next, but it is worth discussing briefly the origins and concepts behind the two seemingly different approaches. It is also important to recognize that the term “preimplantation embryo” covers a range of developmental stages with specific morphologies ( Fig. 1 ), which can dictate how these cells are manipulated in vitro or cryopreserved.

Micrographs of mouse embryos of different developmental stages (magnification ×40).(A) Two-cell embryos at day 1 after fertilization. A group of two-cell embryos; for each, the acellular glycoprotein coating zona pellucida—surrounds the two equally sized blastomeres produced at the first cleavage stage of each fertilized oocyte. (B) Four- to eight-cell embryos at day 2 after fertilization. Each embryo is still surrounded by its’ zona pellucida; some embryos have cleaved at a slightly different rate. (C) Blastocysts at day 5 after fertilization. Multiple cell divisions have taken place yielding many small blastomeres (more than 60). In several cases, the blastocysts have “hatched” or broken free from the zona pellucida leaving an empty, fractured zona in a step that would be a preparation for implantation in vivo.
The earliest successes with mouse embryo cryopreservation were achieved with eight-cell mouse embryos employing prior exposure to a cryoprotective agent (CPA) and cooling slowly, at a constant rate, to deep subzero temperatures (8). In this case, the CPA was dimethyl sulfoxide at a concentration of 1.5 M. The contemporary work of the period highlighted the sensitivity of embryos to the cooling rate, and from this fact was the need to cool slowly dictated (at <−1°C/min). Cryomicroscope observations of embryos during this cooling procedure demonstrated the extreme dehydration encountered during the process when ice formed from pure water as extracellular ice formed around the cells, leaving the embryos in the small, residual hypertonic unfrozen fraction (10). Conditions that permitted intracellular ice to form (by cooling too fast [11] and leaving water molecules capable of nucleating ice crystal growth) were universally found to be damaging. It was also argued that slow warming was necessary to avoid cell volume stress, which might be encountered if the dehydrated embryos were warmed rapidly driving near-instantaneous redistribution of cell water content. The target temperature of the slow cooling was selected as −80°C, known from other cell types to be sufficiently low to inhibit (at a logistically practical level) further ice crystal growth, before transferring the embryos to liquid nitrogen temperature for true long-term storage. In reality, later work suggested that by using this approach, ice crystal growth inside the individual blastomeres of the embryos was avoided by the extreme dehydration, leaving the cell contents in a “glassy,” amorphous state at very low temperatures (12).
In the intervening time, further investigations demonstrated that this low-temperature glass (and successful embryo cryopreservation) could be achieved if the embryos were slowly cooled only to a relatively high subzero temperature, and then transferred directly to −196°C. In this case, warming needed to be rapid to achieve high viability (by direct immersion of the tubes into a warm water bath between 30 and 37°C). It was here argued that this interrupted slow cool had not resulted in conversion of all water potentially available for extracellular ice formation into ice crystals, leaving a possibility for harmful intracellular ice to nucleate and form during warming. Rapid warming was needed to “out-race” the intracellular ice formation. At a prosaic level, this reduced time of cooling and rapid warming was technically attractive, making the protocols easier to handle. In general, the interrupted slow cool has become the favored approach for most groups using slow cooling in embryo cryopreservation.
The second approach (vitrification) has its’ roots in the observations made by Luyet in the 1930s, that it might be possible to recover living cells from very low temperatures if they were cooled in a way that inhibited ice crystal growth all together, achieving a glass (or vitreous state) throughout the whole sample (13). In retrospect, it has become recognized that this is another facet of the requirement to produce an “intracellular” glass either by slow or rapid cooling, discussed previously. At first, this seemed an unattainable goal in real biological samples because the rate of cooling would need to be extremely high (in excess of thousands of degrees per min), but the pioneering work of Rall and Fahy (14) showed that by careful manipulation of high concentrations of CPA and application of small sample sizes, a “quasi-vitreous” state could be achieved in mouse embryos. As long as warming was again sufficiently rapid, high rates of survival in eight-cell mouse embryos were achieved. This work had led to growing interest in the technique and its’ application to different embryonic stages across a range of species, including human embryos. Much of the effort has been directed toward developing small sample holders (such as the tiny nylon loops [15] pioneered by Lane et al.) that allow embryos to be vitrified in volumes of a few microliters. Such small volumes are necessary to permit sufficient rapid heat transfer to enable very rapid cooling, and especially very rapid warming (to “outrun” the potential growth of ice crystals during rewarming). The other main area of investigation has been the concerned selection of less toxic mixtures of CPA. These are often needed in the range of 50% (w/v) to achieve the glassy state.
More extensive information concerning the underlying principles in mammalian embryo cryopreservation across a range of species can be found in a number of reviews ([16–21]; Chapter 3). There are interspecies differences that have dictated survival from cryopreservation. The well-documented sensitivity of porcine embryos to chilling and cryopreservation, often related to the high-lipid content of the blastomeres, has long been a major hurdle to widespread application of the technology, but vitrification may offer a hope of improvements (21). In in vitro-cultured bovine embryos, a similar problem of blastomere lipid inclusions has been encountered, and specific approaches, such as cell centrifugation, have been applied to enhance recovery from cryopreservation (18).
Beyond the descriptions of cryopreservation technologies, there are many other practical issues to consider when establishing embryos banks that are beyond the scope of the current chapter, but include clear and unambiguous methods for marking stored material (in cryovials, straws, or other containers), and a well-organized cryostorage facility with detailed and fail-safe records and inventory system for tracing banked embryos which may be held in the repository for many years. Nevertheless, the importance of cryopreserved embryo banks, both from a scientific and commercial standpoint in areas such as transgenic animal technology, is clearly established (22).
2 Materials
These are essentially the same as those needed for oocyte cryopreservation (see Chapter 22) but will be repeated for clarity. All chemicals, reagents, and water should be of the highest grade (analytical reagent or tissue culture grades).
-
1.
A source of liquid nitrogen, liquid nitrogen storage tanks, and Dewars for handling liquid nitrogen, as well as oxygen monitors for rooms where large quantities of the cryogen are stored (see Notes 1 and 2 ).
-
2.
A controlled-rate freezing machine (available from several sources such as Planer plc, Middlesex, UK or Asymptote, Cambridge, UK).
-
3.
Safety equipment, e.g., cryogloves, face shield, and an oxygen depletion monitor.
-
4.
37°C gassed incubators for culture.
-
5.
Equipment for handling and manipulating embryos including an inverted microscope for visualising embryo transfer (for example, available from Nikon.co.uk), pulled glass pipets, or an automated pipet.
-
6.
Heated water bath.
-
7.
Embryo culture medium, such as human tubule fluid (HTF) medium, (available from several sources, including Cook IVF, Brisbane, Australia and CGA/Diasint, Florence, Italy).
-
8.
Petri dishes (Falcon, BD Biosciences, Oxford, UK).
-
9.
Dulbecco’s phosphate-buffered solution (PBS; Gibco Life Technologies, Paisley, UK) supplemented when required with 30% (w/v) protein supplement, e.g., plasma protein supplement (Baxter AG, Vienna, Austria) or serum protein supplement (Pacific Andrology, CGA/Diasint). For animal embryos, heat-inactivated fetal bovine serum may be used (Invitrogen, Paisley, UK). These are collectively called serum-supplemented PBS (PBSs).
-
10.
Plastic straws (CryoBiosystem, L’Aigle, France) or plastic cryovials (Nunc, Roskilde, Denmark) are commonly used to contain embryos during cryopreservation. There are particular points of consideration when using straws, such as their heat transfer capacity that dictate care in handling frozen specimens, and their safe storage (see Notes 3 and 4 ). There are also tried and tested methods for filling straws with the various cryoprotectant solutions and Diluents to enhance the cryopreservation protocol (see Note 5 ), and these should be practiced before embarking on a full cryopreservation run.
-
11.
Microscope (×40 magnification).
-
12.
Freezing solutions: 1.5 M 1,2-propanediol (PrOH) and 1.5 M PrOH plus 0.2 M sucrose, both made up in PBSs.
-
13.
Thawing solutions: 1.0 M PrOH plus 0.2 M sucrose. 0.5 M PrOH plus 0.2 M sucrose, and 0.2 M sucrose, all made up in PBSs.
-
14.
Vitrification solutions: 10% (w/v) glycerol + 20% (w/v) 1,2 propanediol in PBSs, and 25% (w/v) glycerol + 25% (w/v) 1,2-propanediol.
-
1.
Thawing solutions for vitrification: 1 M sucrose in PBSs.
-
2.
For vitrification (optional): small nylon loops, as described by Lane and colleagues (15), or open-pulled straws (MINITÜB, Abfüll - und Labortechnik GmbH and Co. Tiefenbach, Germany). This company also supplies equipment sets for embryo vitrification). Another source of open-pulled straws is SZIGTA, Clayton, Australia.
-
1.
3 Methods
Three different methods are described here that cover the range of cryopreservation protocols for embryos of different developmental stages, applying either slow, controlled-rate cooling or vitrification (see Note 6 ). This obviously is not a comprehensive list of protocols in current use, but they do represent methods that are relatively straightforward, have been confirmed by several groups, and can be seen as basic expertise, which, once mastered, can be applied to other cryopreservation strategies if desired.
There are many other factors which, on a day-to-day basis, will affect the success of embryo cryopreservation procedures (see Notes 7 and 8 ). These need to be kept in mind when reviewing the success of embryo cryopreservation within an individual unit.
3.1 Slow Controlled-Rate Cooling of Early-Stage Embryos
The use of slow, controlled-rate cooling using a purpose-built freezing machine for embryo cryopreservation is currently the most common technique in both clinical and veterinary embryo transfer practices. One reason is that records of cooling profiles can be recorded and documented, so that the best practice can be monitored. The method described here for slow cooling of early-stage preimplantation embryos has found application in a variety of species, and is based on the method described by several authors, including Byrd (23). (For embryos from one-cell to four- to eight-cells).
-
1.
Straws should be loaded with a column of 1.5 M PrOH plus 0.2 M sucrose and held at room temperature (20 ± 2°C) (see Note 8 ; Fig. 1 ; Chapter 22).
Prepare droplets (0.5 mL each) of PBS plus protein supplement, for example, 20% (v/v) serum, (PBSs), 0.5 M PrOH in PBSs, 1.0 M PrOH in PBSs, and 1.5 M PrOH with 0.2 M sucrose in PBSs. The droplets are placed in a tissue culture dish at room temperature. Label each droplet area.
-
2.
Place the cohort of embryos (usually not more than six per droplet) in the PBSs for an initial wash, and then transfer to 0.5 M PrOH for 5 min at room temperature.
-
3.
Transfer the embryos into the 1.0 M PrOH for another 5 min, and then into the 1.5 M PrOH plus 0.2 M sucrose for a final 5 min. (Total cryoprotectant exposure time of 15 min.)
-
4.
Transfer the embryos into the prepared straws (usually two to three embryos per straw) into the column of 1.5 M PrOH plus 0.2 M sucrose. Plug the straws and place them into the cooling machine set at 20°C. Initiate cooling at a rate of −1°C/min to a holding temperature of −7°C.
-
5.
On reaching −7°C, ice nucleation or “seeding” is carried out in the solution containing the embryos (see Note 9 ). The straws are returned to the cooling chamber and held at this same temperature for 10 min to allow dissipation of the latent heat of ice formation.
-
6.
The next cooling stage is then initiated at a rate of −0.3°C/min to −35°C, and then followed by a rapid cooling phase at −50 to −150°C. The straws may then be transferred into a flask of liquid nitrogen, and finally into the liquid nitrogen storage facility. Appropriate protective equipment should be worn at all stages when handling cryogens. There are important issues concerning management of storage facilities and decontaminating outer surfaces of straws or cryovials as part of cryopreservation protocols in general (see Note 10 and Chapter 1).
-
7.
When rewarming is required, first prepare dishes containing 1-mL droplets of dilution media: PBSs + 0.2 M sucrose, PBSs + 0.1 M sucrose, and culture medium + serum supplement. Prepare a water bath at 30°C.
-
8.
Using protective equipment, transfer the chosen straws into a flask of liquid nitrogen from the storage facility. In the laboratory, warm each straw by holding in air for 30 s then transfer the straw into the water bath at 30°C until all visible ice melts.
-
9.
Expel the embryos plus freezing medium into the droplet of PBSs + 0.2 M sucrose (see Note 11 ), and hold them at room temperature for 5 min. Then move the embryos into the droplet of PBSs + 0.1 M sucrose, and again hold at room temperature for 5 min.
-
10.
Move the embryos into tissue culture medium + serum at room temperature and hold for a further 10 min. Finally, the embryos can be transferred into the chosen tissue culture medium at 37°C for subsequent culture.
3.2 Cryopreservation of Blastocysts by Controlled-Rate Cooling
In centers where culture of embryos to the blastocyst stage is the method of choice, cryopreservation can be achieved based on a slow cooling method using glycerol as cryoprotectant. The described method is based on those previously reported by Menezo (19) and Tucker (24) using day 5/6 embryos at blastocyst or hatching blastocyst stages. Cryovials are often used in the process, but straws can also be used.
-
1.
Prepare droplets of medium (usually modified HTF medium plus 10% [v/v] human serum albumin [HAS]: HTF-HSA, HTF-HSA + 5% (w/v) glycerol, and HTF + HSA + 10% (w/v) glycerol + 0.2 M sucrose. Fill a Dewar flask with some liquid nitrogen.
-
2.
Transfer the blastocysts into HTF-HSA for 2 min at room temperature, then move them into the droplet of HTF-HSA + 5% (w/v) glycerol, and hold for 10 min at room temperature.
-
3.
Move the blastocysts into the droplet of HTF-HSA +10% (w/v) glycerol + 0.2 M sucrose at room temperature for a further 10 min.
-
4.
Transfer embryos into 0.3 mL of HTF-HSA +10% glycerol + 0.2 M sucrose in standard (1.2 mL) cryovials at room temperature.
-
5.
Transfer the vials to the cooling machine and cool at −2°C/min to −7°C, and hold for 5 min.
-
6.
Initiate ice formation or “seeding” by clamping the sides of the cryovial with forceps cooled in liquid nitrogen, then return the cryovials to the chamber of the machine at −7°C and hold for 10 min.
-
7.
Initiate the slow cooling phase at a rate of −0.3°C/min to −38°C. Using suitable protective equipment, transfer the cryovials into the flask of liquid nitrogen. Take the vials to the liquid nitrogen storage facility for long-term banking.
-
8.
When the embryos are required, set a water bath at 30°C in the laboratory and prepare dishes with 1-mL droplets of dilution media at room temperature: HTF-HSA + 10% (w/v) glycerol + 0.4 M sucrose, HTF-HSA + 5% (w/v) glycerol + 0.4 M sucrose, HTF-HSA + 2.5% (w/v) glycerol + 0.4 M sucrose, HTF-HSA + 0.4 M sucrose, HTF-HSA + 0.2 M sucrose, HTF-HSA + 0.1 M sucrose, and HTF-HSA. Set the warming stage to 37°C.
-
9.
Remove the cryovials from the storage facility wearing protective equipment, and place in a flask of liquid nitrogen for transport to the laboratory.
-
10.
Hold cryovials in air for 1 min, then transfer to a water bath until all visible ice melts.
-
11.
Expel embryos into the droplet of HTF-HSA + 10% (w/v) glycerol + 0.4 M sucrose at room temperature and locate them (about 30 s).
-
12.
Transfer the embryos into HTF-HSA + 5% (w/v) glycerol + 0.4 M sucrose at room temperature and hold them for 3 min.
-
13.
Transfer to HTF-HSA + 2.5% (w/v) glycerol + 0.4 M sucrose at room temperature for 3 min.
-
14.
Transfer to HTF-HSA + 0.4 M sucrose at room temperature for 2 min.
-
15.
Transfer to HTF-HSA + 0.2 M sucrose at room temperature for 2 min.
-
16.
Transfer to HTF-HSA + 0.1 M sucrose at room temperature, and move to the warm stage (37°C).
-
17.
Wash in standard tissue culture medium alone (three washes at 37°C), then move the embryos into standard culture conditions before embryo transfer.
-
18.
In cases where large numbers of animal embryos have been cryopreserved, it is possible to simplify the washing steps (accepting a possible slight reduction in overall recovery as a balance for convenience when handling more embryos) as:
-
a.
Expel thawed embryos into medium (serum supplemented) + 0.5 M sucrose for 10 min at room temperature.
-
b.
Transfer into medium (serum supplemented) + 0.2 M sucrose at room temperature for 10 min.
-
c.
Transfer into medium alone (serum supplemented), and move to the warm stage. Wash (three times in medium at 37°C) and move to standard culture conditions.
-
a.
3.3 Vitrification of Murine Morulae and Early Blastocysts
There has been a rapid expansion of different methods for embryo vitrification over the past few years employing a variety of CPA mixtures and receptacles to achieve very rapid cooling rates. Many of these approaches require considerable operator skill and experience. We describe here one of the earliest methods for embryo vitrification described by Scheffen et al. (25). This method has the advantages that the CPA mixture is relatively nontoxic (mouse morulae and early blastocysts can tolerate vitrifiable concentrations for 10 min at room temperature), and cooling can be achieved in traditional 0.25-mL straws. The sample loading can be achieved in a simple way to facilitate rapid dilution upon thawing (see Note 12 ). In the recent past, several other new container systems have been developed for embryo vitrification (see Note 2 ). The Scheffen method has also been reproduced in other laboratories ([26]; see Note 13 ). It should be seen as one method to train new users in embryo vitrification who could then go on to tackle more exacting techniques.
-
1.
Mouse embryos recovered on day 4 of pregnancy (d 1 = presence of vaginal plug) and classified as (1) compacted morulae, (2) early blastocyst, and (3) expanded blastocyst. The method is most successful for categories 1 and 2.
-
2.
Prepare culture dishes with droplets of PBSs Massip equilibration mixture (MEM 500-µL volume): also prepare 10% (w/v) glycerol + 20% (w/v) 1,2-propanediol in PBSs at room temperature, and a batch of PBSs + 1 M sucrose as Diluent to load straws, and another dish on ice at 4°C with droplets of Massip vitrification medium (MVM) (25% [w/v] glycerol + 25% [w/v] 1,2-propanediol in PBSs).
-
3.
Rinsed 0.25-mL straws with MVM at 4°C then loaded columns with 100 µL 1 M sucrose in PBSs (Diluent) solution as described in the original method by syringe at this stage: sealing powder to seal one end, followed by (see Subheading 3.1. step 6) and held at 4°C. Fill a Dewar flask with liquid nitrogen (wearing appropriate safety equipment).
-
4.
Embryos are washed in the droplet of PBSs and then transferred to the 500-µL droplet of MEM and held for 10 min at room temperature.
-
5.
Embryos are next transferred to the droplet of MVM at 4°C for 30 s then loaded into a 20-µL droplet of MVM in straw. This is done (as described in the original method) by loading (1) 100 µL 1 M sucrose in PBSs (Diluent; already loaded), (2) an air bubble, (3) the embryos in 20 µL of MVM, (4) an air bubble, and (5) Diluent to the plug. The Diluent columns do not vitrify (see Note 14 ).
-
6.
The straws are sealed with the plug (see Note 5 ), held for 30 s in the vapor just above the surface of liquid nitrogen (wearing appropriate safety equipment) in the Dewar flask (to prevent straw fracture from extremely fast cooling), and then plunged into liquid nitrogen. A simple method for holding in the vapor can be devised from a plastic “hook” (see Note 15 ). Transfer to the liquid nitrogen storage facility.
-
7.
When required after storage, wearing appropriate safety equipment, the straws are transferred to a flask of liquid nitrogen and taken to the laboratory. Prepare a water bath at 20°C. Prepare dishes with droplets (1 mL) of Diluent and fresh PBSs at room temperature. The straws are removed from liquid nitrogen, held in air for 10 s, and then warmed in a 20°C water bath until the ice melts (approx 20 s). The contents of the straws are then expelled into Diluent (see Note 12 ; see also Chapter 22, Subheading 3.2. ) and held at room temperature for 5 min.
-
8.
The embryos are then washed three times in droplets of fresh PBSs at room temperature and transferred to the chosen culture medium at 37°C.
4 Notes
Some of the information in this section has been repeated from Chapter 22 for the reader’s convenience.
-
1.
Staff should familiarize themselves with the safety equipment and the procedures for handling liquid nitrogen. The cryogen is generally safe and easy to handle, but avoid direct handling of metal objects cooled in liquid nitrogen (e.g., metal lids of storage containers) or freeze-burns can be experienced. Treat Dewar flasks with care (they are most often constructed of mirrored glass inner sections, evacuated by vacuum, and dropping heavy objects into the chamber or the knocking the flasks themselves, can crack the glass and cause an explosion as the vacuum is lost).
-
2.
Vitrification using some of the small sample holders (such as open-pulled straws) can result in direct exposure to liquid nitrogen. In addition to problems of security for the cryopreserved samples inside the pulled straws, it is important to remember in clinical practice that interpatient infection of equipment such as cooling tanks may be possible, and to consider equipment sterilization between usage. Some commercially available vitrification chambers have been designed with this in mind (e.g., vitset from http://www.minitube.de). New techniques for sealing open-pulled straws are under development (27), but will need validation before general acceptance.
-
3.
It should be noted that straws allow rapid heat transfer and hence are susceptible to temperature change during handling, for example on transfer from the cooling machine to liquid nitrogen for storage and during handling for identification purposes prior to thawing. Auditing of cryopreserved samples should only be performed after careful consideration of the risks of warming the samples. Both liquid nitrogen and liquid nitrogen vapor should be considered to contain pathogens. Straws that are not intact should be discarded. Care should be taken to prevent the bending of straws, which may lead to cracks and entry of contaminants from the liquid nitrogen, as well as a risk of explosion on warming as liquid nitrogen within the vessel expands. If storing in the vapor phase, the level of liquid nitrogen should be carefully monitored to ensure stability of storage temperature. Alarms and automatic filling systems are available, but it is recommended that the level of liquid nitrogen still be checked manually at regular intervals.
-
4.
Straws are convenient receptacles for use during embryo cryopreservation and have good heat transfer properties. They do, however, need consideration in handling and storage (e.g., stored away from extreme heat or light sources) before use, as the plastic can “age” and increase the incidence of cracking on exposure to extreme temperature change in the cryopreservation protocol. The practice of allowing a short period of rewarming in air before transfer to warm water helps prevent fracture of the straws from temperature stress. Cryotubes are more resilient but their size and volume restrict the rate of heat transfer, especially if very rapid heat transfer is required.
-
5.
The straw can be filled using a small syringe and needle. Pushing the cotton plug along the straw will reduce the capacity of the straw (see Chapter 22; Fig. 2). The plug should be wetted as this will help prevent liquid nitrogen entry. If the plug is wetted by insertion of a sizeable column of the primary thawing/dilution solution, then expulsion of this solution along with the oocytes following thawing will aid dilution of the cryoprotectant. An air gap should be left between this section and the column containing the embryos—a 1-cm column of 1.5 M PrOH plus 0.2 M sucrose. Straws should be clearly labeled, with an appropriate marker, i.e., one that will not smudge or be erased during storage. Straws can also be closed by heat sealing. In this case, having a “sandwich” arrangement of: Diluent-air gap-CPA medium-air gap-CPA medium plus embryos-air gap-CPA medium can be advantageous as it protects the embryo compartment from excessive heating during sealing (see Chapter 22; Fig. 2).
-
6.
Cryopreservation by slow cooling with freezing machines permits the recording of events such as cooling rate to be recorded directly, which may be important for clinical practice where record keeping in infertility treatment is important to ensure validation of practices. Vitrification protocols may appear more simple but are difficult to oversee on a day-to-day basis, and good continuous supervision is necessary to eliminate small changes introduced unwittingly into the multiple embryo handling steps by individual technologists.
-
7.
In clinical practice (and in some veterinary or biotechnological applications), the optimally developed cohort of embryos from the initial embryo collection or in vitro fertilization procedure may be selected for immediate transfer to recipients. This leaves a pool of lower grade embryos available for banking by cryopreservation. Inevitably, recovery rates from this second-grade pool of embryos may be lower than would be expected if all the starting embryos were of high grade, and this needs to be recognized as a limiting factor on the success of embryo cryobanking.
-
8.
Some studies have claimed that embryos at the exponential stage of development (e.g., 2, 4, 8 cells) may be more resistant to cryodamage during low-temperature banking than embryos cooled when at intermediate developmental stages (3, 5, 7 cells). This probably results from all the blastomeres being in interphase with chromosome completely confined within the nuclear membrane, thus avoiding potential abnormalities.
-
9.
Seeding is in the initiation of ice nucleation. This can be achieved automatically in some freezing machines, or can be initiated manually by removing the straws from the machine and touching the solution with forceps that have been precooled in liquid nitrogen.
-
10.
It is beyond the scope of the current chapter, but in all cryopreservation protocols, good management of the storage banks requires clear and unequivocal labeling and tracking of repositories, as well as safe methods for filling and sealing straws. This is particularly important in the clinical setting. Comprehensive ranges of technology to achieve these ends are commercially available (e.g., see http://www.cryobiosystem.com and http://www.planer.co.uk). Different methods for labeling straws, such as bar coding, colored insertable plugs, or colored sleeves with imprinted numerical ID can be selected. Another point of growing significance is the use of heat sealing of ionomeric resin straws to ensure security of samples against contamination from liquid nitrogen, and reliable filling and sealing equipment is now produced (http://www.cryobiosystem.com). To further ensure security, use of an outer, slightly larger, security straw can be used and heat sealed in a similar fashion. The presence of the second straw does not alter cooling profiles significantly during slow cooling techniques. This will also be of importance when considering rapid cooling or vitrification techniques (see Note 2 ) and has been termed the “straw-instraw” technique (28). Storage in the vapor phase above liquid nitrogen can reduce the risk of any cross-infection and is the method of choice in many clinical centers. A new generation of liquid nitrogen tanks is being developed to facilitate the best practice for vapor storage, and automatic filling systems may be provided for large-scale operations (see http://www.thamescryogenic.com). It is also recommended that the outer surfaces of straws and vials be decontaminated by wiping with active agents after filling (before cooling), and after warming (especially using a water bath) before expelling the embryos ([29]; see also Chapter 22), not only in clinical laboratories but as good practice when cryopreserving any embryos.
-
11.
The straw contents can be expelled by inserting a 1-mL syringe containing at least 0.5 mL of primary thawing/dilution solution and expelling the contents of both the straw and syringe into a dish.
-
12.
In vitrification using the Massip method, a straightforward way to load and expel embryos after thawing is to make the following steps. The 0.25-mL straws are plugged with the cotton/polyvinyl alcohol plug, which is sealed on wetting by carefully injecting a 4-cm long column with 1 M sucrose. Diluent into the straw from a 1-mL syringe (Kendall Tyco, Gosport, UK) with a 0.5 × 16-mm needle. Care is taken to avoid wetting the sides of the straw. An air gap of 0.5 cm is left, and then 0.5 mL of MVM is injected into the column and the straws are placed on ice. The equilibrated embryos are injected into the MVM column in the straw, and the straw is sealed with a wetted plastic plug. After the thawing step, the plastic plug is removed and the straw cut through in the mid region of the sucrose column, followed by flushing out the embryos in MVM using fresh 1 M sucrose (1 mL) Diluent from a syringe into the centre well of an organ culture dish. The embryos are then held at room temperature for 5 min before washing in PBSs as described previously (see Chapter 22, Subheading 3.2. , step 6).
-
13.
Survival rates of compacted murine morulae using the Massip vitrification method are typically between 60 and 80% (25,26) and normal offspring have been born after embryo transfer (25).
-
14.
It is worth noting that the PBSs + 1 M sucrose Diluent does not vitrify even on rapid cooling, but rather freezes, giving a “milky” visual appearance to the straw during cooling. It is possible to omit the Diluent from the straw, place only a column of MVM holding the embryos in the straw, and then expel the thawed embryos into a large droplet of fresh Diluent in a dish.
-
15.
A piece of plastic that can be inserted into a straw and is approximately twice the length of a straw is ideal. The plastic is inserted into the end of the straw and then bent through 90°. The straw can then be placed close to the nitrogen in the horizontal position and the holder can be held by hand at a safe distance from the nitrogen.
-
16.
Vitrification using some of the small sample holders (such as open pulled straws) can result in direct exposure to liquid nitrogen. In addition to problems of security for the cryopreserved samples inside the pulled straws, it is important to remember in clinical practice that interpatient infection of equipment such as cooling tanks may be possible, and to consider equipment sterilization between usage. Some commercially available vitrification chambers have been designed with this in mind (e.g,. vitset from http://www.minitube.de). New techniques for sealing open pulled straws are under development (29), but will need validation before general acceptance.
References
Hammond, J., Jr. (1949) Recovery and culture of tubal mouse ova. Nature 163, 28–39.
McLarren, A. and Biggers, J. D. (1958) Successful development and birth of mice cultivated in vitro as early embryos. Nature 182, 877–888.
Steptoe, P. C., Edwards, R. G., and Purdy, J. M. (1971) Human blastocysts grown in culture. Nature 229, 132–133.
Brackett, B. G., Bousquet, D., Boice, M. L., Donawick, W. J., Evans, J. E, and Dressel, M. A. (1982) Normal development following in vitro fertilization in the cow. Biol. Reprod. 27, 147–158.
Massip, A., Leibo, S. P., and Blesbois, E. (2004) Cryobiology of gametes and the breeding of domestic animals. In: Life in the Frozen State, (Fuller, B. J., Lane, N., and Benson E. E., eds.), CRC Press, Boca Raton, FL, pp. 371–392.
Shaw, J. and Nakagata, H. (2002) Cryopreservation of transgenic mouse lines. Methods Mol. Biol. 180, 207–228.
Gerris, J., De Neubourg, D., De Sutter, P., Van Royen, E., Mangelschots, K., and Vercruyssen, M. (2003) Cryopreservation as a tool to reduce multiple birth. Reprod. Biomed. Online 7, 286–294.
Whittingham, D. G., Leibo, S. P., and Mazur, P. (1972) Survival of mouse embryos frozen to −196°C and −269°C. Science 178, 411–414.
Wilmut, I. (1972) The effect of cooling rate, warming rate, cryoprotective agent and stage of development on survival of mouse embryos during freezing and thawing. Life Sci. 11, 1071–1079.
Leibo, S. P., Mazur, P., and Jackowski, S. (1974) Factors affecting survival of mouse embryos during freezing and thawing. Exp. Cell Res. 89, 79–88.
Mazur, P. (1970) Cryobiology; the freezing of biological systems. Science 168, 939–949.
Rall, W. F. (1987) Factors affecting the survival of mouse embryos cryopreserved by vitrification. Cryobiology 24, 387–402.
Luyet, B. J. and Gehenio, P. M. (1940) Life and Death at Low Temperatures. Biodynamica, Normandy, MO.
Rall, W. F. and Fahy, G. (1985) Ice-free cryopreservation of mouse embryos at −196°C by vitrification. Nature 313, 573–575.
Lane, M., Bavister, B., Lyons, E., and Forest, K. (1999) Containerless vitrification of mammalian oocytes and embryos. Nature Biotechnol. 17, 1234–1236.
Fuller, B. and Paynter, S. (2004) Fundamentals of cryobiology in reproductive medicine. Reprod. Biomed. Online 9, 680–691.
Kasai, M. and Mukada, T. (2004) Cryopreservation of animal and human embryos by vitrification. Reprod. Biomed. Online 9, 164–170.
Tominaga, K. (2004) Cryopreservation and sexing of in vivo and in vivo- produced bovine embryos for their practical use. J. Repro. Dev. 50, 29–38.
Menezo, Y. J. (2003) Blastocyst freezing. Eur. J. Obstet. Gynecol. Reprod. Biol. 115, S2–S5.
Shaw, J. and Nakagata, N. (2002) Cryopreservation of transgenic mouse lines. Methods Mol. Biol. 180, 207–228.
Dobrinsky, J. R. (2001) Cryopreservation of pig embryos: adaptation of vitrification technology for embryo transfer. Reprod. Suppl. 58, 325–333.
Landel, C. (2005) Archiving mouse strains by cryopreservation. Lab. Animal 34, 50–57.
Byrd, W. (2002) Cryopreservation, thawing and transfer of human embryos. Seminars Reprod. Med. 20, 37–43.
Tucker, M. J., Morton, P., Sweitzer, C., and Wright, G. (1995) Cryopreservation of human embryos and oocytes. Curr. Opin. Obstet. Gynecol. 7, 188–192.
Scheffen, B., Van der Zwalen, P., and Massip, A. (1986) A simple and efficient procedure for preservation of mouse embryos by vitrification. CryoLetters 7, 260–269.
Cseh, S., Horlacher, W., Brem, G., et al. (1999) Vitrification of mouse embryos in two cryoprotectant solutions. Theriogenology 52, 103–111.
Isachenko, V., Montag, M., Isachenko, E., et al. (2005) Aseptic technology of vitrification of human pronuclear oocytes using open pulled straws. Hum. Reprod. 20, 492–496.
Kuleshova, L. and Shaw, J. M. (2000) A strategy for rapid cooling of mouse embryos within a double straw to eliminate the risk of contamination during storage in liquid nitrogen. Hum. Reprod. 15, 2604–2609.
Mortimer, D. (2004) Current concepts and practices in human sperm cryopreservation. Reprod. Biomed. Online 9, 134–151.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2007 Humana Press Inc., Totowa, NJ
About this protocol
Cite this protocol
Fuller, B.J., Paynter, S.J. (2007). Cryopreservation of Mammalian Embryos. In: Day, J.G., Stacey, G.N. (eds) Cryopreservation and Freeze-Drying Protocols. Methods in Molecular Biology™, vol 368. Humana Press. https://doi.org/10.1007/978-1-59745-362-2_23
Download citation
DOI: https://doi.org/10.1007/978-1-59745-362-2_23
Publisher Name: Humana Press
Print ISBN: 978-1-58829-377-0
Online ISBN: 978-1-59745-362-2
eBook Packages: Springer Protocols