
Abstract
Background
Germline mutations in the genes BRCA1 and BRCA2 account for only a proportion of hereditary breast cancer, suggesting that additional genes contribute to hereditary breast cancer. Recently a heterozygous variant in the ataxia–telangiectasia mutated (ATM) gene, IVS10-6T→G, was reported by an Australian multiple-case breast cancer family cohort study (the Kathleen Cuningham Foundation Consortium for Research into Familial Breast Cancer) to confer a substantial breast cancer risk. Although this variant can result in a truncated ATM product, its clinical significance as a high-penetrance breast cancer allele or its role as a low-penetrance risk-modifier is controversial.
Methods
We determined the frequency of ATM IVS10-6T→G variants in a cohort of individuals affected by breast and/or ovarian cancer who underwent BRCA1 and BRCA2 genetic testing at four major Australian familial cancer clinics.
Results
Seven of 495 patients (1.4%) were heterozygous for the IVS10-6T→G variant; the carrier rate in unselected Australian women with no family history of breast cancer is reported to be 6 of 725 (0.83%) (P = 0.4). Two of the seven probands also harboured a pathogenic BRCA1 mutation and one patient had a BRCA1 unclassified variant of uncertain significance.
Conclusion
These findings indicate that the ATM IVS10-6T→G variant does not seem to occur at a significantly higher frequency in affected individuals from high-risk families than in the general population. A role for this variant as a low-penetrance allele or as a modifying gene in association with other genes (such as BRCA1) remains possible. Routine testing for ATM IVS10-6T→G is not warranted in mutation screening of affected individuals from high-risk families.
Similar content being viewed by others

Introduction
Germline mutations in the two major breast cancer susceptibility genes, BRCA1 and BRCA2 (MIM113705 and 600185), are frequently found in families containing multiple individuals affected by breast and ovarian cancer [1]. However, BRCA1 and BRCA2 mutations are only identified in about 15–20% of multiple-case families affected by breast cancer alone [1, 2]. Other breast cancer-predisposing genes might account for a proportion of the remaining cases.
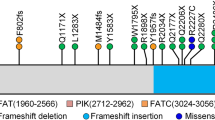
The ATM (ataxia–telangiectasia mutated) gene (MIM 208900, 607585), whose product has a central role in DNA repair after damage induced by ionising radiation [3, 4] and phosphorylates BRCA1 [5, 6], has been proposed as one such candidate breast cancer-predisposing gene. Individuals harbouring homozygous (or compound heterozygous) deleterious mutations in the ATM gene develop ataxia–telangiectasia (A–T), which is characterised by progressive cerebellar degeneration, telangiectasia, immunodeficiency, extreme sensitivity to ionising radiation and a predisposition to lymphoid malignancies [7]. Most pathogenic ATM mutations described so far (now in excess of 300) result in truncating mutations that produce little or no detectable ATM protein, but pathogenic missense mutations have also been described. About 1% of the population are asymptomatic heterozygous carriers. However, because the ATM protein forms high-molecular-mass complexes, it is conceivable that heterozygous missense mutations (or certain truncating mutations) could have a dominant-negative effect, interfering with the function of the normal allele and thereby resulting in an increased predisposition to cancer [8].
Clinical observation and epidemiological studies since the 1970s have shown that blood relatives of A–T patients seem to be at increased risk for breast cancer, suggesting that heterozygosity for mutations in the ATM gene might predispose to breast cancer [9, 10]. After the identification of the gene in 1995 [7], several studies demonstrated an association between ATM heterozygosity and increased risk for breast cancer [11–15]. However, other studies have failed to demonstrate an association [16–18], concluding that the contribution of ATM heterozygosity to familial breast cancer is minimal. It is difficult to reconcile the different outcomes of these studies because they differed in sample size, in subject selection criteria, and in the mutation detection methods used.
A recent study of multiple-case breast cancer families in Australia suggested that two ATM variants, ATM 7271T→G and IVS10-6T→G, confer a substantial risk for breast cancer in families with multiple cases [19]. The ATM 7271T→G missense variant was subsequently not detected in two large independent cohorts of breast cancer families [20, 21], indicating that the variant is of limited clinical significance. The ATM IVS10-6T→G variant leads to incorrect splicing at exon 11 and results in a truncated ATM product [22]. In the Australian study, this variant was detected in 2 of 76 (2.6%) breast cancer patients with a strong family history of breast cancer, 0 of 268 breast cancer patients without a family history of the disease, and 0 of 68 women with no personal or family history of breast cancer [19]. In the two families with this variant, the penetrance (in terms of breast cancer risk) was estimated to be 78% (95% confidence interval 36–99%) by 70 years of age. An earlier study had also demonstrated an association between this variant and breast cancer risk [22]. However, three subsequent studies in North America and Europe failed to identify a significant role for this variant in hereditary or sporadic breast cancer [20, 21, 23]. Nevertheless, it has been argued that the ATM IVS10-6T→G allele represents a biologically and clinically significant variant because ATM kinase activity is reduced to 25–40% in heterozygous cells [19].
The possibility that ATM IVS10-6T→G could be a high-penetrance breast cancer susceptibility allele, or even a low-penetrance risk-modifying allele, has major ramifications for genetic testing and clinical management of individuals with a hereditary predisposition to breast and ovarian cancer. Because the association had been made in a cohort of (ethnically diverse) multiple-case Australian families, we determined the frequency and relevance of this variant in an independent series of families from Australian familial cancer clinics. We compared the frequency of the ATM IVS10-6T→G variant in affected individuals undergoing genetic testing for BRCA1 and BRCA2 at four major Australian familial cancer clinics with the carrier rate in Australian women without a family history of breast cancer.
Materials and methods
Samples
Patients who had been affected by either breast and/or ovarian cancer and were index cases within a family that had initiated BRCA1 and BRCA2 mutation detection were ascertained from four Australian familial cancer clinics: Genetic Health Services Victoria (GHSV), Melbourne, the Royal Melbourne Hospital (RMH), Melbourne, the South Australian Familial Cancer Service (SAFCS), Adelaide, and Westmead Hospital (WH), Sydney. For GHSV and RMH, the series included peripheral blood leucocyte genomic DNA samples collected between July 1999 and June 2003 (inclusive), for which retrospective patient (or next of kin) consent was obtained [48 of 59 (81%) and 85 of 97 (88%), respectively]. For SAFCS and WH, a consecutive series from probands, for whom testing at that stage had not detected a BRCA1 or BRCA2 mutation, was screened for the ATM IVS10-6T→G variant (201 and 130 samples, respectively). Testing was subsequently extended at WH to include BRCA1 affected mutation carriers (31 samples). Approval to conduct ATM testing was obtained from each relevant institutional ethics committee, unless the standard clinical genetic testing consent form covered such testing.
Affected women's families were categorised as being at potentially high, moderate or average risk for developing breast cancer on the basis of family history, according to the National Health and Medical Research Council (Australia) guidelines [24], as follows.
Potentially high risk was defined as the presence of at least two first-degree or second-degree relatives on one side of a family diagnosed with breast or ovarian cancer (including the patient) plus at least one of the following high-risk features: additional relative(s) with breast or ovarian cancer, breast cancer diagnosed before the age of 40 years, ovarian cancer diagnosed before the age of 50 years, bilateral breast cancer, breast and ovarian cancer in the same woman, Jewish ancestry, or breast cancer in a male relative.
Moderate risk was defined as one or two first-degree relatives diagnosed with breast cancer (including the patient) before the age of 50 years, two first-degree or second-degree relatives on the same side of the family with breast or ovarian cancer, or one first-degree relative with ovarian cancer before the age of 50 years (in all cases without additional high-risk features). Standard risk was defined as the affected woman falling outside either of the other two risk categories.
Mutation screening
Samples were screened for the ATM IVS10-6T→G variant essentially as described previously [19]. Briefly, a 193-base-pair fragment spanning the IVS10-6 region was amplified from genomic DNA by polymerase chain reaction with the primers 5'-ACAGCGAAACTCTGGCTCAAA-3' and 5'-TGATCTTTTATTACTTCCCAGCCTAGT-3'. Because the T→G variant creates a novel RsaI restriction site, heterozygous carriers were detected by RsaI restriction digest, which produces 58-base-pair and 135-base-pair variant-specific fragments in addition to the wild-type 193-base-pair fragment. Fragments were separated and detected on either a 12% SDS-polyacrylamide gel or a 1.5% agarose gel. Alternatively, the restriction fragments were separated by denaturing high-performance liquid chromatography (details available from the authors on request). A positive control genomic sample was kindly provided by Dr G Chenevix-Trench (Queensland Institute of Medical Research, Brisbane, Australia). For sequencing, independently amplified polymerase chain reaction products were generated and confirmed by automated sequencing with the ABI Prism BigDye Terminator Cycle Sequencing Kit (Perkin Elmer).
Statistical analysis
Two-tailed P values were generated with Fisher's Exact Test. In accordance with convention, P < 0.05 was considered significant.
Results and discussion
To investigate the frequency of the ATM IVS10-6T→G variant in patients at high probability of carrying a gene predisposing them to breast cancer, we ascertained 495 patients who had attended one of four familial cancer clinics located in three Australian States. These patients had been affected by either breast or ovarian cancer and had undergone genetic testing for BRCA1 and BRCA2 mutations. In most cases (90.7%), the family was classified as 'potentially high risk' for breast and/or ovarian cancer predisposition [24]. A small proportion (7.5%) were categorised as being in the moderate risk group, although these generally exhibited unusual features (such as breast and ovarian cancer in a single individual in the absence of a family history), and insufficient information on risk was available for the remaining 1.8%. The proportion of families in the different risk categories was similar at the four centres (Table 1; data not shown). For patients from GHSV, RMH and WH, the average age of breast cancer diagnosis of the proband was 45 years (range 22–78) and an average of 3.4 breast cancers and 0.42 ovarian cancers were documented per family. Of the potentially high-risk kindreds, the majority (71%) of families contained breast-only cancer cases, whereas breast and ovarian cancers were noted in the remaining families. For SAFCS families, the average age of breast cancer diagnosis for the proband was 48 years, and an average of 3.2 breast cancers and 0.25 ovarian cancers were documented per family. The mean predictions for GHSV and RMH patients carrying a BRCA1 or BRCA2 mutation were 0.22 and 0.19, respectively, as determined by either the BRCAPRO or the MYRIAD II statistical model [25].
We screened probands from non-BRCA1/BRCA2 families in whom no mutation had been identified at the time (n = 464) and probands with known BRCA1 mutations (WH cohort, n = 31). Of the 495 probands screened, 7 (1.4%) were found to be heterozygous for the ATM IVS10-6T→G variant. Four of these were ascertained through SAFCS and one from each of the other centres (Table 2). None of these ATM heterozygotes had been reported in the study by Chenevix-Trench and colleagues [19]. Their age at diagnosis, family histories and family risk status were quite diverse (Table 3). Their mean age at first cancer diagnosis was 53 years (range 35–62). None had a history of prior radiation exposure. Three of the seven individuals had a family history of breast/ovarian cancer, one a family history of breast/thyroid cancer, and the remaining three families had a history of breast cancer alone. Three heterozygous individuals were from moderate-risk families. No heterozygous carriers had clinical features attributable to A–T such as ataxia, telangiectasia or immunodeficiency.
BRCA1 and BRCA2 genetic testing results were subsequently available for all seven individuals. Two were found to harbour pathogenic truncating mutations in BRCA1 (both from families with a history of breast/ovarian cancer), and one a BRCA1 variant of uncertain significance (from a moderate-risk family). For both BRCA1 and ATM IVS10-6T→G carriers (probands 1 and 7 in Table 3), the histopathological features of the primary breast and ovarian cancers were consistent with the phenotype associated with BRCA1 tumours [26, 27]. The breast cancer from proband 1 was a grade III oestrogen receptor-negative and progesterone receptor-negative infiltrating ductal carcinoma with lymphocytic infiltrate and pushing margins. The ovarian cancer from proband 7 was a high-grade serous carcinoma with marked nuclear pleomorphism, together with a large cyst containing a serous cystadenoma and smaller cysts containing borderline malignancy. There were no remarkable histopathological features in the tumours from the other five cases, including proband 4 (with the BRCA1 unclassified variant). Thus, the ATM IVS10-6T→G allele was not apparently associated with a distinct tumour phenotype.
The frequency (1.4%) of the ATM IVS10-6T→G variant is somewhat greater than the reported frequency of 6 of 725 (0.8%) for a cohort of Australian women ascertained without a personal or family history of breast cancer [28]; however, this difference is not significantly different (P = 0.4). This frequency is also similar to control cases reported in Dutch, German and Austrian populations [21, 22, 29, 30], and a recent study in the USA [23], although minor differences might be due to population heterogeneity (Table 4). These results are consistent with the observation that the ATM IVS10-6T→G variant is an ancient mutation that might be widely distributed across Europe, the Middle East and western Asia [30]. In the study by Chenevix-Trench and colleagues, analysis was performed on non-BRCA1/BRCA2 cases containing more than three breast cancers per family, and families with male breast cancer(s) were excluded [19]. By restricting the analysis of our samples (GHSV, RMH, WH) to those with more than three breast or ovarian cancers within a family and no cases of male breast cancer, the frequency was 2 of 197 (1.0%), but both cases also carried pathogenic BRCA1 mutations. The basis for the increased frequency reported for kindreds in the Kathleen Cuningham Foundation Consortium for Research into Familial Breast Cancer is unclear, although a subsequent report now suggests a lower frequency at 6 of 385 (1.6%) [28].
It was not feasible to evaluate the co-segregation of the ATM IVS10-6T→G allele with the breast or ovarian cancers in each kindred in our cohort. In the two ATM IVS10-6T→G families reported by Chenevix-Trench and colleagues, carriers had an estimated disease penetrance of 78% (confidence interval 36–99%) to age 70 years, equivalent to a 26-fold increased risk [19]. However, it is noteworthy that the LOD (logarithm of odds) score of 1.18 for linkage with ATM fell well short of standard criteria for significance.
A recent study by Szabo and colleagues evaluated five ATM IVS10-6T→G families with non-BRCA1/BRCA2 breast cancer and concluded that the variant did not confer an increase in risk for breast cancer. That study also did not observe an increase in the frequency of the ATM IVS10-6T→G variant among BRCA1/BRCA2-positive families (0.5%) [21]. In our study, two of the seven ATM IVS10-6T→G heterozygotes harboured pathogenic BRCA1 mutations and a further proband carried a BRCA1 unclassified variant. This possible association is intriguing because ATM is known to phosphorylate BRCA1 [5, 6], and BRCA1 has recently been shown to be required for certain ATM functions, including the phosphorylation of substrates such as p53 and Chk2 that influence cell cycle arrest and apoptosis after DNA damage [31]. Further investigation of this variant as a low-penetrance modifier allele might be warranted.
In contrast, it has been argued that ATM IVS10-6T→G is a high-penetrance allele but our study has failed to support this view. Although this truncating variant has been postulated to act in a dominant-negative manner [19], the identification of a truncated product in heterozygotes has not been reported, suggesting that the product undergoes rapid degradation. It is known that the variant allele produces less than 10% of full-length ATM mRNA [29]; it therefore remains possible that heterozygous carriers simply display reduced ATM levels and that the residual ATM kinase activity is sufficient for maintaining normal cellular responses under most circumstances.
Conclusion
The frequency of the ATM IVS10-6T→G splice-site variant was similar in affected individuals from our clinic-based cases with a strong family history to that reported for individuals with no personal or family history of breast or ovarian cancer. Screening for the IVS10-6T→G variant in a familial cancer clinic setting is therefore unlikely to be of clinical significance. The relatively high prevalence of this variant among unaffected Europeans [30] further undermines its relevance in a clinical context. However, it remains plausible that the ATM IVS10-6T→G variant could function as a low-penetrance breast cancer risk-modifier under certain circumstances.
Abbreviations
- A–T:
-
ataxia–telangiectasia
- ATM :
-
ataxia–telangiectasia mutated
- GHSV:
-
Genetic Health Services Victoria
- RMH:
-
Royal Melbourne Hospital
- SAFCS:
-
South Australian Familial Cancer Service
- WH:
-
Westmead Hospital.
References
Ford D, Easton DF, Stratton M, Narod S, Goldgar D, Devilee P, Bishop DT, Weber B, Lenoir G, Chang-Claude J, Sobol H, Teare MD, Struewing J, Arason A, Scherneck S, Peto J, Rebbeck TR, Tonin P, Neuhausen S, Barkardottir R, Eyfjord J, Lynch H, Ponder BA, Gayther SA, Birch JM, Lindblom A, Stoppa-Lyonnet D, Bignon Y, Borg A, Hamann U, Haites N, Scott RJ, Maugard CM, Vasen H, Seitz S, Cannon-Albright LA, Schofield A, Zelada-Hedman M, the Breast Cancer Linkage Consortium: Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. The Breast Cancer Linkage Consortium. Am J Hum Genet. 1998, 62: 676-689. 10.1086/301749.
Antoniou AC, Pharoah PD, McMullan G, Day NE, Ponder BA, Easton D: Evidence for further breast cancer susceptibility genes in addition to BRCA1 and BRCA2 in a population-based study. Genet Epidemiol. 2001, 21: 1-18. 10.1002/gepi.1014.
Khanna KK, Jackson SP: DNA double-strand breaks: signaling, repair and the cancer connection. Nat Genet. 2001, 27: 247-254. 10.1038/85798.
Shiloh Y: ATM and related protein kinases: safeguarding genome integrity. Nat Rev Cancer. 2003, 3: 155-168. 10.1038/nrc1011.
Cortez D, Wang Y, Qin J, Elledge SJ: Requirement of ATM-dependent phosphorylation of brca1 in the DNA damage response to double-strand breaks. Science. 1999, 286: 1162-1166. 10.1126/science.286.5442.1162.
Gatei M, Scott SP, Filippovitch I, Soronika N, Lavin MF, Weber B, Khanna KK: Role for ATM in DNA damage-induced phosphorylation of BRCA1. Cancer Res. 2000, 60: 3299-3304.
Savitsky K, Bar-Shira A, Gilad S, Rotman G, Ziv Y, Vanagaite L, Tagle DA, Smith S, Uziel T, Sfez S, Ashkenazi M, Pecker I, Frydman M, Harnik R, Patanjali SR, Simmons A, Clines GA, Sartiel A, Gatti RA, Chessa L, Sanal O, Lavin MF, Jaspers NGJ, Taylor AMR, Arlett CF, Miki T, Weissman SM, Lovett M, Collins FS, Shiloh Y: A single ataxia telangiectasia gene with a product similar to PI-3 kinase. Science. 1995, 268: 1749-1753.
Gatti RA, Tward A, Concannon P: Cancer risk in ATM heterozygotes: a model of phenotypic and mechanistic differences between missense and truncating mutations. Mol Genet Metab. 1999, 68: 419-423. 10.1006/mgme.1999.2942.
Swift M, Reitnauer PJ, Morrell D, Chase CL: Breast and other cancers in families with ataxia-telangiectasia. N Engl J Med. 1987, 316: 1289-1294.
Swift M, Morrell D, Massey RB, Chase CL: Incidence of cancer in 161 families affected by ataxia-telangiectasia. N Engl J Med. 1991, 325: 1831-1836.
Athma P, Rappaport R, Swift M: Molecular genotyping shows that ataxia-telangiectasia heterozygotes are predisposed to breast cancer. Cancer Genet Cytogenet. 1996, 92: 130-134. 10.1016/S0165-4608(96)00328-7.
Inskip HM, Kinlen LJ, Taylor AM, Woods CG, Arlett CF: Risk of breast cancer and other cancers in heterozygotes for ataxia-telangiectasia. Br J Cancer. 1999, 79: 1304-1307. 10.1038/sj.bjc.6690209.
Janin N, Andrieu N, Ossian K, Lauge A, Croquette MF, Griscelli C, Debre M, Bressac-de-Paillerets B, Aurias A, Stoppa-Lyonnet D: Breast cancer risk in ataxia telangiectasia (AT) heterozygotes: haplotype study in French AT families. Br J Cancer. 1999, 80: 1042-1045. 10.1038/sj.bjc.6690460.
Geoffroy-Perez B, Janin N, Ossian K, Lauge A, Croquette MF, Griscelli C, Debre M, Bressac-de-Paillerets B, Aurias A, Stoppa-Lyonnet D, Andrieu N: Cancer risk in heterozygotes for ataxia-telangiectasia. Int J Cancer. 2001, 93: 288-293. 10.1002/ijc.1329.
Olsen JH, Hahnemann JM, Borresen-Dale AL, Brondum-Nielsen K, Hammarstrom L, Kleinerman R, Kaariainen H, Lonnqvist T, Sankila R, Seersholm N, Tretli S, Yuen J, Boice JD, Tucker M: Cancer in patients with ataxia-telangiectasia and in their relatives in the nordic countries. J Natl Cancer Inst. 2001, 93: 121-127. 10.1093/jnci/93.2.121.
Vorechovsky I, Rasio D, Luo L, Monaco C, Hammarstrom L, Webster AD, Zaloudik J, Barbanti-Brodani G, James M, Russo G: The ATM gene and susceptibility to breast cancer: analysis of 38 breast tumors reveals no evidence for mutation. Cancer Res. 1996, 56: 2726-2732.
FitzGerald MG, Bean JM, Hegde SR, Unsal H, MacDonald DJ, Harkin DP, Finkelstein DM, Isselbacher KJ, Haber DA: Heterozygous ATM mutations do not contribute to early onset of breast cancer. Nat Genet. 1997, 15: 307-310.
Chen J, Birkholtz GG, Lindblom P, Rubio C, Lindblom A: The role of ataxia-telangiectasia heterozygotes in familial breast cancer. Cancer Res. 1998, 58: 1376-1379.
Chenevix-Trench G, Spurdle AB, Gatei M, Kelly H, Marsh A, Chen X, Donn K, Cummings M, Nyholt D, Jenkins MA, Scott C, Pupo GM, Dörk T, Bendix R, Kirk J, Tucker K, McCredie MR, Hopper JL, Sambrook J, Mann GJ, Khanna KK: Dominant negative ATM mutations in breast cancer families. J Natl Cancer Inst. 2002, 94: 205-215. 10.1093/jnci/94.3.205.
Lei H, Pospisilova D, Lindblom A, Vorechovsky I: Re: Dominant negative ATM mutations in breast cancer families. J Natl Cancer Inst. 2002, 94: 951-952. 10.1093/jnci/94.12.951.
Szabo CI, Schutte M, Broeks A, Houwing-Duistermaat JJ, Thorstenson YR, Durocher F, Oldenburg RA, Wasielewski M, Odefrey F, Thompson D, Floore AN, Kraan J, Klijn JG, van den Ouweland AM, Wagner TM, Devilee P, Simard J, van't Veer LJ, Goldgar DE, Meijers-Heijboer H: Are ATM mutations 7271T→G and IVS10-6T→G really high-risk breast cancer-susceptibility alleles?. Cancer Res. 2004, 64: 840-843.
Broeks A, Urbanus JH, Floore AN, Dahler EC, Klijn JG, Rutgers EJ, Devilee P, Russell NS, van Leeuwen FE, van't Veer LJ: ATM-heterozygous germline mutations contribute to breast cancer-susceptibility. Am J Hum Genet. 2000, 66: 494-500. 10.1086/302746.
Bernstein JL, Bernstein L, Thompson WD, Lynch CF, Malone KE, Teitelbaum SL, Olsen JH, Anton-Culver H, Boice JD, Rosenstein BS, Borresen-Dale AL, Gatti RA, Concannon P, Haile RW: ATM variants 7271T>G and IVS10-6T>G among women with unilateral and bilateral breast cancer. Br J Cancer. 2003, 89: 1513-1516. 10.1038/sj.bjc.6601289.
National Health and Medical Research Council: Clinical Practice Guidelines. Familial aspects of cancer: a guide to clinical practice. 1999, Commonwealth of Australia, Canberra, [http://www.health.gov.au/nhmrc/publications/synopses/cp67syn.htm]
Berry DA, Iversen ES, Gudbjartsson DF, Hiller EH, Garber JE, Peshkin BN, Lerman C, Watson P, Lynch HT, Hilsenbeck SG, Rubinstein WS, Hughes KS, Parmigiani G: BRCAPRO validation, sensitivity of genetic testing of BRCA1/BRCA2, and prevalence of other breast cancer susceptibility genes. J Clin Oncol. 2002, 20: 2701-2712. 10.1200/JCO.2002.05.121.
Johannsson OT, Idvall I, Anderson C, Borg A, Barkardottir RB, Egilsson V, Olsson H: Tumour biological features of BRCA1-induced breast and ovarian cancer. Eur J Cancer. 1997, 33: 362-371.
Armes JE, Trute L, White D, Southey MC, Hammet F, Tesoriero A, Hutchins AM, Dite GS, McCredie MR, Giles GG, Hopper JL, Venter DJ: Distinct molecular pathogeneses of early-onset breast cancers in BRCA1 and BRCA2 mutation carriers: a population-based study. Cancer Res. 1999, 59: 2011-2017.
Chenevix-Trench G, Jenkins MA, Khanna KK, Spurdle AB, Marsh A, Chen X, Gatei M, Hobson K, Southey MC, Tesoriero AA, MacAulay P, Karpowicz J, Giles GG, McCredie MRE, Venter DJ, Mann G, Pupo G, Sambrook J, kConFab , Easton DF, Goldgar DE, Antoniou A, Thompson D, Hopper JL: Risk of breast cancer in female carriers of ATM IVS10-6T>G. In The Breast Cancer Linkage Consortium and the International Collaborative Group on Familial Breast and Ovarian Cancer 14th General Meeting: Madrid, Spain. 2003, 48-
Dörk T, Bendix R, Bremer M, Rades D, Klöpper K, Nicke M, Skawran B, Hector A, Yamini P, Steinmann D, Weise S, Stuhrmann M, Karstens JH: Spectrum of ATM gene mutations in a hospital-based series of unselected breast cancer patients. Cancer Res. 2001, 61: 7608-7615.
Broeks A, Urbanus JH, de Knijff P, Devilee P, Nicke M, Klöpper K, Dörk T, Floore AN, van't Veer LJ: IVS10-6T>G, an ancient ATM germline mutation linked with breast cancer. Hum Mutat. 2003, 21: 521-528. 10.1002/humu.10204.
Foray N, Marot D, Gabriel A, Randrianarison V, Carr AM, Perricaudet M, Ashworth A, Jeggo P: A subset of ATM- and ATR-dependent phosphorylation events requires the BRCA1 protein. EMBO J. 2003, 22: 2860-2871. 10.1093/emboj/cdg274.
Sommer SS, Buzin CH, Jung M, Zheng J, Liu Q, Jeong SJ, Moulds J, Nguyen VQ, Feng J, Bennett WP, Dritschilo A: Elevated frequency of ATM gene missense mutations in breast cancer relative to ethnically matched controls. Cancer Genet Cytogenet. 2002, 134: 25-32. 10.1016/S0165-4608(01)00594-5.
Acknowledgements
We thank all individuals who participated in this study. We are grateful to Dr Georgia Chenevix-Trench and Heather Thorne for providing positive control samples and discussions, and to counselling and laboratory staff (including Amanda Goncalves dos Santos Silva and Margie Smith) of the GHSV, RMH, SAFCS and WH Familial Cancer Services. Laboratory work performed in Melbourne was supported by the Department of Medicine (Melbourne University) and the Victorian Breast Cancer Research Consortium.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Rights and permissions
About this article
Cite this article
Lindeman, G.J., Hiew, M., Visvader, J.E. et al. Frequency of the ATM IVS10-6T→G variant in Australian multiple-case breast cancer families. Breast Cancer Res 6, R401 (2004). https://doi.org/10.1186/bcr806
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/bcr806