
Abstract
Purpose
The ataxia telangiectasia-mutated (ATM) gene is a moderate susceptibility gene for breast cancer. However, little is known about the breast cancer phenotypes associated with ATM mutation. We therefore investigated the spectrum and clinical characteristics of ATM germline mutations in Chinese breast cancer patients.
Methods
A multi-gene panel was performed to screen for ATM germline mutations in 7657 BRCA1/2-negative breast cancer patients. All deleterious mutations were validated by independent polymerase chain reaction (PCR)-Sanger sequencing.
Results
A total of 31 pathogenic mutations in the ATM gene across 30 carriers were identified, and the ATM mutation rate was 0.4% (30/7,657) in this cohort. The majority of the mutations (90.3%, 28/31) were nonsense or frameshift mutations. Of the total ATM mutations, 61.3% (19/31) were novel mutations and 13 recurrent mutations were found. ATM mutations carriers were significantly more likely to have a family history of breast and/or ovarian cancer (26.7% in carriers vs. 8.6% in non-carriers, p < 0.001), as well as a family history of any cancer (60.0% in carriers vs. 31.5% in non-carriers, p = 0.001). In addition, ATM mutations carriers were significantly more likely to have oestrogen receptor (ER)-positive (p = 0.011), progesterone receptor (PR)-positive (p = 0.040), and lymph node-positive breast cancer (p = 0.034).
Conclusions
The prevalence of the ATM mutation is approximately 0.4% in Chinese BRCA1/2-negative breast cancer. ATM mutation carriers are significantly more likely to have a family history of cancer and to develop ER- and/or PR-positive breast cancer or lymph node-positive breast cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The ataxia telangiectasia-mutated (ATM) gene is located on chromosome 11q22-23 and encodes a serine/threonine protein kinase. The ATM protein plays a central role in the cellular DNA damage response that is necessary to maintain genome stability. When DNA damage occurs, ATM directly phosphorylates TP53, BRCA1, and other proteins involved in the DNA double-strand break (DSB) response. ATM deficiency exhibits a higher predisposition to breast cancer and other malignant diseases [1, 2], and has been demonstrated to be a moderate breast cancer susceptibility gene [3].
Together with BRCA1, BRCA2, TP53, CHEK2, and several other genes involved in breast cancer predisposition, ATM is currently tested in most gene panel assays performed for breast cancer patients [4]. In these studies, the prevalence of the ATM mutation ranged from 0.45 to 1.0% [5,6,7], and a rare mutation c.T7271G (p.V2424G) was linked with a particularly high risk [8,9,10]. However, germline mutations in the ATM gene have not been well documented in Chinese women. A recent study using a multiple gene-sequencing assay identified an ATM mutation rate of 0.64% among 937 Chinese breast cancer patients with high hereditary risk [11]. However, the sample size of this study was relatively small. Importantly, the relationship between the ATM germline mutation and clinical characteristics is still unknown, though recent study found that lower expression of ATM in breast cancer was associated with a higher grade in these patients [12, 13]. Therefore, the clinical relevance of the spectrum of ATM mutations in Chinese breast cancer patients needs to be fully elucidated.
In this study, we identified ATM germline mutations in 7657 BRCA1/2-negative breast cancer patients who were unselected for age at diagnosis or a family history of breast cancer. We further analysed the association of ATM germline mutations with clinical characteristics in this cohort.
Materials and methods
Study population
A total of 10,378 patients were diagnosed with breast cancer at the Breast Center of Peking University Cancer Hospital from October 2003 to May 2015. Among these patients, 8085 were sequenced on a 62-gene panel as described in our prior study [14]. After excluding 428 patients with BRCA1/2 mutations, 7657 patients were included in our analysis. The patients’ ages at diagnosis ranged from 19 to 98 years, with a mean age of 51 years (Online resource 1). The definition of a family history of breast and/or ovarian cancer, or family history of any cancer, is described in our previous study [14]. The clinical and tumour characteristics were abstracted from medical records and the family history of cancer was collected from both medical records and telephone interviews with each patient. This study was approved by the Research Ethics Committee of Peking University Cancer Hospital (No. 2011KT12), and written informed consent was obtained from all participants.
Pathology
Oestrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) were profiled using an immunohistochemical (IHC) assay on breast cancer tissue obtained from core-needle biopsies or surgery, as previously described [15]. A positive result for ER or PR was defined as ≥ 1% of tumour cells displaying positive nuclear staining. HER2 positivity was defined as a score of 3+ or by HER-2 gene amplification using fluorescent in situ hybridization.
ATM mutation screening
Blood samples were collected from above breast cancer participants, and peripheral DNA was extracted from patient blood samples using the whole blood genome DNA isolation kit (Bioteke, Beijing, China). A 62-gene panel assay was used to screen ATM mutations using the HiSeq 2500 platform (Illumina Inc., San Diego, CA, USA) as described in our previous study [14]; 2 µg of genomic DNA was used for the screening. The panel covered all coding regions and splice sites of the ATM gene. All pathogenic mutations were validated by polymerase chain reaction (PCR)-Sanger sequencing.
Mutation classification
Nonsense and frameshift mutations that lead to the formation of truncated proteins were classified as pathogenic mutations. Missense and splice-site mutations were classified by ClinVar (http://www.ncbi.nlm.nih.gov/clinvar) and the American College of Medical Genetics and Genomics guidelines [16]. Previously published data and prediction software were used to support the classifications. In this study, only pathogenic or likely pathogenic mutations were included for further analysis.
Statistical analysis
The differences in age between ATM mutation carriers and non-carriers were described as the means ± standard deviation (SD) and were tested by one-way analysis of variance (ANOVA). Differences in clinical characteristics between ATM mutation carriers and non-carriers were tested using Pearson’s χ2 test and Fisher’s exact test when violation existed. Two-sided p values < 0.05 were considered to be statistically significant. All analyses were carried out using SPSS 20.0 software (Chicago, IL, USA).
Results
Prevalence and the spectrum of ATM germline mutations
A total of 31 ATM germline mutations were identified in 30 of the 7657 BRCA1/2-negative breast cancer patients (Fig. 1; Tables 1, 2). One patient carried two ATM mutations, c.8929_8930insT and c.8915_8924del (Table 2). Among the 31 ATM mutations, 28 (90.3%) were either frameshift or nonsense mutations (9 frameshift and 19 nonsense mutations). Additionally, two missense mutations c.C6679T (p.R2227C) and c.A8711G (p.E2904G) were detected, which were previously reported as pathogenic mutations [17,18,19]. In total, the prevalence of pathogenic ATM mutations in this cohort was 0.4% (30/7,657).

The distribution of identified germline mutations in the ATM gene. ATM comprises 3056 amino acids with 4 important domains: Ter1/ATM N-terminal motif (TAN, amino acid residues 1–166), FRAP-ATM-TRRAP domain (FAT, amino acid residues 1960–2566), PI-3 kinase domain (PIK, amino acid residues 2712–2962), C-terminal FATC domain (FATC, amino acid residues 3024–3056), and a p53 interaction region (amino acid residues 2862–3012). Each solid circle presents a case with ATM mutation
Among these 31 ATM mutations, 13 were recurrent (p.R2486X, n = 3; Y155X, n = 2; p.F802fr, n = 2; p.W1795X, n = 2; p.Q2206X, n = 2; p.R2227C, n = 2; Fig. 1; Table 1), accounting for 41.9% (13/31) of all ATM mutations. Of the total ATM mutations, 61.3% (19/31) were novel and not found in databases or previous publications (Table 1). The distribution of the pathogenic mutations spanned the entire ATM coding sequence.
Clinicopathological characteristics
The clinicopathological characteristics of the 7657 BRCA1/2-negative patients are presented in Online resource 1. Among the 30 ATM mutation carriers, 8 (26.7%) patients had a family history of breast and/or ovarian cancer, while 18 (60.0%) had a family history of any cancer. Among the 7627 non-carriers, 653 (8.6%) had a family history of breast and/or ovarian cancer while 2406 (31.5%) had a family history of any cancer. The ATM mutation carriers had a significantly higher frequency of a family history of any cancer (60.0% in carriers vs. 31.5% in non-carriers, p = 0.001), especially breast and/or ovarian cancer (26.7% in carriers vs. 8.6% in non-carriers, p < 0.001) (Table 3). The available pedigrees are provided in Fig. 2. Additionally, the ATM mutation carriers were more likely to manifest as ER-positive (p = 0.011), PR-positive (p = 0.040), and lymph node-positive (p = 0.034) than non-carriers (Table 3). No significant association was found between ATM mutations and age at diagnosis, tumour size, bilateral breast cancer, tumour grade, or HER-2 status in this cohort of 7657 patients.

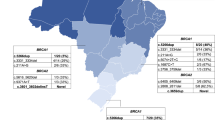
Pedigrees of ATM germline mutations with a family history of breast cancer. Solid circles represent patients with breast cancer. Arrowheads represent probands. Slashed symbols represent deceased individuals. The age at diagnosis and the age at death (Dx.+age) are included under the symbol. a Pedigree of the family with proband (II-2) carrying the p.K468fr mutation of ATM. b Pedigree of the family with proband (II-3) and her sister (II-4) carrying the p.Q2206X mutation of ATM. c Pedigree of the family with proband (II-3) carrying the p.E2904G mutation of ATM. d Pedigree of the family with proband carrying the p.R2486X mutation of ATM
Discussion
In this study, we screened ATM mutations in a large cohort of 7,657 unselected Chinese patients with BRCA1/2-negative breast cancer. To our knowledge, this is currently the largest study investigating the prevalence of ATM mutations and its effect on breast cancer in Asian population. In our study, 30 patients (0.4%) carried ATM germline mutations. ATM mutation carriers were more likely to have a family history of cancer and to develop ER-positive and/or PR-positive breast cancer, or lymph node-positive breast cancer.
The prevalence of the ATM mutation in our study was 0.4%, which is lower than that observed in Caucasian patients. Two previous large-scale gene panel studies found that the prevalence of ATM mutation was approximately 1% in patients with a majority of European ancestry [6, 7]. Recently, Li et al. determined the frequency of ATM mutation among Chinese breast cancer patients with high hereditary risk. They reported an ATM mutation rate of 0.77% (6/778) in BRCA1/2-negative patients [11]. In this study, we found that the prevalence of ATM mutations was 1.2% in familial breast cancer patients, which is similar to that of Li et al.
Among these 31 mutations, 90.3% mutations were either frameshift or nonsense mutations that led to a truncated protein; therefore, these mutations were classified as pathogenic mutations. Additionally, the remaining two missense mutations p.R2227C and p.E2904G were also considered as pathogenic mutations. The p.R2227C mutation was located in the FRAP-ATM-TRRAP (FAT) domain of the ATM protein, and the p.R2227C mutation leads to the ATM protein instability and eliminates phosphorylation in the S1981 self-phosphorylation site [17, 18]; these studies indicated that p.R2227C is a pathogenic mutation. Another missense mutation (p.E2904G) was located in the PI-3 kinase (PIK) domain of the ATM protein and was previously reported to be deleterious due to the mutation causing an apparent instability of the protein [19]. Approximately 61.3% of the ATM mutations detected in our current study have not been previously reported, suggesting that these mutations could be specific for Chinese women. The dominant negative p.V2424G mutation confers a particularly high risk but was not found in any of the Chinese breast cancer patients in our study, which indicates that the ATM p.V2424G mutation is absent or quite infrequent in Chinese women.
The prevalence of ATM mutations was significantly higher in patients with a family history of breast and/or ovarian cancer or any cancer, which is similar to that of patients with BRCA1/2 mutation [14, 33]. Our results were consistent with previous reports that ATM mutations were more frequent in breast cancer with a first-degree family history [30, 34]. It is well documented that ATM is a moderate-penetrance breast cancer susceptibility gene, the relative risk of breast cancer in ATM mutation carriers was 2.2–3.3-fold [4, 7, 35,36,37,38], and the cumulative risk of breast cancer in ATM mutation carriers was 16–43% by age 80 years [3, 36, 39,40,41]. Of note, the breast cancer risk associated with ATM mutations varies widely and should be used with caution in clinical practice. Therefore, the family history of breast cancer should be taken into account during genetic counselling. The results from other studies also found ATM mutations confer an increased risk of gastric cancer, pancreatic cancer, prostate cancer, colorectal cancer, and melanoma [42, 43]. According to the 2018 National Comprehensive Cancer Network guidelines, women who are heterozygous for a pathogenic ATM mutation should undergo yearly mammographic screening starting by at least 40 years of age because their lifetime risk of breast cancer is likely greater than 25%. For women who also have a strong family history of breast cancer, earlier initiation of high-risk screening with both MRI and mammography should be considered [44]. This indicates that further surveillance is necessary for patients with ATM mutation and their close relatives.
As our understanding of the genetic heterogeneity of breast cancer grows, evidences that mutations in different genes may be associated with different breast cancer subtypes have emerged. It is known that BRCA1 mutations are associated with triple-negative breast cancer [14, 33], whereas TP53 mutations are associated with HER2-positive breast cancer [11]. In our study, ATM mutations were particularly frequent in ER-positive and/or PR-positive breast cancer, which is consistent with the findings of Renault et al. [45] who reported that ATM-associated breast cancers were mostly Luminal B subtype. Additionally, we found that ATM mutation tumours were more likely to be lymph node-positive.
ATM is the main transducer in the repair of DNA DSB, and DSB damage results in a clinical benefit from poly (ADP-ribose) polymerase (PARP) inhibitors [46]. Recent studies suggest that multiple cancer cells with lower expression of ATM [47,48,49], including breast cancer cell lines [49], were sensitive to DNA damage drug PARP1 inhibitors, and ATM mutant lymphoid tumour cells also benefit from PARP1 inhibitors [50]. Two recent phase II double-blind studies indicated that low ATM expressed metastatic gastric cancer [51] and ATM mutant metastatic prostate cancers patients [52] benefit from the PARP inhibitor olaparib. Therefore, ATM mutation carriers may be potential candidates for treatment with PARP inhibitors.
In conclusion, we found that 0.4% of BRCA1/2-negative breast cancer patients carry ATM germline mutations in this large cohort, and many mutations are specific to the Chinese population. Our study also demonstrates the characteristics of ATM mutations in the Chinese population. In the current study, we found ATM mutations were strongly associated with breast cancer patients who have a family history of breast and/or ovarian cancer. Therefore, we suggested that ATM should be added in genetic testing in Chinese familial breast cancer patients. And the ATM mutation carriers should be offered intensive surveillance and would potentially benefit from targeted therapy. Large case–control studies are needed to fully elucidate the risk and implication of ATM mutations in breast cancer in the Chinese population.
Abbreviations
- ATM :
-
The ataxia telangiectasia-mutated gene
- ANOVA:
-
One-way analysis of variance
- DSB:
-
DNA double-strand break
- ER:
-
Oestrogen receptor
- FAT:
-
FRAP-ATM-TRRAP
- HER2:
-
Human epidermal growth factor receptor 2
- IHC:
-
Immunohistochemical
- PARP:
-
Poly (ADP-ribose) polymerase
- PCR:
-
Polymerase chain reaction
- PIK:
-
PI-3 kinase
- PR:
-
Progesterone receptor
- SD:
-
Standard deviation
- TNBC:
-
Triple-negative breast cancer
References
Lavin MF (2008) Ataxia-telangiectasia: from a rare disorder to a paradigm for cell signalling and cancer. Nat Rev Mol Cell Biol 9(10):759–769. https://doi.org/10.1038/nrm2514
Shiloh Y, Ziv Y (2013) The ATM protein kinase: regulating the cellular response to genotoxic stress, and more. Nat Rev Mol Cell Biol 14(4):197–210
Tung N, Domchek SM, Stadler Z et al (2016) Counselling framework for moderate-penetrance cancer-susceptibility mutations. Nat Rev Clin Oncol 13(9):581–588. https://doi.org/10.1038/nrclinonc.2016.90
Easton DF, Pharoah PD, Antoniou AC et al (2015) Gene-panel sequencing and the prediction of breast-cancer risk. N Engl J Med 372(23):2243–2257. https://doi.org/10.1056/NEJMsr1501341
Thompson ER, Rowley SM, Li N et al (2016) Panel testing for familial breast cancer: calibrating the tension between research and clinical care. J Clin Oncol 34(13):1455–1459. https://doi.org/10.1200/jco.2015.63.7454
Buys SS, Sandbach JF, Gammon A et al (2017) A study of over 35,000 women with breast cancer tested with a 25-gene panel of hereditary cancer genes. Cancer 123(10):1721–1730. https://doi.org/10.1002/cncr.30498
Couch FJ, Shimelis H, Hu C et al (2017) Associations between cancer predisposition testing panel genes and breast cancer. JAMA Oncol 3(9):1190–1196. https://doi.org/10.1001/jamaoncol.2017.0424
Southey MC, Goldgar DE, Winqvist R et al (2016) PALB2, CHEK2 and ATM rare variants and cancer risk: data from COGS. J Med Genet 53(12):800–811. https://doi.org/10.1136/jmedgenet-2016-103839
Bernstein JL, Teraoka S, Southey MC et al (2006) Population-based estimates of breast cancer risks associated with ATM gene variants c.7271T> G and c.1066-6T> G (IVS10-6T> G) from the Breast Cancer Family Registry. Hum Mutat 27(11):1122–1128. https://doi.org/10.1002/humu.20415
Chenevix-Trench G, Spurdle AB, Gatei M et al (2002) Dominant negative ATM mutations in breast cancer families. J Natl Cancer Inst 94(3):205–215
Li J, Jing R, Wei H et al (2018) Germline mutations in 40 cancer susceptibility genes among Chinese patients with high hereditary risk breast cancer. Int J Cancer. https://doi.org/10.1002/ijc.31601
Bueno RC, Canevari RA, Villacis RA et al (2014) ATM down-regulation is associated with poor prognosis in sporadic breast carcinomas. Ann Oncol 25(1):69–75. https://doi.org/10.1093/annonc/mdt421
Feng X, Li H, Dean M et al (2015) Low ATM protein expression in malignant tumor as well as cancer-associated stroma are independent prognostic factors in a retrospective study of early-stage hormone-negative breast cancer. Breast Cancer Res 17:65. https://doi.org/10.1186/s13058-015-0575-2
Sun J, Meng H, Yao L et al (2017) Germline mutations in cancer susceptibility genes in a large series of unselected breast cancer patients. Clin Cancer 23(20):6113–6119. https://doi.org/10.1158/1078-0432.ccr-16-3227
Yao L, Liu Y, Li Z et al (2011) HER2 and response to anthracycline-based neoadjuvant chemotherapy in breast cancer. Ann Oncol 22(6):1326–1331. https://doi.org/10.1093/annonc/mdq612
Richards S, Aziz N, Bale S et al (2015) Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med 17(5):405–424. https://doi.org/10.1038/gim.2015.30
Becker-Catania SG, Chen G, Hwang MJ et al (2000) Ataxia-telangiectasia: phenotype/genotype studies of ATM protein expression, mutations, and radiosensitivity. Mol Genet Metab 70(2):122–133. https://doi.org/10.1006/mgme.2000.2998
Mitui M, Nahas SA, Du LT et al (2009) Functional and computational assessment of missense variants in the ataxia-telangiectasia mutated (ATM) gene: mutations with increased cancer risk. Hum Mutat 30(1):12–21. https://doi.org/10.1002/humu.20805
Ziv Y, Bar-Shira A, Pecker I et al (1997) Recombinant ATM protein complements the cellular A–T phenotype. Oncogene 15(2):159–167. https://doi.org/10.1038/sj.onc.1201319
Buzin CH, Gatti RA, Nguyen VQ et al (2003) Comprehensive scanning of the ATM gene with DOVAM-S. Hum Mutat 21(2):123–131. https://doi.org/10.1002/humu.10158
Keimling M, Volcic M, Csernok A et al (2011) Functional characterization connects individual patient mutations in ataxia telangiectasia mutated (ATM) with dysfunction of specific DNA double-strand break-repair signaling pathways. FASEB J 25(11):3849–3860. https://doi.org/10.1096/fj.11-185546
Nakamura K, Du L, Tunuguntla R et al (2012) Functional characterization and targeted correction of ATM mutations identified in Japanese patients with ataxia-telangiectasia. Hum Mutat 33(1):198–208. https://doi.org/10.1002/humu.21632
Kurian AW, Hare EE, Mills MA et al (2014) Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J Clin Oncol 32(19):2001–2009. https://doi.org/10.1200/jco.2013.53.6607
Micol R, Ben Slama L, Suarez F et al (2011) Morbidity and mortality from ataxia-telangiectasia are associated with ATM genotype. J Allergy Clin Immunol 128(2):382–389.e381. https://doi.org/10.1016/j.jaci.2011.03.052
Lin CH, Lin WC, Wang CH et al (2010) Child with ataxia telangiectasia developing acute myeloid leukemia. J Clin Oncol 28(14):e213–e214. https://doi.org/10.1200/jco.2009.25.5067
Jacquemin V, Rieunier G, Jacob S et al (2012) Underexpression and abnormal localization of ATM products in ataxia telangiectasia patients bearing ATM missense mutations. Eur J Hum Genet 20(3):305–312. https://doi.org/10.1038/ejhg.2011.196
Magliozzi M, Piane M, Torrente I et al (2006) DHPLC screening of ATM gene in Italian patients affected by ataxia-telangiectasia: fourteen novel ATM mutations. Dis Mark 22(4):257–264
Susswein LR, Marshall ML, Nusbaum R et al (2016) Pathogenic and likely pathogenic variant prevalence among the first 10,000 patients referred for next-generation cancer panel testing. Genet Med 18(8):823–832. https://doi.org/10.1038/gim.2015.166
Telatar M, Wang Z, Udar N et al (1996) Ataxia-telangiectasia: mutations in ATM cDNA detected by protein-truncation screening. Am J Hum Genet 59(1):40–44
Teraoka SN, Malone KE, Doody DR et al (2001) Increased frequency of ATM mutations in breast carcinoma patients with early onset disease and positive family history. Cancer 92(3):479–487
Laake K, Jansen L, Hahnemann JM et al (2000) Characterization of ATM mutations in 41 Nordic families with ataxia telangiectasia. Hum Mutat 16(3):232–246. https://doi.org/10.1002/1098-1004(200009)16:3%3C232::aid-humu6%3E3.0.co;2-l
Barone G, Groom A, Reiman A et al (2009) Modeling ATM mutant proteins from missense changes confirms retained kinase activity. Hum Mutat 30(8):1222–1230. https://doi.org/10.1002/humu.21034
Zhang J, Sun J, Chen J et al (2016) Comprehensive analysis of BRCA1 and BRCA2 germline mutations in a large cohort of 5931 Chinese women with breast cancer. Breast Cancer Res Treat 158(3):455–462. https://doi.org/10.1007/s10549-016-3902-0
Thorstenson YR, Roxas A, Kroiss R et al (2003) Contributions of ATM mutations to familial breast and ovarian cancer. Cancer Res 63(12):3325–3333
Renwick A, Thompson D, Seal S et al (2006) ATM mutations that cause ataxia-telangiectasia are breast cancer susceptibility alleles. Nat Genet 38(8):873–875. https://doi.org/10.1038/ng1837
Thompson D, Duedal S, Kirner J et al (2005) Cancer risks and mortality in heterozygous ATM mutation carriers. J Natl Cancer Inst 97(11):813–822. https://doi.org/10.1093/jnci/dji141
Decker B, Allen J, Luccarini C et al (2017) Rare, protein-truncating variants in ATM, CHEK2 and PALB2, but not XRCC2, are associated with increased breast cancer risks. J Med Genet 54(11):732–741. https://doi.org/10.1136/jmedgenet-2017-104588
Lu HM, Li S, Black MH et al (2018) Association of breast and ovarian cancers with predisposition genes identified by large-scale sequencing. JAMA Oncol. https://doi.org/10.1001/jamaoncol.2018.2956
van Os NJ, Roeleveld N, Weemaes CM et al (2016) Health risks for ataxia-telangiectasia mutated heterozygotes: a systematic review, meta-analysis and evidence-based guideline. Clin Genet 90(2):105–117. https://doi.org/10.1111/cge.12710
Marabelli M, Cheng SC, Parmigiani G (2016) Penetrance of ATM gene mutations in breast cancer: a meta-analysis of different measures of risk. Genet Epidemiol 40(5):425–431. https://doi.org/10.1002/gepi.21971
Swift M, Lukin JL (2008) Breast cancer incidence and the effect of cigarette smoking in heterozygous carriers of mutations in the ataxia-telangiectasia gene. Cancer Epidemiol Biomark Prev 17(11):3188–3192. https://doi.org/10.1158/1055-9965.Epi-08-0414
Dombernowsky SL, Weischer M, Allin KH et al (2008) Risk of cancer by ATM missense mutations in the general population. J Clin Oncol 26(18):3057–3062. https://doi.org/10.1200/jco.2007.14.6613
Helgason H, Rafnar T, Olafsdottir HS et al (2015) Loss-of-function variants in ATM confer risk of gastric cancer. Nat Genet 47(8):906–910. https://doi.org/10.1038/ng.3342
Daly MB, Pilarski R, Berry M et al NCCN Clinical practice guidelines in oncology. In: Genetic/Familial high-risk assessment: breast and ovarian version1.2018. Accessed 17 June 2018
Renault AL, Mebirouk N, Fuhrmann L et al (2018) Morphology and genomic hallmarks of breast tumours developed by ATM deleterious variant carriers. Breast Cancer Res 20(1):28. https://doi.org/10.1186/s13058-018-0951-9
Choi M, Kipps T, Kurzrock R (2016) ATM Mutations in cancer: therapeutic implications. Mol Cancer Ther 15(8):1781–1791. https://doi.org/10.1158/1535-7163.Mct-15-0945
Williamson CT, Muzik H, Turhan AG et al (2010) ATM deficiency sensitizes mantle cell lymphoma cells to poly(ADP-ribose) polymerase-1 inhibitors. Mol Cancer Ther 9(2):347–357. https://doi.org/10.1158/1535-7163.Mct-09-0872
Kubota E, Williamson CT, Ye R et al (2014) Low ATM protein expression and depletion of p53 correlates with olaparib sensitivity in gastric cancer cell lines. Cell Cycle 13(13):2129–2137. https://doi.org/10.4161/cc.29212
Gilardini Montani MS, Prodosmo A, Stagni V et al (2013) ATM-depletion in breast cancer cells confers sensitivity to PARP inhibition. J Exp Clin Cancer Res 32:95. https://doi.org/10.1186/1756-9966-32-95
Weston VJ, Oldreive CE, Skowronska A et al (2010) The PARP inhibitor olaparib induces significant killing of ATM-deficient lymphoid tumor cells in vitro and in vivo. Blood 116(22):4578–4587. https://doi.org/10.1182/blood-2010-01-265769
Bang YJ, Im SA, Lee KW et al (2015) Randomized, double-blind phase II trial with prospective classification by atm protein level to evaluate the efficacy and tolerability of olaparib plus paclitaxel in patients with recurrent or metastatic gastric cancer. J Clin Oncol 33(33):3858–3865. https://doi.org/10.1200/jco.2014.60.0320
Mateo J, Carreira S, Sandhu S et al (2015) DNA-Repair defects and olaparib in metastatic prostate cancer. N Engl J Med 373(18):1697–1708. https://doi.org/10.1056/NEJMoa1506859
Acknowledgements
This study was supported by the National Natural Science Foundation of China (81772824, 81773209 and 81372832).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was conducted in accordance with Helsinki Declaration, and was approved by the Research Ethics Committee of Peking University Cancer Hospital.
Informed consent
Written informed consent was obtained from all participants.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Yang, Z., Ouyang, T., Li, J. et al. Prevalence and characterization of ATM germline mutations in Chinese BRCA1/2-negative breast cancer patients. Breast Cancer Res Treat 174, 639–647 (2019). https://doi.org/10.1007/s10549-018-05124-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-018-05124-5