
Abstract
Background
Recently, several new endoscopic treatments have been used to treat patients with Barrett's esophagus with high grade dysplasia. This systematic review aimed to determine the safety and effectiveness of these treatments compared with esophagectomy.
Methods
A comprehensive literature search was undertaken to identify studies of endoscopic treatments for Barrett's esophagus or early stage esophageal cancer. Information from the selected studies was extracted by two independent reviewers. Study quality was assessed and information was tabulated to identify trends or patterns. Results were pooled across studies for each outcome. Safety (occurrence of adverse events) and effectiveness (complete eradication of dysplasia) were compared across different treatments.
Results
The 101 studies that met the selection criteria included 8 endoscopic techniques and esophagectomy; only 12 were comparative studies. The quality of evidence was generally low. Methods and outcomes were inconsistently reported. Protocols, outcomes measured, follow-up times and numbers of treatment sessions varied, making it difficult to calculate pooled estimates.
The surgical mortality rate was 1.2%, compared to 0.04% in 2831 patients treated endoscopically (1 death). Adverse events were more severe and frequent with esophagectomy, and included anastomotic leaks (9.4%), wound infections (4.1%) and pulmonary complications (4.1%). Four patients (0.1%) treated endoscopically experienced bleeding requiring transfusions. The stricture rate with esophagectomy (5.3%) was lower than with porfimer sodium photodynamic therapy (18.5%), but higher than aminolevulinic acid (ALA) 60 mg/kg PDT (1.4%). Dysphagia and odynophagia varied in frequency across modalities, with the highest rates reported for multipolar electrocoagulation (MPEC). Photosensitivity, an adverse event that occurs only with photodynamic therapy, was experienced by 26.4% of patients who received porfimer sodium.
Some radiofrequency ablation (RFA) or argon plasma coagulation (APC) studies (used in multiple sessions) reported rates of almost 100% for complete eradication of dysplasia. But the study methods and findings were not adequately described. The other studies of endoscopic treatments reported similarly high rates of complete eradication.
Conclusions
Endoscopic treatments offer safe and effective alternatives to esophagectomy for patients with Barrett's esophagus and high grade dysplasia. Unfortunately, shortcomings in the published studies make it impossible to determine the comparative effectiveness of each of the endoscopic treatments.
Similar content being viewed by others


Background
Barrett's esophagus (BE) is a benign condition where abnormal cells (intestinal metaplasia), replace the normal lining of the esophagus. It is typically caused by long-term gastroesophageal reflux disease. Between 2% to 6% of Canadians may have Barrett's esophagus[1]. Similar prevalence rates have been reported in studies from Sweden (1.6%) and the United States (5.9%)[2, 3].
Although Barrett's esophagus itself is not harmful, in some individuals, precancerous dysplasia develops in the Barrett's tissue. The presence of dysplasia carries a higher risk of developing esophageal adenocarcinoma - a type of esophageal cancer. In addition to the cancer risk, Barrett's esophagus decreases patients' quality of life and increases health care costs[4–7].
The rising incidence of esophageal adenocarcinoma has focused attention on preventing cancer by removing the dysplasia and allowing normal, squamous esophageal mucosa to regenerate. Endoscopic techniques have been developed as a result. They can be applied sequentially to increase diagnostic yield and improve treatment outcomes. There are two categories: endoscopic mucosal resection (EMR) and endoscopic ablation. EMR with a cautery snare excision technique can remove visible raised or flat lesions for diagnostic and therapeutic roles. Diagnostically, it allows for complete histopathological assessment of the target mucosa. Those with superficial lesions can go on to further ablative techniques. Lesions that are found to invade submucosa may need referral for surgical resection. Therapeutically, EMR can be used for curative intent if the target lesion is small. However, in most cases of Barrett's esophagus, it is used to remove dysplastic nodules leaving the larger surface area for endoscopic ablation.
Photodynamic therapy (PDT) is one of the new endoscopic treatments used to remove dysplasia. Other endoscopic treatments include: argon plasma coagulation (APC), cryoablation, laser ablation, multipolar electrocoagulation (MPEC), radiofrequency ablation (RFA), and thermocoagulation. Depending on the extent of dysplasia, several endoscopic treatment sessions or a combination of treatments may be used.
Patients also receive long-term drug therapy to control gastroesophageal reflux and prevent further damage to the esophagus[8]. Endoscopic therapies are less invasive alternatives to esophagectomy (surgical removal of the esophagus), which is associated with high rates of morbidity and mortality, and with decreased quality of life[9–11].
Clinicians now have a variety of technologies to choose from when treating Barrett's esophagus with dysplasia. This systematic review of published clinical studies compares the evidence on the safety and effectiveness of the endoscopic treatments and of esophagectomy and may provide some guidance for clinical practice.
Methods
Data collection
Literature search
An extensive search for published and unpublished studies of endoscopic and non-endoscopic procedures for Barrett's esophagus was performed. Search terms included keywords and controlled vocabulary terms used to describe Barrett's, photodynamic therapy and other endoscopic techniques, and esophagectomy. Searches for the alternative treatments (i.e., other than PDT) were limited to studies from 2003 to January 2009. The bibliographic databases searched included: PubMed (MEDLINE), The Cochrane Library, the UK Centre for Reviews and Dissemination (DARE, Health Technology Assessment, and NHS Economic Evaluation) databases, EMBASE, CINAHL, Web of Science and EconLit. Monthly update searches in PubMed were run throughout the project to identify new studies. Meeting abstracts from the American Society of Clinical Oncology and Digestive Disease Week, as well as practice guidelines and clinical trials web sites were also searched, as were the reference lists from relevant papers and earlier health technology assessments.
Study selection
Results from the literature searches were imported into a Reference Manager® database to remove duplicates and manage bibliographic citations. Titles and abstracts (where available), were independently screened by two researchers. The full papers of potentially relevant studies were retrieved and assessed against pre-defined inclusion criteria (Table 1). Non-English language studies were excluded, unless an English language abstract provided sufficient detail on patients and outcomes.
Critical appraisal and synthesis
Information from the studies was extracted by two reviewers using a pre-tested data abstraction form and a set of decision rules. The form contained elements for examining the purpose and methods of each study (Table 2). Missing data were sought from study authors. Consensus between reviewers on the information collected was assessed using the Kappa statistic.
The quality of each study was also assessed by two reviewers using the Oxford Centre for Evidence-based Medicine Levels of Evidence[12]. Discrepancies were resolved through consensus and Kappa scores were calculated.
Data analysis
Qualitative
Information was summarized in tabular form to more easily identify trends or patterns in findings reported across studies.
Quantitative
Results from individual studies were pooled using weighted mean values to generate summary estimates for each of the outcomes of interest. All quantitative analyses were conducted in accordance with intention-to-treat principles (i.e., patients were analyzed in the groups to which they were originally allocated, regardless of whether or not they received the assigned treatment).
Results
Description of studies
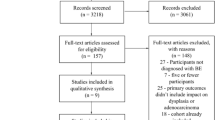
Over 400 potentially relevant papers were selected from the literature search results and reviewed for inclusion (Figure 1). Of these, 99 papers, reporting on 101 separate studies and 3042 patients, met the inclusion criteria. Descriptions of each study are presented in Additional files 1, 2, 3, 4, 5, 6, 7, and 8. A breakdown of studies by the type of intervention and study design is presented in Table 3.

Flow diagram of study selection. Notes:*10 new studies were added since the first literature review. Of these studies, 6 were included, and 4 were excluded.
Quality of studies
The quality of the evidence reviewed was generally low. Only 12 studies were comparative (Table 3), and of these, 5 were cohort studies with uncontrolled allocation of patients to each treatment group. Details of the study methods used were sparse, with missing information or inconsistent reporting of outcomes across patient groups.
Seven randomized controlled trials (RCTs) were identified, but these compared only APC with PDT (4 trials[13–16]), or APC with MPEC (2 trials[17, 18]), or RFA with sham procedure (1 trial[19]). Sample sizes were small and follow-up times were short. Because the types of patients and the treatment protocols (e.g., number of treatment sessions) varied a meta-analysis was not used.
In the non-comparative studies of endoscopic techniques (single arm clinical trials or case series), the treatment protocols (e.g., number of treatment sessions), outcomes measured, and follow-up times also differed. There were few studies that reported long-term follow up results, and so pooling of study outcome and adverse event results is limited. As well, the number of treatment sessions provided before outcomes were measured was not often reported, although in many cases, it was after a single ablation. Patients often received interventions in addition to the study treatment. For example, in most studies EMR was performed during endoscopy to confirm the diagnosis of dysplasia. In addition, if one treatment failed to eradicate the dysplasia another treatment would typically be administered. The analyses of outcomes did not usually account for the effects of these additional interventions.
Safety
Adverse events reported for individual studies of esophagectomy and endoscopic alternatives are summarized in Table 4 and Additional file 9. The pooled estimates for esophagectomy and endoscopic treatments are shown in Tables 5 and 6. There were 2 deaths [20, 21] attributed to esophagectomy among the 170 patients who underwent the procedure (a mortality rate of 1.2%). (The surgical studies employed various approaches; in some studies, the actual approach was not specified, and in the others, a number of approaches were used (i.e., the patients did not all have the same surgical approach). Therefore, data could not be analysed according to individual surgical approaches). In contrast, 1 death [13] was reported in the 2831 patients who received endoscopic treatment (0.04%). This death was due to cardiac arrhythmia in a patient who received PDT with aminolevulinic acid (ALA) at a dose of 60 mg/kg of body weight[13].
In the studies that reported bleeding complications following endoscopic treatments, 4 of 2218 patients (0.2%) experienced bleeding requiring transfusions: 1 after PDT[22], 2 after APC[23] and 1 after laser ablation[24]. Strictures were most frequently reported with porfimer sodium PDT (18.5%), followed by laser ablation (4.4%) and APC (2.9%) (Table 6). Although there were no perforations reported in the PDT studies that used a single photosensitizer (reported in Table 6), there was a perforation reported in the Prasad et al study [21], which compared esophagectomy with PDT using two different photosensitizers. Since it was impossible to separate the patients according to the photosensitizer type, this study was not included in Table 6. Patients experiencing dysphagia and odynophagia varied across the treatment modalities, but were highest with MPEC (Table 6). Photosensitivity following PDT was more common with porfimer sodium (26.4%) than with ALA (ranging from 0% to 13.6%). However, in a small series of 5 patients who received hematoporphyrin derivative (HpD), 40% experienced photosensitivity reactions (Table 6).
The most commonly reported adverse events associated with esophagectomy were anastomotic leaks (9.4%), strictures (5.3%), wound infections (4.1%) and pulmonary complications (4.1%) (Table 5). None of the studies discussed the relationship between adverse events and clinician experience.
Efficacy or effectiveness
Values reported for the complete eradication of BE or high grade dysplasia (HGD) with endoscopic treatments are presented in Additional files 10 and 11. Pooled values for complete eradication of BE and HGD with endoscopic treatments are presented in Table 7. For the purposes of this analysis, only the complete eradication rates reported in the individual studies within the first 3 months after ablation were included. Few studies provided enough data on longer follow up periods to make pooling of the data meaningful. The studies did not all report the number of ablations that were provided before the outcome was measured, and in many cases, the authors reported a range of number of treatments.
Results of 2 of the 3 RCTs of PDT (with ALA) versus APC in patients with BE demonstrated a significant difference in complete eradication, favouring APC over PDT[13, 14]. Specifically, the complete eradication rates in the APC group were almost double that of the PDT group (Additional file 10). In the third RCT, complete eradication rates were not reported for both groups of patients[16].
Two RCTs reported on complete eradication of HGD[15, 19]. In the RCT which compared PDT using porfimer sodium to APC, there was no statistically significant difference in complete eradication rate between treatment groups at 4 months follow-up[15]. In the RCT which compared RFA with sham procedure, there was a statistically significant difference in complete eradication rate between the group treated by RFA (81.0%) and the control group (19.0%) at 12 months follow-up[19].
Discussion
Endoscopic therapies appear to be viable and effective treatment options for Barrett's esophagus with high grade dysplasia. All of the endoscopic therapies are safer (i.e., have fewer adverse events and lower mortality rates) than esophagectomy.
Some key questions regarding these treatments cannot yet be answered and further studies are needed to address these "gaps in the evidence". In particular, we need studies:
-
to confirm the long-term safety of these endoscopic treatments, and their effectiveness in preventing esophageal cancer
-
to identify the endoscopic treatments (or combinations of treatments) that produce the best outcomes
-
to determine whether or not continued drug therapy (e.g., with proton pump inhibitors) or surgery (e.g., fundoplication) to treat gastroesophageal reflux is beneficial after endoscopic treatment of dysplasia
-
to provide guidance on the optimal frequency of post-treatment endoscopic surveillance for patients with Barrett's esophagus
-
to measure patient preferences for, and quality of life after, the different endoscopic treatments.
Conclusions
Given the current limitations in the evidence (in terms of both quantity and quality of studies), it was not possible to conclusively determine the comparative effectiveness of the different endoscopic treatments. However, the evidence suggests that endoscopic treatments are safe and reasonably effective alternatives to esophagectomy for patients with Barrett's esophagus with high grade dysplasia. Endoscopic treatments have the additional advantages of being outpatient procedures with shorter recovery times. They also provide treatment options for patients who would not be considered for esophagectomy due to other health conditions.
Of the endoscopic therapies, photosensitivity is only an issue with photodynamic therapy (more so with porfimer sodium than with other photosensitizing agents). Preventing adverse events due to photosensitivity requires patient and caregiver compliance and education.
There appears to be little difference between the endoscopic technologies in terms of overall efficacy. Patient and physician preferences, and the local availability of the different technologies will likely guide decision making. A combination of different endoscopic treatments may provide the best outcomes. Given that relatively few patients need these treatments each year, offering them at specialized centres will concentrate clinical expertise and be the most cost-effective approach.
References
Tougas G, Chen Y, Hwang P, Liu MM, Eggleston A: Prevalence and impact of upper gastrointestinal symptoms in the Canadian population: findings from the DIGEST study. Domestic/International Gastroenterology Surveillance Study. Am J Gastroenterol. 1999, 94: 2845-2854. 10.1111/j.1572-0241.1999.01427.x.
Ronkainen J, Aro P, Storskrubb T, Johansson SE, Lind T, Bolling-Sternevald E, Vieth M, Stolte M, Talley NJ, Agreus L: Prevalence of Barrett's esophagus in the general population: an endoscopic study. Gastroenterology. 2005, 129: 1825-1831. 10.1053/j.gastro.2005.08.053.
Esquivel RF, Boolchang V, Kumar N, Camargo L, Kim JL, Fass R, Sampliner RE: The prevalence of Barrett's esophagus in veteran patients with and without GERD symptoms undergoing outpatient colonoscopy [abstract]. Gastrointest Endosc. 2008, 67: AB172-10.1016/j.gie.2008.03.402.
Lao CD, Simmons M, Syngal S, Bresalier RS, Fortlage L, Normolle D, Griffith KA, Appelman HD, Brenner DE: Dysplasia in Barrett esophagus. Cancer. 2004, 100: 1622-1627. 10.1002/cncr.20149.
Hookey LC: Barrett's esophagus--who, how, how often and what to do with dysplasia?. Can J Gastroenterol. 2006, 20: 463-466.
Yousef F, Cardwell C, Cantwell MM, Galway K, Johnston BT, Murray L: The incidence of esophageal cancer and high-grade dysplasia in Barrett's esophagus: a systematic review and meta-analysis. Am J Epidemiol. 2008, 168: 237-249. 10.1093/aje/kwn121.
Willich SN, Nocon M, Kulig M, Jaspersen D, Labenz J, Meyer-Sabellek W, Stolte M, Lind T, Malfertheiner P: Cost-of-disease analysis in patients with gastro-oesophageal reflux disease and Barrett's mucosa. Aliment Pharmacol Ther. 2006, 23: 371-376. 10.1111/j.1365-2036.2006.02763.x.
Amonkar MM, Kalsekar ID, Boyer JG: The economic burden of Barrett's esophagus in a Medicaid population. Ann Pharmacother. 2002, 36: 605-611. 10.1345/aph.1A309.
Green S, Tawil A, Barr H, Bennett C, Bhandari P, DeCaestecker J, Ragunath K, Singh R, Jankowski J: Surgery versus radical endotherapies for early cancer and high grade dysplasia in Barrett's oesophagus. Cochrane Library. 2009
Reynolds JV, McLaughlin R, Moore J, Rowley S, Ravi N, Byrne PJ: Prospective evaluation of quality of life in patients with localized oesophageal cancer treated by multimodality therapy or surgery alone. Br J Surg. 2006, 93: 1084-1090. 10.1002/bjs.5373.
Qureshi I, Nason KS, Luketich JD: Is minimally invasive esophagectomy indicated for cancer?. Expert Rev Anticancer Ther. 2008, 8: 1449-1460. 10.1586/14737140.8.9.1449.
Phillips B, Ball C, Sackett D, Badenoch D, Straus S, Haynes B, Dawes M: Oxford Centre for Evidence-based Medicine levels of evidence and grades of recommendation. 2001, Oxford (UK): Oxford Centre for Evidence-based Medicine
Hage M, Siersema PD, van DH, Steyerberg EW, Haringsma J, van d V, Grool TE, van Veen RL, Sterenborg HJ, Kuipers EJ: 5-aminolevulinic acid photodynamic therapy versus argon plasma coagulation for ablation of Barrett's oesophagus: a randomised trial. Gut. 2004, 53: 785-790. 10.1136/gut.2003.028860.
Kelty CJ, Ackroyd R, Brown NJ, Stephenson TJ, Stoddard CJ, Reed MW: Endoscopic ablation of Barrett's oesophagus: a randomized-controlled trial of photodynamic therapy vs. argon plasma coagulation. Aliment Pharmacol Ther. 2004, 20: 1289-1296. 10.1111/j.1365-2036.2004.02277.x.
Ragunath K, Krasner N, Raman VS, Haqqani MT, Phillips CJ, Cheung I: Endoscopic ablation of dysplastic Barrett's oesophagus comparing argon plasma coagulation and photodynamic therapy: a randomized prospective trial assessing efficacy and cost-effectiveness. Scand J Gastroenterol. 2005, 40: 750-758. 10.1080/00365520510015737.
Zoepf T, Alsenbesy M, Jakobs R, Apel D, Rosenbaum A, Riemann JF: Photodynamic therapy (PDT) versus argon plasma, coagulation (APC) for ablative therapy of Barrett's esophagus [abstract]. Gastrointest Endosc. 2003, 57: AB139-
Dulai GS, Jensen DM, Cortina G, Fontana L, Ippoliti A: Randomized trial of argon plasma coagulation vs. multipolar electrocoagulation for ablation of Barrett's esophagus. Gastrointest Endosc. 2005, 61: 232-240. 10.1016/S0016-5107(04)02576-3.
Sharma P, Wani S, Weston AP, Bansal A, Hall M, Mathur S, Prasad A, Sampliner RE: A randomised controlled trial of ablation of Barrett's oesophagus with multipolar electrocoagulation versus argon plasma coagulation in combination with acid suppression: long term results. Gut. 2006, 55: 1233-1239. 10.1136/gut.2005.086777.
Shaheen NJ, Sharma P, Overholt BF, Wolfsen HC, Sampliner RE, Wang KK, Galanko JA, Bronner MP, Goldblum JR, Bennett AE, et al: Radiofrequency ablation in Barrett's esophagus with dysplasia. N Eng J Med. 2009, 360: 2277-2288. 10.1056/NEJMoa0808145.
Reed MF, Tolis G, Edil BH, Allan JS, Donahue DM, Gaissert HA, Moncure AC, Wain JC, Wright CD, Mathisen DJ: Surgical treatment of esophageal high-grade dysplasia. Ann Thorac Surg. 2005, 79: 1110-1115. 10.1016/j.athoracsur.2004.09.006.
Prasad GA, Wang KK, Buttar NS, Wongkeesong LM, Krishnadath KK, Nichols FC, Lutzke LS, Borkenhagen LS: Long-term survival following endoscopic and surgical treatment of high-grade dysplasia in Barrett's esophagus. Gastroenterology. 2007, 132: 1226-1233. 10.1053/j.gastro.2007.02.017.
Mackenzie G, Clark BR, Selvasekar C, Jamieson N, Novelli M, Thorpe S, Mosse C, Bown S, Lovat L: Photodynamic therapy with 5 aminolevulinic acid for high grade dysplasia in Barrett's esophagus: Longterm follow up of 51 patients [abstract]. Gastroenterology. 2005, 128: A238-10.1053/j.gastro.2004.11.026.
Manner H, May A, Miehlke S, Dertinger S, Wigginghaus B, Schimming W, Kramer W, Niemann G, Stolte M, Ell C: Ablation of nonneoplastic Barrett's mucosa using argon plasma coagulation with concomitant esomeprazole therapy (APBANEX): a prospective multicenter evaluation. Am J Gastroenterol. 2006, 101: 1762-1769. 10.1111/j.1572-0241.2006.00709.x.
Fisher RS, Bromer MQ, Thomas RM, Cohen S, Krevsky B, Horwitz B, Glazier KD, Das K, Das KA: Predictors of recurrent specialized intestinal metaplasia after complete laser ablation. Am J Gastroenterol. 2003, 98: 1945-1951. 10.1111/j.1572-0241.2003.07628.x.
Behrens A, May A, Gossner L, Gunter E, Pech O, Vieth M, Stolte M, Seitz G, Ell C: Curative treatment for high-grade intraepithelial neoplasia in Barrett's esophagus. Endoscopy. 2005, 37: 999-1005. 10.1055/s-2005-870352.
Ortner MA, Zumbusch K, Liebetruth J, Ebert B, Fleige B, Dietel M, Lochs H: Is topical delta-aminolevulinic acid adequate for photodynamic therapy in Barrett's esophagus? A pilot study. Endoscopy. 2002, 34: 611-616. 10.1055/s-2002-33247.
Ortner M, Zumbusch K, Liebetruth J, Ernst H, Weber J, Wirth J, Wedel S, Lochs H: Photodynamic therapy of Barrett's esophagus after local administration of 5-aminolaevulinic acid [abstract]. Gastroenterology. 1997, 112: A633-
Ackroyd R, Kelty CJ, Brown NJ, Stephenson TJ, Stoddard CJ, Reed MW: Eradication of dysplastic Barrett's oesophagus using photodynamic therapy: long-term follow-up. Endoscopy. 2003, 35: 496-501. 10.1055/s-2003-39676.
Ackroyd R, Davis MF, Brown NJ, Stephenson TJ, Stoddard CJ, Reed MWR: Photodynamic therapy (PDT): a new treatment for Barrett's oesophagus [abstract]. Lasers Med Sci. 1997, 12: 292-
Ackroyd R, Brown NJ, Davis MF, Stephenson TJ, Stoddard CJ, Reed MWR: Aminolaevulinic acid-induced photodynamic therapy in the treatment of dysplastic Barrett's oesophagus and adenocarcinoma. Lasers Med Sci. 1999, 14: 278-285. 10.1007/s101030050095.
Mackenzie G, Selvasekar C, Clark BR, Novelli M, Thorpe S, Mosse C, Bown S, Lovat L: Randomised controlled trial of photodynamic therapy using low dose 5 aminolevulinic acid activated by red or green light for high grade dysplasia in Barrett's esophagus [abstract]. Gastroenterology. 2005, 128: A238-10.1053/j.gastro.2004.11.026.
Peters F, Kara M, Rosmolen W, Aalders M, ten KF, Krishnadath K, van LJ, Fockens P, Bergman J: Poor results of 5-aminolevulinic acid-photodynamic therapy for residual high-grade dysplasia and early cancer in barrett esophagus after endoscopic resection. Endoscopy. 2005, 37: 418-424. 10.1055/s-2005-861198.
van Hillegersberg R, Haringsma J, Ten Kate FJ, Tytgat GN, van Lanschot JJ: Invasive carcinoma after endoscopic ablative therapy for high-grade dysplasia in Barrett's oesophagus. Dig Surg. 2003, 20: 440-444. 10.1159/000072713.
Barr H, Shepherd NA, Dix A, Roberts DJ, Tan WC, Krasner N: Eradication of high-grade dysplasia in columnar-lined (Barrett's) oesophagus by photodynamic therapy with endogenously generated protoporphyrin IX. Lancet. 1996, 348: 584-585. 10.1016/S0140-6736(96)03054-1.
Gossner L, Stolte M, Sroka R, Rick K, May A, Hahn EG, Ell C: Photodynamic ablation of high-grade dysplasia and early cancer in Barrett's esophagus by means of 5-aminolevulinic acid. Gastroenterology. 1998, 114: 448-455. 10.1016/S0016-5085(98)70527-X.
Gossner L, May A, Sroka R, Ell C: A new long-range through-the-scope balloon applicator for photodynamic therapy in the esophagus and cardia. Endoscopy. 1999, 31: 370-376. 10.1055/s-1999-31.
Kashtan H, Umansky M, Birkenfeld S, Scherubl H, Haddad R, Greenberg R, Konikoff F: Photodynamic therapy of Barrett's esophagus with dysplasia using systemic aminolevulinic acid and a non-laser light source. A phase I/II study. Gastrointestinal Oncology. 2002, 4: 153-157. 10.1080/1475956021000017020.
Mackenzie GD, Dunn JM, Novelli MR, Mosse S, Thorpe SM, Bown SG, Lovat LB: Preliminary results of a randomised controlled trial into the safety and efficacy of ALA versus photofrin photodynamic therapy for high grade dysplasia in Barrett's oesophagus [abstract]. Gut. 2008, 57: A14-
Macrae FA, Rajesekaram R, Thomas R, Bhathal PS: Photodynamic therapy in high grade dysplasia in Barrett's oesophagus using 5 amino-laevulinic acid sensitization [abstract]. Gastrointest Endosc. 2004, 59: P252-10.1016/S0016-5107(04)01128-9.
Mellidez JC, Mackenzie G, Selvasekar C, Novelli M, Thorpe S, Mosse C, Bown S, Lovat L: Reversal of Barrett's esophagus following photodynamic therapy using high dose 5 aminolevulinic acid activated by red or green laser light [abstract]. Gastroenterology. 2005, 128: A239-10.1053/j.gastro.2004.11.027.
Laukka MA, Wang KK: Initial results using low-dose photodynamic therapy in the treatment of Barrett's esophagus. Gastrointest Endosc. 1995, 42: 59-63. 10.1016/S0016-5107(95)70245-8.
Wang KK, Wongkeesong LM, Nourbakhsh A, Laukka M, Gutta K, Geller A, Balm R: Controlled trial of low dose photodynamic therapy for Barrett's esophagus [abstract]. Gastroenterology. 1997, 112: A676-
Wang KK, Nijhawan P, Nourbakhsh A, Lutzke L, WongKeeSong M, Anderson M: Does residual Barrett's esophagus progress after photodynamic therapy? [abstract]. Gastroenterology. 1999, 116: A348-
Javaid B, Watt P, Krasner N: Photodynamic therapy (PDT) for oesophageal dysplasia and early carcinoma with mTHPC (m-tetrahydroxyphenyl chlorin): a preliminary study. Lasers Med Sci. 2002, 17: 51-56. 10.1007/s10103-002-8266-5.
Lovat LB, Jamieson NF, Novelli MR, Mosse CA, Selvasekar C, Mackenzie GD, Thorpe SM, Bown SG: Photodynamic therapy with m-tetrahydroxyphenyl chlorin for high-grade dysplasia and early cancer in Barrett's columnar lined esophagus. Gastrointest Endosc. 2005, 62: 617-623. 10.1016/j.gie.2005.04.043.
Attila T, Kortan P, Kandel GT, Marcon N: Photodynamic therapy (PDT) for Barrett's esophagus with high grade dysplasia (BE-HGD) [abstract]. Gastrointest Endosc. 2005, 61: AB127-10.1016/S0016-5107(05)00760-1.
Bronner M, Taylor S, Overholt B, Wang K, Burdick S, Lightdale C, Kimmey M, Nava H, Sivak M, Nishioka N, et al: Squamous overgrowth in a 5-year randomized phase III trial of photodynamic therapy using porfirmer sodium in ablation of high-grade dysplasia in Barrett's esophagus [abstract]. Gastroenterology. 2006, 130: A121-
Keeley SB, Pennathur A, Gooding W, Landreneau RJ, Christie NA, Luketich J: Photodynamic therapy with curative intent for Barrett's esophagus with high grade dysplasia and superficial esophageal cancer. Ann Surg Oncol. 2007, 14: 2406-2410. 10.1245/s10434-007-9392-x.
Overholt BF, Wang KK, Burdick JS, Lightdale CJ, Kimmey M, Nava HR, Sivak MV, Nishioka N, Barr H, Marcon N, et al: Five-year efficacy and safety of photodynamic therapy with Photofrin in Barrett's high-grade dysplasia. Gastrointest Endosc. 2007, 66: 460-468. 10.1016/j.gie.2006.12.037.
Overholt BF, Panjehpour M, Halberg DL: Photodynamic therapy for Barrett's esophagus with dysplasia and/or early stage carcinoma: long-term results. Gastrointest Endosc. 2003, 58: 183-188. 10.1067/mge.2003.327.
Overholt BF, Panjehpour M, Ayres M: Photodynamic therapy for Barrett's esophagus: cardiac effects. Lasers Surg Med. 1997, 21: 317-320. 10.1002/(SICI)1096-9101(1997)21:4<317::AID-LSM2>3.0.CO;2-T.
Weiss AA, Wiesinger HAR, Owen D: Photodynamic therapy in Barrett's esophagus: Results of treatment of 17 patients. Can J Gastroenterol. 2006, 20: 261-264.
Wolfsen HC, Hemminger LL, Wallace MB, DeVault KR: Clinical experience of patients undergoing photodynamic therapy for Barrett's dysplasia or cancer. Aliment Pharmacol Ther. 2004, 20: 1125-1131. 10.1111/j.1365-2036.2004.02209.x.
Yachimski P, Puricelli WP, Nishioka NS: Patient predictors of esophageal stricture development after photodynamic therapy. Clin Gastroenterol Hepatol. 2008, 6: 302-308. 10.1016/j.cgh.2007.12.001.
Thomas T, Richards CJ, de Caestecker JS, Robinson RJ: High-grade dysplasia in Barrett's oesophagus: natural history and review of clinical practice. Aliment Pharmacol Ther. 2005, 21: 747-755. 10.1111/j.1365-2036.2005.02401.x.
Attwood SE, Lewis CJ, Caplin S, Hemming K, Armstrong G: Argon beam plasma coagulation as therapy for high-grade dysplasia in Barrett's esophagus. Clin Gastroenterol Hepatol. 2003, 1: 258-263. 10.1016/S1542-3565(03)00128-9.
Basu KK: Effects of low-power argon plasma coagulation thermoablation of Barrett's epithelium on oesophageal motility. Eur J Gastroenterol Hepatol. 2006, 18: 733-737. 10.1097/01.meg.0000216928.91618.9a.
Brand B, Porthun M, von Schrenck T, Matsui U, Bohnacker S, Jackle S, Thonke F, Seitz U, Soehendra N: Endoscopic Argonplasma coagulation for eradication of Barett's epithelium. Zentralbl Chir. 2000, 125: 437-442.
Bright T, Watson DI, Tam W, Game PA, Astill D, Ackroyd R, Wijnhoven BP, Devitt PG, Schoeman MN: Randomized trial of argon plasma coagulation versus endoscopic surveillance for barrett esophagus after antireflux surgery: late results. Ann Surg. 2007, 246: 1016-1020. 10.1097/SLA.0b013e318133fa85.
Dumoulin FL, Terjung B, Neubrand M, Scheurlen C, Fischer HP, Sauerbruch T: Treatment of Barrett's esophagus by endoscopic argon plasma coagulation. Endoscopy. 1997, 29: 751-753. 10.1055/s-2007-1004302.
Familiari L: Endoscopic treatment of Barrett's epithelium with Argon Plasma Coagulation. Long-term follow-up. Minerva Gastroenterol Dietol. 2003, 49: 63-70.
Ferraris R, Fracchia M, Foti M, Sidoli L, Taraglio S, Vigano' L, Giaccone C, Rebecchi F, Meineri G, Senore C, et al: Barrett's oesophagus: long-term follow-up after complete ablation with argon plasma coagulation and the factors that determine its recurrence. Aliment Pharmacol Ther. 2007, 25: 835-840. 10.1111/j.1365-2036.2007.03251.x.
Formentini A: Treatment of Barrett's esophagus with argon plasma coagulation and antireflux surgery. A retrospective analysis. Hepato-Gastroenterology. 2007, 54: 1991-1996.
Grade AJ, Shah IA, Medlin SM, Ramirez FC: The efficacy and safety of argon plasma coagulation therapy in Barrett's esophagus. Gastrointest Endosc. 1999, 50: 18-22. 10.1016/S0016-5107(99)70338-X.
Madisch A, Miehlke S, Bayerdorffer E, Wiedemann B, Antos D, Sievert A, Vieth M, Stolte M, Schulz H: Long-term follow-up after complete ablation of Barrett's esophagus with argon plasma coagulation. World J Gastroenterol. 2005, 11: 1182-1186.
Manner H, May A, Rabenstein T, Pech O, Nachbar L, Enderle MD, Gossner L, Ell C: Prospective evaluation of a new high-power argon plasma coagulation system (hp-APC) in therapeutic gastrointestinal endoscopy. Scand J Gastroenterol. 2007, 42: 397-405. 10.1080/00365520600898130.
Manner H, May A, Faerber M, Rabenstein T, Ell C: Safety and efficacy of a new high power argon plasma coagulation system (hp-APC) in lesions of the upper gastrointestinal tract. Dig Liver Dis. 2006, 38: 471-478. 10.1016/j.dld.2006.03.022.
Pedrazzani C, Catalano F, Festini M, Zerman G, Tomezzoli A, Ruzzenente A, Guglielmi A, de MG: Endoscopic ablation of Barrett's esophagus using high power setting argon plasma coagulation: a prospective study. World J Gastroenterol. 2005, 11: 1872-1875.
Pereira-Lima JC, Busnello JV, Saul C, Toneloto EB, Lopes CV, Rynkowski CB, Blaya C: High power setting argon plasma coagulation for the eradication of Barrett's esophagus. Am J Gastroenterol. 2000, 95: 1661-1668. 10.1111/j.1572-0241.2000.02197.x.
Pinotti AC, Cecconello I, Filho FM, Sakai P, Gama-Rodrigues JJ, Pinotti HW: Endoscopic ablation of Barrett's esophagus using argon plasma coagulation: a prospective study after fundoplication. Dis Esophagus. 2004, 17: 243-246. 10.1111/j.1442-2050.2004.00415.x.
Tigges H, Fuchs KH, Maroske J, Fein M, Freys SM, Muller J, Thiede A: Combination of endoscopic argon plasma coagulation and antireflux surgery for treatment of Barrett's esophagus. J Gastrointest Surg. 2001, 5: 251-259. 10.1016/S1091-255X(01)80045-7.
Van Laethem JL, Jagodzinski R, Peny MO, Cremer M, Deviere J: Argon plasma coagulation in the treatment of Barrett's high-grade dysplasia and in situ adenocarcinoma. Endoscopy. 2001, 33: 257-261. 10.1055/s-2001-12803.
Van Laethem JL, Cremer M, Peny MO, Delhaye M, Deviere J: Eradication of Barrett's mucosa with argon plasma coagulation and acid suppression: immediate and mid term results. Gut. 1998, 43: 747-751. 10.1136/gut.43.6.747.
Dumot JA, Vargo JJ, Zuccaro G, Falk GW, Frey L, Rice T: Results of cryospray ablation for esophageal high grade dysplasia (HGD) and intramucosal cancer (Imca) in high risk non-surgical patients [abstract]. Digestive Disease Week. 2008, M1304-
Johnston MH: Cryoablation of Barrett's esophagus: A pilot study. Gastrointest Endosc. 2005, 62: 842-848. 10.1016/j.gie.2005.05.008.
Wolfsen HC, Hemminger LL, Raimondo M, Woodward TA: Photodynamic therapy and endoscopic mucosal resection for Barrett's dysplasia and early esophageal adenocarcinoma. South Med J. 2004, 97: 827-830. 10.1097/01.SMJ.0000136265.34296.62.
Michopoulos S, Tsibouris P, Bouzakis H, Sotiropoulou M, Kralios N: Complete regression of Barrett's esophagus with heat probe thermocoagulation: mid-term results. Gastrointest Endosc. 1999, 50: 165-172. 10.1016/S0016-5107(99)70219-1.
Giovannini M, Bories E, Pesenti C, Moutardier V, Monges G, Danisi C, Lelong B, Delpero JR: Circumferential endoscopic mucosal resection in Barrett's esophagus with high-grade intraepithelial neoplasia or mucosal cancer. Preliminary results in 21 patients. Endoscopy. 2004, 36: 782-787. 10.1055/s-2004-825813.
Mino-Kenudson M, Brugge WR, Puricelli WP, Nakatsuka LN, Nishioka NS, Zukerberg LR, Misdraji J, Lauwers GY: Management of superficial Barrett's epithelium-related neoplasms by endoscopic mucosal resection - Clinicopathologic analysis of 27 cases. Am J Surg Pathol. 2005, 29: 680-686. 10.1097/01.pas.0000154129.87219.fa.
Seewald S, Akaraviputh T, Seitz U, Brand B, Groth S, Mendoza G, He XK, Thonke F, Stolte M, Schroeder S, et al: Circumferential EMR and complete removal of Barrett's epithelium: a new approach to management of Barrett's esophagus containing high-grade intraepithelial neoplasia and intramucosal carcinoma. Gastrointest Endosc. 2003, 57: 854-859. 10.1016/S0016-5107(03)70020-0.
Tang SJ, Tang L, Jazrawi SF: Circumferential endoscopic mucosal resection of a 14-cm Barrett's dysplasia with the Duette mucosectomy device (with videos). Gastrointest Endosc. 2008, 68: 786-789. 10.1016/j.gie.2008.01.018.
Barham CP, Jones RL, Biddlestone LR, Hardwick RH, Shepherd NA, Barr H: Photothermal laser ablation of Barrett's oesophagus: endoscopic and histological evidence of squamous re-epithelialisation. Gut. 1997, 41: 281-284. 10.1136/gut.41.3.281.
Bonavina L, Ceriani C, Carazzone A, Segalin A, Ferrero S, Peracchia A: Endoscopic laser ablation of nondysplastic Barrett's epithelium: Is it worthwhile?. J Gastrointest Surg. 1999, 3: 194-198. 10.1016/S1091-255X(99)80033-X.
Bowers SP, Mattar SG, Waring PJ, Galloway K, Nasir A, Pascal R, Hunter JG: KTP laser ablation of Barrett's esophagus after anti-reflux surgery results in long-term loss of intestinal metaplasia. Potassium-titanyl-phosphate. Surg Endosc. 2003, 17: 49-54. 10.1007/s00464-001-8155-1.
Ertan A, Zimmerman M, Younes M: Esophageal adenocarcinoma associated with Barretts esophagus - long-term management with laser-ablation. Am J Gastroenterol. 1995, 90: 2201-2203.
Norberto L, Polese L, Angriman I, Erroi F, Cecchetto A, D'Amico DF: High-energy laser therapy of Barrett's esophagus: Preliminary results. World J Surg. 2004, 28: 350-354. 10.1007/s00268-003-7332-x.
Salo JA, Salminen JT, Kiviluoto TA, Nemlander AT, Ramo OJ, Farkkila MA, Kivilaakso EO, Mattila SP: Treatment of Barrett's esophagus by endoscopic laser ablation and antireflux surgery. Ann Surg. 1998, 227: 40-44. 10.1097/00000658-199801000-00006.
Faigel DO, Lieberman DA, Weinstein WM, Fanning S, Fennerty MB, Sampliner RB: Effect of multipolar electrocoagulation on EUS findings in Barrett's esophagus. Gastrointest Endosc. 2002, 55: 23-26. 10.1067/mge.2002.120100.
Kovacs BJ, Chen YK, Lewis TD, DeGuzman LJ, Thompson KS: Successful reversal of Barrett's esophagus with multipolar electrocoagulation despite inadequate acid suppression. Gastrointest Endosc. 1999, 49: 547-553. 10.1016/S0016-5107(99)70380-9.
Montes CG, Brandalise NA, Deliza R, de Magalhaes AFN, Ferraz JGP: Antireflux surgery followed by bipolar electrocoagulation in the treatment of Barrett's esophagus. Gastrointest Endosc. 1999, 50: 173-177. 10.1016/S0016-5107(99)70220-8.
Sampliner RE, Fennerty B, Garewal HS: Reversal of Barrett's esophagus with acid suppression and multipolar electrocoagulation: Preliminary results. Gastrointest Endosc. 1996, 44: 532-535. 10.1016/S0016-5107(96)70004-4.
Bumgarner JM, Panjehpour M, Long M, Dellon ES, Overholt BF, Shaheen NJ: Comparison of catheter-based radiofrequency ablation and photodynamic therapy for Barrett's esophagus [abstract]. Gastroenterology. 2008, 134: A436-10.1016/S0016-5085(08)62035-1.
Eldaif SM, Lin E, Singh KA, Force SD, Miller DL: Radiofrequency ablation of Barrett's esophagus: short-term results. Ann Thorac Surg. 2009, 87: 405-410. 10.1016/j.athoracsur.2008.11.043.
Fleischer DE, Overholt BF, Sharma VK, Reymunde A, Kimmey MB, Chuttani R, Chang KJ, Lightdale CJ, Santiago N, Pleskow DK, et al: Endoscopic ablation of Barrett's esophagus: a multicenter study with 2.5-year follow-up. Gastrointest Endosc. 2008, 68: 867-876. 10.1016/j.gie.2008.03.008.
Ganz RA, Overholt BF, Sharma VK, Fleischer DE, Shaheen NJ, Lightdale CJ, Freeman SR, Pruitt RE, Urayama SM, Gress F, et al: Circumferential ablation of Barrett's esophagus that contains high-grade dysplasia: a U.S. Multicenter Registry. Gastrointest Endosc. 2008, 68: 35-40. 10.1016/j.gie.2007.12.015.
Hernandez JC, Reicher S, Chung D, Pham BV, Tsai F, Disibio G, French S, Eysselein VE: Pilot series of radiofrequency ablation of Barrett's esophagus with or without neoplasia. Endoscopy. 2008, 40: 388-392. 10.1055/s-2007-995747.
Hubbard N, Velanovich V: Endoscopic endoluminal radiofrequency ablation of Barrett's esophagus in patients with fundoplications. Surg Endosc. 2007, 21: 625-628. 10.1007/s00464-007-9199-7.
Pouw RE, Gondrie JJ, Sondermeijer CM, Ten Kate FJ, van Gulik TM, Krishnadath KK, Fockens P, Weusten BL, Bergman JJ: Eradication of Barrett esophagus with early neoplasia by radiofrequency ablation, with or without endoscopic resection. J Gastrointest Surg. 2008, 12: 1627-1636. 10.1007/s11605-008-0629-1.
Roorda AK, Marcus SN, Triadafilopoulos G: Early experience with radiofrequency energy ablation therapy for Barrett's esophagus with and without dysplasia. Dis Esophagus. 2007, 20: 516-522. 10.1111/j.1442-2050.2007.00728.x.
Sharma VK, Wang KK, Overholt BF, Lightdale CJ, Fennerty MB, Dean PJ, Pleskow DK, Chuttani R, Reymunde A, Santiago N, et al: Balloon-based, circumferential, endoscopic radiofrequency ablation of Barrett's esophagus: 1-year follow-up of 100 patients. Gastrointest Endosc. 2007, 65: 185-195. 10.1016/j.gie.2006.09.033.
Smith CD, Bejarano PA, Melvin WS, Patti MG, Muthusamy R, Dunkin BJ: Endoscopic ablation of intestinal metaplasia containing high-grade dysplasia in esophagectomy patients using a balloon-based ablation system. Surg Endosc. 2007, 21: 560-569. 10.1007/s00464-006-9053-3.
Sharma VK, Jae KH, Das A, Wells CD, Nguyen CC, Fleischer DE: Circumferential and focal ablation of Barrett's esophagus containing dysplasia. Am J Gastroenterol. 2009, 104: 310-317. 10.1038/ajg.2008.142.
Vassiliou MC, von RD, Wiener DC, Gordon SR, Rothstein RI: Treatment of ultralong-segment Barrett's using focal and balloon-based radiofrequency ablation. Surg Endosc. 2009
Velanovich V: Endoscopic endoluminal radiofrequency ablation of Barrett's esophagus: initial results and lessons learned. Surg Endosc. 2009, 23: 2175-2180. 10.1007/s00464-009-0364-z.
Gondrie JJ, Pouw RE, Sondermeijer CMT, Peters FP, Curvers WL, Rosmolen WD, Krishnadath KK, Ten Kate F, Fockens P, Bergman JJ: Stepwise circumferential and focal ablation of Barrett's esophagus with high-grade dysplasia: results of the first prospective series of 11 patients. Endoscopy. 2008, 40: 359-369. 10.1055/s-2007-995567.
Gondrie JJ, Pouw RE, Sondermeijer CM, Peters FP, Curvers WL, Rosmolen WD, ten KF, Fockens P, Bergman JJ: Effective treatment of early Barrett's neoplasia with stepwise circumferential and focal ablation using the HALO system. Endoscopy. 2008, 40: 370-379. 10.1055/s-2007-995589.
Ferguson MK, Naunheim KS: Resection for Barrett's mucosa with high-grade dysplasia: implications for prophylactic photodynamic therapy. J Thorac Cardiovasc Surg. 1997, 114: 824-829. 10.1016/S0022-5223(97)70087-4.
Nguyen NT, Schauer P, Luketich JD: Minimally invasive esophagectomy for Barrett's esophagus with high-grade dysplasia. Surgery. 2000, 127: 284-290. 10.1067/msy.2000.103489.
Romagnoli R: Outcomes of dysplasia arising in Barrett's esophagus: A dynamic view. J Am Coll Surg. 2003, 197: 365-371. 10.1016/S1072-7515(03)00417-4.
Sujendran V, Sica G, Warren B, Maynard N: Oesophagectomy remains the gold standard for treatment of high-grade dysplasia in Barrett's oesophagus. Eur J Cardiothorac Surg. 2005, 28: 763-766. 10.1016/j.ejcts.2005.08.018.
Thomson BNJ, Cade RJ: Oesophagectomy for early adenocarcinoma and dysplasia arising in Barrett's oesophagus. ANZ J Surg. 2003, 73: 121-124. 10.1046/j.1445-2197.2003.02646.x.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-230X/10/111/prepub
Acknowledgements
This study was made possible through a financial contribution from Alberta Health and Wellness and under the auspices of the Alberta Health Technologies Decision Process initiative: the Alberta model for health technology assessment and policy analysis. The views expressed herein do not necessarily represent the official policy of Alberta Health and Wellness. The authors would like to thank Leigh-Ann Topfer for conducting the literature searches and editing the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
CW was the recipient of a one time clinical implementation grant from Axcan in 2007, and has given educational talks funded through unrestricted grants from Axcan. The remaining author(s) declare that they have no competing interests
Authors' contributions
DM and CW made substantial contributions to the conception and design of the study, to interpretation of the data, and have reviewed and revised the manuscript for important intellectual and clinical content. TS made a substantial contribution to the conception and design of the study, interpretation of data, and was involved in writing and critically reviewing drafts of the manuscript. HW was involved in the acquisition, analysis and interpretation of the data and making major revisions to draft manuscripts. DL was involved in the conception and design of the study, acquisition and analysis of data and drafting the manuscript. All authors have given approval for submission of this version.
Electronic supplementary material
12876_2010_502_MOESM1_ESM.DOC
Additional file 1: Studies of photodynamic therapy (PDT) for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of PDT for BE with/without dysplasia are presented in Additional file 1. (DOC 361 KB)
12876_2010_502_MOESM2_ESM.DOC
Additional file 2: Studies of argon plasma coagulation (APC) for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of APC for BE with/without dysplasia are presented in Additional file 2. (DOC 264 KB)
12876_2010_502_MOESM3_ESM.DOC
Additional file 3: Studies of cryoablation, combined endoscopic mucosal resection (EMR) and photodynamic therapy (PDT), and thermocoagulation for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of cryoablation, combined EMR and PDT, and thermocoagulation for BE with/without dysplasia are presented in Additional file 3. (DOC 96 KB)
12876_2010_502_MOESM4_ESM.DOC
Additional file 4: Studies of endoscopic mucosal resection (EMR) for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of EMR for BE with/without dysplasia are presented in Additional file 4. (DOC 101 KB)
12876_2010_502_MOESM5_ESM.DOC
Additional file 5: Studies of laser ablation for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of laser ablation for BE with/without dysplasia are presented in Additional file 5. (DOC 102 KB)
12876_2010_502_MOESM6_ESM.DOC
Additional file 6: Studies of multipolar electrocoaguation (MPEC) for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of MPEC for BE with/without dysplasia are presented in Additional file 6. (DOC 104 KB)
12876_2010_502_MOESM7_ESM.DOC
Additional file 7: Studies of radiofrequency ablation (RFA) for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of RFA for BE with/without dysplasia are presented in Additional file 7. (DOC 194 KB)
12876_2010_502_MOESM8_ESM.DOC
Additional file 8: Studies of esophagectomy for Barrett's esophagus with/without dysplasia. Details of study and patient characteristics, outcomes and study quality of the included studies of esophagectomy for BE with/without dysplasia are presented in Additional file 8. (DOC 124 KB)
12876_2010_502_MOESM9_ESM.DOC
Additional file 9: Studies of adverse events (endoscopic treatments). Adverse events reported for individual studies of endoscopic alternatives are presented in Additional file 9. (DOC 520 KB)
12876_2010_502_MOESM10_ESM.DOC
Additional file 10: Studies of complete eradication of Barrett's esophagus (endoscopic treatments). Values reported for the complete eradication of BE with endoscopic treatments are presented in Additional file 10. (DOC 428 KB)
12876_2010_502_MOESM11_ESM.DOC
Additional file 11: Studies of complete eradication of high grade dysplasia (endoscopic treatments). Values reported for the complete eradication of HGD with endoscopic treatments are presented in Additional file 11. (DOC 286 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Menon, D., Stafinski, T., Wu, H. et al. Endoscopic treatments for Barrett's esophagus: a systematic review of safety and effectiveness compared to esophagectomy. BMC Gastroenterol 10, 111 (2010). https://doi.org/10.1186/1471-230X-10-111
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-230X-10-111