
Abstract
Over the last decade, we have witnessed considerable progress in gender dysphoria (GD) terminology in an attempt to better describe the condition based on certain criteria. The ever-increasing social acceptance and destigmatization of children and adolescents with GD have resulted in an increased number of transgender individuals seeking endocrine care. In addition to terminology and diagnostic criteria, the tremendous progress of genetics and neuroimaging has enabled us to have a deeper understanding of the complex pathogenesis of GD. Although helpful guidelines for treatment with GnRH analogs and gender-affirming hormones have been proposed, several challenges and controversies still exist. In this article, the current knowledge about GD in adolescents is reviewed, with particular emphasis on terminology, clinical manifestations, and epidemiologic data. The neurobiological basis of the condition is presented, and both hormonal treatment and mental issues of transgender individuals are discussed. Undoubtedly, further research will optimize the diagnostic and therapeutic approach of children and adolescents with GD.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction to terminology in gender dysphoria
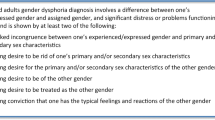
The past decade has witnessed a rapid evolution in gender dysphoria (GD) terminology, a disorder initially termed gender identity disorder, then gender dysphoria (DSM-V), and, most recently, gender incongruence (ICD-11). Gender incongruence is characterized by a marked and persistent incongruence between an individual’s experienced gender and the assigned sex. Gender variant behavior and preferences alone are not a basis for assigning the diagnosis in this group [1]. These changes in nomenclature reflect changes in how the condition is perceived within both the medical profession and the public domain. Expert professionals working in specialist centers have moved away from definitions relating to psychiatric disorders, which has aided demedicalizing individuals [2]. Currently, the term GD is most commonly used and refers to the distress that may accompany the incongruence between one’s experienced or expressed gender and one’s assigned sex at birth [3]. The terminology applied to gender dysphoria still remains confusing for non-specialists but continues to be a key to our understanding of the clinical presentation. Biological sex, gender identity, and gender presentation should be considered separately so as to best comprehend the whole.
Biological sex is determined by the karyotype (classically, either 46,XX in females or 46,XY in males) and the reproductive organs of the individual. Gender identity is the inner understanding and perception of oneself as a man or a woman or anything along the spectrum between them. Gender presentation is how we express our gender on the male to female scale. Additionally, gender presentation is influenced by culture and norms in society [4, 5]. The expected perception is that all three terms should be in agreement with one another in an individual; however, sometimes this expectation is not manifested in reality [6]. In GD, the person’s gender identity and biological sex are inconsistent, resulting in marked distress, which is heightened at onset of puberty and the associated development of secondary sex characteristics [3]. The distress can be so debilitating that it can hinder normal development and activities of daily living, often resulting in depression, suicidal ideation, and drug use. Access to treatment, including psychotherapy, hormones, and surgery, improves prognosis [4].
Clinical manifestations
Children may express a dislike of their sex characteristics and a desire for the characteristics of the experienced gender. Cross-dressing, cross-gender roles in plays, preference for toys and activities of the other gender, friends of the opposite gender, and rejection of cultural gender roles are all commonly reported and currently used as diagnostic criteria for GD [3, 7]. Difficulties in childhood often arise from social intolerance and resultant poor social relations with peers, as well as negative psychological outcome in children with GD [8]. A cross-national study carried out in Canada and the Netherlands in children with GD showed more emotional problems and poorer peer relations in the former country than in the latter. Good peer relations were of more importance than IQ, social status, marital status of parents, and ethnicity as predictors of positive emotional outcomes in children with GD [9].
Importantly, young children may or may not continue to identify themselves as transgender in adolescence and adulthood [10]. Indeed, gender incongruence will desist by early adolescence for the majority of them [11, 12]. Several studies have shown that the percentage of “persisters” lies between 10 and 39% [7, 13]. Therefore, medical treatment should be considered for those adolescents with GD that persists or even intensifies when Tanner breast or genital stage is 2 [14]. Steensma and collaborators have demonstrated that the critical time period for GD persistence or desistence is between the ages of 10 and 13 years [13]. Important factors that have been associated with persistence of GD in adolescence/adulthood include the severity of symptoms of GD; the persistence, insistence, and consistence of statements; and behaviors in childhood, as well as a strong tendency to report their gender [15].
In recent years, clinicians have seen an ever-increasing number of postpuberty cases of GD in birth-assigned females with rapid-onset clinical manifestations. This new phenomenon, termed “rapid-onset gender dysphoria” (ROGD), has been described by parents who have reported in online panels that their adolescents displayed a sudden or rapid onset of GD without having had a history of gender variance during childhood [16, 17]. Of note, clinical features suggestive of GD were observed in adolescents within a group of peers, with several members becoming gender dysphoric. In addition, adolescents with ROGD were characterized by an intense immersion in social media, suggesting an influence by peers and the Internet in triggering GD [16, 17]. Lisa Littman was the first to investigate ROGD in a systematic fashion, in 2018. Littman collected 256 parent-completed surveys, which showed that the majority of adolescents with ROGD were birth-assigned females (82.8%), with a mean age of 16.4 years. In addition, there was a high percentage of mental health disorders or neurodevelopmental disabilities, as well as several psychosocial stressors, which preceded the onset of GD. Furthermore, both mental health and the adolescent-parent relationship were worsened when GD “came out” [16]. Littman’s study received both supportive and non-supportive comments, leaving space for further future studies on this new clinical phenomenon [17,18,19,20].
Epidemiology of GD
The prevalence of GD according to published reports is highly variable. Several studies in children and adolescents have shown a prevalence of GD of between 1.2 and 2.7%, although a relatively high percentage of the participants answered that they did not understand the question [21,22,23]. In DSM-V, the prevalence in adulthood for birth-assigned males with GD ranges between 0.005 and 0.014% and for birth-assigned females with GD between 0.002 and 0.003%. These published prevalence rates are assumed to underestimate true prevalence, as there is ascertainment bias in how these data are collected due to the inclusion only of those individuals who seek treatment in a specialist center. Individuals will not be included if they do not seek treatment or if they receive treatment outside of a specialist center [3]. Self-reported prevalence rates of 0.5–1.3% have also been documented [10, 24].
There are geographical differences in the prevalence of gender dysphoria relating to cultural norms and differences in diagnostic criteria internationally [6]. In addition, there has been a significant increase in individuals with GD presenting to specialist clinics [17, 25,26,27]. Over the last 6 years, the rate of individuals seeking reassignment has risen by 18% per year (95% CI 1.08–1.30). Moreover, the age of help-seeking is younger. Several explanations have been proposed, including increase in population prevalence, change in help-seeking behavior, raised public awareness along with increased media presentation, the Internet as a source of information and support system, LGBTQ support groups, campaigns for transsexual rights, reduced discrimination, greater awareness of GD among health professionals, and advances in understanding the cause of GD [28].
In addition to these epidemiological changes, there has been a shift in the sex ratio among individuals with GD. In 2015, Aitken and collaborators found that the birth-assigned males to birth-assigned females ratio was 2.11:1 for the years 1999–2005 in Toronto, whereas the sex ratio changed to 1:1.76 from 2006 to 2013 [29]. Most of the subsequent studies have demonstrated a clear shift in the sex ratio favoring birth-assigned females [26, 27, 30, 31]. However, since the “true prevalence” of GD is unknown, safe conclusions cannot as yet be extracted.
Nevertheless, it is clear that the number of children and adolescents with GD who seek professional help is rising and the age of presentation is decreasing. Taking into account the growing numbers, there is a need for further research into the etiology of GD, the determination of which is highly likely to improve health outcomes among GD individuals [32].
The neurobiological basis of GD
The possible etiologies of GD have been investigated by studies in several areas: structural neuroanatomy, functional neuroimaging, genetics, and exposure to prenatal androgens (Fig. 1). However, a possible limitation of the studies performed so far might be the small number of participants. Furthermore, in some studies, the subjects were considered as homogenous, whereas young people with GD may belong to multiple subgroups [33]. It is also possible that all the etiologic factors discussed below are interconnected. For example, brain structure and functionality might be related to prenatal androgen exposure, while genes can influence neuroanatomy. The studies presented below show that GD does not concern psychological functioning alone but is a complex interaction of different variables, such as neuroanatomy, genes, and hormones [34].

The complex neurobiological basis of GD. AR, androgen receptor; BSTc, bed nucleus of stria terminalis; ERα, estrogen receptor alpha; ERβ, estrogen receptor beta; CYP19, aromatase cytochrome P450; INAH, interstitial nucleus of the anterior hypothalamus; MRNs, mental rotation networks; RSNs, resting state networks; RYR3, ryanodine receptor 3; WMNs, working memory networks
Structural neuroanatomy
Studies in structural neuroanatomy or functional neuroimaging comparing cisgender and transgender individuals have been inconclusive with often conflicting results.
Several areas in the brain have been postulated to show differences between individuals with and without GD, including the bed nucleus of the stria terminalis, the hypothalamic uncinate nucleus, kisspeptin-expressing neurons, and the putamen. The bed nucleus of the stria terminalis (BSTc) differs between cis-males, cis-females, and trans-females (Fig. 2), whereas the BSTc was of similar size and had similar neuronal numbers in trans-females and in cis-females [35]. The BSTc is innervated by somatostatin-expressing neurons, of which cis-females have similar numbers to those of trans-females, while cis-men had almost twice as many somatostatin neurons as cis-women. Trans-males had similar neuron numbers to those of cis-men. Hormone therapy in adulthood had no influence on neuron numbers [36].

Localization of the bed nucleus of the stria terminalis
The hypothalamic uncinate nucleus is composed of several subnuclei of which the interstitial nucleus of the anterior hypothalamus 3 (INAH3) and 4 (INAH4) were found to have sex dimorphism (Fig. 3) [33]. INAH3 was larger in volume and in neuron number in cis-males compared to cis-females. In trans-females, both the volume and number of neurons in INAH3 were similar to cis-female subjects, and, conversely, the trans-males had similar INAH3 volume and number of neurons compared to the cis-males. Since treatment with testosterone in trans-males had been discontinued 3 years prior to the sampling, it was inferred that the similarity to the INAH3 in cis-males was not a consequence of the acute activating effect of androgens [33]. Taking into account that no difference was found in INAH3 volume and number of neurons between pre- and postmenopausal cis-females, the authors speculated that estrogen treatment in trans-females would have no effect on the presentation of their INAH3. The authors concluded that this sex reversal of the INAH3 in transgender subjects could be partly a marker of an early dysfunction in sex differentiation of the brain [33]. In the same study, the shape and size of the INAH4 were investigated. In cis-male subjects and in trans-males who received testosterone, the INAH4 was elongated, whereas it is spherical in cis-female subjects [33]. Further studies are required to elucidate the role of the alterations of the INAH4 in GD.

Localization of INAH 3 and INAH 4. INAH, interstitial nucleus of the anterior hypothalamus
In addition to BSTc, INAH3, and INAH4, research has focused on the role of the hypothalamic kisspeptin system in transgender individuals. Taziaux and collaborators studied kisspeptin expression in the infundibular nucleus of postmortem hypothalamic tissues [37]. They found that the number of kisspeptin-expressing neurons was similar in cisgender females and transgender females, as well as in cisgender males and transgender males, suggesting that the brain sex (represented by kisspeptin neurons) and the body sex features can develop in opposing directions [37].
The putamen has also been proposed as a region of the brain showing sex dimorphism. A study including 24 transgender females, 30 cisgender males, and 30 cisgender females who underwent magnetic resonance imaging (MRI) showed that the volume of gray matter in transgender females was mostly similar to that of the cis-male group. However, the putamen in trans-females was found to be larger than that of cis-males and within the expected volume of cis-female subjects. The transgender group had not received any hormone therapy prior to the study, indicating that exogenous hormones could not be the reason for the difference [38]. In another study, 12 transgender females, prior to hormonal therapy, were examined using a positron emission tomography scan and were found to have different activation in the left putamen from that of a cis-male subject when smelling odorous steroids [39].
Challenging the above studies, a study published in 2011 inspected the gray and white matter, hemispheric asymmetry, and volume of the hippocampus, thalamus, caudate, and putamen, concluding that the brain of transgender females is structurally similar to that of cisgender males. Furthermore, there was an asymmetry of the right hemisphere volume that was detected both in cis-males and in trans-females, while there was symmetry between the two hemispheres in cis-females. The study, however, found a difference in putamen and thalamus volumes, which were smaller in the trans-females compared to the cis-male and cis-female groups. The authors suggested that gender dysphoria may relate to a network of changes and not to a single structure dimorphism [40].
Functional neuroimaging
Functional resting state networks have been studied, and differences have been found in individuals with GD. In one study, the resting state functional magnetic resonance was measured in both transgender male and transgender female subjects during GnRH agonist therapy and again 4 months after gender-affirming hormone therapy, and was compared to cisgender female and cisgender male control groups. In the working memory network, cis-males had greater functional connectivity (FC) than cis-females in the right caudate nucleus. There was no difference between the two transgender groups. The addition of gender-affirming hormone therapy or circulating endogenous sex steroids did not affect FC. It was concluded that cis-females and cis-males have a difference in the right working memory network, but this difference is smaller in transgender individuals [41].
In addition, functional MRI has been used to explore the FC patterns of resting state networks in the brain of prepubertal and adolescents with gender dysphoria and non-gender dysphoric peers. In the networks tested, there were GD-specific and sex-atypical patterns in adolescents with GD. However, these differences in FC were not found in prepubertal children with GD, which may indicate that the differences arise in puberty [42].
Functional MRI has also been used to show differences in a group of transgender females before and after gender-affirming hormone therapy, compared to cisgender male controls. Schöning and collaborators studied the patterns of brain activation associated with a mental rotation task in 11 transgender females before receiving gender-affirming hormone therapy, and 11 transgender females during hormone therapy, compared to cisgender men [43]. Functional MRI showed that the mental rotation network was activated in all groups; however, cis-males showed higher activation in the left parietal cortex, where both transgender groups displayed stronger activation in the temporo-occipital regions [43]. According to the authors of the study, these results show that differences between cisgender men and transgender individuals exist a priori and remain stable during hormonal treatment.
Genetics
The role of genetics in the etiology of GD has been investigated through family or twin studies and associations between GD and specific mutations or polymorphisms in genes related mostly to sex hormones.
Almost 20 years ago, Green suggested that genes may have a role in the etiology of GD in families in which there is co-occurrence [44]. In his study, 10 sets of siblings or parent-child pairs with GD were described, indicating that a genetic factor might be involved in GD in such cases [44]. A subsequent study investigating the familial occurrence of GD in non-twin siblings showed that siblings of a transgender subject have a very low possibility of also having GD [45]. To explore the genetic role even more closely, a concordance rate for GD in either monozygotic or dizygotic twins was established [46, 47]. In both studies, the frequency of concordance of GD was much higher in the monozygotic twin group than in the dizygotic twins, suggesting a role of genetic factors in GD.
Although most studies found minimal clinical utility of (molecular) karyotype in the work-up of children and adolescents with GD [48, 49], a recent cytogenetic analysis of karyotypes in 444 transgender females and 273 transgender males in Spain demonstrated a five times higher incidence of cytogenetic alterations in individuals with GD compared to the general population [50], whereas a study of a similar number of adolescents found no increase in karyotype variations [27]. Using G-banding and high-resolution microarrays, the authors found a significantly high frequency of Klinefelter syndrome and a 17q21.31 microduplication of 572 Kb, which included the KANSL1 gene [50]. Future studies are needed to shed light on the role of cytogenetic defects in the pathogenesis of GD.
Assuming that GD is a consequence of altered sex differentiation of the brain, it is worth considering which factors might play a role in early brain development [51]. Animal experiments have shown the influence of testosterone on sex dimorphism in fetal brain development, leading investigators to postulate that this effect could be mediated via the androgen receptor (AR) or estrogen receptor (ER) [52]. Three polymorphisms were investigated for their role in the development of GD among 29 transgender females and 229 cisgender male controls, namely, CAG repeat sequence in the first exon of the AR gene, tetra nucleotide repeat polymorphism in intron 4 of the aromatase gene, and CA repeat polymorphism in intron 5 of the ERβ gene. The only difference found was the mean length of ERβ repeat. There was a partial effect for all three polymorphisms and an effect of the interaction between AR and aromatase gene polymorphisms on the occurrence of GD. Less active AR enhanced the occurrence of GD, as occurs in complete androgen insensitivity syndrome in which individuals identify as females [53].
In a similar study, investigators studied the link between the development of GD in transgender females and gene variants known to be related to under-masculinization or feminization [54]. CAG repeat length in the AR gene, CA repeat length in the ERβ gene, and TTTA repeat length in the CYP19 gene were tested in 112 transgender females and 258 cisgender male controls. In the transgender group, the AR repeat length was longer than in the control group. The AR repeat length is known to be associated with a weaker affinity of AR to testosterone during development [55, 56]. In contradiction to the previous study, no effect of the interaction due to the length of the three genes on GD was found; however, the study also supports the role of AR gene in GD. Additional large studies aiming to find polymorphisms in candidate sex hormone-related genes, encoding androgen receptor (AR), estrogen receptors alpha (ERα) and beta (ERβ), aromatase (CYP19), and progesterone receptor (PR) have failed to show any genetic relation to GD susceptibility [57, 58].
Similarly, studies in transgender male individuals have attempted to identify a role for the sex hormone-related genes ERβ, AR, and CYP19A1 on the development of GD in transgender males. A sample of 273 transgender males and 371 cisgender female controls was tested for the CA repeats in intron 5 of ERβ, the CAG repeats in exon 1 of AR, and the TTTA repeats in intron 4 of CYP19A1. The length of the ERβ gene was higher in the transgender group compared to the control group. The study also concluded that the chance of developing GD had a higher odds ratio, i.e., 2.001 [1.15–3.46] in the homozygote of long alleles. A possible mechanism might involve the fact that greater length might lead to increased transcription of the receptor. Subsequently, the higher activation might cause less feminization of the female brain [59].
So far, the evidence for a role of sex hormone-related genes is conflicting. This might result from the small sample groups and heterogeneity in the transgender population in terms of the onset of gender dysphoria (either before or after puberty) and their sexual orientation [60]. To investigate a more homogenous group, the AR, ERα, ERβ, and CYP19A1 genes were tested in a twofold subject control analysis: 549 transgender females were compared to 728 cis-males, while 425 transgender males were compared to 599 cis-females. In the transgender females, there was an interaction between ERβ and AR when one of these genes was short and the other was long. In the transgender males, there was a connection between the ERβ and ERα, but no interaction was found between these polymorphisms [60]. A recent study aimed to find an association between GD and genes that participate in sex hormone signaling [61]. To this end, 380 transgender women and 344 cisgender males were recruited for DNA genotyping for 12 sex hormone-signaling genes. The authors found an association between GD and several functional variants, suggesting that the link between the phenotype and sex hormone signaling might be oligogenic [61].
The tremendous progress made in biotechnology will undoubtedly uncover novel genetic factors in the complex pathogenesis of GD. Indeed, Yang and collaborators used whole-genome and whole-exome sequencing in nine transgender males and four transgender females, respectively [62]. They found three heterozygous damaging mutations in the RYR3 gene in unrelated transgender males but none in controls. This gene encodes a ryanodine receptor that functions as a calcium transporter from intracellular storage. Structural biology assays showed that one of these RYR3 mutations, p.1518R > H, produced the largest structural alteration in the expressed protein [62].
Exposure to prenatal androgens
Prenatal androgen exposure has been proposed as having a role in postnatal gender expression. Sex dimorphism in skeletal development (2D:4D finger ratio) has been used as a surrogate marker in postnatal life of prenatal exposure to androgens [63]. The 2D:4D finger ratio was studied in 96 birth-assigned male adults and 51 birth-assigned female adults with GD compared to 90 birth-assigned male adults and 112 birth-assigned female adults, as well as in 67 birth-assigned male children and 34 birth-assigned female children with GD compared to 74 birth-assigned male children and 72 birth-assigned female children without GD. In birth-assigned males, both adults and children, no difference was found between GD and controls in 2D:4D ratio. In birth-assigned females, there was a difference between GD and controls. The adult birth-assigned females with GD had a more masculine 2D:4D finger ratio compared to controls. This leads to the assumption that different hormone exposure contributes to GD in birth-assigned females [64]. However, when 56 GD patients (39 trans-females and 17 trans-males) were compared to 176 cis-men and 190 cis-women, right hand finger ratio in trans-females was different from that of cis-male subjects and similar to that of cis-female subjects. The authors suggested a possible effect of low prenatal exposure to testosterone on the development of GD in birth-assigned females, but failed to show a similar effect on the development of GD in birth-assigned males. [65]. These studies, although non-conclusive, suggested that there is a role of prenatal exposure to androgens in the development of GD. There is a need for further studies to support these results.
Clinical management
A child or young person with gender dysphoria should be referred to a specialist center with multidisciplinary support [26]. Multidisciplinary team (MDT) work for GD management has evolved due to the increasing complexity of diagnostic and treatment decision-making. An MDT approach aims to bring together the range of specialists required to discuss and agree treatment recommendations and ongoing management for individual patients. The multidisciplinary clinic should be comprised of pediatric and adult endocrinologists, clinical psychologists, psychiatrists, and nurse specialists. Treatment options are tailored to the individual but will be guided by the age of the person and staging of puberty (prepubertal, mid-puberty, and postpubertal), the birth-assigned sex, and capacity to provide consent, among other factors. In a prepubertal child, the preference is to avoid taking any irreversible steps due to the findings of desistance of GD in the majority of prepubertal children with gender variance [66].
The use of GnRH analogs is appropriate in those young people who have evidence of puberty on clinical examination [Tanner stage 2: initiation of breast development in girls, testicular volume ˃ 4 mL in boys [67]]. GnRH analogs are long-acting GnRH agonists that desensitize the GnRH receptor, leading to suppression of gonadotropin release; therefore, they block puberty and halt the further development of secondary sex characteristics until the person can consent, as an adult, to the transition. Through stopping pubertal progression, GnRH analogs help children with established GD to alleviate their distress and anxiety, which are both linked to appearance of secondary sex characteristics [4, 68,69,70,71,72,73]. The efficacy and safety of GnRH analogs in adolescents with GD are both well established [74]; however, adolescents should fulfill certain criteria to be eligible for pubertal suppression. According to the Endocrine Society, treatment with GnRH analogs should be proposed if (i) GD has been diagnosed based on clinical criteria; (ii) initiation of puberty has been confirmed and contraindications to GnRH analog treatments do not exist; (iii) the adolescent and their parents have been fully informed about the effects, the side effects, and the impact of the treatment on future surgical procedures, as well as about the fertility preservation possibilities; (iv) the adolescent has fully understood the treatment protocol and has signed their informed consent form. If the legal age has not been reached, then their parents should give their signed informed consent; and (v) pubertal suppression is proposed by a multidisciplinary team with expertise in transgender health [14]. GnRH analogs are administered by intramuscular or subcutaneous injections, preferably once per month rather than once per 3 months to ensure adequate inhibition of gonadotropin secretion [75, 76]. During treatment, menses will stop and breasts will become atrophic in birth-assigned girls, while the appearance of facial hair will be discontinued in birth-assigned boys [4]. Side effects include redness and swelling reported by 9% of young people and local pain in up to 10–20% [72]. In addition, transient effects on bone mineral density, reduced growth velocity, decrease in lean body mass and increase in body fat percentage, mood changes, worsening acne, vaginal bleeding, vaginal pain, and itching, while fewer erections, have been reported in young people receiving pubertal suppression [72, 74, 77]. Side effects of GnRH analogs are consistent with the physiological effects of hypogonadism, such as vasomotor instability and hot flushes, headaches and emotional lability, and mood disturbance.
The timing of initiation of GnRH agonist therapy in birth-assigned boys relative to pubertal stage has an impact on future options for surgery and should be discussed with families prior to starting treatment. Prevalent techniques for gender-affirming genital surgeries include gonadectomy, penectomy, and creation of a neovagina. Surgeons invert the skin of the penis to form the wall of the vagina and the scrotum becomes the labia majora. Both starting GnRH analogs early in puberty and the prolonged hormonal intake can together culminate in inadequate penile length and scrotal hypoplasia, making penoscrotal inversion vaginoplasty not feasible, thus leading to more complex surgical techniques. Young people and their families should be duly informed prior to starting treatment, especially at an early pubertal stage [14].
In adolescents willing to proceed via hormonal transitioning and in adults, the treatment involves the use of gender-affirming hormones, i.e., estrogens for trans-females and testosterone for trans-males. Importantly, the Endocrine Society does not specify a minimum age for the hormonal treatment but suggests an age when the adolescent is capable of understanding the benefits and risks of therapy [4, 14]. Hormonal treatment should be initiated progressively, with the dose increasing gradually, and should occur in parallel with psychological treatment and support from the multidisciplinary team and support groups. Additional specialists can include speech and language therapists and specialists working in assisted conception. After an agreed upon time (known as social gender role transition) during which the person will live according to their identified gender, the option for genital reconstructive surgery is offered [78].
Loss of fertility incurred as a consequence of hormonal treatment requires consideration before initiation of treatment. The discussion with young people and their families will be influenced by their stage of puberty, biological gender, and degree of gender dysphoria and the availability and acceptance of assisted reproductive technologies (ART). Before starting treatment with GnRH agonist therapy, sperm and oocyte retrieval and banking can be offered to those who are postpubertal. In birth-assigned males, at Tanner stage 3, ejaculation or electroejaculation can take place and yield sufficient sperm for preservation. In birth-assigned females, oocyte harvesting is only available if they are postmenarchal. Young people who commence GnRH agonist therapy at Tanner stage 2 and continue on to gender-affirming hormones will achieve neither spermatogenesis nor menarche and will therefore not have the opportunity to bank gametes using cryopreservation. If individuals subsequently want to preserve fertility after having started GnRH agonists, it may take 6 months or more for the reproductive axis to recover, and the reproductive capacity will only be the same as at the point of starting blocker treatment. Nevertheless, for many young people and families, after appropriate informed consent, the benefits of pubertal suppression still outweigh the risks. The current experiences of trans people with ART service providers is mostly negative, even in countries where there are no legal barriers to access to ART. With future options on the way, an ethical and legal debate is essential, taking into account the right to equality and non-discrimination and the right of transgender people to procreate [4, 27].
Mental health
Mental health remains one of the major issues in transgender young people. Indeed, high rates of anxiety, eating disorders, depression, self-harm, and suicidal ideation have been well-documented in adolescents and adults with GD [79,80,81,82,83]. In a retrospective study, 56% of transgender young people reported previous suicidal ideation, and one in three reported a previous suicide attempt, compared with 20 and 11% of matched cisgender individuals, respectively [80]. Mental illness in transgender individuals seems to be multifactorial. In fact, social rejection, stigma, discrimination, low access to healthcare providers with expertise in transgender health, and limited availability to multidisciplinary team of experts contribute substantially to mental disorders [84].
Young people who were treated and cared for in trained multidisciplinary teams showed similar mental health outcomes as the general population [85]. When treated, patients with psychiatric disorders, such as dissociative disorders combined with GD, showed better outcome as regards their psychiatric illness [86]. In addition, an affirming model of care, including validation from family and community, is considered to have better mental health outcomes in GD [87]. It is important for health professionals to support and educate families about GD so that they in turn can support their children.
Ongoing research to help elucidate the mechanism of GD development will hopefully provide resources for educating communities and parents, culminating in better outcomes among GD children. Many psychological factors within a family unit and cultural factors which may contribute to the expression of a young person’s gender identity have been explored [4]. Within a young person’s family, it is known that there is no influence of parental prenatal sex preference. Parental tolerance toward gender dysphoria can either be interpreted as reinforcement of gender dysphoria or an appropriate adaptation to a young person with gender dysphoria and therefore cannot clearly be seen as influential. The worldwide presence of gender dysphoria, including in non-Western countries, would suggest that cultural aspects might not be a major influence. A psychoanalytic hypothesis suggests that a person’s identity represents a knot comprising several dimensions (the real body, the body image, and the symbolic dimension). Transgender individuals may be experiencing a discrepancy between these dimensions, and this could be improved by transitioning [88].
Conclusions and future perspectives
Thanks to ever-increasing social acceptance and destigmatization of children and adolescents with GD, the number of transgender young people seeking endocrine care has increased over recent years. Although there are increasing numbers of clinical specialist centers in more countries, a large number of transgender individuals are seen in pediatric tertiary centers, thereby providing a fruitful ground for clinical research. During the last decade, we have witnessed tremendous progress in terminology and specific criteria to set the diagnosis, while a growing body of evidence suggests that several factors contribute synergistically to the complex pathogenesis of GD. Guidelines for treatment with GnRH analogs and gender-affirming hormones are now available; however, a number of challenges and controversies still exist. Undoubtedly, there are several areas in which questions remain unanswered. Future and larger studies are clearly required to delineate the long-term effects of pubertal suppression and cross-sex hormone therapy, especially on metabolism, on the growing skeleton, and on brain development and cognition. In addition, it is still imperative to improve prepubertal fertility preservation and mental health in this vulnerable population. Further research into these issues will optimize the approach and management of children and adolescents with GD.
References
World Health Organization (2018) International statistical classification of diseases and related health problems (11th revision)
Unger CA (2014) Care of the transgender patient: the role of the gynecologist. Am J Obstet Gynecol 210(1):16–26
American Psychiatric Association (2013) The diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing, Arlington
Martinerie L, Condat A, Bargiacchi A, Bremont-Weill C, de Vries MC, Hannema SE (2018) Management of endocrine disease: approach to the management of children and adolescents with gender Dysphoria. Eur J Endocrinol 179(5):R219–R237
T'Sjoen G, Arcelus J, Gooren L, Klink DT, Tangpricha V (2019) Endocrinology of transgender medicine. Endocr Rev 40(1):97–117
Atkinson SR, Russell D. Gender dysphoria. FOCUS 792 REPRINTED FROM AFP (Vol. 44). 2015. Retrieved from http://genderrights.org.au/sites/default/files/u9/AGAInfoPack2014.pdf
Ristori J, Steensma TD (2016) Gender dysphoria in childhood. Int Rev Psychiatry 28(1):13–20
Cohen-Kettenis PT, Owen A, Kaijser VG, Bradley SJ, Zucker KJ (2003) Demographic characteristics, social competence, and behavior problems in children with gender identity disorder: a cross-national, cross-clinic comparative analysis. J Abnorm Child Psychol 31(1):41–53
Steensma TD, Zucker KJ, Kreukels BPC, VanderLaan DP, Wood H, Fuentes A, Cohen-Kettenis PT (2014) Behavioral and emotional problems on the teacher’s report form: a cross-national, cross-clinic comparative analysis of gender dysphoric children and adolescents. J Abnorm Child Psychol 42(4):635–647
Shumer DE, Nokoff NJ, Spack NP (2016) Advances in the care of transgender children and adolescents. Adv Pediatr Infect Dis 63(1):79–102
Drummond KD, Bradley SJ, Peterson-Badali M, Zucker KJ (2008) A follow-up study of girls with gender identity disorder. Dev Psychol 44:34–45
Wallien MSC, Quilty LC, Steensma TD, Singh D, Lambert SL, Leroux A et al (2009) Cross-national replication of the gender identity interview for children. J Pers Assess 91:545–552
Steensma TD, Biemond R, de Boer F, Cohen-Kettenis PT (2011) Desisting and persisting gender dysphoria after childhood: a qualitative follow-up study. Clin Child Psychol Psychiatry 16:499–516
Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH et al (2017) Endocrine treatment of gender-dysphoric/gender-incongruent persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 102:3869–3903
Steensma TD, Kreukels BPC, de Vries ALC, Cohen-Kettenis PT (2013) Gender identity development in adolescence. Horm Behav 64:288–297
Littman L (2018) Parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria. PLoS One 13(8):e0202330
Zucker KJ (2019) Adolescents with gender dysphoria: reflections on some contemporary clinical and research issues. Arch Sex Behav
Brandelli CA (2019) Formal comment on: parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria. PLoS One 14(3):e0212578
Restar AJ, Methodological Critique of Littman's (2018) Parental-respondents accounts of "rapid-onset gender dysphoria". Arch Sex Behav 2019
Hutchinson A, Midgen M & Spiliadis A. In support of research into rapid-onset gender dysphoria. Arch Sex Behav. 2019
Shields JP, Cohen R, Glassman JR, Whitaker K, Franks H, Bertolini I (2013) Estimating population size and demographic characteristics of lesbian, gay, bisexual, and transgender youth in middle school. J Adolesc Health 52:248–250
Clark TC, Lucassen MFG, Bullen P, Denny SJ, Fleming TM, Robinson EM, Rossen FV (2014) The health and well-being of transgender high school students: results from the New Zealand adolescent health survey (Youth’12). J Adolesc Health 55:93–99
Eisenberg ME, Gower AL, McMorris BJ, Rider G, Shea G, Coleman E (2017) Risk and protective factors in the lives of transgender/gender nonconforming adolescents. J Adolesc Health 61:521–526
Zucker KJ (2017) Epidemiology of gender dysphoria and transgender identity. Sex Health 14(5):404
de Graaf NM, Giovanardi G, Zitz C, Carmichael P (2018) Sex ratio in children and adolescents referred to the gender identity development services in the UK (2009–2016) [letter to the editor]. Arch Sex Behav 47:1301–1304
Skordis N, Butler G, de Vries MC, Main K, Hannema SE (2018) ESPE and PES international survey of centers and clinicians delivering specialist care for children and adolescents with gender dysphoria. Horm Res Paediatr 90(5):326–331
Butler G, De Graaf N, Wren B, Carmichael P (2018) Assessment and support of children and adolescents with gender dysphoria. Arch Dis Child 103(7):631–636
Fielding J, Bass C (2018) Individuals seeking gender reassignment: marked increase in demand for services. BJPsych Bull 42(5):206–210
Aitken M, Steensma TD, Blanchard R, VanderLaan DP, Wood H, Fuentes A et al (2015) Evidence for an altered sex ratio in clinic-referred adolescents with gender dysphoria. J Sex Med 12(3):756–763
Sumia M, Lindberg N, Työläjärvi M, Kaltiala-Heino R (2017) Current and recalled childhood gender identity in community youth in comparison to referred adolescents seeking sex reassignment. J Adolesc Health 56:34–39
Levitan N, Barkmann C, Richter-Appelt H, Schulte-Markwort M, Becker-Hebly I (2019) Risk factors for psychological functioning in German adolescents with gender dysphoria: poor peer relations and general family functioning. Eur Child Adolesc Psychiatry
Saleem F, Rizvi SW (2017) Transgender associations and possible etiology: a literature review. Cureus. 9(12):e1984
Garcia-Falgueras A, Swaab DF (2008) A sex difference in the hypothalamic uncinate nucleus: relationship to gender identity. Brain. 131(12):3132–3146
Rosenthal SM (2014) Approach to the patient: transgender youth: endocrine considerations. J Clin Endocrinol Metab 99(12):4379–4389
Zhou J-N, Hofman MA, Gooren LJG, Swaab DF (1995) A sex difference in the human brain and its relation to transsexuality. Nature. 378(6552):68–70
Kruijver FPM, Zhou J-N, Pool CW, Hofman MA, Gooren LJG, Swaab DF (2000) Male-to-female transsexuals have female neuron numbers in a limbic nucleus. J Clin Endocrinol Metab 85(5):2034–2041
Taziaux M, Staphorsius AS, Ghatei MA, Bloom SR, Swaab DF, Bakker J (2016) Kisspeptin expression in the human Infundibular nucleus in relation to sex, gender identity, and sexual orientation. J Clin Endocrinol Metab 101(6):2380–2389
Luders E, Sánchez FJ, Gaser C, Toga AW, Narr KL, Hamilton LS, Vilain E (2009) Regional gray matter variation in male-to-female transsexualism. NeuroImage. 46(4):904–907
Berglund H, Lindstrom P, Dhejne-Helmy C, Savic I (2008) Male-to-female transsexuals show sex-atypical hypothalamus activation when smelling odorous steroids. Cereb Cortex 18(8):1900–1908
Savic I, Arver S (2011) Sex dimorphism of the brain in male-to-female transsexuals. Cereb Cortex 21(11):2525–2533
Nota NM, Burke SM, den Heijer M, Soleman RS, Lambalk CB, Cohen-Kettenis PT et al (2017) Brain sexual differentiation and effects of cross-sex hormone therapy in transpeople: a resting-state functional magnetic resonance study. Neurophysiol Clin 47(5–6):361–370
Nota NM, Kreukels BPC, den Heijer M, Veltman DJ, Cohen-Kettenis PT, Burke SM, Bakker J (2017) Brain functional connectivity patterns in children and adolescents with gender dysphoria: sex-atypical or not? Psychoneuroendocrinology. 86:187–195
Schöning S, Engelien A, Bauer C, Kugel H, Kersting A, Roestel C et al (2010) Original research —intersex and gender identity disorders : neuroimaging differences in spatial cognition between men and male-to-female transsexuals before and during hormone therapy. J Sex Med 7(5):1858–1867
Green R (2000) Family cooccurrence of “gender dysphoria”: ten sibling or parent–child pairs. Arch Sex Behav 29(5):499–507
Gómez-Gil E, Esteva I, Almaraz MC, Pasaro E, Segovia S, Guillamon A (2010) Familiality of gender identity disorder in non-twin siblings. Arch Sex Behav 39:546–552
van Beijsterveldt CEM, Hudziak JJ, Boomsma DI (2006) Genetic and environmental influences on cross-gender behavior and relation to behavior problems: a study of Dutch twins at ages 7 and 10 years. Arch Sex Behav 35:647–658
Heylens G, De Cuypere G, Zucker KJ, Schelfaut C, Elaut E, Vanden Bossche H et al (2012) Gender identity disorder in twins: a review of the case report literature. J Sex Med 9(3):751–757
Inoubli A, De Cuypere G, Rubens R, Heylens G, Elaut E, Van Caenegem E, Menten B, T’Sjoen G (2011) Karyotyping, is it worthwhile in transsexualism? J Sex Med 8:475–478
Pang KC, Feldman D, Oertel R, Telfer M (2018) Molecular karyotyping in children and adolescents with gender dysphoria. Transgender Health 3(1):147–153
Fernández R, Guillamón A, Gómez-Gil E, Esteva I, Almaraz MC, Cortés-Cortés J et al (2018) Analyses of karyotype by G-banding and high-resolution microarrays in a gender dysphoria population. Genes Genom 40(5):465–473
Henningsson S, Westberg L, Nilsson S, Lundström B, Ekselius L, Bodlund O et al (2005) Sex steroid-related genes and male-to-female transsexualism. Psychoneuroendocrinology. 30(7):657–664
Cooke B, Hegstrom CD, Villeneuve LS, Breedlove SM (1998) Sexual differentiation of the vertebrate brain: principles and mechanisms. Front Neuroendocrinol 19(4):323–362
Wilson JD (1999) The role of androgens in male gender role behavior. Endocr Rev 20(5):726–737
Hare L, Bernard P, Sánchez FJ, Baird PN, Vilain E, Kennedy T et al (2009) Androgen receptor repeat length polymorphism associated with male-to-female transsexualism. Biol Psychiatry 65(1):93–96
Kazemi-Esfarjani P, Trifiro MA, Pinsky L (1995) Evidence for a repressive function of the long polyglutamine tract in the human androgen receptor: possible pathogenetic relevance for the (CAG)n-expanded neuronopathies. Hum Mol Genet 4(4):523–527
Pol HEH, Cohen-Kettenis PT, Van Haren NEM, Peper JS, Brans RGH, Cahn W et al (2006) Changing your sex changes your brain: influences of testosterone and estrogen on adult human brain structure. Eur J Endocrinol 155(suppl_1):S107–S114
Ujike H, Otani K, Nakatsuka M, Ishii K, Sasaki A, Oishi T et al (2009) Association study of gender identity disorder and sex hormone-related genes. Prog Neuro-Psychopharmacol Biol Psychiatry 33(7):1241–1244
Fernández R, Esteva I, Gómez-Gil E, Rumbo T, Almaraz MC, Roda E et al (2014) Association study of ERβ, AR, and CYP19A1 genes and MtF transsexualism. J Sex Med 11(12):2986–2994
Fernández R, Esteva I, Gómez-Gil E, Rumbo T, Almaraz MC, Roda E et al (2014) The (CA)n polymorphism of ERβ gene is associated with FtM transsexualism. J Sex Med 11(3):720–728
Fernández R, Guillamon A, Cortés-Cortés J, Gómez-Gil E, Jácome A, Esteva I et al (2018) Molecular basis of gender dysphoria: androgen and estrogen receptor interaction. Psychoneuroendocrinology. 98:161–167
Foreman M, Hare L, York K, Balakrishnan K, Sánchez FJ, Harte F et al (2019) Genetic link between gender dysphoria and sex hormone signaling. J Clin Endocrinol Metab 104(2):390–396
Yang F, Zhu XH, Zhang Q, Sun NX, Ji YX, Ma JZ et al (2017) Genomic characteristics of gender Dysphoria patients and identification of rare mutations in RYR3 gene. Sci Rep 7(1):8339
Rivas MP, Moreira LMA, Santo LDE, Marques ACSS, El-Hani CN, Toralles MBP (2014) New studies of second and fourth digit ratio as a morphogenetic trait in subjects with congenital adrenal hyperplasia. Am J Hum Biol 26(4):559–561. https://doi.org/10.1002/ajhb.22545
Wallien MSC, Zucker KJ, Steensma TD, Cohen-Kettenis PT (2008) 2D:4D finger-length ratios in children and adults with gender identity disorder. Horm Behav 54(3):450–454
Kraemer B, Noll T, Delsignore A, Milos G, Schnyder U, Hepp U (2009) Finger length ratio (2D:4D) in adults with gender identity disorder. Arch Sex Behav 38(3):359–363
Wallien MSC, Cohen-Kettenis PT (2008) Psychosexual outcome of gender-dysphoric children. J Am Acad Child Adolesc Psychiatry 47(12):1413–1423
Carel JC, Léger J (2008) Clinical practice. Precocious puberty. N Engl J Med 358:2366–2377
Costa R, Carmichael P, Colizzi M (2016) To treat or not to treat: puberty suppression in childhood-onset gender dysphoria. Nat Rev Urol 13(8):456–462
de Vries AL, Klink D, Cohen-Kettenis PT (2016) What the primary care pediatrician needs to know about gender incongruence and gender dysphoria in children and adolescents. Pediatr Clin N Am 63(6):1121–1135
Kaltiala-Heino R, Bergman H, Työläjärvi M, Frisén L (2018) Gender dysphoria in adolescence: current perspectives. Adolesc Health Med Ther 9:31–41
Rafferty J, COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH; COMMITTEE ON ADOLESCENCE; SECTION ON LESBIAN, GAY, BISEXUAL, AND TRANSGENDER HEALTH AND WELLNESS (2018) Ensuring comprehensive care and support for transgender and gender-diverse children and adolescents. Pediatrics 142(4):e20182162
Panagiotakopoulos L (2018) Transgender medicine - puberty suppression. Rev Endocr Metab Dis 19(3):221–225
Butler G, Wren B, Carmichael P (2019) Puberty blocking in gender dysphoria: suitable for all? Arch Dis Child 104(6):509–510
Schagen SEE, Cohen-Kettenis PT, Delemarre-van de Waal HA, Hannema SE (2016) Efficacy and safety of gonadotropin-releasing hormone agonist treatment to suppress puberty in gender dysphoric adolescents. J Sex Med 13:1125–1132
Badaru A, Wilson DM, Bachrach LK, Fechner P, Gandrud LM, Durham E et al (2006) Sequential comparisons of one-month and three-month depot leuprolide regimens in central precocious puberty. J Clin Endocrinol Metab 91:1862–1867
Carel JC, Eugster EA, Rogol A, Ghizzoni L, Palmert MR, ESPE-LWPES GnRH Analogs Consensus Conference Group et al (2009) Consensus statement on the use of gonadotropin-releasing hormone analogs in children. Pediatrics. 123:e752–e762
Lee JW, Kim HJ, Choe YM, Kang HS, Kim SK, Jun YH et al (2014) Significant adverse reactions to long-acting gonadotropin-releasing hormone agonists for the treatment of central precocious puberty and early onset puberty. Ann Pediatr Endocrinol Metab 19(3):135–140
Hess J, Rossi Neto R, Panic L, Rübben H, Senf W (2014) Satisfaction with male-to-female gender reassignment surgery. Dtsch Arztebl Int 111(47):795–801
Clements-Nolle K, Marx R, Katz M (2006) Attempted suicide among transgender persons: the influence of gender-based discrimination and victimization. J Homosex 51(3):53–69
Almeida J, Johnson RM, Corliss HL, Molnar BE, Azrael D (2009) Emotional distress among LGBT youth: the influence of perceived discrimination based on sexual orientation. J Youth Adolesc 38(7):1001–1014
Haas AP, Eliason M, Mays VM, Mathy RM, Cochran SD, D'Augelli AR et al (2011) Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: review and recommendations. J Homosex 58(1):10–51
Colizzi M, Costa R, Todarello O (2014) Transsexual patients’ psychiatric comorbidity and positive effect of cross-sex hormonal treatment on mental health: results from a longitudinal study. Psychoneuroendocrinology. 39:65–73
Connolly MD, Zervos MJ, Barone CJ II, Johnson CC, Joseph CL (2016) The mental health of transgender youth: advances in understanding. J Adolesc Health 59(5):489–495
Edwards-Leeper L, Spack NP (2012) Psychological evaluation and medical treatment of transgender youth in an interdisciplinary “gender management service” (GeMS) in a major pediatric center. J Homosex 59(3):321–336
Lopez X, Stewart S, Jacobson-Dickman E (2016) (2016). Approach to children and adolescents with gender dysphoria. Pediatr Rev 37(3):89–98
Colizzi M, Costa R, Todarello O (2015) (2015). Dissociative symptoms in individuals with gender dysphoria: is the elevated prevalence real? Psychiatry Res 226(1):173–180
Hidalgo MA, Ehrensaft D, Tishelman AC, Clark LF, Garofalo R, Rosenthal SM et al (2013) The gender affirmative model: what we know and what we aim to learn. Hum Dev. 56(5):285–290
Condat A, Mendes N, Drouineaud V, Gründler N, Lagrange C, Chiland C, Wolf JP, Ansermet F, Cohen D (2018) Biotechnologies that empower transgender persons to self-actualize as individuals, partners, spouses and parents are defining new ways to conceive a child: psychological considerations and ethical issues. Philos Ethics Humanit Med 13(1):1
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Skordis, N., Kyriakou, A., Dror, S. et al. Gender dysphoria in children and adolescents: an overview. Hormones 19, 267–276 (2020). https://doi.org/10.1007/s42000-020-00174-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42000-020-00174-1