
Abstract
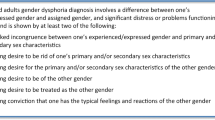
Gender incongruence (GI) is defined as discrepancy between the experienced gender and the gender assigned at birth. When this condition causes clinically significant distress or impairment in social, occupational, or other important areas of functioning, it is defined as gender dysphoria (GD).
There has been an increasing prevalence of individuals referring for gender-affirming treatment over the past several years. With regards to adolescents, the Endocrine Society recommends suppression with gonadotropin-releasing hormone agonists (GnRHas) for gender-dysphoric/gender-incongruent young persons who have entered puberty at least Tanner Stage 2. GnRHas are long-acting analogues of Gonadotropin Releasing Hormone that temporarily suppress the endogenous production of sex hormones, therefore interrupting pubertal development. Clinicians may start gender-affirming hormonal therapy after a multidisciplinary team has confirmed the persistence of gender dysphoria/gender incongruence in the adolescent.
Although few data are currently available in adolescents, they support the fact that the proven psychological benefits of early medical intervention in transgender adolescents effectively outweigh the potential, but still low, risks of medical treatment.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
14.1 Introduction
Gender incongruence (GI) is defined by a marked and persistent incongruence between an individual’s experienced gender and the assigned sex at birth [1]. When this condition leads to a clinically significant distress or impairment in social, occupational, or other important areas of functioning, we refer to it as Gender Dysphoria (GD) [1]. Individuals whose gender identity does not completely and/or permanently match their sex characteristics may describe themselves as trans or transgender [1]. In particular, we use the term trans men for those assigned female at birth who identify as men, and trans women for those assigned males who identify as women. GI/GD represent a dimensional phenomenon that can occur with different degrees of intensity, of which the most extreme form is accompanied by a desire for gender-affirming treatment, including hormonal treatment and/or surgical interventions.
GI/GD may develop during childhood and remit in most prepubertal children [2, 3]. Afterwards, it can persist during adolescence and adulthood only in a minority of cases. The percentage of “persisters” appears to be between 10% and 27% [2, 4, 5].
During the management of children and adolescents with GI/GD, health care professionals should broadly conform to the Standards of Care of the World Professional Association for Transgender Health (WPATH) [6] and to the Endocrine Society’s guidelines [7]. These are both mainly inspired by the pioneering work of Delamarre-van de Waal and Cohen-Kettenis [8] who described for the first time the “Dutch Approach,” a clinical protocol for the management of GI/GD during adolescence. This protocol is characterized by a “Combined Approach,” including both psychological support and medical intervention, structured in three different phases: (i) a first diagnostic phase without medical interventions; (ii) the extended diagnostic phase, characterized by puberty suspension with GnRH analogues (GnRHa);` and [3] induction of puberty congruent with gender identity.
In the first phase, a psychological support and evaluation is offered, with the aim to assess the presence and intensity of GI/GD [1] and to evaluate the presence of interfering psychological and/or social conditions. In this phase, the mental health professional (MHP) should also evaluate the presence of adequate psychological and social support, actively including parents. In line with WPATH recommendations, this phase should be conducted by a MHP with a specific training in child and adolescent developmental psychopathology and skilled in GI/GD [6].
During the establishment of the therapeutic relationship, the clinician should maintain a neutral attitude regarding any possible outcome in order to help the adolescent to explore his/her gender identity openly. Finally, in this phase the MHP should inform the adolescent and the family accurately regarding different treatment options, and consequences (including those related to fertility preservation) in order to prevent unrealistic expectations.
In case GD persists, the MHP’s role is also to assess the presence of criteria for pubertal suppression with GnRHa, as reported in Table 14.1.
In particular, it is recommended to start puberty suppression with GnRHa not earlier than Tanner stage G2/B2, in case the early pubertal modifications lead to a worsening of GD feelings [6, 7]. In fact, emotional reactions to the undesired body changes—in the opposite direction from the experienced gender identity—have an important diagnostic value for the MHP.
14.2 Puberty Suspension
During the extended diagnostic phase, the administration of GnRHa allows to suspend pubertal development. In fact, these long-acting analogues temporarily suppress the endogenous production of sex steroids by GnRH receptor desensitization, after an initial increase of gonadotropins during 10 days after the first and the second injection [9]. Despite several GnRHa being available, triptorelin is the most studied in GD/GI adolescents [8]. The most used protocol contemplates the administration of triptorelin with a monthly formulation (3.75 mg every 28 days). In case gonadotropins are well suppressed, after 6 months, it is possible to switch to a trimestral formulation (11.25 mg). In transboys (assigned female at birth adolescents) the initial interval may be shortened, repeating the second injection (3.75 mg) after 12 days, in order to avoid menstrual bleeding risk.
GnRH antagonist could represent a potential alternative to GnRHa, since they immediately suppress pituitary gonadotropin secretion [10, 11]. This could represent an advantage through the elimination of the initial “flare” in gonadotropic axis activation. However, the absence of evidences regarding the safety and efficacy of GnRH antagonists does not allow their use in GD/GI adolescents.
GnRHa effectively suspend pubertal development, leaving these adolescents in a “limbo” in which they can explore their gender identity, without the distress derived by the undesired body modifications. In fact, already at the onset of Tanner 2 puberty, body changes—such as breast development in transboys and increasing testicular size in transgirls (assigned male at birth adolescents)—may become unbearable. With the progression of puberty, other modifications occur, such as menarche/menses in transboys and deepening of voice, virilizing hair pattern, development of facial dimorphic characteristics, and spontaneous erections in transgirls. These undesired body modifications are perceived as devastating and humiliating. At this point, GD/GI adolescents realize that they cannot avoid the natural expression of their biological sex, which is incongruent with their gender identity. In fact, the onset of puberty is usually associated in transgender youth with a worsening of GD, distress, and psychological functioning and well-being [12].
During GnRHa treatment, slight development of secondary sex characteristics may regress or stop. Among the effects, we can mention breast atrophy, menses cessation in transgirls, and decrease in body hair distribution and in testicular volume, as well as reduction of spontaneous erections in transgirls [13].
Because of the suppression of pubertal development, GnRHa treatment immediately reduces the subject’s suffering and may prevent emotional and psychological impairment [14, 15]. Furthermore, GnRH treatment extends the diagnostic phase, by leaving the body in a neutral early pubertal state. During this period the adolescent can continue to self-explore his/her gender identity, without the distress caused by pubertal modifications [7], allowing the clinicians to “gain time” during the extended diagnostic phase.
An important advantage of GnRHa is the reversibility of the intervention. If the adolescent decides not to follow with the transition path, pubertal block can be discontinued. Spontaneous pubertal development will resume immediately and the subject can resume the maturation in the biological direction [16].
Furthermore, physical treatment outcome in adolescents treated with GnRHa is more satisfactory compared to treatment started later in puberty, when secondary sex characteristics have already been developed [17, 18]. Starting earlier medical treatment may reduce the invasiveness of future medical and surgical interventions [19]. For example, electrolysis hair removal, voice therapy, or surgery could not be necessary in transwomen individuals, as well as chest surgery in transmen.
Psychological support to the adolescent is crucial during all this delicate phase. Therefore, meetings with a skilled MHP are encouraged in order to evaluate all the aspects of psychological and social functioning, as well as exploring GD/GI and its possible outcomes [20].
Furthermore, during GnRHa treatment, guidelines recommend measuring gonadotropins and sex steroids levels to confirm adequate gonadal axis suppression [7]. In case gonadal axis is not completely suppressed, the time between GnRHa administrations can be shortened or the dose increased. Moreover, it is important to monitor negative effects of delaying puberty, such as halted growth spurt and impaired bone mineral accretion.
14.2.1 Criticalities of GnRHa Treatment
Overall, GnRHa appear to be an effective and safe treatment to block endogenous pubertal development in GD/GI adolescents. However, most of the evidences are based on studies in which GnRHa treatment was used to suppress precocious puberty and long-term follow-up studies are still quite limited.
The main risk of pubertal suppression in GD/GI adolescents may include an impairment of bone mineralization. In fact, puberty is the most important period in life for correct bone mass achievement, since about 85–90% of the total bone mass will have been acquired at the end of puberty [21]. Few data are available on the effect of GnRHa on bone mineral density (BMD) in adolescents with GD/GI. Contrasting evidences come from studies in different settings. For example, some studies reported that men with constitutionally delayed puberty have decreased BMD in adulthood [22], while others showed a normal BMD in this population [23, 24]. Similarly, a decrease of BMD is described in children with central precocious puberty treated with GnRHa in some studies [25], while others did not confirm these findings [26].
Concerning GnRHa treatment in GD/GI adolescents, data demonstrated no change of absolute areal BMD during GnRHa treatment, but a decrease in BMD Z-scores, mainly the lumbar spine [8, 27, 28]. The subsequent hormonal treatment to induce puberty led to an increase of BMD Z-score in both transmen and transwomen; however, even after 24 months of gender-affirming hormonal treatment, pretreatment Z-score values were not reached in most of transgender adolescents [28]. Considering these evidences, dual-energy X-ray absorptiometry (DXA) scans remain important in follow up of bone health of transgender adolescents. Besides, calcium and vitamin D supplementation in case of deficiency may improve bone health during GnRHa treatment, as well as an appropriate lifestyle (including physical activity and smoking avoidance/cessation). With regard to body composition, GnRHa have not been associated with a change in body mass index (BMI) standard deviation score in GD/GI adolescents [27]. However, GnRHa treatment seems to modify body composition leading to an increase in fat mass and a decrease in lean body mass percentage [13]. Comparable results have been observed also in girls treated for precocious puberty with GnRHa [29, 30].
Another criticality of GnRHa treatment is represented by the potential effects on brain development. Puberty has been suggested to represent a second organizational period during brain development both in animals and humans [31, 32], especially regarding the development of executive functioning. The question arises if pubertal suppression with GnRHa affects the development of this task. Limited data are available regarding this aspect. A single cross-sectional study [33], comparing the performance on the Tower of London (ToL) task of adolescents under GnRHa treatment with control boys and girls, demonstrated no compromise of executive function. Unexpectedly, when evaluating brain activation patterns during ToL performance, GnRHa treated adolescents with GD showed sex differences in neural activation similar to their natal sex control group.
An additional side effect reported in a few girls treated with GnRHa for precocious/early puberty is arterial hypertension [34, 35]. Similar evidences have not yet been reported in GD/GI adolescents treated with GnRHa, however blood pressure monitoring before and during treatment is recommended [7].
Furthermore, treated adolescents may also experience hot flashes, fatigue, and mood alterations as a consequence of pubertal suppression and reduction of sex steroids levels. Though, there is no consensus on treatment of these side effects in this context.
Finally, fertility issues should be adequately explored before the start of GnRHa treatment. Puberty suppression can pause the maturation of germ cells, and thus, affect fertility potential. However, data on fertility outcome after GnRHa treatment are lacking and fertility preservation options in these individuals are still investigational.
14.3 Puberty Induction
Clinicians can start gender-affirming hormones after a multidisciplinary team has confirmed the persistence of gender dysphoria/gender incongruence in adolescents with a sufficient mental (and legal) capacity to give informed consent to this partially irreversible treatment (Table 14.2).
Although in many countries adolescents are able to start treatments since 16 years old, the timing of sex hormones starting in transgender adolescents remains under debate. The Endocrine Society guidelines supports the initiation of treatment at the age of 16 years and even earlier in selected cases evaluated by a multidisciplinary team with expertise in gender identity development in children [7]. However, minimal data supporting an earlier use currently exist. When GnRHa treatment is started in the early stages of pubertal development, a puberty congruent with the experienced gender identity is induced with a dose scheme characterized by a progressive increase of hormonal treatment doses in order to simulate a physiological puberty, such as in hypogonadal patients. Alternatively, in late puberty gender-affirming treatment can be given at higher doses until the expected adult dose [7].
This gradually increasing schedule of sex steroid doses does not allow to effectively suppress endogenous sex steroid secretion. For this reason, the continuation of GnRHa treatment is advised until gonadectomy, even if further studies are necessary to evaluate its long-term effects.
Furthermore, transgender adolescents and their parents/other caretakers need to be clearly informed about the potential loss of fertility (impaired spermatogenesis and oocyte maturation) induced by hormonal therapy to make a reasoned and balanced decision and potentially access to fertility preservation clinic.
14.3.1 Transgender Girls
Treatment for induction of a female puberty in transgirls consist in oral or transdermal estrogens formulations.
The oral administration of 17β-estradiol should be started at a dosage of 5 μg/kg/d, increasing the dose every 6 months of 5 μg/kg (to 20 μg/kg/d) until a maintenance dosage of 2 mg is reached.
The transdermal 17β-estradiol may be an alternative for the oral one with an initial dosage from 6.25–12.5 μg/24 h to 37.5 μg/24 h until the adult dose (50–200 μg/24 h) is achieved, raising the dose every 6 months. The use of transdermal alternative is increasing, but the absence of specific low-dose estrogen patches may be uncomfortable: Individuals need to cut the patches themselves to obtain a size corresponding to the appropriate dosage, which is sometimes difficult to calculate and realize; the patches glue may cause allergic reactions; new patches need to be placed every 3.5 day at the same hour of the day [36].
After a period of gonadal suppression varying from 3 to 6 months, estrogens can be given at a daily start dosage of 1 mg and increased to 2 mg after 6 months [7].
The effects of the addition of 17b-estradiol were studied prospectively in 28 transgender girls [37]. Estrogen treatment was started at a median age of 16 years after a median duration of 24.8 months of GnRHa monotherapy. When the adult dose of 2 mg of estradiol daily was reached during a median duration of 2 years, the median serum estradiol was 27 pg/mL (100 pmol/L) [range, 6.5–103 pg/mL (24–380 pmol/L)] and no changes in prolactin levels, hemoglobin, hematocrit, glycated hemoglobin, liver enzymes, and creatinine were seen [38]. Furthermore, physical changes were observed such as the breast development (started within 3 months, and after 1 year median Tanner breast stage was 3 progressing to 5 after 3 years), the increase of hip circumference and the decrease of waist circumference [38]. Although BMI increased, BMI SD scores did not: absolute BMD and Z-scores in the lumbar spine (not in the hip) increased [27, 28], but after 2 years of estrogens Z-scores were still below those of age- and sex-assigned–matched norms [28].
Studies regarding treatment with estrogens on pubertal development and short-term safety demonstrate feminization of the body without adverse events [38], although data on long-term outcomes are still sparse.
14.3.2 Transgender Boys
For male pubertal induction the use of testosterone ester injections is recommended. The initial dose is 25 mg/m2 IM every 2 weeks, progressively increasing 25 mg/m2 every 6 months. The maintenance dosages vary from 100 to 200 mg per 2 weeks for testosterone monoesters, such as testosterone enanthate, to 250 mg per 3 to 4 weeks for testosterone ester mixtures. For transgender boys who started treatment in late puberty, testosterone can be started at 75 mg IM every 2 weeks, followed by the maintenance dosage after 6 months [7]. With androgens treatment, virilization of the body occurs in the first 3–6 months, including lowering of the voice, facial, and body hair growth, muscular development (particularly in the upper body), and clitoral growth [7, 8]. In post-menarche adolescent transboys, a progestogen can be added to stop or decrease menses frequency; instead, the adult dosage alone will be sufficient to suppress gonadal axis.
Prospective data on combined GnRHas and androgens are still scarce. The clinical effects, including those metabolic parameters, in transgender boys have been investigated retrospectively in two studies, one single-center study (n = 42) [39] and one multicenter study center (n = 72) [40]. Only the single-center study reported on side effects, which were fatigue and acne. Clinically, there was a weight gain as both BMI [40] and BMI SD scores increased [39]. Although testosterone preparation and dosages differed, both studies reported an increase in both hemoglobin and hematocrit and in alanine aminotransferase, aspartate aminotransferase, and creatinine (even if they remained in the normal range), a worsening of lipid profile (cholesterol and low-density lipoprotein increase, high-density lipoprotein decrease); glucose homeostasis parameters (HbA1c, insulin, glucose, homeostatic model assessment index) were not affected [41]. In transgender boys the bone density and Z-scores of the lumbar spine and the femoral region increased after 2 years of testosterone therapy even if they don’t reach the pretreatment values [28, 42, 43].
14.4 Conclusions
Knowledge regarding the treatment of gender dysphoria and nonconforming youth has steadily advanced during the past 10 years [44, 45]. The current available research on transgender adolescents treatment is based mostly on cross-sectional studies with limited longitudinal data as well as paucity of information on diverse ethnic and socioeconomic populations (mostly from Western Europe and higher-income countries where many participants undergo surgical procedures and drop the follow-up). Nevertheless, the few somatic data available in adolescents are favorable and hither to support the fact that the proven psychological benefits of early medical intervention in transgender adolescents effectively outweigh the potential medical risks [36].
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5). Arlington, VA: American Psychiatric Publishers; 2013.
Wallien MS, Cohen-Kettenis PT. Psychosexual outcome of gender-dysphoric children. J Am Acad Child Adolesc Psychiatry. 2008;47:1413–23.
Zucker KJ, Bradley S. Gender identity disorder and psychosexual problems in children and adolescents. Guilford: New York, NY; 1995.
Drummond KD, Bradley SJ, Peterson-Badali M, Zucker KJ. A follow-up study of girls with gender identity disorder. Dev Psychol. 2008;44:34–45.
Steensma TD, McGuire JK, Kreukels BP, et al. Factors associated with desistence and persistence of childhood gender dysphoria: a quantitative follow-up study. J Am Acad Child Adolesc Psychiatry. 2013;52:582–90.
Standard of care, 2011 W.P.A.T.H. (World Professional Association of Transgender Health).
Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, Rosenthal SM, Safer JD, Tangpricha V, T’Sjoen GG. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an endocrine society clinical practice guideline. Endocr Pract. 2017;23(12):1437.
Delemarre-van de Waal HA, Cohen-Kettenis PT. Clinical management of gender identity disorder in adolescents: a protocol on psychological and paediatric endocrinology aspects. Eur J Endocrinol. 2006;155(suppl 1):S131–7.
Roth CL, Brendel L, Rückert C, Hartmann K. Antagonistic and agonistic GnRH analogue treatment of precocious puberty: tracking gonadotropin concentrations in urine. Horm Res. 2005;63(5):257–62.
Roth C. Therapeutic potential of GnRH antagonists in the treatment of precocious puberty. Expert Opin Investig Drugs. 2002;11(9):1253–9.
Tuvemo T. Treatment of central precocious puberty. Expert Opin Investig Drugs. 2006;15(5):495–505.
Fisher AD, Ristori J, Castellini G, Sensi C, Cassioli E, Prunas A, Mosconi M, Vitelli R, Dèttore D, Ricca V, Maggi M. Psychological characteristics of Italian gender dysphoric adolescents: a case-control study. J Endocrinol Investig. 2017;40(9):953–65.
Schagen SE, Cohen-Kettenis PT, Delemarre-van de Waal HA, Hannema SE. Efficacy and safety of gonadotropin-releasing hormone agonist treatment to suppress puberty in gender dysphoric adolescents. J Sex Med. 2016;13(7):1125–32.
Cohen-Kettenis PT, Delemarre-van de Waal HA, Gooren LJG. The treatment of adolescent transsexuals: changing insights. J Sex Med. 2008;5:1892–7.
De Vries AL, Steensma TD, Doreleijers TA, Cohen-Kettenis PT. Puberty suppression in adolescents with gender identity disorder: a prospective follow-up study. J Sex Med. 2011;8(8):2276–83.
Manasco PK, Pescovitz OH, Feuillan PP, Hench KD, Barnes KM, Jones J, Hill SC, Loriaux DL, Cutler JRGB. Resumption of puberty after long term luteinizing hormone-releasing hormone treatment of central precocious puberty. J Clin Endocrinol Metab. 1988;67:368–72.
Cohen-Kettenis PT, van Goozen SH. Sex reassignment of adolescent transsexuals: a follow-up study. J Am Acad Child Adolesc Psychiatry. 1997;36:263–71.
Smith YL, van Goozen SH, Cohen-Kettenis PT. Adolescents with gender identity disorder who were accepted or rejected for sex reassignment surgery: a prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 2001;40:472–81.
Cohen-Kettenis PT, Pfafflin F. Transgenderism and intersexuality in childhood and adolescence. London: Sage Publications, Making Choices; 2003.
Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. Int J Transgend. 2011;13:165–232.
Van Coeverden SC, Netelenbos JC, Roos JC, de Ridder CM, Delemarre-van de Waal HA. Reference values for bone mass in Dutch white pubertal children and their relation to pubertal maturation characteristics. Ned Tijdschr Geneeskd. 2001;145(38):1851–6.
Finkelstein JS, Klibanski A, Neer RM. A longitudinal evaluation of bone mineral density in adult men with histories of delayed puberty. J Clin Endocrinol Metab. 1996;81(3):1152–5.
Bertelloni S, Baroncelli GI, Ferdeghini M, Perri G, Saggese G. Normal volumetric bone mineral density and bone turnover in young men with histories of constitutional delay of puberty. J Clin Endocrinol Metab. 1998;83(12):4280–3.
Darelid A, Ohlsson C, Nilsson M, Kindblom JM, Mellström D, Lorentzon M. Catch up in bone acquisition in young adult men with late normal puberty. J Bone Miner Res. 2012;27(10):2198–207.
Saggese G, Bertelloni S, Baroncelli GI, Battini R, Franchi G. Reduction of bone density: an effect of gonadotropin releasing hormone analogue treatment in central precocious puberty. Eur J Pediatr. 1993;152(9):717–20.
Neely EK, Bachrach LK, Hintz RL, Habiby RL, Slemenda CW, Feezle L, Pescovitz OH. Bone mineral density during treatment of central precocious puberty. J Pediatr. 1995;127(5):819–22.
Klink D, Caris M, Heijboer A, van Trotsenburg M, Rotteveel J. Bone mass in young adulthood following gonadotropin-releasing hormone analog treatment and cross-sex hormone treatment in adolescents with gender dysphoria. J Clin Endocrinol Metab. 2015;100(2):E270–5.
Vlot MC, Klink DT, den Heijer M, Blankenstein MA, Rotteveel J, Heijboer AC. Effect of pubertal suppression and cross-sex hormone therapy on bone turnover markers and bone mineral apparent density (BMAD) in transgender adolescents. Bone. 2017;95:11–9.
Pasquino AM, Pucarelli I, Accardo F, Demiraj V, Segni M, Di Nardo R. Long-term observation of 87 girls with idiopathic central precocious puberty treated with gonadotropin-releasing hormone analogs: impact on adult height, body mass index, bone mineral content, and reproductive function. J Clin Endocrinol Metab. 2008;93(1):190–5.
Magiakou MA, Manousaki D, Papadaki M, Hadjidakis D, Levidou G, Vakaki M, Papaefstathiou A, Lalioti N, Kanaka-Gantenbein C, Piaditis G, Chrousos GP, Dacou-Voutetakis C. The efficacy and safety of gonadotropin-releasing hormone analog treatment in childhood and adolescence: a single center, long-term follow-up study. J Clin Endocrinol Metab. 2010;95(1):109–17.
Juraska JM, Sisk CL, DonCarlos LL. Sexual differentiation of the adolescent rodent brain: hormonal influences and developmental mechanisms. Horm Behav. 2013;64:203–10.
Romeo RD. Puberty: a period of both organizational and activational effects of steroid hormones on neurobehavioural development. J Neuroendocrinol. 2003;15:1185–92.
Staphorsius AS, Kreukels BPC, Cohen-Kettenis PT, Veltman DJ, Burke SM, Schagen SEE, Wouters FM, Delemarre-van de Waal HA, Bakker J. Puberty suppression and executive functioning: an fMRI-study in adolescents with gender dysphoria. Psychoneuroendocrinology. 2015;56:190–9.
Calcaterra V, Mannarino S, Corana G, Codazzi AC, Mazzola A, Brambilla P, Larizza D. Hypertension during therapy with triptorelin in a girl with precocious puberty. Indian J Pediatr. 2013;80(10):884–5.
Siomou E, Kosmeri C, Pavlou M, Vlahos AP, Argyropoulou MI, Siamopoulou A. Arterial hypertension during treatment with triptorelin in a child with Williams-Beuren syndrome. Pediatr Nephrol. 2014;29(9):1633–6.
T’Sjoen G, Arcelus J, Gooren L, Klink D, Tangpricha V. Endocrinology of transgender medicine. Endocr Rev. 2019;40(1):97–117.
Laron Z, Kauli R, Zeev ZB, Comaru-Schally AM, Schally AV. D-TRP5-analogue of luteinizing hormone releasing hormone in combination with cyproterone acetate to treat precocious puberty. Lancet. 1981;2(8253):955–6.
Hannema SE, Schagen SEE, Cohen-Kettenis PT, Delemarre-van de Waal HA. Efficacy and safety of pubertal induction using 17b-estradiol in transgirls. J Clin Endocrinol Metab. 2017;102(7):2356–63.
Tack LJ, Craen M, Dhondt K, Vanden Bossche H, Laridaen J, Cools M. Consecutive lynestrenol and cross-sex hormone treatment in biological female adolescents with gender dysphoria: a retrospective analysis. Biol Sex Differ. 2016;7(1):14.
Jarin J, Pine-Twaddell E, Trotman G, Stevens J, Conard LA, Tefera E, Gomez-Lobo V. Cross-sex hormones and metabolic parameters in adolescents with gender dysphoria. Pediatrics. 2017;139(5):e20163173.
Crowley WF Jr, Comite F, Vale W, Rivier J, Loriaux DL, Cutler GB Jr. Therapeutic use of pituitary desensitization with a long-acting LHRH agonist: a potential new treatment for idiopathic precocious puberty. J Clin Endocrinol Metab. 1981;52(2):370–2.
De Roo C, Lierman S, Tilleman K, Peynshaert K, Braeckmans K, Caanen M, Lambalk CB, Weyers S, T’Sjoen G, Cornelissen R, De Sutter P. Ovarian tissue cryopreservation in female-to-male transgender people: insights into ovarian histology and physiology after prolonged androgen treatment. Reprod Biomed Online. 2017;34(6):557–66.
Lierman S, Tilleman K, Braeckmans K, Peynshaert K, Weyers S, T’Sjoen G, De Sutter P. Fertility preservation for trans men: frozen-thawed in vitro matured oocytes collected at the time of ovarian tissue processing exhibit normal meiotic spindles. J Assist Reprod Genet. 2017;34(11):1449–56.
Cohen-Kettenis PT, Schagen SE, Steensma TD, de Vries AL, Delemarre-van de Waal HA. Puberty suppression in a gender-dysphoric adolescent: a 22-year follow-up. Arch Sex Behav. 2011;40(4):843–7.
Cohen-Kettenis PT, Klink D. Adolescents with gender dysphoria. Best Pract Res Clin Endocrinol Metab. 2015;29(3):485–95.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Fisher, A.D., Senofonte, G., Cocchetti, C., Lombardo, F. (2021). Gender Dysphoria: Management in the Transition age. In: Foresta, C., Gianfrilli, D. (eds) Pediatric and Adolescent Andrology. Trends in Andrology and Sexual Medicine. Springer, Cham. https://doi.org/10.1007/978-3-030-80015-4_14
Download citation
DOI: https://doi.org/10.1007/978-3-030-80015-4_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-80014-7
Online ISBN: 978-3-030-80015-4
eBook Packages: MedicineMedicine (R0)