
Abstract
The global public health impact of COVID-19 has been enormous, severe and grievous since its outbreak. The notable global responses to mitigate and curb the COVID-19 pandemic include quarantine, isolation, total lockdown and vaccination. The COVID-19 vaccination is a latter and current response with different levels of compliance across countries. This study addresses the dearth of information on how acceptance of the vaccines relates to cases of COVID-19 across geo-political zones in Nigeria. A quantitative design was employed for the study. Secondary data on COVID-19 cases and vaccination, population census and GIS shapefiles of Nigeria were analysed using a descriptive classification method based on the Jenks Natural Break Algorithm in ArcGIS Desktop 10.3. Findings revealed the South West showed high incidences of all COVID-19 cases and moderate incidences of the first and second doses, but a high incidence of booster dose of the vaccination. Meanwhile, the North West in which the COVID-19 cases showed low incidences had high rates of vaccination. This study concludes that there is a regional variation in the incidences of COVID-19 cases and the administration of COVID-19 vaccination in Nigeria.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There seems to be nothing new in our world about public health disasters as historical accounts provide us with several instances of infectious diseases that had manifested as endemic, epidemic and pandemic, respectively at local, regional and global scales. These past experiences are repeating themselves and such is the case of the deadly virus resonating in the world today. First evolving as an epidemic, there was an outbreak of the novel coronavirus (COVID-19 or SARS-CoV-2) in Wuhan, a densely populated city of over 14 million population and the transportation hub of China (Zhu et al. 2020). At the early stage, there were spatially dispersed confirmed cases of COVID-19 in the city, with some cases purportedly linked to Wuhan Seafood Wholesale Market (Wu et al. 2020). By February 19, 2020, the city had been badly hit by the virus with 44,412 infection cases and 1497 deaths (Zhu et al. 2020); a situation to be accounted a disaster. The city of Wuhan was therefore totally locked down to contain the virus but before then, human mobility had already caused the spread of coronavirus to cities within China. Cases evident throughout China as of 24 February 2020 were 2663 deaths, 77,658 confirmed cases and 2824 suspected cases (National Health Commission of the People’s Republic of China (NHCPRC) 2020). Three thousand, three hundred and forty-three deaths from a total of 83,157 cases of coronavirus were reported in China up to April 7, 2020 (Wang et al. 2020).
Over time, the whole world was taken by surprise by the novel coronavirus. Since inter-country travel restrictions were delayed, migration had concomitantly caused the spread of coronavirus to countries outside China. The USA and many European countries such as Italy, Spain, Iran, France and the UK started accounting for their losses. African countries are not exempted, as the first case of COVID-19 was discovered in Egypt on 14 February (World Health Organisation 2020). In Nigeria, the recorded coronavirus index case was in Lagos on February 27 in respect of an Italian national who flew in from Milan, a hotspot in Italy (Nigeria Centre for Disease Control 2020). By the second week of the third month in the first quarter of 2020 (March 11 precisely), there was a declaration of a pandemic while it was evident that 114 countries had been affected by COVID-19 with 118,000 cases worldwide and a global death toll of 4291 persons (World Health Organisation 2020). Individual countries’ attempts at combating the spread of COVID-19 were not proactive because many lately started responding with travel restrictions to and fro places of high cases of coronavirus infections and deaths.
The global public health impact of COVID-19 has been enormous, severe and grievous since its outbreak. Aside from the health impact of the virus, the situation around COVID-19 has social, economic and political dimensions (Akanmu et al. 2020; Demirbas et al. 2020; Lebni et al. 2020; Nakaduna et al. 2021). Foremost, the economies of countries affected by the COVID-19 pandemic took a severe downturn as different sectors of the economy including transportation, tourism and travel, entertainment, education and finance were affected by the COVID-19 quarantine and lockdown measures (Dey and Loewenstein 2020; US Department of Labour 2020). Besides the economically important human capital lost to COVID-19 death, there are other consequences including loss of employment, reduction in patronage, sales and revenues for businesses and reduction in family and household incomes. Socially, people’s lifestyles were disrupted by restrictions placed on social gatherings. Politically, more new policies were formulated with huge financial backing to meet the needs of the population.
In Nigeria, to be specific, the social impact comprised an increase in organised crime, rising levels of cybercrime, violent crime, gender-based domestic violence and extrajudicial killings, while palliative fraud, the spread of poverty to urban areas, underemployment and unemployment as well as hunger and starvation, among others, were found to be the economic effects of the COVID-19 pandemic (Gomment et al. 2022). Furthermore, major economic impacts are at first attributed to external shocks, including weakened global demand for oil and a global economic recession while COVID-19 only dwelt on these existing conditions to further negatively impact the nation (Andam et al. 2020). According to these authors, there are therefore four major impact channels by which the economic position of Nigeria could be measured. These are “(i) government revenue shortfalls; (ii) reduced foreign remittances; (iii) direct impacts from a 5-week “lockdown” policy that restricted movement of people and economic activities within the Federal Capital Territory (FCT) Abuja, and Kano, Lagos and Ogun States, as well state-level lockdowns lasting 8 weeks in Akwa Ibom, Borno, Ekiti, Kwara, Osun, Rivers and Taraba States; and (iv) indirect impacts of the lockdown policies on the rest of the country outside of the affected sectors or areas” (p. 146).
Notable global responses to mitigate and curb the COVID-19 pandemic are quarantine and isolation of infected persons, hand washing and sanitising, use of personal protective equipment, social distancing as well as restriction of movement, total lockdown and vaccination (Cirrincione et al. 2020; Filonchyk and Peterson 2020; Dadras et al. 2021; Odunsi et al. 2022). The COVID-19 vaccination is a latter and current response with different levels of compliance across countries (Cordina et al. 2021; Lindholt et al. 2021). Drawing on the vaccination programme in Nigeria, the government has been administering COVID-19 vaccines to its population. Some studies (Elimian et al. 2020; Okoroiwu et al. 2020; Okoroiwu et al. 2021) have provided information on the incidence of COVID-19 while others (Onanuga et al. 2020; Adeleke et al. 2022; Hassan et al. 2022; Odunsi et al. 2022; Olu-Abiodun et al. 2022) on acceptance of COVID-19 vaccines. Little is known about the incidences of the administration of vaccination vis-a-vis the incidences of COVID-19 cases in the geo-political zones in Nigeria. Hence, a dearth of information on how acceptance of the vaccines relates to cases of COVID-19 across geo-political zones in Nigeria. This raises the questions: (i) what are the incidences of COVID-19 cases across the geo-political zones? And (ii) what are the incidences of COVID-19 vaccination across the geo-political zones?
Providing answers to these questions would provide information on the nature of COVID-19 cases in the different geo-political zones in Nigeria. It would likewise provide information on the acceptance and hesitancy of the vaccine by the public in the geo-political zones. This information would help identify the health risks that COVID-19 posed to the Nigerian population in the geo-political zones in the country. The information would therefore be able to direct the approaches and strategies required for COVID-19 policy amendments and decision adjustments. Based on the foregoing, the study embarked on spatially analysing the variation in COVID-19 pandemic and the vaccination of the Nigerian population.
Literature Review: COVID-19 and Geographic Information System
Globally, spatial analysis has been used since the COVID-19 outbreak to describe and explain the geographic context of the pandemic. The contemporary spatial analysis approach is the geographic information system (GIS) which Aronoff (1989) defined as a manual or computer-based set of procedures for storing and manipulating geographically referenced data. The computer-based GIS is a system of hardware, software and processes that supports the collection, management, modification, analysis, modelling and display of geographically referenced data to solve complex planning and management challenges (Rhind 1989). It integrates different components consisting of computer software and hardware, data, methods and personnel and allows for automation and a high level of accuracy (Ali 2020). Contemporary GIS is therefore described as a science and technology that revolve around empirical methods and computer-based applications in the collection, analysis, visualisation and management of spatially referenced real-time data. In other words, a series of computerised techniques and methods are involved to acquire, analyse, display and manage real-world geographic data for policy formulation and decision-making purposes.
In 2020, numerous studies (Guan et al. 2020; Liu et al. 2020; Mo et al. 2020; Raju 2020) were published on GIS application to COVID-19 across the globe. Guan et al. (2020) earlier on reviewed 63 scholarly articles that focused on the geographical aspect of the COVID-19 pandemic using geospatial and geo-statistical analyses. The five disease mapping categories identified from the articles are spatiotemporal analysis, health and social geography, environmental variables, data mining and web-based mapping. The review is one of the early resources that provides an extensive understanding of the development of technologies used in the management of this significant pandemic of the twenty-first century while offering helpful information, insights and guides for future research and bibliographic searches. Since this first scoping review, more works have been published to demonstrate the application of GIS in COVID-19 worldwide.
Another scoping review of COVID-19 geospatial articles was conducted by Fatima et al. (2021). The authors reviewed 74 articles while focusing on four main themes which are the spatial techniques, software used and geographic extent of the selected articles. It was found that most studies were “ecological-based”. Space-time scan statistics, clustering and hotspot analysis and regression “modelling” were the most frequently employed spatial techniques. In applying spatial analysis for disease mapping, exposure mapping and epidemiological modelling, researchers employed a variety of spatial and statistical software. In addition, it is primarily concentrated in China, Brazil and the USA, which are countries in the Asian and American continents. There are still many studies published in 2021 that were not captured in the scoping review. One of these is Moazzam et al. (2021) which focused on spatiotemporal mapping of COVID-19 pandemic in Italy. The data collected on active, recovery, death and confirmed cases were from January 2020 to August 23, 2021. According to the data, the total number of reported COVID-19 cases in Italy was 4,168,699, of which 128,715 died, 3,904,429 recovered and 135,555 were still active carriers. The data were analysed using the inverse distance weighting (IDW) geospatial method. Findings revealed that the emergence of COVID-19 in Italy has significantly affected the urban areas such as Bologna, Florence, Milan, Naples and Rome. The study demonstrated how the geospatial method has played an important statistical role in tracking COVID-19 cases by identifying locations of high prevalence. Thus, spatial methods are recognised as important tools in statistically assessing the spread of disease and its control in populations.
Wang et al. (2020) worked on geospatial analysis of COVID-19 in China. The cumulative outcomes for each of confirmed, cured and death cases of the new-type corona pneumonia from January to July 2020 were connected with the vector map of China using the spatial analysis function of ArcGIS and the statistical function of Microsoft Excel. The results revealed that COVID-19 was primarily concentrated in Hubei province at the time, spreading to the nearby provinces of Hunan, Henan, Jiangxi and Anhui. In addition, only a small number of areas experienced sudden occurrences of COVID-19. Another study conducted by Jesri et al. (2021) used local indicators of spatial association (LISA) to perform the geographical analysis of COVID-19 in Qom province, Iran. The objective was to assess how geographic factors associated with the prevalence of COVID-19 infection through spatial analysis could have an impact on public health initiatives aimed at containing the virus. COVID-19 data from February 19th to September 30th, 2020 were analysed using Moran coefficient in a GIS environment, and the LISA method was used to compute the spatial autocorrelation of COVID-19 for different urban districts of the province. The study estimated the COVID-19 prevalence in the province as 356.75 per 100,000 populations and provided that its pattern of spatial distribution is clustered.
A number of studies (Szilagyi et al. 2020; Cordina et al. 2021; Guidry et al. 2021; Lindholt et al. 2021) have highlighted and discussed several factors responsible for acceptance of or hesitancy in COVID-19 vaccine. In Europe, vaccine acceptance varies greatly by country, from 83% in Denmark to 47% in France and Hungary. The non-acceptance of vaccines is linked to conspiratorial thinking, no trust in authorities and scientists and a lack of concern about COVID-19. In the USA, Cordina et al. (2021) found that respondents hesitated in taking the vaccine with 32.6% saying they were doubtful and 15.6% saying they were unwilling to receive the vaccine. The main justification given for refusing to receive the vaccine was a lack of vaccine safety. However, those who were willing to take the vaccine stated their reasons to include the belief that the COVID-19 vaccine will protect one’s health, respect for medical professionals’ opinions regarding the COVID-19 vaccine’s efficacy, having received the influenza vaccine the previous year and encouraging one’s elderly parents to receive the vaccine.
In Africa, studies (Ackah et al. 2022; Berihun et al. 2021; Dubik 2022) have also established different scenarios of vaccination in terms of acceptance and hesitation. With a focus on Nigeria, a study by Al-Mustapha et al. (2022) with 3076 recruited participants revealed a 50.7% acceptance rate for COVID-19 vaccination while a literature review (Olu-Abiodun et al. 2022) of 10 articles on the six geo-political zones of Nigeria with 9287 survey participants showed that the adult vaccination acceptance rate ranged from 20.0 to 58.2%. However, based on the true population, Odunsi et al. (2022) showed that 191 million people in Nigeria (97.95%) have not yet received their first dose of COVID-19 vaccination, which is an extremely low acceptance rate when compared to population shares overall. Not everyone who received the first dose also received the second dose, even though the low acceptance rate of the first dose was maintained. Therefore, less than 1.5 million persons (0.27%) in Nigeria have received all of their vaccination.
Using an exploratory research design, Busari and Nwokporo (2023) investigated the access to and use of COVID-19 vaccine in Ebonyi State, Nigeria. The results demonstrated that disparity exists in vaccine acceptance across urban and rural areas in Ebonyi state. This disparity is also evident in people with disabilities and those with underlying health issues. It was found that access to vaccine was moderate, with a large portion of the state’s population not obtaining the vaccine. The knowledge of peers or family members who had received the COVID-19 vaccination was one of the social determinants of health that influenced vaccine acceptance. This study concluded that there is vaccine disparity at all levels, with the donated vaccines expiring at an alarming rate despite low acceptance. However, the findings cannot be generalised for the country because the sample used is not a representative of the Nigerian population. As a result, there is a dearth of information about the country’s variance in vaccine acceptance, prompting this study.
Various determinants of the administration of COVID-19 vaccination have been documented (Abedin et al. 2021; Abubakar et al. 2021; Ayodele et al. 2021; Bhadra et al. 2021; Mishra et al. 2021; Adeleke et al. 2022; Olu-Abiodun et al. 2022). For example, Adeleke et al. (2022) indicated socioeconomic attributes including gender, age, income and religion as factors responsible for the acceptance and non-acceptance of COVID-19 vaccines in Nigeria. Olu-Abiodun et al. (2022) further stated that misinformation, worries about negative side effects and conspiracy beliefs were the causes of vaccine resistance. Inferences from the reviewed literature showed the likely causes of the low turnout rate in acceptance of COVID-19 vaccine in the geo-political zones of Nigeria. The causes include knowledge and awareness, attitude, education, culture, transparency and accountability, conspiracy theories and scepticism towards authorities and politics.
The implications drawn from the foregoing studies have shown that within the context of the COVID-19 pandemic, GIS has provided many advantages. One, GIS provides such a benefit as integrating several aspects of location-related COVID-19 data to relay real-time information on the incidence, prevalence and spread of the infection. Two, such information is necessary for monitoring, curtailment and management of the pandemic. There is, however, little information on GIS-based works relating COVID-19 cases to vaccination in Nigeria. The few available ones have addressed these events in isolation. In bridging this gap, this study presents the mapping of both the pandemic and vaccination in Nigeria, thus adding to the body of GIS and COVID-19 literature. The GIS method also provides a spatial context for the available non-spatial COVID-19 cases and vaccination data in Nigeria. Furthermore, the method provides a theoretical ground to better understand the data based on natural classification.
Materials and Methods
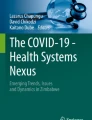
The study area is Nigeria, the sixth largest population in the world (World Population Review 2023) and the most populous country in Africa (World Population Review 2022). The country is located in West Africa and lies within longitude 3° and 14° and latitude 4° and I4°. It is bordered to the north, west, east and south by the Republic of Niger, Republic of Benin, Republic of Niger and the Atlantic Ocean, respectively. It measures an estimated 1050 km from north to south and 1200 km from east to west, thereby occupying a landmass of 923,769 km2. The country has thirty-six States and the Federal Capital Territory and is regionalised into six geo-political zones, namely: North Central, North East, North West, South East, South and South West (Fig. 1). The climatic condition of Nigeria comprises the dry and wet seasons with savannah vegetation in the North and the rain forest vegetation in the South.

The geo-political zones in Nigeria: the thirty-six states and the Federal Capital Territory (FCT) in the country by their respective geo-political zones
Nigeria is a country of 201,135,262 population (Table 1), and the major tribes in the country comprise the Yorubas, Igbos and Hausas. According to the literature (Bashir 2006; Okereke 2013; Oguche 2018; Oguche et al. 2018), the North Central is predominantly occupied by the Tiv, Idoma and Nupe; North West by the Hausa and Fulani ethnic groups and North East by the Kanuri, Tiv and Jukun. The major economic activity in this zone is agriculture including crop production and livestock rearing. The South East is occupied by the Igbo; South by the Ijaw, Itsekiri and Urhobo and South West by the Yoruba. These people are majorly involved in commercial and industrial activities. Estimations (Table 1) also indicated that the North West has a high population density, followed by the North Central, South , North East, South East and South West. The prevailing transport mode in all the geopolitical zones is by road, with several major highways linking the regions, although rail, air and water transports are operational (Oni and Okanlawon 2006; Adetola 2014).
A quantitative design was employed in this study using secondary data that were descriptively analysed. The data obtained were (1) COVID-19 cases, (2) COVID-19 vaccination, (3) population census and (4) GIS shapefiles. The COVID-19 cases data for Nigeria were downloaded from the website of Nigeria Centre for Disease Control (NCDC) (https://covid19.ncdc.gov.ng) as a comma separated value (csv) file. The COVID-19 cases data file is dated 24th October–6th November 2022 which was the last update at the time of data collection for this study. The COVID-19 vaccination data for the country were downloaded from the National Primary Health Care Development Agency (NPHCDA) (https://nphcda.gov.ng/), an agency charged with the primary health care system in Nigeria and responsible for the administration of the COVID-19 vaccines in the country. Similarly, the COVID-19 vaccination data from NPHCDA was dated 24th November 2022, being the last update at the time of data collection for this study. The dataset was downloaded as a csv file.
The currently available information on the Nigerian population is the estimated 2019 population census. The dataset was obtained from the National Population Commission as contained in the National Bureau of Statistics (2020) documentation (https://nigerianstat.gov.ng/elibrary). The GIS data comprised three different shapefiles for administrative boundaries at national/country, state and local levels, depicted as level- 0, 1 and 2 data, respectively. The level-0 data comprised only one (1) feature; the level-1 contained thirty-eight (38) features and the level-2 contained seven hundred and seventy-five (775) features. This is based on the conventional standard for shapefile designation as “endorsed by the Office of the Surveyor General of the Federal Republic of Nigeria (OSGOF) and the IMWG Feb 2017” (Humanitarian Data Exchange 2020). All these shapefiles were downloaded from an open-source website of DIVA-GIS (https://www.diva-gis.org/gdata). These data are available in the geographic coordinate system (GCS) with a global datum of WGS84 (EPSG: 4326).
The data obtained were analysed using a descriptive classification method based on the Jenks Natural Break Algorithm. The tools utilised were Microsoft Excel, version 2016 (MS Excel 2016) and ArcGIS Desktop 10.3. The csv files containing the cases of COVID-19, the distribution of COVID-19 vaccines and population census were imported into MS Excel 2016. The data collected for the Nigerian States were categorised by geo-political zones. The data were later exported as one csv file which served as attribute data in the GIS environment. The shapefiles for Nigeria were collected as designated above.
In the GIS datasets for Nigeria, shapefiles for the geo-political zones are non-existent since those available are for the country (national), states and local government areas. The way out was to produce these shapefiles. The following stages were then involved in the process: (1) the Nigeria national boundary and state shapefiles were loaded into the ArcGIS 10.3a environment from a repository on the computer desktop. (2) The state shapefiles were extracted by their geo-political zone using the attribute query, and each geo-political zone was exported as a shapefile into the repository. (3) The water body was likewise extracted using the attribute query and exported to the repository. (4) All geo-political zones and water body shapefiles were re-imported from the repository into the GIS environment. (5) Each geo-political zone shapefile was geo-processed using the Dissolved Tool. (6) All the dissolved geo-political zones’ shapefiles and that of the water body were again geo-processed using the Merge Tool.
The output of this process was the geo-political zone shapefiles of Nigeria which was further utilised in this study. As such, the csv file containing the attribute data (COVID-19 cases, COVID-19 vaccination and population census) was later joined to the Nigerian geo-political zone shapefiles. All the data were used to produce thematic maps in the GIS environment based on the Jenks natural break classification. According to Chen et al. (2013: 47), this kind of classification also termed “the Jenks optimisation method, is a data classification method designed to determine the best arrangement of values into different classes. This is done by seeking to minimise each class’s average deviation from the class mean, while maximising each class’s deviation from the means of the other groups”. In essence, the thematic maps descriptively show COVID-19 cases and the acceptance of COVID-19 vaccination using Choropleth maps. All the data was normalised using the population of each geo-political zone. The outputs were further computed in MS Excel 2016 to show the incidence of COVID-19 cases and the acceptance of COVID-19 vaccination by the share of the population across the geo-political zones.
Results and Discussion
Results on COVID-19 Cases by the Share of the Population
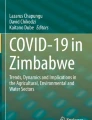
The first research question (what are the incidences of COVID-19 cases across the geo-political zones?) is answered by rating the COVID-19 cases. As presented in Fig. 2 and Table 2, the South West is rated high, the South and North Central are rated moderate and the South East, North West and North East are rated low. The Fig. 3 and Table 2 show that the South West is rated high, the South and North Central are rated moderate while the South East, North West and North East are rated low. Furthermore, the South West is rated high, the South and North Central are rated moderate and the South East, North West and North East are rated low (Fig. 4, Table 2). Lastly, Fig. 5 and Table 2 indicate that the South West and North Central are rated high, the South is rated moderate and the South East, North West and North East are rated low.

Regional distribution of COVID-19 cases: the number of confirmed cases per 100,000 population across the six geo-political zones in Nigeria

Regional distribution of COVID-19 cases: the number of recovery cases per 100,000 population across the six geo-political zones in Nigeria

Regional distribution of COVID-19 cases: the number of death cases per 100,000 population across the six geo-political zones in Nigeria

Regional distribution of COVID-19 cases: the number of active cases per 100,000 population across the six geo-political zones in Nigeria
Results on COVID-19 Vaccination by the Share of the Population
The results of the second research question (what are the incidences of COVID-19 vaccination across the geo-political zones?) are provided in this section. The results (Fig. 6, Table 3) of the first dose of COVID-19 vaccination indicate that the North West is rated high, the South West and North Central are rated moderate and the North East, South East and South are rated low. Considering the results (Fig. 7, Table 3) of the second dose, the North West is rated high the South West, North Central and North East are rated moderate and the South East and South South are rated low. The results (Fig. 8, Table 3) for the booster dose show that the North West, North Central and South West are rated high, the North East and South East are rated moderate and the South South is rated low.

Regional distribution of COVID-19 vaccinations: the number of first doses per 100,000 population across the six geo-political zones in Nigeria

Regional distribution of COVID-19 vaccinations: the number of second doses per 100,000 population across the six geo-political zones in Nigeria

Regional distribution of COVID-19 vaccinations: the number of booster doses per 100,000 population across the six geo-political zones in Nigeria
Discussion
COVID-19 is not only infectious but deadly and as a pandemic has inflicted social and economic pains on the global population. Worldwide, there are several severe cases of confirmed infected persons, recoveries and deaths. The tested and active (current) cases are not left out. The COVID-19 vaccine is an essential weapon in the fight against the pandemic, and a huge amount of resources have been invested in its development (Lindholt et al. 2021). The brands of vaccine developed and recommended by the World Health Organisation include Johnson & Johnson, Sinopharm, CanSino Biologics Ad5-nCoV-S, Pfizer-BioNTech, Sinovac, Covovax Modena (mRNA-1273), COVAXIN, Novavax and Oxford/AstraZeneca. The vaccine is expected to be widely accepted as a way to control the spread of the virus to mitigate its negative impacts. However, many people in both developed and developing countries have shown different dispositions to the acceptance of COVID-19 vaccines at personal and public levels.
In Nigeria, COVID-19 cases and dispositions to acceptance of the vaccine require urgent attention through the lens of the data obtained by dedicated government agencies. In the North Central region, this study found a moderate incidence of confirmed, recovery and death cases of COVID-19. This region also had moderate incidences of the first and second doses of COVID-19 vaccination and a high incidence of booster dose. This may suggest that the people in the North Central region are more receptive to the COVID-19 vaccination programme and are likely to comply with booster dose recommendations. The North East region, on the other hand, had low incidences of COVID-19 cases, indicating that the preventive measures put in place might be working in this region. However, the low incidences of the first dose of the COVID-19 vaccination may suggest that the people in this region may be less receptive to the vaccine or have limited access to it. The moderate incidences of the second and booster doses could suggest that the vaccination campaign has been effective in convincing people who initially refused to take the vaccine. In the North West region, all COVID-19 cases showed low incidences. This is a positive indication and it could suggest that the preventive measures put in place, such as social distancing and wearing of face masks, are working in this region. The high incidences of vaccination in this region could indicate that the people are more receptive to the vaccination programme, or there might be better access to the vaccine in this region.
The South East region also showed all COVID-19 cases indicating low incidences which is proper for public health outcomes. However, the low incidences of the first and second doses of the vaccination suggest that the vaccination campaign may not have been as effective in this region. The moderate incidence of the booster dose could indicate that people in this region are more receptive to booster dose, or there might be better access to booster dose compared to the initial doses. The South West region showed high incidences of all COVID-19 cases. This situation is alarming. However, the moderate incidences of the first and second doses could suggest that people in this region are receptive to the vaccination programme. The high incidence of the booster dose could indicate that the people in this region are more receptive to booster dose, or there might be better access to booster dose in this region. The South South region has moderate incidences of all COVID-19 cases. This could suggest that the preventive measures put in place, such as social distancing and wearing of face masks, are working in this region. However, the low incidences of all doses of the vaccination could suggest that the vaccination campaign may not have been as effective in this region.
Understanding the underlying factors that might be responsible for the observed variations in COVID-19 cases and vaccination rates across the regions is crucial. However, the findings of this study have been unable to provide the factors influencing acceptance and hesitancy of the vaccines and the rationales behind them. This is because they are not inherent in the available data. The rationales are, however, not farfetched being the results of current research. For instance, the population density of a region might affect the spread of COVID-19 in line with provisions of extant studies (Abubakar et al. 2021; Ayodele et al. 2021; Bhadra et al. 2021). More so, the availability and accessibility of COVID-19 vaccines might also vary across the regions, and this might impact the vaccination rates. These issues have also been put forward in literature (Abedin et al. 2021; Mishra et al. 2021). To sum up, since vaccination, alongside other preventive measures such as social distancing and wearing of face masks, are essential to controlling the spread of COVID-19 in Nigeria, and all its regions, tailoring the preventive measures to suit the peculiarities of each region in the country is significant.
Conclusion and Implications
The study focused on COVID-19 pandemic and the vaccination in Nigeria. In summarising the findings, the North Central, with moderate incidences of COVID-19 confirmed, recovery and death cases, has moderate incidences of first and second doses of COVID-19 vaccination and a high incidence of the booster dose. The North East which has low incidences of COVID-19 cases has a low incidence of the first dose of the vaccination and moderate incidences of the second and booster dose. In the North West, all the COVID-19 cases showed low incidences but the vaccination showed high incidences. The South East also has all the COVID-19 cases indicating low incidences with the first and second doses of the vaccination also indicating low incidences, but the booster dose indicated a moderate incidence. The South West showed high incidences of all COVID-19 cases, moderate incidences of the first and second doses, but a high incidence of the booster dose. Finally, the South South indicated moderate incidences of all the COVID-19 cases but low incidences of all the doses of the vaccination.
This study concludes that there is a regional variation in the incidences of COVID-19 cases and the administration of COVID-19 vaccination in Nigeria. Although the study employed a basic descriptive analysis, the results are generalisable as the COVID-19 data collected are about the Nigerian population (true population not sample population). Hence, the analysis requires no inferential statistics indicating causality between COVID-19 incidence and acceptance of COVID-19 vaccines. Based on the findings, it is recommended that the population of South West Nigeria should be more cautious of COVID-19 protocol and should also respond more to the COVID-19 vaccination programme. In addition, it is crucial to ensure that there is equitable access to vaccines across all regions of Nigeria to achieve herd immunity and control the spread of COVID-19. It is therefore recommended that the Nigerian government should intensify efforts towards creating awareness about the importance of taking the COVID-19 vaccine, especially in regions with high incidences of COVID-19 cases and among populations with lower vaccination rates. This could be done through community engagement programmes, mass media campaigns and other targeted interventions.
Finally, the peculiarities of each zone in terms of cultural practices, population density and transport, among others, might have contributed to the variation that is evident in this study. Further studies are therefore required to confirm the underlying factors responsible for these variations and tailor preventive measures and vaccination campaigns to suit the peculiarities of each region. It should also be noted that the study has a limitation which suggests that the COVID-19 data utilised are likely to be dated at the publication period with more updates released by agencies in charge. It is therefore expected that this kind of study will continue into the future as much as more updated COVID-19 data are made available.
Data Availability
The datasets generated and/or analysed during the current study are available in the Nigeria Centre for Disease Control (NCDC), National Primary Health Care Development Agency (NPHCDA), National Bureau of Statistics (NBS) and DIVA-GIS repositories, (https://covid19.ncdc.gov.ng, https://nphcda.gov.ng/, https://nigerianstat.gov.ng/elibrary and https://www.diva-gis.org/gdata) respectively.
References
Abedin M, Islam MA, Rahman FN, Reza HM, Hossain MZ, Hossain MA, Arefin A, Hossain A (2021) Willingness to vaccinate against COVID-19 among Bangladeshi adults: understanding the strategies to optimize vaccination coverage 2021. PloS One 16(4):e0250495
Abubakar I, Dalglish SL, Ihekweazu CA, Bolu O, Aliyu SH (2021) Lessons from co-production of evidence and policy in Nigeria’s COVID-19 response BMJ. Global Health 6(3):e004793
Ackah BBB, Woo M, Stallwood L et al (2022) COVID-19 vaccine hesitancy in Africa: a scoping review Global Health Res Policy, 7(21), 1-20 https://doi.org/10.1186/s41256-022-00255-1
Adeleke OR, Adegboro JS, Olofintuyi OO, Ayenigbara IO, Aina SI, Fadero EO, Oluwadare RS, Olaseyo T (2022) Factors of predicting the acceptance of the COVID-19 vaccine in West Africa: a cross-sectional study in Nigeria. J Appl Health Sci 81(8):5–13
Adetola AE (2014) A conceptual collaborative engagement framework for road infrastructure management in Nigeria, Doctoral dissertation. University of Central Lancashire
Akanmu AA, Salisu UO, Daramola OP, Ogunsesan AS, Fasina SO, Adejare JA, Sanni SM, Olatunji OM (2020) Dynamics of security and socio-economic challenges of COVID-19 lockdown measures in Nigeria. Afr J Sci Nature 11:215–229
Ali E (2020) Geographic information system (GIS): definition, development, applications & components. Department of Geography, Ananda Chandra College
Al-Mustapha AI, Okechukwu O, Olayinka A et al (2022) A national survey of COVID-19 vaccine acceptance in Nigeria. Vaccine 40(33):4726–4473. https://doi.org/10.1016/j.vaccine.2022.06.050
Ayodele KP, Jimoh H, Fagbamigbe AF, Onakpoya OH (2021) The dynamics of COVID-19 outbreak in Nigeria: a sub-national analysis. Sci Afr 13:e00914
Bashir A (2006) Settlements patterns dynamics in the Northeast region of Nigeria: implications for locality identification for national population and housing census. Glob J Soc Sci 5(2):69–75
Berihun G, Walle Z, Berhanu L, Teshome D (2021) Acceptance of COVID-19 vaccine and determinant factors among patients with chronic disease visiting Dessie Comprehensive Specialized Hospital, Northeastern Ethiopia. Patient Prefer Adherence 15:1795–1805. https://doi.org/10.2147/ppa.s324564
Bhadra A, Mukherjee A, Sarkar K (2021) Impact of population density on Covid-19 infected and mortality rate in India. Model Earth Syst Environ 623:–9
Busari DA, Nwokporo EI (2023) Equity, access and utilization of COVID-19 vaccine in Ebonyi State, Nigeria. J Geovis Spat Anal 7:24. https://doi.org/10.1007/s41651-023-00154-0
Chen J, Yang S, Li H, Zhang B, Lv J (2013) Research on geographical environment unit division based on the method of natural breaks (Jenks). ISPRS. https://doi.org/10.5194/isprsarchives-XL-4-W3-47-2013
Cirrincione L, Plescia F, Ledda C, Rapisarda V, Martorana D, Moldovan RE, Theodoridou K, Cannizzaro E (2020) COVID-19 pandemic: prevention and protection measures to be adopted at the workplace. Sustainability 12:3603. https://doi.org/10.3390/su12093603
Cordina M, Lauri MA, Lauri J (2021) Attitudes towards COVID-19 vaccination, vaccine hesitancy and intention to take the vaccine. Pharm Pract 19(1):2317. https://doi.org/10.18549/pharmpract.2021.1.2317
Dadras O, Alinaghi SAS, Karimi A et al (2021) Effects of COVID-19 prevention procedures on other common infections: a systematic review. Eur J Med Res 26(1):67. https://doi.org/10.1186/s40001-021-00539-1
Demirbas D, Bozkurt V, Yorgun S (2020) The COVID-19 pandemic and its economic, social, and political impacts Istanbul. Istanbul University Press, Turkey
Dey M, Loewenstein M (2020) How many workers are employed in sectors directly affected by COVID-19 shutdowns, where do they work, and how much do they earn? Mon Labor Rev. https://doi.org/10.21916/mlr.2020.6
Dubik SD (2022) Understanding the facilitators and barriers to COVID-19 vaccine uptake among teachers in the Sagnarigu Municipality of Northern Ghana: a cross-sectional study. Risk Manag Healthc Policy 15:311–322. https://doi.org/10.2147/rmhp.s352584
Elimian KO, Ochu CL, Ilori E et al (2020) Descriptive epidemiology of coronavirus disease 2019 in Nigeria, 27 February - 6 June 2020. Epidemiol Infect 148:e208. https://doi.org/10.1016/j.ijid.2020.11.012
Fatima M, O’Keefe KJ, Wei W, Arshad S, Gruebner O (2021) Geospatial analysis of COVID-19: a scoping review. Int J Environ Res Public Health 18:2336. https://doi.org/10.3390/ijerph18052336
Filonchyk M, Peterson M (2020) Air quality changes in Shanghai, China, and the surrounding urban agglomeration during the COVID-19 lockdown. J Geovis Spat Anal 4:22. https://doi.org/10.1007/s41651-020-00064-5
Gomment TI, Musa AB, Audu M, Akpata OG, Kashim A, Alih L (2022) The impact of COVID-19 pandemic on Nigeria: a substantial threat to the attainment of sustainable development goals (SDGs). J Sustain Dev Afr 24(1):43–54
Gross B, Zheng Z, Liu S et al (2020) Spatio-temporal propagation of COVID-19 pandemics. Europhysics Letters 131(5):58003
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Zhong NS (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 382(18):1708–1720
Guidry JPD, Laestadius LI, Vraga EK et al (2021) Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am J Infect Control 49(2):137–142. https://doi.org/10.1016/j.ajic.2020.11.018
Hassan A, Hassan Z, Muhammad H (2022) Assessment of COVID-19 vaccine acceptance and willingness to pay by Nigerians. Health 14:137–157. https://doi.org/10.4236/health.2022.141011
Human Rights Watch (2021) Between hunger and the virus: the impact of the COVID-19 pandemic on people living in poverty in Lagos, Nigeria. United States of America, Human Rights Watch
Humanitarian Data Exchange (2020) Nigeria: subnational administrative boundaries OCHA, Centre for Humanitarian Data https://datahumdataorg/m/dataset/cod-ab-nga? Access 19th December 2022
Kamel Boulos MN, Geraghty EM (2020) Geographical tracking and mapping of coronavirus disease COVID-19/severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic and associated events around the world: how 2first century GIS technologies are supporting the global fight against outbreaks and epidemics. Int J Health Geogr 19(1):1–12
Lebni JY, Abbas J, Moradi F, Salahshoor MR, Chaboksavar F, Irandoost SF, Nezhaddadgar N, Ziapour A (2020) How the COVID-19 pandemic effected economic, social, political, and cultural factors: a lesson from Iran International. J Soc Psychiatry 67(3). https://doi.org/10.1177/0020764020939984
Lindholt MF, Jørgensen F, Bor A, Peterson MB (2021) Public acceptance of COVID-19 vaccines: cross-national evidence on levels and individual-level predictors using observational data. BMJ Open 11:e048172. https://doi.org/10.1136/bmjopen-2020-048172
Liu Q, Sha D, Liu W et al (2020) Spatiotemporal Patterns of COVID-19 Impact on human activities and environment in mainland China using nighttime light and air quality data. Remote Sens (Basel) 12(10):1576. https://doi.org/10.3390/rs12101576
Mishra A, Sutermaster S, Smittenaar P, Stewart N, Sgaier SK (2021) COVID-19 Vaccine Coverage Index: identifying barriers to COVID-19 vaccine uptake across US counties MedRxiv. Jun 22:2021-06.
Mo C, Tan D, Mai T, Bei C, Qin J, Pang W, Zhang Z (2020) An analysis of spatiotemporal pattern for COIVD-19 in China based on space-time cube. J Med Virol 92(9):1587–1595. https://doi.org/10.1002/jmv.25834
Nakaduna Y, Ahmad AA, Mohammed MO (2021) Economic and political implications of covid-19 pandemic: a case of Nigeria. Asian People J 4(1):34–49. https://doi.org/10.37231/apj.2021.4.1.243
National Bureau of Statistics (2020) Demographic statistics bulletin. A Publication of Demographic Statistics Division, National Bureau of Statistics, Nigeria
National Health Commission of the People’s Republic of China (NHCPRC) (2020) Guideline for Psychological Crisis Intervention during 2019-nCoV. National Health Commission of the People’s Republic of China http://www.nhc.gov.cn/jkj/s3577/202001/6adc08b966594253b2b791be5c3b9467.shtml
Odunsi OM, Onanuga MY, Adeleke OR, Sowole PA, Owolabi OA (2022) Regional analysis of acceptance of COVID-19 vaccines in Nigeria. J Appl Health Sci 8(2):251–259. https://doi.org/10.24141/1/8/2/12
Oguche D (2018) The state of institutional repositories and scholarly communication in Nigeria. Glob Knowl Mem Commun 67(1/2):19–33
Oguche D, Kundu S, Mondal P, Isibika IS, Kavishe GF, Lwoga ET, Sukums F, Rasaki EO, Abioye A, Chaputula AH, Mutula S (2018) Glob Knowl Mem Commun. https://doi.org/10.1108/GKMC-04-2017-0033
Okereke CNE (2013) Anatomy of conflicts in Northern Nigeria. In: State Fragility, State Formation, and Human Security in Nigeria, pp 147–187
Okoroiwu HU, Ogar CO, Nja GME, Abunimye DA, Ejemot-Nwadiaro RI (2021) COVID-19 in Nigeria: account of epidemiological events, response, management, preventions and lessons learned. GERMS 11(3):391–402. https://doi.org/10.18683/germs.2021.1276
Okoroiwu HU, Uchendu IK, Ogar CO, Okafor M (2020) COVID-19 in Nigeria: situation update and combative measures taken by the government. GERMS 10(3):274–278. https://doi.org/10.18683/germs.2020.1218
Olu-Abiodun O, Abiodun O, Okafor N (2022) COVID-19 vaccination in Nigeria: a rapid review of vaccine acceptance rate and the associated factors. PloS One 17(5):e0267691. https://doi.org/10.1371/journal.pone.0267691
Onanuga MY, Odunsi OM, Onafeso OD (2020) Spatial variation of COVID-19 in Southwestern Nigeria. Afr J Sci Nat 11:123–136
Oni SI, Okanlawon K (2006) Nigeria’s transport infrastructural development: an integral part of the national economic empowerment and development strategy (NEEDS). J Soc Policy Issues 3(2):7–13
Raju K (2020) Application of GIS in COVID -19 monitoring and surveillance. Int J Res Appl Sci Eng Technol 8:1435–1440. https://doi.org/10.22214/ijraset.2020.5231
Szilagyi PG, Thomas K, Shah MD et al (2020) National trends in the US public’s likelihood of getting a COVID-19 vaccine. JAMA 325(4):396–398. https://doi.org/10.1001/jama.2020.26419
US Department of Labour (2020) COVID-19 impact: the COVID-19 virus continues to impact the number of initial claims and insured unemployment. In: Employment and Training Administration, Washington, DC
Wang X, Zhou Q, He Y et al (2020) Nosocomial outbreak of COVID-19 pneumonia in Wuhan, China. Eur Respir J 55(6):2000544
World Population Review (2022) Countries in Africa 2022 https://worldpopulationreviewcom//country-rankings/countries-in-africa Accessed 2nd December 2022
World Population Review (2023) Nigeria population. https://worldpopulationreview.com/countries
Wu JT, Leung K, Leung GM (2020) Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: a modelling study. Lancet 395(10225):689–697. https://doi.org/10.1016/s0140-6736(20)30260-9
Zhu H, Wei L, Niu P (2020) The novel coronavirus outbreak in Wuhan, China. Glob Health Res Policy 5(6). https://doi.org/10.1186/s41256-020-00135-6
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by OMO, UOS, AOT, BOO, AIB, SOF, OTD, NOO, SOM, TMA, ORA and GAO. The first draft of the manuscript was written by OMO, UOS, AOT and MYO, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical Approval
No requirement for ethical approval for this study in Nigeria as the data utilised are secondary and readily available in public databases.
Informed Consent
No informed consent is required because the study involved no primary human participants. The publicly available data being utilised by this study are without any disclosure of personal and sensitive information as well as re-identification of individuals.
Competing Interests
The authors declare no competing interests.
Compliance with Ethical Standards
The article adheres to all ethical standards as contained in the Committee on Publication Ethics (COPE) guidelines.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Odunsi, O.M., Salisu, U.O., Taiwo, A.O. et al. Geo-Visualisation of COVID-19 Pandemic and Vaccination in Nigeria: a Regional Approach. J geovis spat anal 7, 29 (2023). https://doi.org/10.1007/s41651-023-00159-9
Accepted:
Published:
DOI: https://doi.org/10.1007/s41651-023-00159-9