
Abstract
Though studies on multidimensional poverty have been gaining research and programmatic attention, no attempt has been made to understand the association of multidimensional poverty with consumption poverty in India. Using data from the National Family Health Survey-4, 2015–16, this paper examined the association and spatial clustering of multidimensional and consumption poverty in the districts of India. Context-specific indicators were chosen to provide robust estimates of multidimensional poverty. The Alkire and Foster method was used to estimate the indices of multidimensional poverty. The spatial patterns of multidimensional and consumption poverty were examined using Moran’s I statistics, Local Indicator of Spatial Association, and cluster maps. A set of spatial regression models was used to understand the predictors of multidimensional poverty. The results suggest that 30.3% of the population in India was multidimensionally poor, with an average intensity of poverty of 44.2% and a multidimensional poverty index of 0.13. The state variations in multidimensional poverty were high. The univariate Moran’s I statistic of multidimensional poverty was 0.75, while that of consumption poverty was 0.56, suggesting that multidimensional poverty was spatially clustered. Though spatial regression model shows multidimensional poverty is positively associated to consumption poverty, the extent of association is limited. Besides, fertility level, share of rural population, health insurance, and percentage of scheduled caste population were significant predictors of multidimensional poverty. Based on the results, we suggest that multidimensional poverty measures may be integrated along with consumption poverty and that districts with high levels of multidimensional and consumption poverty should be prioritized for evidence-based planning.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Poverty reduction remains a major challenge worldwide. Globally, an estimated 783 million people live below USD 1.90 per person per day, and 1300 million people are multidimensionally poor (OPHI, 2019; World Bank, 2018). The progress in the reduction of both money-metric and multidimensional poverty has been slow and largely uneven within and across countries. Reduction of multidimensional poverty is a priority developmental agenda globally, nationally, and locally. Goal 1 of the Sustainable Development Goals (SDGs) aims to eradicate poverty in all its forms by 2030 (UN SDGs, 2015). Estimating multidimensional poverty is useful for tracking the progress of SDGs and national developmental programs. Many national governments have intensified efforts to reduce the extent of multidimensional poverty in recent decades.
Conceptualizing and measuring poverty is challenging for academia and policy makers. Conventional poverty is primarily measured within the economic domain and drawn from income or consumption data. The World Bank uses the international poverty line (USD 1.90 PPP), while the national governments adopt varying methods to estimate the poverty level. The national estimates of money-metric poverty are often context-specific, follow absolute and relative approach in poverty measurement, do not capture the non-monetary aspects of poverty, and are not comparable across countries. Some countries use consumption and expenditure criteria, while others use income-based poverty line in their official estimates of poverty (Haughton & Khandker, 2009). The concept of multidimensional poverty is a comprehensive one and captures multiple deprivations such as deprivation in material well-being, health, nutrition, education, and other key aspects of human development. The need for measuring poverty in multiple domains was emphasized in the capability approach, where poverty was defined as the lack of an individual’s ability to lead a fully functioning life (Sen, 1985). There has been growing interest in the measurement and applications of multidimensional poverty in recent years. Many countries, including Bhutan, Chile, Costa Rica, Columbia, Ecuador, El Salvador, Honduras, and Mexico have integrated national estimates of poverty with the multidimensional nature of poverty. For instance, the Government of Columbia has estimated multidimensional poverty by incorporating five dimensions (household education condition, childhood and youth condition, employment, health, and access to public utilities and housing condition) and used it in their poverty reduction plan (Angulo et al., 2016).
Studies on multidimensional poverty focus on methodological development, developing context-specific dimensions and indicators, making empirical estimates, and delineating determinants of multidimensional poverty. Methodological development includes the use of union and intersection approach, fuzzy set approach, axiomatic approach, and relative and absolute factor analysis (Anand & Sen, 1997; Bourguignon & Chakravarty, 2003; Gordon et al., 2003; Chakravarty & D’Ambrosio, 2006; Wagle, 2008; Alkire & Foster, 2011; Coromaldi & Zoli, 2012; Alkire et al. 2015). The dimensions range from education, health, living standard, and environment to women empowerment, social security, energy, and health insurance, among others. (Alkire & Seth, 2015; Bader et al., 2016; Dehury & Mohanty, 2015; Gerlitz, 2015; Mishra & Ray, 2013; Mishra & Shukla, 2016). A number of studies have provided empirical estimates on multidimensional poverty using various methods (Alkire & Santos, 2010; Alkire et al., 2017; Hanadita & Tampubolon, 2016; Jayaraj & Subramanian, 2010; Mohanty, 2011; Mohanty et al., 2018; Montoya & Teixeira, 2017).
For the last ten years, the Oxford Poverty and Human Development initiative (OPHI) has been providing the estimates of multidimensional poverty indices for about 100 countries (Alkire et al., 2019). It provides estimates for three common indices, namely poverty head count ratio, intensity of poverty, and multidimensional poverty index (MPI) (Alkire & Foster, 2011; Alkire & Santos, 2013). A set of ten indicators, in the dimensions of knowledge, health, and living standard, is used for estimating multidimensional poverty indices. The estimates of multidimensional poverty vary from as high as 91.9% in South Sudan to as low as 0.19% in Armenia (OPHI, 2019).
India is the second most populous country in the world and is home to 176 million poor people (accounting for nearly 25% of the global poor) (World Bank, 2018). The national estimates of poverty are based on the calorie intake derived from the consumption expenditure data collected by the National Sample Survey. The country has made a significant improvement in the reduction of money-metric poverty, from 37% in 2004–05 to 22% by 2011–12 (Government of India Planning Commission, 2013). Nonetheless, the non-monetary estimates of poverty remain high. About two-fifths of children are stunted or underweight (IIPS 2017). Premature mortality is on the rise, and accessible basic health care services are beyond the reach of the poor and marginalized in rural India (Dubey & Mohanty, 2014; Iyengar & Dholakia, 2012). Though educational enrolment at the primary level has been increasing, the average years of schooling remain low (IIPS 2017). In this context, the aim of this paper is to examine the spatial patterns of consumption and multidimensional poverty in districts of India. The paper has been conceptualised with the following rationale.
First, though the national and global efforts to incorporate multidimensional poverty have been intensified at the policy level, little is known about the association of money-metric and multidimensional poverty at the sub-national level. Studies suggest that increase in the economic well-being of households does not necessarily reduce the extent of multidimensional poverty (Klasen, 2000; Meyer & Sullivan, 2012; Suppa, 2016; Wang, 2016). Using longitudinal data, a study suggested that while children living in monetary poverty are more likely to stay in multidimensional poverty, children who escape from monetary poverty do not necessarily exit from multidimensional poverty either (Kim, 2019). There is no study that explores the association of multidimensional and consumption poverty in districts of India. Second, the global multidimensional poverty index, using uniform dimensions and indicators, does not capture the extent of multidimensional poverty in the developed states of India. For example, the estimated multidimensional poverty is 1% in Kerala, 5% in Sikkim, and 52.5% in Bihar (OPHI, 2018). Third, the districts of India are large and a key administrative unit in the country. The national and state averages conceal the large variations in the poverty level among the districts of India. As of Census 2011, there were 640 districts of India, with large variations in the level of development. Districts are not homogenous in the level of development and exhibit considerable variations in the key dimensions of human development (Khan & Mohanty, 2018). Given this, it is pertinent to make a spatial analysis to identify the clusters of districts with high consumption and high multidimensional poverty so as to target poverty geographically. Such an analysis would be very helpful in planning and implementing poverty alleviating programs more effectively.
2 Data and Methodology
2.1 Data Source
We used the unit data from the National Family Health Survey, round 4 (NFHS-4), 2015–16, for the analysis. NFHS-4 was a nation-wide, large-scale cross-sectional demographic health survey that provided demographic, socio-economic and health information at the household and individual levels. It interviewed a sample of 601,509 households, 699,686 women in the age group 15–49, and 112,122 men in the age group 15–54. The details of the sampling design, the survey instruments, and the findings are available in the national report of the survey (IIPS 2017). NFHS-4 provided detailed information on a wide range of variables relating to fertility, mortality, reproductive health, child nutrition, child mortality, immunization, birth history of women, and household characteristics (housing amenities, sanitation, water, and living standard). The survey was designed to provide estimates at the district, state and national levels in India. It covered all 640 districts, with an average number of 940 households from each district. We utilized unit level information on mortality, child health, education, and basic housing amenities to estimate multidimensional poverty at the level of districts and states of India. The district level estimates of consumption poverty were taken from the published source (Mohanty et. al., 2016). Consumption poverty in the districts of India was estimated from the consumption data contained in the National Sample Survey (NSS).
2.2 Methodology
We used descriptive statistics, estimated indices of multidimensional poverty, and carried out spatial analysis. Descriptive analyses were used to understand the variations in multidimensional poverty across the districts of India. The Alkire and Foster (AF) methodology was used to estimate the indices of multidimensional poverty. The methodology uses the dual cut-off method in which the poor are identified for each weighted indicator and then aggregated into different dimensions. It helps in decomposing the multidimensional poverty index into different dimensions/indicators and geographical locations, which aids in evidence-based planning. In this paper, we considered three dimensions, namely, education, health, and standard of living, along the lines of the global MPI specification. However, we used context-specific indicators in each of the dimensions. Each indicator was directly or indirectly related to the SDG indicators. Of the ten indicators, eight (school attendance, nutrition, electricity, sanitation, drinking water, cooking fuel, housing, and assets) were similar to the global MPI; their inclusion in the index has been described elsewhere (Alkire & Kanagartnam, 2018). Two indicators, namely child mortality and years of schooling, were revised/modified to suit the Indian context. The inclusion of premature mortality in place of child mortality was due to the high premature mortality in India (Dubey & Mohanty, 2014). As for years of schooling, we used the cut-off point of eight years of schooling given that school attendance among those aged 7–14 years has been increasing in the last two decades. Even the eligibility to work in the organized sector is a minimum of ten years of schooling in India. Both indicators cover all ages. The description of the dimensions, the indicators, the cut-off point, and the weights has been given in Table 1. Equal weights were assigned to each dimension, and within each dimension, equal weights were given to each indicator. Three types of estimates were made: percentage of multidimensionally poor (H), intensity of poverty (A), and multidimensional poverty index (MPI). A brief description of each of these indices is given below.
Percentage of multidimensionally poor is denoted by H and defined as:
where q is the number of people who are multidimensionally poor, and n is the total population.
Intensity of poverty is denoted by A and defined as:
where c is the deprivation score that the poor experienced. Intensity of poverty is a weighted average deprivation experienced by the multidimensionally poor. We presented A in terms of percentage for the convenience of interpreting the results (Table 2).
Multidimensional poverty index is denoted by MPI and calculated as:
MPI is the product of the proportion of the multidimensionally poor and the intensity of poverty. MPI provides the index value and suggests the share of the population that is multidimensionally poor and adjusted by the intensity of deprivation suffered.
In addition to these three indices, we estimated severe multidimensional poverty and vulnerability to multidimensional poverty. Severe multidimensional poverty is defined as deprivation in more than 50% of weighted indicators, whereas vulnerability to multidimensional poverty is defined as deprivation in 20% of weighted indicators (Alkire & Kanagartnam, 2018).
Next, we decomposed the MPI by dimensions and indicators to assess the contribution of the various dimension/indicators to overall poverty. The contribution of a particular indicator to overall multidimensional poverty was computed as:
where \(w_{i}\) is the weight of the \(i^{th}\) indicator (given in Table 1) and \({\text{CH}}_{i}\) is the censored head count ratio of the \(i^{th}\) indicator. Censored head count ratio of the \(i^{th}\) indicator is defined as the proportion of people who are multidimensionally poor and deprived in the \(i^{th}\) indicator.
3 Spatial Analysis
The spatial analysis was done to understand the spatial dependence and clustering of multidimensional and consumption poverty in India. The practice of spatial analysis is motivated by Waldo Tobler’s first law of geography, and its use has been increasing in recent decades in the various domains such as health, demography, and economics. (Remirez & Loboguerrero, 2002; Anselin et al. 2004; Lolayekar & Mukopadhyay 2019; Monica & Mishra, 2020). For our analysis, we used univariate and bivariate Moran’s I statistic and a set of spatial regression models. Moran’s I statistic and Local Indicators of Spatial Association (LISA) cluster and significance maps were used to examine the spatial autocorrelation and the spatial clustering patterns of multidimensional and consumption poverty in the districts of India. The analysis was performed with the help of GIS (ArcGis and Geoda). Moran’s I statistic gives the global spatial autocorrelation of variables, which provides the degree of association (Anselin, 1995). Univariate Moran’s I statistic is computed as:
where \({x}_{i}\) and \({x}_{j}\) are consumption/multidimensional poverty in districts \(i\) and \(j\) and N is the total number of districts.
We used the queen contiguity weight matrix of order one since it uses both common boundaries and corners to define neighbors. More specifically, \(W\) is \(\left(N\times N\right)\) weight matrix, with element \({W}_{ij}\) representing the interaction between district \(i\) and \(j\). \({W}_{ij}\) is equal to 1 if \(i\) and \(j\) share a common boundary and corner, and 0 otherwise (Khomiakova, 2008).
Moran’s I statistic ranges from − 1 to + 1, where a positive value indicates the clustering of similar attribute values, and a negative value indicates the clustering of dissimilar values. A zero value indicates a random distribution, with no spatial autocorrelation. Global Moran’s I statistic provides a single value of association, helping to understand the spatial autocorrelation as a whole. It does not, however, reveal the spatial clustering patterns in regional or sub-regional locations. Hence, we estimated univariate and bivariate local Moran’s I statistics (Anselin, 2013) and generated the LISA cluster and significance maps to understand the spatial clustering patterns of multidimensional and consumption poverty in districts of India. The Monte Carlo simulation computation technique was used to examine the significance of Moran’s I statistic. Univariate LISA statistics was computed as follows:
Local Moran’s I statistic generates four types of spatial association: high-high association (hot spot) and low-low association (cold spot), which indicate spatial clustering of similar values, and high-low association and low–high association, which indicate clustering of dissimilar values in the neighborhood area (spatial outlier) (Anselin, 2013).
A set of regression models were used to identify the correlates associated with multidimensional poverty across the districts of India. First, we used the ordinary least square (OLS) model to understand the preliminary association of multidimensional poverty with its correlates. The OLS model was used for diagnostic testing. Estimated Moran’s I statistic in the residuals was significant (see Table 3), confirmed a significant spatial autocorrelation in the residuals. Hence, the OLS model was found to be inefficient to produce reliable results, and we proceeded with the spatial error and spatial lag models. Since our objective was to predict multidimensional poverty by its correlates, considering the neighborhood effect among the districts of India, we determined that the spatial lag model (also known as spatial autoregressive model) and the spatial error model were best suited to our study. The spatial lag model (SLM) considers the endogenous interaction effect, explaining the spatial dependency among the dependent variables in the neighborhood area, while the spatial error model (SEM) explains the spatial autocorrelation among the disturbance terms (or error terms) in the neighborhood area. The spatial error model, unlike the spatial lag model, takes into account the effect of the omitted variables which are not present in the model but may affect it.
Subsequently, we carried out two Lagrange Multiplier tests (diagnostic tests to check spatial dependency and decide the most appropriate specification between spatial error and spatial lag) with the respective robust versions of both the models. Since the value of the Lagrange Multiplier for each of the model was significant (\(p<0.0001)\), we compared the Akaike information criterion (AIC) value to identify the final model. The SEM model was found to be the best fit since the AIC value of the model was lower and its log likelihood value greater than that of the other model. The basic linear regression model (OLS) can be expressed as:
where \(Y_{i}\) is the dependent variable in the \(i^{th}\) district, \(\alpha\) and \(\beta\) are the parameters to be estimated, \(X_{i}\) is the vector of the explanatory variable, and \(\in_{i}\) is the disturbance term assumed to be independently and identically distributed (i.i.d.). If spatial autocorrelation is found to be significant in disturbance terms, the OLS model provides biased and inconsistent estimates of the model parameter. To control the effect of the spatial interaction, we used the SLM and SEM models as given below.
The spatial lag model can be expressed mathematically as:
where \(\rho\) is the spatial lag parameter, and \(W_{y}\) is the spatial weightatrix explaining the endogenous interaction effect.
The spatial error model can be expressed as:
where \(Y_{i}\) denotes the percentage of the multidimensionally poor in the \(i^{th}\) district\(,\) \(\beta\) denotes the regression coefficient, \(\lambda\) is the spatial autoregressive coefficient, \(W_{{ij{ }}}\) is the spatial weight explaining the interaction effect among the disturbance terms of proximity between districts \(i\) and \(j\), \(Y_{j}\) is the percentage of the multidimensionally poor in the \({j}^{th}\) district, \({\epsilon }_{j}\) is the residuals, and \({X}_{j}\) is the predictor variable. Predictor variables included in the study are as follows: consumption poor, no health insurance, rural population, scheduled caste, scheduled tribe, Muslim population, and the Total fertility rate (TFR) in the \({j}^{th}\) district. The choice of these explanatory variables was guided by the exclusion of the variables used in the estimation of multidimensional poverty as well as by data constraints. Since our primary interest was with regards to the association of consumption and multidimensional poverty, consumption poverty was taken as the main independent variable. Health insurance was included because it is an important variable to save households from catastrophic health spending (Ranjan et al., 2018). Similarly, rural areas were included because the extent of multidimensional poverty is higher in those areas. The inclusion of the SCs and STs was guided by the fact that they are a marginalized population and have a higher incidence of deprivation (Meenakshi at el., 2000). Similarly, the demographic factor, such as fertility level proxied by TFR, is an important correlate of poverty. The description of summary statistics of the variables used in the analysis has been given in Table 4. To understand the role of the omitted variables, an SEM model was estimated, including the variables used in Eq. 9 and the ten indicators used in the estimation of multidimensional poverty (Appendix A.3).
4 Result
4.1 Descriptive Statistics
Table 4 presents the mean, standard deviation, minimum, maximum, and Moran’s I of the variables used in the analysis. The distribution of the variables suggests the wide variation of dependent and independent variables in districts of India. The multidimensional poverty in India was estimated at 30%, with the lowest in the Kottayam district (0.6%) of Kerala and highest in the Alirajpur district (78.5%) of Madhya Pradesh in India. Similarly, the average consumption poverty across districts of India was estimated at 33%, with a standard deviation of 18.6%. The average share of the Muslim population was also varied from as high as more than 99% to as low as low as less than 1%. A similar pattern of variation was observed for scheduled caste and scheduled tribe in India. Three-fourth of the population in India was not covered with any health insurance scheme. It varied from 12.3% in the Bijapur district to almost 99% in the Senapati district of India. The average Total fertility rate across districts of India was 2.8 in India. Moran’s I statistics suggests multidimensional poverty was more cluster than consumption poverty. It was highest for TRF (0.77) and lowest for the proportion of the rural population (0.42).
4.2 Multidimensional Poverty Indices Across States of India
Table 2 presents multidimensional poverty indices in India. In India, 30.3% of the population were multidimensionally poor, 19% were vulnerable to multidimensional poverty, and 6.7% were severely multidimensionally poor; the MPI was estimated at 0.13. The state variations in the multidimensional poverty estimates were very large. The extent of multidimensional poverty was the highest in Bihar (57%), followed by Jharkhand (49.7%), and Uttar Pradesh (43.6%). Kerala had the lowest percentage of multidimensionally poverty (1.8%), followed by Sikkim (5.4%), Delhi (5.6%), and Chandigarh (5.7%). The MPI varied from 0.01 in Kerala to 0.27 in Bihar. About 11 of 36 states had higher multidimensional poverty than the national average. About 19% population was severely multidimensionally poor in Jharkhand, followed by 12% in Uttar Pradesh, and 10.7% in Assam.
4.3 Robustness of Multidimensional Poverty
A robustness test for the multidimensional poverty estimates was performed by varying the cut-off points (k) of the weighted deprivation vector for the rural and urban areas. When the poverty cut-off point was 10%, multidimensional poverty was estimated to be 82% in rural areas and 46% in urban areas. When k was increased to 30%, multidimensional poverty decreased to 40% in rural areas and to 11% in urban areas. We found multidimensional poverty to be higher in the rural areas compared to the urban ones at each poverty cut-off point (Fig. 1).

Percentage of multidimensional poverty (H) in rural and urban India for varying cut-off points
4.4 Decomposition of Multidimensional Poverty in India
Multidimensional poverty was decomposed to understand the distinct contribution of various dimensions and indicators to multidimensional poverty in India. Figure 2 shows the contribution of different indicators to the multidimensional poverty index in India. Among the ten indicators, undernutrition contributed the highest (about 26%) to multidimensional poverty, followed by years of schooling (21%). Unimproved sanitation and asset ownership were found to contribute the least to multidimensional poverty at 2.8% and 3.2% respectively. Among the three domains, standard of living contributed the most (41.6%) to multidimensional poverty, followed by health (31.6%) and education (26.7%).

Percentage contribution of indicators to multidimensional poverty in India, 2015–16
4.5 Multidimensional Poverty Across Districts of India
Figure 3 presents the multidimensional poverty indices in the districts of India. More than one-fourth of the districts (179 out of 640 districts) had less than 15% of the multidimensionally poor people (districts shown in leafy green). Multidimensional poverty was the highest in the Alirajpur district (78.5%) of Madhya Pradesh, followed by Shrawasti (76.7%) in Uttar Pradesh. It was the lowest in the Kottayam district of Kerala (0.6%) followed by Ernakulam (0.8%) and Khozikode (1.1%). About 45% of the districts (300 districts) were estimated to have multidimensional poverty higher than the national average. The multidimensional poverty index was also found to be the highest in the district of Alirajpur (0.410), followed by Shrawasti (0.395), and to be the lowest in the district of Kottayam (0.002), followed by Ernakulam (0.003). The extent of multidimensional poverty varied greatly among districts within a state. For example, in Maharashtra, Nadurbar district had the highest percentage of multidimensionally poor (64.4%), while Mumbai had the lowest percentage (4.5%). Figure 4 depicts the consumption poverty in districts of India. About 15% of people were living below the consumption poverty level in 111 districts of India. The extent of consumption poverty varied from over 90% in the Malkangiri district in Odisha to less than 1% in the West Kemang district in Arunachal Pradesh.

Percentage of multidimensionally poor in districts of India, 2015–16

Consumption poverty in the districts of India, 2011–12
4.6 Spatial Clustering of Consumption and Multidimensional Poverty
Figure 5a and b present the univariate Moran’s I statistic, depicting the extent of spatial autocorrelation of consumption and multidimensional poverty in the districts of India. The univariate Moran’s I value for consumption poverty was 0.56, and that of multidimensional poverty was 0.75. These estimates show a clear spatial pattern of autocorrelation in both consumption and multidimensional poverty. Multidimensional poverty showed a higher level of spatial clustering than consumption poverty. Consumption poverty and multidimensional poverty have been abbreviated as consu_etry and HCR respectively in the following graphs and maps.

a Scatter plot of consumption poverty and Moran’s I statistic in the districts of India; b Scatter plot of multidimensional poverty and Moran’s I statistic in the districts of India
4.7 Univariate LISA Cluster Map
Univariate LISA cluster and significance maps were generated to identify the clustering patterns of consumption and multidimensional poverty. Figure 6a and b present the univariate LISA cluster and significance maps (\(p\hspace{0.17em}\)< 0.05) of consumption poverty in the districts of India. The LISA significance map shows that 286 of 640 districts (45% of all districts) were clustered significantly. The LISA cluster map shows a clear pattern of clustering in consumption poverty in the districts of India. It identifies 123 of 640 districts as hot spots (shown in red color), indicating the clustering of a high level of consumption poverty among the neighboring districts. These districts were mainly in the states of Bihar, Uttar Pradesh, and Jharkhand. About 22% of all districts (138 out of 640 districts) can be seen as cold spots (shown in blue color), which shows the clustering of a low level of consumption poverty among the neighboring districts.

a Univariate LISA cluster map of consumption poverty in the districts of India; b Univariate LISA significance map of consumption poverty in the districts of India
Figure 7a and b depict the univariate LISA cluster and significance maps (\(p\) < 0.05) of multidimensional poverty in the districts of India. About 50% of all the districts (321 out of 640 districts) were clustered significantly (Fig. 7b). The LISA cluster map suggests that 144 districts were classified as hot spots (shown in red color), indicating clustering of districts with similarly high multidimensional poverty. These districts were mainly in the states of Uttar Pradesh, Bihar, Jharkhand, Chhattisgarh, Odisha, and parts of Assam. By contrast, 167 of 321 districts were identified as cold spots (shown in blue color), indicating clustering of similarly low multidimensionally poor neighboring districts. Appendix A.2 also presents the bivariate Moran’s I and LISA cluster and significant maps of multidimensional and consumption poverty in the districts of India.

a Univariate LISA cluster map of multidimensional poverty in districts of India; b Univariate LISA significance map of multidimensional poverty in districts of India
4.8 Spatial Regression Model
Table 3 provides the estimated results from the Ordinary Least Square (OLS), Spatial Lag Model (SLM), and Spatial Error Model (SEM) for percentage of multidimensional poverty in districts, India, 2015–16. First, we examined the association of multidimensional poverty with a set of predictors at the district level using the OLS estimation model. The results suggest that TFR, share of rural population, and consumption poverty were significant predictors of multidimensional poverty. However, the diagnostic test of the OLS model in the subsequent step provided the spatial autocorrelation among the residuals (Moran’s I = 0.43, p value = 0.00001), which can also be seen in the residual map (see appendix Fig A.1). Additionally, the residuals were not normally distributed (Jarque–Bera statistics, p value < 0.05). Hence, the results obtained from the OLS model were not reliable.
Since, the results of the both tests, namely the Lagrange multiplier test and the robustness test for the error and lag models were statistically significant (indicating spatial lag and error dependence in the data), it was difficult to identify the best fit model. Hence, we employed both the spatial lag model and the spatial error model (Table 3). Between the two of them, the spatial error model showed a lower AIC and a higher log likelihood and, so, was considered the best fit in our data. Results of SEM model suggest that the coefficient of consumption poverty was 0.12, suggesting that a 10% decrease in consumption poverty was associated with a 1.2% decrease in multidimensional poverty. It also found TFR, rural residence, scheduled caste, and health insurance to be significant predictors of multidimensional poverty. The coefficient of TFR was 10.05, indicating that multidimensional poverty would decrease by 10% if TFR declined by 1 unit. Not being covered with health insurance and belonging to a scheduled caste meant being more likely to be multidimensionally poor. The SEM showed a pseudo R square value of 0.88, indicating that the model explained 88% of the variations in multidimensional poverty with the help of the predictors (Table 3).
5 Discussion and Conclusion
Though studies on multidimensional poverty are increasingly available in India, the association of consumption and multidimensional poverty has not been examined. This is the first ever study that aims to understand the association of multidimensional and consumption poverty in the districts of India. Earlier studies were limited to providing only estimates at state/district level (Alkire et al., 2018; Mehta, 2003) and did not examine the association of consumption and multidimensional poverty in the districts of India. We chose district as the unit of analysis as district is a key administrative unit in India and shows large variations in the level of socio-economic development. The number of districts are large enough (640) to draw valid inferences. We estimated multidimensional poverty by using three dimensions and ten indicators, using the Alkire-Foster (AF) method. While for eight of the ten indicators, are similar to global MPI, we modified two indicators, namely years of schooling and premature mortality. Under the education domain, a household is considered deprived if no one in the household has completed eight years of schooling and a school-age child (up to class 8) is not attending school. Given the increase in educational attainment across states and socio-economic groups, this is a reasonable assumption. Premature mortality, that includes any death under age 70, was also included as an indicator. The rationale behind including this context-specific indicator was that child mortality has been declining and has remained low in many parts of the country, while adult mortality is on the rise. The estimates of consumption poverty at the district level were taken from the published paper of Mohanty et al., 2011. We also believed that multidimensional and consumption poverty are spatially correlated as there is a geographic concentration of poverty in the country. The following are the salient findings of the study.
First, at the national level, 30.3% of the population was multidimensionally poor and 6.7% was severely multidimensionally poor. Over half of the population in the state of Bihar was multidimensionally poor, while only 10% or less of the population was so in the developed sates of Tamil Nadu (8.8%), Himachal Pradesh (8.2%), Punjab (7.8%), Goa (6.7%), and Kerala (1.7%). The district variations in multidimensional poverty were large within and among the states of India. About 25% of the districts had less than 15% multidimensional poverty, and about 20% of the districts had more than 50% multidimensional poverty.
Second, the decomposition of multidimensional poverty by its indicators suggests that among the ten indicators, the undernutrition made the largest contribution (26%) to multidimensional poverty, followed by years of schooling (21%). Hence, improving undernutrition and educational attainment are a prerequisite to reducing multidimensional poverty in India. Third, the spatial analysis shows a clear pattern of clustering in multidimensional poverty and consumption poverty across the districts of India. The univariate Moran’s I statistic of multidimensional poverty was 0.75, suggesting that the extent of spatial clustering in multidimensional poverty was high across the districts of India and was higher than that of consumption poverty (0.56). The geographical locations of hot and cold spots were identified for multidimensional and consumption poverty from the LISA significance and cluster maps. About half of districts for multidimensional (50%) and consumption poverty (45%) were observed significantly clustered.. Fourth, the multivariate analysis suggested that TFR, share of rural population, scheduled caste, and health insurance are significant predictors of multidimensional poverty in India.
We put forward some plausible explanations in support of the results. Our estimates of a high incidence of multidimensional poverty in the poorer states of Bihar, Jharkhand, Uttar Pradesh, Madhya Pradesh, and Odisha are consistent with literature (Alkire et al., 2018). These states are historically under-developed, with low level of industrialization, low infrastructural development, high population growth, and low literacy rate. However, our findings also suggest high intra-state and inter-district variations in multidimensional poverty. The spatial clustering of multidimensional poverty suggests that many of the districts are clustered in regions/states. Similarly, the moderate association of multidimensional and consumption poverty suggests that districts with a low level of consumption poverty do not necessarily have low multidimensional poverty.
We now put forward some limitations of the study. First, our estimates of multidimensional poverty were primarily dependent on the NFHS-4 data that had only a limited number of variables to measure the missing dimensions of employment, environment, and energy. We believe that the estimates would have been higher had these domains been included. Second, our analysis relates to the pre-COVID situation and does not capture the increase in multidimensional poverty due to the pandemic. Third, the analysis was limited to districts and did not extend to smaller units such as blocks or villages due to the limited size of the sample. Despite these limitations, we believe that the paper contributes to the literature on multidimensional poverty.
Here are the implications of the study. First, we suggest that multidimensional poverty be included in the official estimation of poverty. Estimates of both consumption and multidimensional poverty may be provided at the state and district levels. Second, this study is helpful in understanding the spatial variations in consumption and multidimensional poverty in the districts of India. The district variations are very large and uneven, suggesting the need for a greater focus on the districts with high consumption and multidimensional poverty to achieve the poverty eradication goal. The spatial association of consumption and multidimensional poverty was revealed to be statistically significant in our study and helped identify the cluster of districts with high multidimensional and consumption poverty in India. Reduction of consumption poverty alone is not sufficient to reduce multidimensional poverty. Improving educational attainment and making secondary education compulsory for children can reduce educational deprivation. Besides, implementing health-specific intervention programs, improving water quality, increasing sanitation coverage, and using safe cooking fuel through an integrated multisectoral approach are needed to reduce multidimensional poverty in India.
Data Availability
The unit label data is available online form Demographic Health Survey (DHS) data repository and could be accessed upon a data request through www.dhsprogram.com/data/ (DHS, 2018).
References
Alkire, S., & Foster, J. (2011). Counting and multidimensional poverty measures. Journal of Public Economics, 95(7–8), 476–487.
Alkire, S., Foster, J. E., Seth, S., Santos, M. E., Roche, J. M., & Ballon, P. (2015). Overview of methods for multidimensional poverty assessment. In S. Alkire, J. E. Foster, S. Seth, M. E. Santos, J. M. Roche, & P. Ballon (Eds.), Multidimensional poverty measurement and analysis (pp. 70–122). Oxford University Press.
Alkire, S., & Kanagaratnam, U. (2018). Multidimensional Poverty Index Winter2017–18: Brief methodological note and results. OPHI Methodological Notes, 45.
Alkire, S., Kanagaratnam, U., & Suppa, N. (2019). The Global Multidimensional Poverty Index (MPI) 2019. OPHI MPI Methodological Note 47, Oxford poverty and human development initiative, University of Oxford. Available from: https://ophi.org.uk/ophi-mpi-methodological-note-47/.
Alkire, S., Oldiges, C., & Kanagaratnam, U. (2018). Multidimensional poverty reduction in India 2005/6–2015/16: still a long way to go but the poorest are catching up. Oxford Poverty and Human Development Initiative (OPHI).
Alkire, S., Roche, J. M., & Vaz, A. (2017). Changes over time in multidimensional poverty: Methodology and results for 34 countries. World Development, 94, 232–249.
Alkire, S., & Santos, M. E. (2010). Acute multidimensional poverty: A new index for developing countries. OPHI working paper No. 38. Available at: https://ophi.org.uk/acute-multidimensional-poverty-a-new-index-for-developing-countries/.
Alkire, S., & Santos, M. E. (2013). A multidimensional approach: Poverty measurement & beyond. Social Indicators Research, 112(2), 239–257.
Alkire, S., & Seth, S. (2015). Multidimensional poverty reduction in India 1999–2006: Where and How? World Development, 72, 93–108.
Anand, S., & Sen, A. (1997). Concepts of human development and poverty: A multidimensional perspective. Oxford University Press.
Angulo, R., Díaz, Y., & Pardo, R. (2016). The Colombian multidimensional poverty index: Measuring poverty in a public policy context. Social Indicators Research, 127(1), 1–38.
Anselin, L. (1995). Local indicators of spatial association—LISA. Geographical Analysis, 27(2), 93–115.
Anselin, L. (2013). Spatial econometrics: methods and models (Vol. 4). Dordrecht: Springer Science & Business Media.
Anselin, L., Bongiovanni, R., & Lowenberg-DeBoer, J. (2004). A spatial econometric approach to the economics of site-specific nitrogen management in corn production. American Journal of Agricultural Economics, 86(3), 675–687.
Bader, C., Bieri, S., Wiesmann, U., & Heinimann, A. (2016). A different perspective on poverty in Lao PDR: Multidimensional poverty in Lao PDR for the years 2002/2003 and 2007/2008. Social Indicators Research, 126(2), 483–502.
Bourguignon, F., & Chakravarty, S. R. (2003). The measurement of multidimensional poverty. The Journal of Economic Inequality, 1(1), 25–49.
Chakravarty, S. R., & D’Ambrosio, C. (2006). The measurement of social exclusion. Review of Income and Wealth, 52(3), 377–398.
Coromaldi, M., & Zoli, M. (2012). Deriving multidimensional poverty indicators: Methodological issues and an empirical analysis for Italy. Social Indicators Research, 107(1), 37–54.
Dehury, B., & Mohanty, S. K. (2015). Regional estimates of multidimensional poverty in India. Economics Open-Assessment E-Journal, 9, 1–35.
DHS (2018) The DHS program: Demographic and health surveys. Rockville: ICF Macro. www.dhsprogram.com/data/
Dubey, M., & Mohanty, S. K. (2014). Age and sex patterns of premature mortality in India. British Medical Journal Open. https://doi.org/10.1136/bmjopen-2014-005386
Gerlitz, J. Y., Apablaza, M., Hoermann, B., Hunzai, K., & Bennett, L. (2015). A multidimensional poverty measure for the Hindu Kush-Himalayas, applied to selected districts in Nepal. Mountain Research and Development, 35, 278–288.
Gordon, D., Nandy, S., Pantazis, C., Pemberton, S., & Townsend, P. (2003). The distribution of child poverty in the developing world. Bristol: Centre for International Poverty Research.
Government of India Planning Commission. (2013). Press notes on poverty estimates, 2011-12. Retrieved from: https://niti.gov.in/sites/default/files/2020-05/press-note-poverty-2011-12-23-08-16.
Hanandita, W., & Tampubolon, G. (2016). Multidimensional poverty in Indonesia: Trend over the last decade (2003–2013). Social Indicators Research, 128(2), 559–587.
Haughton, J., & Khandker, S. R. (2009). Handbook on poverty and inequality. World Bank.
IIPS. (2017). International Institute for Population Sciences (IIPS) and ICF. National family health survey (NFHS-4), 2015–16: India. Mumbai: IIPS.
Iyengar, S., & Dholakia, R. H. (2012). Access of the rural poor to primary healthcare in India. Review of Market Integration, 4(1), 71–109.
Jayaraj, D., & Subramanian, S. (2010). A Chakravarty-D’Ambrosio view of multidimensional deprivation: Some estimates for India. Economic and Political Weekly, 45(6), 53–65.
Khan, J., & Mohanty, S. K. (2018). Spatial heterogeneity and correlates of child malnutrition in districts of India. BMC Public Health, 18(1), 1–13.
Khomiakova, T. (2008). Spatial analysis of regional divergence in India: Income and economic structure perspectives. International Journal of Economic Policy Studies, 3(1), 137–161.
Kim, H. (2019). Beyond monetary poverty analysis: The dynamics of multidimensional child poverty in developing countries. Social Indicators Research, 141(3), 1107–1136.
Klasen, S. (2000). Measuring poverty and deprivation in South Africa. Review of Income and Wealth, 46(1), 33–58.
Lolayekar, A. P., & Mukhopadhyay, P. (2019). Spatial dependence and regional income convergence in India (1981–2010). GeoJournal, 84(4), 851–864.
Meenakshi, J. V., Ray, R., & Gupta, S. (2000). Estimates of poverty for SC, ST and female-headed households. Economic and Political Weekly, 35, 2748–2754.
Mehta, A.K. (2003). Multidimensional poverty in India: District level estimates, CPRC-IIPA Working Paper No. 9, Chronic Poverty Research Centre (CPRC), Manchester, UK. Retrieved from http://www.chronicpoverty.org/publications/details/multidimensional-poverty-in-india-district-level-estimates.
Meyer, B. D., & Sullivan, J. X. (2012). Identifying the disadvantaged: Official poverty, consumption poverty, and the new supplemental poverty measure. Journal of Economic Perspectives, 26(3), 111–136.
Mishra, A., & Ray, R. (2013). Multi-dimensional deprivation in India during and after the reforms: Do the household expenditure and the family health surveys present consistent evidence? Social Indicators Research, 110(2), 791–818.
Mishra, U. S., & Shukla, V. (2016). Welfare comparisons with multidimensional well-being indicators: An Indian illustration. Social Indicators Research, 129(2), 505–525.
Mohanty, S. K. (2011). Multidimensional poverty and child survival in India. PLoS ONE, 6(10), e26857.
Mohanty, S. K., Govil, D., Chauhan, R. K., Kim, R., & Subramanian, S. V. (2016). Estimates of poverty and inequality in the districts of India, 2011–2012. Journal of Development Policy and Practice, 1(2), 142–202.
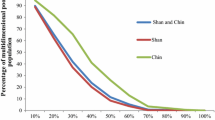
Mohanty, S. K., Rasul, G., Mahapatra, B., Choudhury, D., Tuladhar, S., & Holmgren, E. V. (2018). Multidimensional poverty in mountainous regions: Shan and Chin in Myanmar. Social Indicators Research, 138(1), 23–44.
Monica., & Mishra, R., (2020). An epidemiological study of cervical and breast screening in India: district-level analysis. BMC Women's Health, 20, 225.
Montoya, Á. J. A., & Teixeira, K. M. D. (2017). Multidimensional poverty in Nicaragua: Are female-headed households better off? Social Indicators Research, 132(3), 1037–1063.
Oxford Poverty & Human Development Initiative. (2019). “Global Multidimensional Poverty Index 2019: Illuminating Inequalities”. Oxford: OPHI. https://ophi.org.uk/global-multidimensional-poverty-index-2019-illuminating-inequalities/.
Ramirez, M. T., & Loboguerrero, A. M. (2002). Spatial dependence and economic growth: Evidence from a panel of countries. Borradores de Economia Working Paper, (206). Available at SSRN https://papers.ssrn.com/sol3/papers.cfmabstract_id=1756883.
Ranjan, A., Dixit, P., Mukhopadhyay, I., & Thiagarajan, S. (2018). Effectiveness of government strategies for financial protection against costs of hospitalization care in India. BMC Public Health, 18(1), 501.
Sen, A. K. (1985). Commodities and capabilities. Oxford University Press.
Suppa, N. (2016). Comparing monetary and multidimensional poverty in Germany. OPHI Working Papers, (103). University of Oxford, Oxford.
UN SDGs. (2015). Transforming our world: The 2030 Agenda for Sustainable Development. A/RES/70/1. Available from: https://sustainabledevelopment.un.org/post2015/transformingourworld.
Oxford Poverty and Human Development Initiative. (2018). Global multidimensional poverty index 2018: The most detailed picture to date of the world’s poorest people. Oxford: University of Oxford.
Wagle, U. R. (2008). Multidimensional poverty: An alternative measurement approach for the United States? Social Science Research, 37(2), 559–580.
Wang, X., Feng, H., Xia, Q., & Alkire, S. (2016). On the relationship between income poverty and multidimensional poverty in China. OPHI Working Papers, (101). Oxford: University of Oxford.
World Bank. (2018). Poverty and shared prosperity 2018: Piecing together the poverty puzzle. Washington, DC: World Bank. https://doi.org/10.1596/978-1-4648-1330-6.
Funding
No financial disclosures were reported by the authors of this paper.
Author information
Authors and Affiliations
Contributions
Conceptualisation: GV and SKM, Analyses: GV, Draft: GV and SKM Edit and comment: SKM and GV.
Corresponding author
Ethics declarations
Conflict of interest
All authors have indicated no potential conflict of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix
Appendix A.1: OLS Residuals Standard Deviation Map

Appendix A.2
3.1 Bivariate Moran’s I statistic
The bivariate Moran’s I statistic was estimated to understand the spatial correlation of consumption and multidimensional poverty in the districts of India (Fig.

Bivariate Moran’s I statistic for consumption and multidimensional poverty in districts of India
8). Spatial correlation between consumption and multidimensional poverty was estimated at 0.58, suggesting that consumption poverty was spatially associated with multidimensional poverty in the districts of India. However, the association was not strong. There are four quadrants in the graph showing the different types of association of multidimensional and consumption poverty. The upper right quadrant and the lower left quadrant show a positive association of high consumption and high multidimensional poverty and low consumption and low multidimensional poverty respectively.
3.2 Bivariate LISA Cluster and Significance Maps
Figure

a Bivariate LISA cluster map of consumption and multidimensional poverty in the districts of India; b Bivariate LISA significance map of consumption and multidimensional poverty in the districts of India
9a and b depict the bivariate LISA cluster and significance map (\(p\)<0.05) of consumption and multidimensional poverty in the districts of India. The bivariate cluster map indicates one-fifth of all districts (138 of 640 districts) as hot spots (shown in red), where people lived in a high level of consumption poverty along with a high level of multidimensional poverty. These districts were mainly in the states of Bihar, Uttar Pradesh, Jharkhand, West Bengal, Madhya Pradesh, and Assam. About 142 districts constituted cold spots (low level of consumption poverty and low level of multidimensional poverty) from a few states of southern India and few states of northern India, including Himachal Pradesh, Jammu and Kashmir, and Punjab. While multidimensional and consumption poverty were not spatially associated in 314 districts (about 49% of all the districts), districts with high multidimensional poverty were not necessarily high in consumption poverty or vice versa.
Appendix A.3: Estimated Result from the Spatial Error Model for Percentage of Multidimensional Poverty in Districts, India, 2015–16.
District level correlates of multidimensional poverty | Percentage of multidimensional poor | ||
|---|---|---|---|
Coef | Std. error | P-value | |
Percentage of consumption poor | 0.003 | 0.006 | 0.000 |
Percentage of Muslim population | − 0.005 | 0.007 | 0.499 |
Percentage of schedule tribe | 0.012 | 0.005 | 0.028 |
Percentage of schedule caste | − 0.007 | 0.011 | 0.508 |
Percentage population not covered with health insurance | − 0.007 | 0.006 | 0.239 |
Percentage of rural population | − 0.033 | 0.007 | 0.000 |
Total fertility rate | 0.907 | 0.234 | 0.000 |
Percentage of water deprivation | 0.096 | 0.007 | 0.000 |
percentage of sanitation deprivation | 0.115 | 0.008 | 0.000 |
percentage of floor deprivation | 0.195 | 0.008 | 0.000 |
percentage of cooking fuel deprivation | 0.056 | 0.010 | 0.000 |
percentage of assess deprivation | 0.086 | 0.018 | 0.000 |
percentage of electricity deprivation | 0.130 | 0.011 | 0.000 |
percentage of premature mortality | 0.296 | 0.056 | 0.000 |
Percentage of undernutrition | 0.374 | 0.017 | 0.000 |
Percentage children not attending school | 0.234 | 0.039 | 0.000 |
Percentage of children deprived in 8 years of schooling | 0.385 | 0.019 | 0.000 |
Lambda value (Log coefficient) | 0.648 | 0.037 | 0.000 |
Log likelihood | −1349.561 | ||
AIC value | 2735.12 | ||
Pseudo R square | 0.99 | ||
No of districts | 640 | ||
This is a diagnosis exercise to understand the role of the omitted variables, including the variables used in Eq. 9 and the ten indicators used in the estimation of multidimensional poverty. Results show a minimal association of consumption and multidimensional poverty. Increase in rural population was associated with decrease in multidimensional poverty. While other predictors (Muslim, scheduled tribe, and health insurance) were not significant. Besides, the model reports R2 of 0.99, which is not reliable and gives the biased results. The SEM model provided in Eq. 9 was found to fit our study best.
Rights and permissions
About this article

Cite this article
Vasishtha, G., Mohanty, S.K. Spatial Pattern of Multidimensional and Consumption Poverty in Districts of India. Spat Demogr 9, 213–240 (2021). https://doi.org/10.1007/s40980-021-00089-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40980-021-00089-4