
Abstract
Purpose
To evaluate the clinicopathological entities of adult granulosa cell tumor of ovary.
Method
A retrospective analysis of ten cases of adult granulosa cell tumor of ovary managed in a tertiary care center (VPS Lakeshore hospital, Kochi) from 2004 to 2018.
Results
Ten cases were identified to have adult granulosa cell tumor (GCT). Mean age was 45.3 years (range 31–63 years). Irregular cycles, palpable mass and pain abdomen were presenting complains. Palpable abdomino-pelvic mass was present in 7 (70%). Only one case had preoperative rise in serum Ca125 level. Serum inhibin analysis was done in postoperative period only, and one case had raised inhibin. Out of ten cases, 6 underwent laparoscopic surgery for adnexal mass and diagnosis of GCT was made in the final histopathology report. Five of them underwent completion surgery later on. Adjuvant chemotherapy was given in three of the cases. Total of 7 cases (70%) had recurrence. Pelvis was common site of recurrence, and mean duration of recurrence was 5.08 years (24–132 months). Mean disease-free period was 3.97 years (6–132 months). There were four mortalities. The longest follow-up duration for single case till the date was 13 years with recurrence in between.
Conclusion
Granulosa cell tumor of ovary is rare form of ovarian malignancy. Stage is the important prognostic factor. It has good prognosis compared to epithelial ovarian neoplasm. It is difficult to predict preoperatively. Care should be taken to prevent spillage while dealing with adnexal mass which occurs commonly in minimal access surgery and mini-laparotomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Granulosa cell tumor (GCT) is a rare ovarian tumor originating from sex cord stromal cells [1]. It accounts for 3–5% of all ovarian malignancies and 70% of sex cord stromal tumor [2,3,4]. It has indolent course, and clinical features are sometimes related to functional nature of the tumor. Tumor markers are serum inhibin, estrogen, anti-Mullerian hormones, follicle regulatory protein (FRP) and CA 125 [1, 4]. Treatment is individualized and depends on age, stage and future fertility plan. Prognosis is good compared to ovarian epithelial tumors. GCT is either juvenile or adult type.
Adult type is a common one and represents 95% of GCT [5]. These two have separate epidemiological, clinical and pathological nature. This study is to evaluate clinicopathological features of adult granulosa cell tumor.
Materials and methods
This is a hospital-based, retrospective descriptive study of patients attending Gynecologic Oncology department of VPS Lakeshore hospital—Cochin, Kerala. All cases of adult granulosa cell tumor of ovary attaining medical or surgical oncology units were listed from the hospital records from 2004 to 2018. Clinical details were obtained from hospital record section. Telephonic interview was made to get information where necessary. Cases were labeled as lost to follow-up when information could not be obtained for the last 6 months. Statistical analysis was done with SPSS program 16.
Results
Ten cases of adult granulosa cell tumor were identified from 2004 to 2018. All cases were primarily managed outside the center by the general gynecology department and later presented to this hospital for further evaluation. Different clinical characteristics of patients, primary management done for adnexal mass and stage of disease and recurrence were analyzed as shown in Tables 1, 2 and 3 respectively. Cases with recurrence and mortality were further analyzed and results are shown in Tables 4 and 5.
Discussion
Granulosa cell tumor of ovary is considered as low-grade malignancy that originates from sex cord stromal cells. It is a rare variant of ovarian tumor and constitutes less than 5% of all ovarian malignancies [6]. Rokitansky first described it in 1855 [7]. Its incidence has been reported ranging from 0.5 to 1.5 per 100,000 women per year [6]. Seventy percent of the cases are hormonally active. They are unilateral tumors, and chance of being bilateral is less than 5% [8]. In this study, all cases were unilateral tumors.
There are two distinct subtypes of granulosa cell tumor: adult and juvenile. Ninety-five percent of the cases are adult GCT and common in perimenopausal and postmenopausal age groups [5, 9, 10]. In this study also, both premenopausal and postmenopausal women were equally affected. However, the mean age of diagnosis (mean age 45.3 years) was early in this study group compared to age group of 50–55 years as reported in other literature [9, 10].
Common presenting symptoms are non-specific like pain abdomen and abdominal distension, or 30% cases may present with menstrual disorder secondary to hormonal function of the tumor [1, 10,11,12,13]. These were also common in this study. During fertile period, it is associated with nulliparity [14]. The functional nature of the tumor can lead to other gynecological conditions like endometrial hyperplasia and leiomyomas [9, 10]. Endometrial cancer may be associated in later part of life with the increase in age [14]. In this study, there was no nulliparous woman and mean parity was 2.4 (minimum 1 to maximum 3). Endometrial pathology was not evaluated before surgery. This reason could be due to primary pathology attributed to pelvic mass itself. However, none had any endometrial pathology in the final report in the hysterectomy specimen.
Radiologically, it was a large pelvic mass measuring up to 12 cm in diameter with solid and multicystic component similar in this study also [15]. The size of mass correlates with the prognosis of the tumor [15]. Inhibin is a usual tumor marker for both primary and recurrent diseases [16]. But in this study, inhibin study was done in postoperative period only after the final histopathology report, which may be due to low level of suspicion at the time of presentation.
Management is individualized depending upon age, stage and future fertility plan. Laparoscopic management is contro versial. Exploration of cases managed with laparoscopy is found to have peritoneal disease [17]. However, Nakayama et al. have shown that laparoscopic outcome is reasonable with similar outcome as in laparotomy [18]. In this study also, 60% cases were managed with laparoscopy and recurrence is seen high in this group (4 out of 6 cases, i.e., 66.66%).
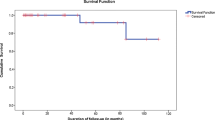
Median duration for recurrence is reported as 4–5 years [19]. In this study, pelvis was the most common site for recurrence and mean duration of recurrence was 61 months (5.08 years). Median relapse-free survival in the literature has been reported as 8.4 years [20]. But in this study, it was found to be 3.9 years only. There were in total four mortalities: 2 each in laparoscopy group and non-laparoscopy group, and all mortalities were due to disease process that occurred due to recurrence and during further management.
Initial stage is the single most important prognostic factor for granulosa cell tumor. Age at time of presentation and presence or absence of residual disease are other important prognostic factors. Tumor size less than 10 cm has also been reported as a favorable prognostic factor [1, 21].
Conclusion
Adult granulosa cell tumor is rare form of ovarian malignancy. It has good prognosis compared to epithelial ovarian neoplasm. A long-term follow-up is suggested due to the chance of late recurrence. Spillage should be avoided specially in laparoscopic surgery and mini-laparotomy.
Change history
03 January 2020
The article “Adult Granulosa Cell Tumor of Ovary: Clinical Study of 10 Cases,” written by S. Kayastha, was originally published electronically on the publisher’s Internet portal (currently SpringerLink) on November 15, 2019, with open access.
References
Sekkate S, Kairouani M, Serji B, Tazi A, Mrabti H, Boutayeb S, Errihani H. Ovarian granulosa cell tumors: a retrospective study of 27 cases and a review of the literature. World J Surg Oncol. 2013;11:142.
Malmström H, Högberg T, Risberg B, Simonsen E. Granulosa cell tumors of the ovary: prognostic factors and outcome. Gynecol Oncol. 1994;52:50–5.
Ayhan A, Salman MC, Velipasaoglu M, Sakinci M, Yuce K. Prognostic factors in adult granulosa cell tumors of the ovary: a retrospective analysis of 80 cases. J Gynecol Oncol. 2009;20:158–63.
Pectasides D, Pectasides E, Psyrri A. Granulosa cell tumor of the ovary. Cancer Treat Rev. 2008;34:1–12.
Bryk S, Färkkilä A, Bützow R, Leminen A, Heikinheimo M, Anttonen M. Clinical characteristics and survival of patients with an adult-type ovarian granulosa cell tumor: a 56-year single-center experience. Int J Gynecol Cancer. 2015;25:33–41.
Duraisamy YD, Balasubramaniam D, Chinnusamy P, Barnwal R. Case series of rare ovarian malignancy: granulosa cell tumor. Int J Res Med Sci. 2017;5:723.
Rokitansky CV. Uberabnormalitiaten des corpus luteum. Allg Wien Med Z. 1859;4:253–8.
Maleemonkol S, Chareonium V, Isariyodom P, Faichamnan S. Granulosa cell tumor of the ovary. J Med Assoc Thai. 1996;79:648–53.
Ukah CO, Ikpeze OC, Eleje GU. Adult granulosa cell tumor associated with endometrial carcinoma: a case report. Eke ACJ Med Case Rep. 2011;5:340.
Adhikari RC, Jha A, Shayami G. Granulosa cell tumor of the ovary: a clinicopathological study of six cases. J Pathol Nepal. 2011;1:96–9.
Outwater EK, Wagner BJ, Mannion C, McLarney JK, Kim B. Sex cord-stromal and steroid cell tumors of the ovary. Radiographics. 1998;18:1523–46.
Stuart GC, Dawson LM. Update on granulosa cell tumours of the ovary. Curr Opin Obstet Gynecol. 2003;15:33–7.
Ranganath R, Sridevi V, Shirley SS, Shantha V. Clinical and pathologic prognostic factors in adult granulosa cell tumors of the ovary. Int J Gynecol Cancer. 2008;18:929–33.
Unkila-Kallio L, Tiitinen A, Wahlström T, Lehtovirta P, Leminen A. Reproductive features in women developing ovarian granulosa cell tumour at a fertile age. Hum Reprod. 2000;15:589–93.
Miller BE, Barron BA, Wan JY. Prognostic factors in adult granulosa cell tumor of the ovary. Cancer. 1997;79:1951–5.
Lappöhn RE, Burger HG, Bouma J, Bangah M, Krans M, de Bruijn HW. Inhibin as a marker for granulosa-cell tumors. N Engl J Med. 1989;12:790–3.
Salani R, Goodrich K, Song C, Grumbine FC. Three case reports of laparoscopic management of granulosa cell tumor with intraoperative rupture and subsequent upstaging. J Minim Invasive Gynecol. 2008;15:511–3.
Nakayama J, Saks E, Pelkofski E, Edwards J, Stine JE, Secord AA, Gehrig PA, Duska L. Laparoscopy compared to laparotomy in the management of granulosa cell tumors of the ovary. Gynecol Oncol. 2015;137:168.
Dehannathparambil VJ, Antony MA, Nair IR, Pavithran K. Recent advances in granulosa cell tumor ovary: a review. Indian J Surg Oncol. 2013;4:37–47.
Dridi M, Chraiet N, Batti R, Ayadi M, Mokrani A, Meddeb K, Yahiaoui Y, Raies H, Mezlini A. Granulosa cell tumor of the ovary: a retrospective study of 31 cases and a review of the literature. Int J Surg Oncol. 2018. https://doi.org/10.1155/2018/4547892.
Lee IH, Choi CH, Hong DG, Song JY, Kim YJ, Kim KT, Lee KW, Park IS, Bae DS, Kim TJ. Clinicopathologic characteristics of granulosa cell tumors of the ovary: a multicenter retrospective study. J Gynecol Oncol. 2011;22:188–95.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Association of Gynecologic Oncologists of India 2019
Rights and permissions
About this article

Cite this article
Kayastha, S., Chitrathara, K., Sigdel, B. et al. Adult Granulosa Cell Tumor of Ovary: Clinical Study of 10 Cases. Indian J Gynecol Oncolog 18, 2 (2020). https://doi.org/10.1007/s40944-019-0343-9
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40944-019-0343-9