
Abstract
Introduction
Despite the fact that black women have a lower incidence of breast cancer compared to white women, black women experience higher death rates than any other group. We examined the stage of breast cancer presentation by race and geographic region using population-based breast cancer incidence in all 115 counties in the state of Missouri.
Methods
We used 2003–2008 breast cancer incidence data from Missouri Cancer Registry and Research Center. County of residence was categorized as urban or rural using the rural–urban continuum code. We computed the conditional proportion of stage at diagnosis by race and metropolitan status and also used Pearson’s chi-squared test with Yates’ continuity correction to determine statistical significance of association.
Results
Results of the study indicate that a greater proportion of black women (38.8 %) compared to white women (30.2 %) were diagnosed with more advanced breast metastasis. Our results further suggest that stage at diagnosis depended on county of residence or metropolitan status (p = .04). Women living in non-metropolitan counties were slightly more likely to have late-stage breast cancer than their metropolitan counterparts (32.0 vs 30.7 %). Overall, black women had 1.5-fold increased odds of late-stage breast cancer diagnosis compared to their white counterparts (OR = 1.50; 95 % CI, 1.39, 1.63; p < 0.0001). While the odds of late diagnosis among women living in non-metropolitan or rural counties was over 11 % higher compared with their metropolitan or urban counterpart.
Conclusion
The current study corroborates previous findings that the risk of late-stage breast cancer diagnosis was higher among women residing in non-metropolitan rural counties.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Breast cancer has remained the leading cause of death in women across racial and ethnic divide in the USA [1]. It accounted for over 232,340 new cases and more than 40,000 deaths in the USA in 2013 [1]. Although black (African-American) women have a lower incidence of breast cancer compared to white women, black women experience higher death rates than any other group [2]. For instance, between 2006 and 2010, the age-adjusted breast cancer incidence rate for non-Hispanic white (white, Caucasian) women was 127.4 (per 100,000 women per year) compared to 121.4 for non-Hispanic black (black, African-American) women in the USA [3]. This resulted in a black/white rate ratio (RR) of 0.95. In the same period, the mortality rates were 22.1 (age-adjusted, per 100,000 women per year) for white women and 30.8 for black women (RR = 1.39) [3]. Similarly, the 2014 racial disparity in breast cancer mortality study by Sinai Urban Health Institute and the Avon Foundation for women confirmed an increasing breast cancer disparity gap between black and white from 1990 to 2009 [4]. The study further indicated that, on average, over 1710 black women die yearly as a result of racial disparities in breast cancer screening and treatment [4].
Other previous studies have also extensively demonstrated that breast cancer disparities in screening, mortality, and survival vary greatly by race, socioeconomic statues, and geographical place of residence, especially distance travel to health-care services in rural areas [5–52]. To assess the impact of geographical factors on racial disparity in breast cancer stage at diagnosis, Keller et al. [7] analyzed breast cancer data from the American College of Surgeons [N = 1,388,186] from 2000 to 2007 using four broad census regions: Northeast, South, Midwest, and West. Results showed a statistically significant variation in stage at presentation between whites and non-whites (black) in the USA. In terms of stage as a function of race, 16.2 % black patients were diagnosed with late-stage breast cancer compared with whites (11.2 %). Additionally, a large geographic variation was also observed in relation to the number of patients diagnosed in stage with regard to race and geographic region. In all four regions across the USA, a significantly higher percentage of non-white (16.2 %) reported with late-stage (stages III and IV) disease compared with whites (11.2 %). These differences were all statistically significant (p < 0.0001). In terms of geographical differences, the South had the highest percentage of late-stage non-white breast cancer diagnosis when compared with whites (17.3 vs 11.2 %) followed by Midwest (16.0 vs 11.7 %) [7].
The US Census Bureau and other federal agencies use different definitions of rural. Each definition emphasizes different criteria such as population size and density, commuting patterns, poverty or unemployment rates, or extent of wild areas and farmland. In the state of Missouri, there are 114 counties and an independent city of St. Louis (115 total). According to the Metropolitan and Statistical Area (MSA) definition, which is usually referenced by the Missouri Department of Health and Senior Services, 101 counties are considered rural [53]. While disparities in rural–urban differences in cancer stage at diagnosis have been examined in states like Illinois, Georgia, and North Carolina [9, 12, 18, 29, 33, 39, 40, 42], findings have been mixed. In 1991, Liff et al. [9] [N = 35,610] reported that the relative excess of non-localized malignancies in rural Georgia was almost twice for blacks (37 %) than for whites (21 %). This finding suggested that for black and other minority populations, the rural–urban disparities were markedly different. However, a recent follow-up study by Markossian et al. [18] [N = 23,500] did not find a significant association between geographic location and late-stage breast cancer diagnosis. Missouri has 14 urban counties, and up until now, no previous studies have explored the geographical influence on racial disparity of breast cancer stage at presentation. This study was conducted to examine the stage of breast cancer presentation by race and geographic region using population-based breast cancer incidence in all 115 counties in Missouri.
Methods
Breast Cancer Incidence Data and Study Population
Breast cancer incidence data for 2003–2008 (N = 29,410) were obtained from the Missouri Cancer Registry and Research Center (MRC-ARC). The registry is tasked to collect demographic, tumor, and treatment information on all newly diagnosed cancers among Missouri residents annually. The study data were limited to women aged 18 years or older who were Missouri residents and diagnosed with breast cancer.
Individual-level data obtained from MCR-ARC included stage at diagnosis, race, and county of residence. Stage data were reported as: stage 0, stage I, stage II, stage III, stage IV, and unknown. To simplify the analysis, stage was dichotomized into early stage (stages 0, I, and II) and late stage consisted of (stages III and IV). Patients with unknown stage were excluded from the analysis. The race data on study participants was classified into white and black. County of residence was categorized as metropolitan (urban or metro) or non-metropolitan (rural or non-metro) using the rural–urban continuum code (RUCC) classifications status [54]. Within this classification system, urban counties have RUCC codes ≤3, and rural counties have RUCA codes ≥6 [54]. This study was considered exempt by the University of Missouri Institutional Review Board.
Statistical Analysis
We applied a two-way contingency table to classify and count subjects by stage at diagnosis and each of the two explanatory variables (race and metropolitan status). We computed the conditional proportion (percentage) of stage at diagnosis by race and metropolitan status. The logit model was used to estimate the relationship between stage at diagnosis and the two explanatory variables (race and metropolitan status). The logit model was appropriate because our response outcome “stage at diagnosis” can take one of two possible values representing “early” or “late” stage at diagnosis. To determine statistical significance of association, we used Pearson’s chi-squared test with Yates’ continuity correction, odds ratio estimated from the logit model, and the corresponding (1 − α)% confidence interval. RStudio version 0.98.501-© 2009–2013 (RStudio, Inc.) statistical package was used for data analysis.
Results
During 2003–2008, the Missouri cancer registry recorded 29,410 cases of women diagnosed with breast cancer. Of these, 19,690 (67 %) were early, 8846 (30 %) were late, and 874 (3 %) were unknown stage. After excluding unknown cases due to missing data, analysis was performed on 28,536 cases.
The proportion of women diagnosed with late stage of breast cancer was significantly higher among black women. Table 1 shows the distribution of late stage at diagnosis by race. It is clear from the table that a greater proportion of black women (38.8 %) than white women (30.2 %) was diagnosed with more advanced breast metastasis. Our results also indicated that stage at diagnosis was also depended on county of residence or metropolitan status. Women living in non-metropolitan counties were slightly more likely to have late-stage breast cancer than their metropolitan counterparts (32.0 vs 30.7 %).
Odds of Late-Stage Diagnosis
The effect of the explanatory variables on the response variable is commonly measured by using the odds ratio of the predictor variable, which represents the factor by which the odds of an outcome change for one unit change in the predictor variable. Table 2 displays the estimated odds ratios and corresponding 95 % confidence intervals of the estimated odds ratio from the logit model. For race, the effect of 0.408 on the logit scale translates into an estimated odds ratio of 1.504. Thus, the odds of late diagnosis among black women were 1.504 or over 50 % higher than those of white women. Since the estimated odds ratio and the 95 % confidence intervals (CI) are greater than one, the relationship between race and stage at diagnosis was not only statistically significant at the 0.05 level, but also positively associated.
Similarly, for metropolitan status, the effect of 0.106 on the logit scale translates into an estimated odds ratio of 1.112. Also, the odds of late diagnosis among women living in non-metropolitan areas were 1.112 or slightly over 11 % higher than women living in the metropolitan areas. In a likewise manner, the estimated odds ratio and the 95 % confidence intervals were higher than one signaling that the relationship between metropolitan status and stage at diagnosis was highly statistically significant at the 0.05 level and positively associated.
Discussion
The stage at cancer diagnosis has a tremendous impact on type of treatment, recovery, and survivor. In most cases, the earlier the cancer is detected and treated, the higher the survival rate for the patient. Studies for several cancer sites have shown that individuals living in poor areas are more likely not to utilize cancer screening services and present at a late stage compared with individuals living in affluent areas [19, 38, 41–44]. Other studies have also found that place of residence and neighborhood socioeconomic characteristics are associated with cancer outcomes and quality of life [13, between place of residence, race, and stage14, 16, 20, 27, 29, 41, 42]. Although some of these study results have been inconclusive, the novelty of this research was to analyze the patterns of breast cancer stage at diagnosis in Missouri with regard to geographic region and race since over 85 % of the counties are considered rural and the proportion of African-American population is less than 12 %.
Differences in Diagnosis by Race
The racial and ethnic composition of Missouri population is 81.0 % Caucasian/White/non-Hispanic, 11.6 % African-American/non-Hispanic, 3.5 % Hispanic/Latino, 1.6 % Asian/non-Hispanic, 0.5 % American Indian/Alaskan Native, 0.1% Native Hawaiian and other Pacific Islander, and 2.1 % two or more races. Thirty-seven percent of Missouri’s population is rural, equating to approximately 2.22 million people in rural areas. However, African-Americans primarily live in urban areas. Based on the US Census Bureau’s 2010 report, only 3.0 % of the rural population is African-American [53]. Despite the small proportion of African-Americans in the state, data from our analysis study revealed that black women in Missouri had a significantly increased odd of being diagnosed with late-stage breast cancer (Table 2).
The American Cancer Society reported that from 2006 to 2010, incidence and death rates for breast cancer were lower among women of other racial and ethnic groups than non-Hispanic white and African-American women [1]. Generally, African-American women in the USA are less likely to be diagnosed with smaller tumors (less than 2.0 cm) and more likely to be diagnosed with larger tumors (greater than 5.0 cm) than white women [1]. A study by Izano et al. [52] [N = 999] analyzed the Metropolitan Detroit Cancer Surveillance System data to investigate the impact of Charlson Comorbidity Score (CSS) following breast cancer diagnosis on the risk of mortality from breast cancer among African-American and white women. Results showed a very significant difference exist between African-American and white when stage at diagnosis was compared between the two groups. African-American women were less likely than their white counterparts to have localized disease—invasive malignancies that are confined to the organ of origin (breast) (43.8 vs. 55.6 % respectively, p = 0.006) and more likely to have regional disease—the cancer spread by direct extension to adjacent organs or tissues, and/or spread to lymph nodes considered regional to the organ of origin, but no further spread has occurred (48.1 vs. 39.2 % respectively, p = 0.03) at the time of diagnosis [52]. Moreover, more African-American women were reported to have died of breast cancer than white women (37.1 vs. 31.4 %, p = 0.15). Using the American College of Surgeons National Cancer Data Base, Sariego [10] examined breast cancer distribution pattern in the USA. Results revealed a large variation exists in breast cancer diagnosis with regard to stage, race, and place of resident. For example, a higher percentage of whites (90.1 %) was reported with early stage disease (stages I and II) as compared with non-whites (85.3 %). These differences were statistically significant (p = 0.001).
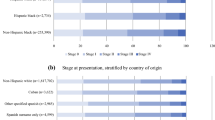
A descriptive analysis by Menck and Mills [35] based on data from California Cancer Registry (1994–1997) comparing the influence of geographical location, age, ethnicity, and income on early-stage breast cancer indicated that few African-American (39.1 %) and Hispanic (41.4 %) women were diagnosed with localized stage disease. These findings were statistically significant (p = .0001). Similarly, in the UK, Cuthbertson et al. [26] examined the racial inequalities in breast cancer diagnosis between ethnic minorities and British white women. Findings showed that ethnic minority groups have a significantly increased risk of diagnosis with late-stage breast cancer relative to the white British group. For the black/black British and Chinese/Other ethnic groups, risk of diagnosis with late-stage breast cancer is more than 25 % higher [RR = 1.28 (95 % CI, 1.11, 1.49) and RR = 1.26 (95 % CI, 1.04, 1.53)]. Consistent with previous findings, the current study has demonstrated increasing disparities gap in the stage at breast cancer diagnosis for white and black (see Tables 1 and 2) despite that less than 4.0 % of Missouri’s population is African-American.
Differences in Diagnosis by Place of Resident
Research has demonstrated a strong relationship between socioeconomic status (SES) and an increased risk of being affected by health disparities [45, 46]. It has been noted that the leading causes of death and disability have a disproportionate impact on African-Americans, Alaska Natives, American Indians, Asian Americans, Hispanic Americans, and Pacific Islanders [46, 47]. Whether assessed by income, level of education, or occupation, SES clearly predicts the health status of an individual. Individuals of lower SES are more likely to live in poorer communities, which experience a higher degree of residential crowding, violence, and environmental pollution. Poorer housing quality further increases the risk of health conditions for individuals of lower SES. In addition, social environments have a significant impact on SES-related health outcomes in regard to risk and prevalence of chronic and infectious diseases. As mentioned earlier, SES determines the ability to purchase health coverage, which has a direct effect on access to health care. Research has demonstrated that uninsured individuals are less likely to receive preventive and primary health-care services than insured individuals [45, 47]. The most significant indirect pathway that influences SES is the impact of behavior and lifestyle. Lower SES is also associated with a sedentary lifestyle as well as poorer nutrition, both of which have an effect on the health status of an individual.
Economic and social factors such as poverty have been directly linked with low usage of mammography screenings [5, 21, 41, 48, 49]. Regardless of race or ethnicity, Campbell et al. [48] noted that poverty has a strong effect on the probability of being diagnosed at the later stages of cancer. As poverty increases by 10 percentage points, the odds of being diagnosed at a regional or distant stage increase by a factor of approximately 1.07, an effect that does not differ by race or ethnicity. Analyzing the geographic differences in late-stage breast cancer in Illinois and the role of socioeconomic and spatial factors, Wang et al. [41] found that people living in areas of high socioeconomic disadvantage were more likely to be diagnosed with late-stage breast cancer. The risk of late diagnosis was also higher for women living in areas with poor geographical access to primary care physicians, indicating a combination of spatial and socioeconomic barriers. MacKinnon et al. [50] found that minorities and socioeconomically disadvantaged people have lower incidence rates of breast cancer but higher mortality rates because they are unable to seek or obtain screening services. Even if disadvantaged people live near a screening center, they sometimes do not seek help because of economic, cultural, and social barriers.
Further, an ecologic study of female breast cancer incidence in North Carolina by Hall et al. [12] reported that in situ breast cancer rates were highest in urban counties when comparing urban with rural counties. Invasive breast cancer rates were also shown to be higher in the most urban counties for whites (IRR = 1.18 comparing most urban with most rural) but not non-whites (IRR = 0.99 for the same comparison). A Danish study by Dalton et al. [13] found that women living in rural areas of Denmark had a 10 % higher odds (OR) of high-risk breast cancer (95 % CI, 1.02, 1.18) while those living in the capital suburban areas had a 15 % lower OR (95 % CI: 078, 0.93) than those living in provincial cities.
A study on the spatial distribution of Chicago’s low or no-cost mammography screening facilities showed overall shorter travel time for low-income residents. However, longer travel time and distances were shown for low-income black neighborhoods than for other low-income neighborhoods [51]. Using the Michigan Cancer Surveillance Program data set from 1998 to 2002 to assess black residential segregation and spatial access to health care on late-stage breast cancer diagnosis in metropolitan Detroit, Dai [49] concluded that segregation, lack of access to mammography screening facility, and low SES increase the risk of advanced diagnosis for black women. McLafferty and Wang [38] reported a J-shaped curve for late-stage breast cancer risk was described for women in Illinois with the most highly urbanized area (Chicago) and most isolated rural areas having the highest risk. All these studies have illustrated the significant role spatial factors have and continued to play in the diagnosis and treatment of cancer and other diseases over the years. In the current study, we did not examine the role of segregation on breast cancer stage at diagnosis. However, consistent with earlier studies, the current study shows a significant association between geographic residency (metropolitan vs non-metropolitan Tables 1 and 2) status and late-stage breast cancer diagnosis.
In contrast, Celaya et al. [15], Henry et al. [16], Klein et al. [17], Markossian et al. [18], Henry et al. [19], Warner et al. [20], Huang et al. [21], and Amey et al. [22] found that geographic place of residence measures was weakly associated with differences in the risk of late-stage breast cancer. For instance, using Florida’s cancer data system and area resource file, Amey et al. [22] reported that rural counties that are adjacent to a metropolitan county have the highest percentage (64.5 %) of women whose breast cancer was detected at an early stage compared to their urban counterparts. Klein and colleagues [17] [N = 4222] analyzed differences in male breast cancer stage, tumor size, and stage at diagnosis using metropolitan and non-metropolitan classification using the Surveillance, Epidemiology, and End Results Program of the National Cancer Institute from 1988 to 2006 and found no statistical differences in proportions of stage or tumor size at diagnosis between the two regions. Nonetheless, the authors stated that the presence of an interaction between non-metropolitan county and regional stage male breast cancer was a significant predictor of poorer survival and quality of life [17]. In spite of these findings, the strength of our study is that it corroborates previous findings that the risk of late-stage breast cancer presentations was highest among women residing in non-metropolitan rural counties in the USA. In addition, African-American women had a greater percentage of patients presenting with more advanced stage breast cancer, suggesting a link between place of residence, race, and stage at diagnosis.
Conclusion
Differences in access to health-care services and the resulting adverse health outcomes are major public health priorities. While breast cancer remains the most common cancer in women, the burden of cancer does not fall equally across all groups and racial and/or ethnic disparities in diagnosis, survivorship, and mortality particularly among African-Americans and rural dwellers.
The findings from this study have provided useful information on provision of health-care access and accessibility regarding what health services is needed and where and to whom coverage is lacking. These results can serve as a guide to policymakers and provide the basis for developing strategies aimed at improving access to breast cancer screening and treatment services for low-income, uninsured, and underserved women in Missouri.
In sum, cancer costs billions of dollars in years of productive life lost. Above and beyond the financial costs, there are huge emotional costs related to losing loved ones prematurely. Reducing the burden of health disparities for minority populations and disadvantaged groups is essential to achieving quality health care for all.
References
American Cancer Society. Cancer facts and figures. 2013–2014: 2013. http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-042725.pdf. Accessed 10 Jan 2014.
Centers for Disease Control and Prevention (CDC). Breast cancer rates by race and Ethnicity; 2014. http://www.cdc.gov/cancer/breast/statistics/race.htm. Accessed 3 Dec 2014.
Hunt BR, Whitman S, Hurlbert MS. Increasing black: white disparities in breast cancer mortality in the 50 largest cities in the United States. Cancer Epidemiol. 2013. doi:10.1016/j.canep.2013.09.009.
Avon Foundation for Women. 2014 racial disparity in breast cancer mortality study; 2014. http://www.avonfoundation.org/causes/breast-cancer-crusade/disparities-study/ Accessed 11 Mar 2015.
Leung J, McKenzie S, Martin J, McLaughlin D. Effect of rurality on screening for breast cancer: a systematic review and meta-analysis comparing mammography. Rural Remote Health. 2014;14(2):2730.
Nguyen-Pham S, Leung J, McLaughlin D. Disparities in breast cancer stage at diagnosis in urban and rural adult women: a systematic review and meta-analysis. Ann Epidemiol. 2014;24:228–35.
Keller D, Guilfoyle C, Sariego J. Geographical influence of racial disparity in breast cancer presentation in the United States. Am Surg. 2011;77:933–6.
Chien LC, Yu HL, Schootman M. Efficient mapping and geographic disparities in breast cancer mortality at the county-level by race and age in the U.S. Spat Spatiotemporal Epidemiol. 2013;5:27–37.
Liff JM, Chow W-H, Greenberg RS. Rural urban differences in stage at diagnosis. Possible relationship to cancer screening. Cancer. 1991;67(5):1454e9.
Sariego J. Patterns of breast cancer presentation in the United States: does geography matter? Am J Surg. 2009;75(7):545–50.
Gregorio DI, Kulldorff M, Barry L, Samociuk H. Geographic differences in invasive and in situ breast cancer incidence according to precise geographic coordinates, Connecticut, 1991–95. Int J Cancer. 2002;100:194–8.
Hall SA, Kaufman JS, Millikan RC, Ricketts TC, Herman D, Savitz DA. Urbanization and breast cancer incidence in North Carolina, 1995–1999. Ann Epidemiol. 2005;15(10):796e803.
Dalton SO, During M, Ross L, Carlsen K, Mortensen PB, Lynch J, et al. The relation between socioeconomic and demographic factors and tumour stage in women diagnosed with breast cancer in Denmark, 1983–1999. Br J Cancer. 2006;95(5):653e9.
Blair SL, Sadler GR, Bristol R, Summers C, Tahir Z, Saltzstein SL. Early cancer detection among rural and urban Californians. BMC Public Health 2006;6.
Celaya MO, Berke EM, Onega TL, Gui J, Riddle BL, Cherala SS, et al. Breast cancer stage at diagnosis and geographic access to mammography screening (New Hampshire, 1998–2004). Rural Remote Health. 2010;10:1361.
Henry KA, Boscoe FP, Johnson CJ, Goldberg DW, Sherman R, Cockburn M. Breast cancer stage at diagnosis: is travel time important? J Community Health. 2011;36(6):933–42.
Klein J, Ji M, Rea NK, Stoodt G. Differences in male breast cancer stage, tumor size at diagnosis, and survival rate between metropolitan and nonmetropolitan regions. Am J Mens Health. 2011;5:430–7.
Markossian TW, Hines RB. Disparities in late stage diagnosis, treatment, and breast cancer-related death by race, age, and rural residence among women in Georgia. Women Health. 2012;52(4):317e35.
Henry KA, Sherman R, Roche LA. Colorectal cancer stage at diagnosis and socioeconomic characteristics in New Jersey. Health Place. 2009;15:505–13.
Warner ET, Gomez SL. Impact of neighborhood racial composition and metropolitan residential segregation on disparities in breast cancer stage at diagnosis and survival between black and white women in California. J Community Health. 2010;35(4):398–408.
Huang B, Dignan D, Han D, Johnson O. Does distance matter? Distance to mammography facilities ad stage at diagnosis of breast cancer in Kentucky. J Rural Health 2009;366–371.
Amey CH, Miller MK, Albrecht SL. The role of race and residence in determining stage at diagnosis of breast cancer. J Rural Health Off J Am Rural Health Assoc Natl Rural Health Care Assoc. 1997;13(2):99e108.
Armstrong W, Borman B. Breast cancer in New Zealand: trends, patterns, and data quality. N Z Med J. 1996;109:221–3.
Bennett H, Marshall R, Campbell I, Lawrenson R. Women with breast cancer in Aotearoa New Zealand: the effect of urban versus rural residence on stage at diagnosis and survival. N Z Med J 2007;120(1266).
Mitchell KJ, Fritschi L, Reid A, McEvoy SP, Ingram DM, Jamrozik K, et al. Rural urban differences in the presentation, management and survival of breast cancer in Western Australia. Breast. 2006;15(6):769–e76.
Cuthbertson SA, Goyder EC, Poole J. Inequalities in breast cancer stage at diagnosis in the Trent region, and implications for the NHS breast screening programme. J Public Health (Oxf). 2009;31(3):398–405.
Baade P, Turrell G, Aitken J. Geographic remoteness, area-level socio-economic disadvantage and advanced breast cancer a cross-sectional, multilevel study. J Epidemiol Community Health. 2011;65(11):1037e43.
Barry J, Breen N. The importance of place of residence in predicting late-stage diagnosis of breast or cervical cancer. Health Place. 2005;11:15–29.
Cho YI, Johnson TP, Barrett RE, Campbell RT, Dolecek TA, Warnecke RB. Neighborhood changes in concentrated immigration and late stage breast cancer diagnosis. J Immigr Minor Health. 2011;13:9–14.
Elliott TE, Elliott BA, Renier CM, Haller IV. Rural-urban differences in cancer care: results from the Lake Superior Rural Cancer Care Project. Minn Med. 2004;87(9):44e50.
Ess S, Savidan A, Frick H, Rageth C, Vlastos G, Lutolf U, et al. Geographic variation in breast cancer care in Switzerland. Cancer Epidemiol. 2010;34:116–21.
Higginbotham JC, Moulder J, Currier M. Rural v. urban aspects of cancer: first year data from the Mississippi Central Cancer Registry. Fam Community Health. 2001;24(2):1e9.
Howe H, Katterhagen G, Yates J, Lehnherr M. Urban-rural differences in the management of breast cancer. Cancer Causes Control. 1992;3(6):533e9.
Innos K, Magi M, Tekkel M, Aareleid T. Place of residence predicts breast cancer stage at diagnosis in Estonia. Eur J Pub Health. 2011;21(3):376–80.
Menck HR, Mills PK. The influence of urbanization, age, ethnicity, and income on the early diagnosis of breast carcinoma. Cancer. 2001;92(5):1299–304.
Montella M, Biondi E, De Marco M, Botti G, Tatangelo F, Capasso I, et al. Sociodemographic factors associated with the diagnostic staging of breast cancer in southern Italy. Cancer. 1995;76(9):1585–e90.
Olson RA, Nichol A, Caron NR, Olivotto IA, Speers C, Chia S, et al. Effect of community population size on breast cancer screening, stage distribution, treatment use and outcomes. Can J Public Health. 2012;103(1):46–52.
McLafferty S, Wang F. Rural reversal? Cancer. 2009;115:2755–64.
McLafferty S, Wang F, Luo L, Butler J. Rural-urban inequalities in late-stage breast cancer: spatial and social dimensions of risk and access. Environ Plann B Plann Des. 2011;38(4):726–40.
Campbell NC, Elliot AM, Sharp L, Ritchie LD, Cassidy J, Little J. Rural factors and survival from cancer: analysis of Scottish cancer registrations. Br J Cancer. 2000;82(11):1863–6.
Wang F, McLafferty S, Escamilla V, Luo L. Late-stage breast cancer diagnosis and health care access in Illinois. Prof Geogr. 2008;60(1):54–69.
Singh GK. Rural-Urban trends and patterns in cervical cancer mortality, incidence, stage, and survival in the United States, 1950–2008. J Commun Health 2011;1–7.
Campbell B, Staley D, Matas M. Who misses appointments? An empirical analysis. Can J Psychiatr. 1991;36:223–5.
Onitilo AA, Liang H, Stankowski RV, Engel JM, Broton M, Doi SA, et al. Geographical and seasonal barriers to mammography services and breast cancer stage at diagnosis. Rural Remote Health. 2014;14:2738.
Adler NE, Newman K. Socioeconomic disparities in health: pathways and policies. Health Aff. 2002;21(2):6076.
Williams DR, Sternthal M. Understanding racial-ethnic disparities in health: sociological contributions. J Health Soc Behav. 2010;51(1):S15–27.
Liburd LC, Giles HW, Mensah GA. Looking through a glass, darkly: eliminating health disparities. Prev Chronic Dis. 2006;3(3):13.
Campbell RT, Li X, Dolecek TA, Barrett RE, Weaver KE, Warnecke RB. Economic, racial and ethnic disparities in breast cancer in the US: towards a more comprehensive model. Health Place. 2009;15(3):855–64.
Dai D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place. 2010;16(5):1038–52.
Mackinnon J, Duncan R, Huang Y, Lee D, Fleming L, Voti L, et al. Detecting an association between socioeconomic status and late stage breast cancer using spatial analysis and area-based measures. Cancer Epidemiol Biomarkers Prev. 2007;16(4):756–62.
Zenk SN, Tarlov E, Sun J. Spatial equity in facilities providing low- or no-fee screening mammography in Chicago neighborhoods. J Urban Health. 2006;83:95–210.
Izano M, Satatiano WA, Tammemagi MC, Ragland D, Moore DH, Allen E, et al. Long-term outcomes among African-American and white women with breast cancer: what is the impact of comorbidity? J Geriatr Oncol. 2014;5:266–75.
Missouri Department of Health and Senior Services Office of Primary Care and Rural Health. 2010–2013 rural health plan. http://health.mo.gov/living/families/ruralhealth/pdf/ruralhealthplan.pdf. Accessed 2 Apr 2015.
U.S. Department of Agriculture and Economic Research Services. The 2013 Rural-Urban Continuum Code. http://www.ers.usda.gov/topics/rural-economy-population/rural-classifications.aspx. Accessed 20 Dec 2014.
Conflict of Interest
Faustine Williams and Emmanuel Thompson declare that they have no competing interests.
Informed Consent
No animal or human studies were carried out by the authors for this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Williams, F., Thompson, E. Disparity in Breast Cancer Late Stage at Diagnosis in Missouri: Does Rural Versus Urban Residence Matter?. J. Racial and Ethnic Health Disparities 3, 233–239 (2016). https://doi.org/10.1007/s40615-015-0132-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-015-0132-9