
Abstract
Recent research suggests living in an economically disadvantaged neighborhood is associated with decreased likelihood of undergoing mammography and increased risk of late-stage breast cancer diagnosis. Long distances and travel times to facilities offering low- or no-fee mammography may be important barriers to adherence to mammography screening recommendations for women living in economically disadvantaged urban neighborhoods, in which African–Americans are disproportionately represented. The purpose of this study was to examine whether the spatial distribution of facilities providing low- or no-fee screening mammography in Chicago, Illinois, is equitable on the basis of neighborhood socioeconomic and racial characteristics. We found that distance and travel times via automobile and public transportation to facilities generally decrease as neighborhood poverty increases. However, we also found that the strength of the association between neighborhood poverty level and two of the spatial accessibility measures—distance and public transportation travel time—is less strong in African–American neighborhoods. Among neighborhoods with the greatest need for facilities (i.e., neighborhoods with the highest proportions of residents in poverty), African–American neighborhoods have longer travel distances and public transportation travel times than neighborhoods with proportionately fewer African–American residents. Thus, it appears that the spatial accessibility of low- and no-fee mammography services is inequitable in Chicago. In view of persistent social disparities in health such as breast cancer outcomes, these findings suggest it is important for researchers to examine the spatial distribution of health resources by both the socioeconomic and racial characteristics of urban neighborhoods.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Despite recent improvements in U.S. breast cancer survival rates, disparities on the basis of social and economic factors persist. Poor women and those who are uninsured have poorer breast cancer survival than their more advantaged counterparts.1 – 5 Compared to non-Hispanic (NH) White women, most U.S. ethnic minority populations have lower breast cancer survival, much of which is attributable to socioeconomic factors.5 – 11 One of the reasons for these disparities in breast cancer outcomes is the well-documented tendency toward later stage at diagnosis among women of lower socioeconomic status (SES) and women of color.5 , 8 , 9 , 12 – 14
Differences in mammography utilization are widely believed to contribute to observed socioeconomic and racial/ethnic variation in prevalence of late-stage diagnosis. Despite recommendations for routine annual or biannual mammography for all women age 40 years and older, significant gaps exist in uptake across population subgroups.15 – 17 Women with lower income and educational attainment and those with no health insurance are less likely to undergo breast cancer screening.18 – 20 Historically, the prevalence of screening mammography among women of color in the U.S. has lagged behind that of their NH White counterparts.20 Although results of recent surveys suggest the gap in screening rates between African–American and NH White women may have closed, racial/ ethnic differences in utilization of screening mammography are likely to have played a significant role in previously observed disparities in late-stage breast cancer diagnosis and survival.18 , 21 – 23
In this study, we explore one potential contributor to disparities in breast cancer screening, stage at diagnosis, and survival: inequity in the spatial distribution of mammography facilities. There is growing evidence that living in a neighborhood with few economic resources is associated with decreased likelihood of participating in mammography screening and increased risk of late-stage breast cancer diagnosis. A national study found that, independent of individual-level characteristics, living in a socioeconomically disadvantaged neighborhood was associated with a decreased likelihood of adherence with breast cancer screening recommendations.24 In another analysis, again controlling for individual social and economic characteristics, the odds of never having a mammogram among women residing in areas (roughly corresponding to census block groups) in which the median education was less than 12 years, compared to areas in which the median education was more than 15 years, were increased by 69%.25 A recent study using Surveillance, Epidemiology, and End Results (SEER) program data from three U.S. metropolitan areas found that among women diagnosed with breast cancer, those who resided in high-poverty census tracts (i.e., census tracts with 40% or more of residents with incomes below poverty) were 39% more likely than those residing in lower-poverty census tracts (i.e., neighborhoods with less than 20% of residents with incomes below poverty) to have late-stage disease.26 In a study of women diagnosed with breast cancer in New York City, the odds of an advanced-stage diagnosis were increased by 50% for African American women and by 75% for White women who lived in areas with lower levels of education and income compared to women living in other areas.27
Information regarding the mechanisms by which neighborhood SES influences breast cancer screening rates or late-stage diagnosis, as with other health behaviors and health outcomes, is lacking. The role of neighborhood social context in influencing stage at breast cancer diagnosis is currently being evaluated in one study (R.B. Warnecke, Ph.D., University of Illinois at Chicago, oral communication, Nov. 2005). Previously proposed explanations for neighborhood effects on breast cancer screening rates and late-stage diagnosis address access issues, principally focusing on supply of health care services.24 – 26 , 28 Geographic location of mammography facilities—creating neighborhood differences in distance or travel time to mammography services—may be an additional explanation for lower utilization of mammography and heightened risk of late-stage diagnosis among residents of economically disadvantaged neighborhoods. Two studies, including one in a major metropolitan area, have found that people who lived farther away from facilities were less likely to undergo mammography than those who lived closer to facilities.29 , 30 Another found no association between distance or travel time and compliance with screening mammography recommendations in rural Michigan.31 Most studies of the association between distance and health care utilization have examined this relationship among residents of rural areas or large regions such as states that include areas of varying rurality.32 – 36 Intraurban variation in the spatial accessibility of mammography and other health care services and its effect on residents' utilization is not well understood.37
Facilities providing low- or no-fee screening mammography may be particularly important resources for midlife women (ages 40–64) residing in economically disadvantaged neighborhoods. Among women aged 45 to 64 years in Illinois with a family income below the federal poverty line, 38% are uninsured.38 Despite financial need and low rates of health insurance, most of these women are categorically ineligible for Medicaid and Medicare, which cover screening mammography. Further, among women with few financial resources, health insurance may not eliminate financial barriers to screening mammography participation arising from deductibles, co-pays, and other costs.39 , 40 To address this need for affordable mammography services, state and federally funded programs offer screening mammography to financially needy women on a sliding-fee scale.41 In Chicago, this service is accessed predominantly through the city or county health department clinics or through one of the Federally Qualified Health Centers participating in the program. The associated mammography facilities are located in some city health department sites, at two county-owned hospitals, and in other area hospitals. These programs and facilities are intended to make routine mammography financially accessible to all Chicago residents for whom screening is recommended (i.e., women age 40 years and older). However, it is not known to what degree these facilities provide equitable spatial access to mammography.
Therefore, in this study, we examined whether the spatial distribution of facilities providing low- or no-fee screening mammography in Chicago, Illinois, is equitable based on neighborhood SES and neighborhood racial composition. This study adheres to the definition of equity as a just spatial distribution of resources in relation to need.42 , 43 Our first objective was to determine whether neighborhoods with higher proportions of residents with incomes below the poverty level, assumed to have the greatest need for the service, have better spatial access, defined as distance and travel time, to low- or no-fee mammography facilities. Because they are more likely to live in high-poverty neighborhoods than other racial/ethnic groups, African–Americans may be particularly vulnerable to the effects of socioeconomic inequity in the spatial distribution of resources.44 Further, African–American neighborhoods have historically been medically underserved. For example, a recent study of Washington, DC, found that almost all areas with substandard spatial accessibility of pediatric primary care providers were predominately African–American.45 Thus, it was also important to investigate whether the relationship between neighborhood poverty and the spatial accessibility of facilities offering low- or no-fee mammograms differs by the proportion of African–American residents in the neighborhood.
Materials and Methods
Setting and Sample
The setting for the study was Chicago, Illinois. Chicago and the surrounding suburbs is one of the most economically and racially segregated urban areas in the U.S.44 , 46 , 47 The sample for this study was neighborhoods in the city of Chicago, defined by the Project on Human Development in Chicago Neighborhoods (PHDCN) based on criteria such as demographic similarity, housing density, major ecological barriers (e.g., main thoroughfares), and local knowledge of neighborhood borders.48 Each of the 343 neighborhoods is composed of one or more census tracts. A more detailed description of these neighborhoods is provided elsewhere.48
Measures
Spatial Accessibility of Mammography Facilities
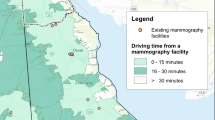
Our interest was in facilities providing low- (on a sliding fee scale) or no-fee screening mammography services through publicly funded programs to low-income and uninsured Chicago residents in 2004. The facilities were identified from information published by the Chicago Department of Public Health (CDPH) and through interviews with key informants associated with the Cook County Bureau of Health Services (CCBHS) and the Breast and Cervical Cancer Early Detection Program (BCCEDP). The facilities were (a) operated by the CDPH or CCBHS or (b) sites to which Chicago residents were referred through the BCCEDP. Facilities were address-matched to the U.S. Census Bureau 2003 TIGER/Line® File using geographic information system (GIS) software.49 , 50
Three measures evaluated the spatial accessibility of the mammography facilities to the neighborhoods: street network distance to the nearest facility, public transportation travel time to the nearest facility (based on straight-line distance), and shortest automobile travel time to a facility. These measures represent one approach to spatial accessibility measurement.37 , 51 , 52 The measures were calculated based on the neighborhood centroids, or geometric centers, and reflect the spatial accessibility of facilities for an individual living in the middle of the neighborhood. The spatial accessibility of facilities will vary for individuals within the neighborhoods. To control for differences in the geographic size (land area) of the neighborhoods and thus imprecision in the measurement of accessibility, the net land area (excluding water) was included as a covariate in regression analyses.
The distance over the street network between the 343 neighborhood centroids and each mammography facility was calculated using GIS.37 , 50 , 53 , 54 This procedure involved moving neighborhood centroids directly onto the closest street segment, that is, portion of a street generally about the length of a city block.54 , 55 The centroids were displaced, on average, 17.8 m with a range of 0.01 to 238.5 m. After the distances were calculated, we identified the minimum street network distance from each neighborhood centroid to a facility.
We estimated public transportation travel time from each neighborhood to the nearest facility using the following procedure. Using GIS, we first determined the facility nearest to each neighborhood based on straight-line distances between the neighborhood centroids and the facilities.53 , 54 Next, we assigned a street address to each neighborhood centroid. We selected the midpoint of the range of addresses for the street segment on which the neighborhood centroid was located. We then used the Trip Planner of the Chicago Transportation Authority to estimate the travel time to the nearest facility.56 To obtain the travel time, we used the following specifications for travel: Tuesday, March 29, 2005; arrival time 11:00 a.m.; maximum walking distance 0.5 mi; and preference for the quickest trip. The date and time were selected arbitrarily although we consider them appropriate since women going to a mammography appointment would generally have traveled during the week and during regular business hours. Because travel times likely vary to some extent by time of the day and to a lesser extent by day of the week and time of the year, these travel times are estimates.
The automobile travel time from the 343 neighborhood centroids to each of the 11 facilities was estimated using modeled 2005 travel time data from the Chicago Area Transportation Study (CATS).57 Automobile travel times used in this analysis are derived from the last step of the CATS four-step demand model: the network “time of day” assignment process. CATS provided automobile travel times that take into account traffic congestion between all traffic analysis zones in metropolitan Chicago for eight time periods over a 24-h day. The traffic analysis zones range in size from approximately 0.06 mi2 in the central business district to 1 mi2 in the rest of Chicago and the immediate vicinity.
To obtain the shortest automobile travel time from each neighborhood to a facility, we used the following procedure. First, using GIS, we identified the traffic analysis zone in which each neighborhood centroid and facility were located.49 Based on the traffic analysis zones, we obtained the modeled automobile travel time from every neighborhood to each facility for three times during the day that corresponded to regular business hours: 9:00–10:00 a.m., 10:00 a.m.–2:00 p.m., and 2:00–4:00 p.m. For those neighborhoods whose centroid was located in the same traffic analysis zone as the facility, we substituted the mean automobile travel time between contiguous traffic analysis zones based on a random sample of ten traffic analysis zones in Chicago. Next, we identified for each neighborhood the minimum automobile travel time to a facility for each of the three time periods. We then averaged the three travel times to obtain an estimate of the shortest automobile travel time to a facility.
Sociodemographics
Summary Tape File 3 (STF-3) of the 2000 decennial census provided measures of neighborhood sociodemographics.58 Data were obtained for census tracts and were then aggregated to the 343 neighborhoods. In this study, neighborhood poverty was defined as the percentage of individuals with incomes below the federal poverty line. Neighborhood racial/ethnic composition was defined as percentage of neighborhood residents in each of four racial/ethnic groups: NH African–American (i.e., African–American), Latino, NH White (i.e., White), and other. To account for differences in neighborhood population, we included population density, the total population per square mile of land in the neighborhood, as a covariate in regression models.
Data Analysis
We first examined means of the three spatial access variables in neighborhoods with different levels of poverty (<10, 10–20, >20% of residents below poverty). We then stratified that analysis further by the proportion of African–American residents (<20, 20–80, >80%). Next, we used ordinary least squares (OLS) regression to estimate relationships between neighborhood poverty and the three measures of the spatial accessibility of facilities providing low- and no-fee screening mammography (distance to the nearest facility, public transportation travel time to the nearest facility, shortest automobile travel time to a facility). The natural log of the accessibility measures was used because distance and travel time are censored variables that cannot have negative values. In Model 1, we estimated the relationship between percentage of neighborhood residents in poverty and the spatial accessibility of facilities, adjusting for percentage African–American residents in the neighborhood. To test whether the relationship between neighborhood poverty and spatial accessibility depends on proportion of African–American residents, Model 2 added a multiplicative interaction term between percentage of neighborhood residents in poverty and percentage African–American residents. With the exception of population density and land area, the variables were centered in these analyses.
We expected strong positive spatial autocorrelation due to the use of distance-based dependent variables. Positive spatial autocorrelation in this study indicates that the distance or travel time to facilities is more similar in neighborhoods closer together than in those farther apart and thus, that observations are not independent.59 Because this can lead to correlated residuals, it violates a key underlying assumption of OLS regression. Indeed, statistically significant Lagrange Multiplier tests for spatial lag and spatial error autocorrelation indicate that the OLS model residuals for Models 1 and 2 exhibit spatial autocorrelation.60 , 61 Robust Lagrange Multiplier tests suggest that a spatial lag regression model is more appropriate than a spatial error regression model. Thus, to attempt to account for spatial autocorrelation, we also estimated the models using spatial endogenous lag regression with a “rook” contiguity matrix.
Results
We identified eight facilities in Chicago and three in surrounding suburbs providing low- or no-fee screening mammography to Chicago residents in 2004. On average, the nearest facility is located 3.4 mi and 23.2 min by public transportation from the neighborhoods (Table 1). The shortest automobile travel time from the neighborhoods to a facility averages 13.8 min. The proportion of residents in poverty and in each of the four racial/ethnic groups in the neighborhoods varies considerably, reflecting the racial and economic segregation in Chicago.
Table 2 presents mean, median, and inter-quartile range of the spatial access variables by neighborhood poverty level. Mean distance and travel times decrease as neighborhood poverty increases such that the mean distance and travel times in the highest poverty category (>20%) are approximately half as long as those in the lowest poverty category (<10%). However, when neighborhoods were further stratified by proportion African–American residents, reductions in mean distance and travel times with increasing poverty are less dramatic in neighborhoods with the highest proportions of African–American residents than in those with lower proportions (Table 3). For example, among low African–American neighborhoods (<20%), the minimum street network distance mean is reduced by 62% in the highest compared to lowest poverty neighborhoods. In contrast, among high African–American neighborhoods (>80%), moving from the highest to the lowest poverty neighborhood reduces that distance by only 38%. Table 3 also shows that, among the highest poverty neighborhoods, the mean distance to the nearest facility is 0.5 mi longer and the mean public transportation travel time is 3.6 min longer in high African–American neighborhoods than in low African–American neighborhoods. Among the highest poverty neighborhoods, the mean automobile travel time does not differ by the proportion African–American residents in the neighborhood.
Table 4 shows results of the two regression models for minimum street network distance, estimated using OLS and spatial lag regression. Because relationships are similar for public transportation travel time and to a lesser extent for automobile travel time, we do not present those regression results and only point out similarities and differences in the findings. Columns one and two, respectively, show the OLS and spatial regression results for Model 1. Controlling for neighborhood racial/ethnic composition (with percentage White residents as the reference category), population density, and land area, increasing percentage of neighborhood residents in poverty is associated with shorter distance to the nearest facility. Columns three and four show, respectively, the OLS and spatial regression results for Model 2. The interaction between percentage of residents in poverty and percentage of African–American residents is positive and statistically significant in both the OLS and spatial lag regression models, indicating that the (negative) effect of increasing poverty on distance becomes smaller (less negative) as the percentage of African–American residents in the neighborhood increases.
The OLS Models 1 and 2 account for 29.5 and 37.4% of the variance in distance to the nearest facility, respectively, (Table 2). For both Model 1 and Model 2, relationships are attenuated in the spatial model relative to the OLS model. As evidenced by the statistically significant likelihood ratio tests for spatial lag dependence, the residuals of the spatial models still exhibit spatial autocorrelation. Substantive relationships are similar for public transportation travel time (results not shown). However, for automobile travel time, the interaction between neighborhood poverty and African–American is statistically significant in the OLS model, but not in the spatial model (results not shown).
To depict the nature of the interaction effect between percentage in poverty and percentage African–American on spatial accessibility, we calculated predicted values based on the OLS results for distance to the nearest facility in neighborhoods with different concentrations of African–American residents: <20, 20–80, and >80% African–American. As shown in Figure the poverty slope is steep and negative for low and medium African–American neighborhoods, but relatively flat for high African–American neighborhoods.

Predicted values1 of distance to the nearest facility (natural log) for neighborhoods with low, medium, and high proportion of African–American (AA) residents.2
1Predicted values were calculated based on OLS regression results. We used the group-specific minimum and maximum values of percentage in poverty and the group-specific means of percent African–American, percentage Latino, percentage other race/ethnicity, population density, and land area.
2African–American (AA) residents: low African–American (<20%), medium African–American (20–80%), high African–American (>80%).
Discussion
Limitations
This study has limitations which should be considered when interpreting the results. First, the automobile and public transportation travel times are estimates. According to the Chicago Area Transportation Study (CATS), the automobile travel times are most useful for relative comparisons of travel times across locations.57 Estimation of public transportation travel times required a number of assumptions including time and date of travel. Thus, it is possible that the travel times are not generalizable for all business hours, days of the week, or throughout 2004, which is the year the facilities included in this study were operational. Public transportation travel times are based on the closest facility and do not necessarily reflect the minimum public transportation travel time between neighborhoods and facilities. In addition, the public transportation travel times are based on transportation schedules and do not take into account how far and thus, time required for residents to walk to and from transportation stops or delays resulting from buses or trains running off-schedule, which may differentially affect neighborhoods. Some evidence suggests, for example, that on-time performance and reliability are worst for a train line serving the south and west sides of Chicago, where most economically disadvantaged African–American neighborhoods are located.62
Successfully taking into account spatial autocorrelation in regression analyses with distance-based dependent variables is very difficult. By the nature of their measurement, distance-based variables exhibit strong positive spatial autocorrelation for small areas. Indeed, in this study, the residuals from the OLS and spatial regression models exhibit positive spatial autocorrelation. As a result, the regression coefficients may be biased or inefficient, which is a second limitation of the study. We tested the sensitivity of the spatial regression results to different spatial weights matrices and found that the “rook” spatial weights matrix provided the most conservative parameter estimates. Thus, we consider our spatial regression results very conservative. Indeed, the magnitude by which the regression coefficients are reduced in the spatial models relative to the OLS models result in substantively meaningless relationships. On the other hand, the robustness of relationships is bolstered by the fact that they remain statistically significant with this relatively small sample (n=343) and conservative spatial weights matrix in spatial regression analysis.
Third, we know of no other facilities that provided low- or no-fee screening mammography to Chicago residents in 2004, but it is possible that grant-funded low- or no-fee screening mammography may have been available at other facilities through community clinic-facility arrangements. That our key informants were unaware of other low- or no-fee mammography facilities suggests that if any were present, they likely served a small number of women. The results reflect the spatial accessibility of facilities with publicly funded programs that aim to provide screening mammography to low-income or uninsured women in Chicago.
Neighborhood Variation in Spatial Accessibility of Mammography Facilities
Despite these limitations, which may be addressed in future research, this study provides insights into the extent to which the spatial accessibility of facilities offering low- or no-fee screening mammography is equitable on the basis of socioeconomic and racial/ethnic characteristics of neighborhoods in Chicago. Given race-based and economic residential segregation in Chicago, it is not surprising that the accessibility of low- and no-fee mammography facilities differ by neighborhood SES and racial/ethnic composition.63 The finding that the distance and travel times to facilities providing low- or no-fee mammograms generally decrease as neighborhood poverty increases (Table 2) suggests that the spatial distribution of this type of health care service may match the spatial distribution of need. From a policy standpoint, this is encouraging and suggests spatial equity according to neighborhood SES. It is important to point out, nevertheless, that 40% of households in neighborhoods in the highest poverty category do not own a car according to estimates from 2000.58 Whereas facilities may be closer and automobile travel times to facilities shorter in economically disadvantaged neighborhoods, the locational advantage of economically disadvantaged neighborhoods may be “more than offset by the low level of auto ownership.”64 When considering the likely transportation mode to reach mammography facilities, women living in economically disadvantaged neighborhoods may have poorer access to facilities providing low- or no-fee mammograms because a much larger proportion of residents in these neighborhoods must rely on public transportation than in the lowest poverty neighborhoods. Our results show that public transportation travel times, on average, are 10 min longer than automobile travel times (Table 1).
We also found that reductions in the distance and travel time with increasing neighborhood poverty are less strong in African–American neighborhoods (Table 3). In fact, when adjusting for population density, geographic size, and proportion of residents in other racial/ethnic groups in the neighborhood, increasing neighborhood poverty is not associated with shorter travel distance in African–American neighborhoods (Fig. 1). Among neighborhoods with the greatest need for facilities offering low- or no-fee screening mammography (i.e., neighborhoods with the highest proportions of residents in poverty), African–American neighborhoods have longer travel distances and public transportation travel times than neighborhoods with proportionately fewer African–American residents. Thus, it appears that facilities offering affordable mammography services to low-income and uninsured women are not optimally spatially distributed in Chicago and that spatial inequity exists among economically disadvantaged neighborhoods, with African–American neighborhoods having somewhat poorer spatial access to facilities. Persistent socioeconomic and racial/ethnic disparities in breast cancer stage at diagnosis and survival suggest that an equitable distribution of affordable mammography is a worthwhile policy goal.
Some prior studies have found that the spatial accessibility of health care facilities, such as primary care, differs by the SES or racial/ethnic composition of urban neighborhoods,45 , 65 , 66 though the evidence is not consistent.67 , 68 This study adds to a growing literature suggesting that the spatial accessibility of some health resources (e.g., supermarkets) and risks (e.g., liquor stores) varies by both the socioeconomic and racial/ethnic characteristics of urban neighborhoods.69 , 70 Unlike these studies, our study shows that the spatial accessibility of a health resource—facilities providing low- and no-fee screening mammography—improves with increasing poverty in Chicago neighborhoods. However, under closer scrutiny, we found that improvements in spatial accessibility with increasing neighborhood poverty are limited to neighborhoods with lower proportions of African–American residents. These studies suggest that future investigations should consider both neighborhood socioeconomic characteristics and racial/ethnic composition when examining the spatial distribution of health resources and risks in urban areas.
One strength of our study is that we examined not only street network distance to mammography facilities, but also public transportation and automobile travel times. Nonetheless, our study was restricted to neighborhood variation in the spatial accessibility of facilities. Researchers may want to incorporate other important dimensions of accessibility at the levels of the facility (e.g., facility capacity, operating hours, wait time, quality of service, treatment by staff) or neighborhood (e.g., safety and comfort traveling to facility) in future studies. Our study did not consider, for example, whether the supply of mammography services, in terms of operating hours and number of providers or technicians, can accommodate demand. It is possible that women living in economically disadvantaged neighborhoods may experience prolonged waiting times for an appointment, despite having relatively good spatial access to facilities offering low- or no-fee screening mammography.
Conclusion
Eliminating racial/ethnic and socioeconomic disparities in breast cancer stage and survival requires understanding factors that contribute to poorer breast cancer outcomes among women of lower SES and women of most ethnic minority populations. Research is needed to examine whether long distances and travel times to facilities offering screening mammograms are barriers to mammography utilization. Whereas equity in the spatial distribution of health resources such as mammography facilities is important, inclusion of non-spatial factors at multiple levels can provide a more comprehensive understanding of the extent to which the accessibility of health resources is equitable across urban neighborhoods and populations and how resource accessibility affects health-related behaviors, health care utilization, and health status.
References
Ayanian JZ, Kohler BA, Abe T, Epstein AM. The relation between health insurance coverage and clinical outcomes among women with breast cancer. N Engl J Med. 1993;329(5):326–331.
Bradley CJ, Given CW, Roberts C. Race, socioeconomic status, and breast cancer treatment and survival. J Natl Cancer Inst. 2002;94(7):490–496.
Franzini L, Williams AF, Franklin J, Singletary SE, Theriault RL. Effects of race and socioeconomic status on survival of 1,332 black, Hispanic, and white women with breast cancer. Ann Surg Oncol. 1997;4(2):111–118.
Greenwald HP, Polissar NL, Dayal HH. Race, socioeconomic status and survival in three female cancers. Ethn Health. 1996;1(1):65–75.
Roetzheim RG, Gonzalez EC, Ferrante JM, Pal N, Van Durme DJ, Krischer JP. Effects of health insurance and race on breast carcinoma treatments and outcomes. Cancer J. 2000;89(11):2202–2213.
Du W, Simon MS. Racial disparities in treatment and survival of women with stage I–III breast cancer at a large academic medical center in metropolitan Detroit. Breast Cancer Res Treat. 2005;91(3):243–248.
Hsu JL, Glaser SL, West DW. Racial/ethnic differences in breast cancer survival among San Francisco Bay Area women. J Natl Cancer Inst. 1997;89(17):1311–1312.
Joslyn SA, West MM. Racial differences in breast carcinoma survival. Cancer J. 2000;88(1):114–123.
Li CI, Malone KE, Daling JR. Differences in breast cancer stage, treatment, and survival by race and ethnicity. Arch Intern Med. 2003;163:49–56.
O'Malley CD, Le GM, Glaser SL, Shema SJ, West DW. Socioeconomic status and breast carcinoma survival in four racial/ethnic groups: a population-based study. Cancer J. 2003;97(5):1303–1311.
Ries LAG, Eisner MP, Kosary CL, et al. SEER Cancer Statistics Review, 1975–2002. Bethesda, MD: National Cancer Institute; 2005. Available at: http://seer.cancer.gov/csr/1975_2002/. Accessed July 18, 2005.
Boyer-Chammard A, Taylor TH, Anton-Culver H. Survival differences in breast cancer among racial/ethnic groups: a population-based study. Cancer Detect Prev. 1999;23(6):463–473.
Hunter CP, Redmond CK, Chen VW, et al. Breast cancer: factors associated with stage at diagnosis in black and white women. Black/White Cancer Survival Study Group. J Natl Cancer Inst. 1993;85(14):1129–1137.
Schwartz KL, Crossley-May H, Vigneau FD, Brown K, Banerjee M. Race, socioeconomic status and stage at diagnosis for five common malignancies. Cancer Causes Control. 2003;14:761–766.
U.S.Preventive Services Task Force*. Screening for breast cancer: recommendations and rationale. Ann Intern Med. 2002;137(5_Part_1):344–346.
Smith RA, Saslow D, ndrews Sawyer K, et al. American cancer society guidelines for breast cancer screening: update 2003. CA: A Cancer Journal for Clinicians. 2003;53(3):141–169.
Practice Bulletin Number 42, April 2003: Breast cancer screening. Obstetrics and Gynecology. 2003;101(4):821–832.
Coughlin SS, Uhler RJ, Bobo JK, Caplan L. Breast cancer screening practices among women in the United States, 2000. Cancer Causes Control. 2004;15(2):159–170.
Leatherman S, McCarthy D. Quality of Health Care for Medicare Beneficiaries: a Chartbook. The Commonwealth Fund; May 2005. Available at: http://www.cmwf.org/publications/publications_show.htm?doc_id=275195. Accessed June 15, 2005.
Swan J, Breen N, Coates RJ, Rimer BK, Lee NC. Progress in cancer screening practices in the United States: results from the 2000 National Health Interview Survey. Cancer J. 2003;97(6):1528–1540.
Armstrong K, Long JA, Shea JA. Measuring adherence to mammography screening recommendations among low-income women. Prev Med. 2004;38(6):754–760.
Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System Prevalence Data [database online]. Available: http://apps.nccd.cdc.gov/brfss/. Atlanta, Georgia: USA Centers for Disease Control and Prevention; 1995–2004.
McPhee SJ, Nguyen TT, Shema SJ, et al. Validation of recall of breast and cervical cancer screening by women in an ethnically diverse population. Prev Med. 2002;35(5):463–473.
Kirby JB, Kaneda T. Neighborhood socioeconomic disadvantage and access to health care. J Health Soc Behav. 2005;46(1):15–31.
Wells BL, Horm JW. Targeting the underserved for breast and cervical cancer screening: the utility of ecological analysis using the National Health Interview Survey. Am J Public Health. 1998;88(10):1484–1489.
Barry J, Breen N. The importance of place of residence in predicting late-stage diagnosis of breast or cervical cancer. Health Place. 2005;11(1):15–29.
Merkin BS, Stevenson L, Powe N. Geographic socioeconomic status, race and advanced stage breast cancer in New York City. Am J Public Health. 2002;92(1):64–70.
Marchick J, Henson DE. Correlations between access to mammography and breast cancer stage at diagnosis. Cancer J. 2005;103(8):1571–1580.
Engelman KK, Hawley DB, Gazaway R, Mosier MC, Ahluwalia JS, Ellerbeck EF. Impact of geographic barriers on the utilization of mammograms by older rural women. J Am Geriatr Soc. 2002;50(1):62–68.
Hyndman JC, Holman CD, Dawes VP. Effect of distance and social disadvantage on the response to invitations to attend mammography screening. J Med Screen. 2000;7(3):141–145.
Kreher NE, Hickner JM, Ruffin MT, Lin CS. Effect of distance and travel time on rural women's compliance with screening mammography: an UPRNet study. Upper Peninsula Research Network. J Fam Pract. 1995;40(2):143–147.
Burgess JF, Jr, DeFiore DA. The effect of distance to VA facilities on the choice and level of utilization of VA outpatient services. Soc Sci Med. 1994;39(1):95–104.
Gregory PM, Malka ES, Kostis JB, Wilson AC, Arora JK, Rhoads GG. Impact of geographic proximity to cardiac revascularization services on service utilization. Med Care. 2000;38(1):45–57.
McCarthy JF, Blow FC. Older patients with serious mental illness: sensitivity to distance barriers for outpatient care. Med Care. 2004;42(11):1073–1080.
Mooney C, Zwanziger J, Phibbs CS, Schmitt S. Is travel distance a barrier to veterans' use of VA hospitals for medical surgical care? Soc Sci Med. 2000;50(12):1743–1755.
Rushton G, Peleg I, Banerjee A, Smith G, West M. Analyzing geographic patterns of disease incidence: rates of late-stage colorectal cancer in Iowa. J Med Syst. 2004;28(3):223–236.
Guagliardo MF. Spatial accessibility of primary care: concepts, methods and challenges. Int J Health Geogr. 2004;3(1):3.
Current Population Survey. Health Insurance Data [database online]. Available: http://www.census.gov/hhes/www/hlthins/data_access.html. Washington, DC: U.S.Census Bureau, Housing and Household Economic Statistics Division; 2004.
Suter LG, Nakano CY, Elmore JG. The personal costs and convenience of screening mammography. J Womens Health Gend Based Med. 2002;11(7):667–672.
McAlearney AS, Reeves KW, Tatum C, Paskett ED. Perceptions of insurance coverage for screening mammography among women in need of screening. Cancer J. 2005;103(12):2473–2480.
The National Breast and Cervical Cancer Early Detection Program—Reducing Mortality Through Screening. US Department of Health and Human Services, Centers for Disease Control and Prevention Web site; May 2004. Available at: http://www.cdc.gov/cancer/nbccedp/about.htm. Accessed October 1, 2005.
Kinman EL. Evaluating health service equity at a primary care clinic in Chilimarca, Bolivia. Soc Sci Med. 1999;49(5):663–678.
Talen E. School, community, and spatial equity: an empirical investigation of access to elementary schools in West Virginia. Annals of the Association of American Geographers. 2001;91(3):465–486.
Jargowsky P. Stunning Progress, Hidden Problems: The Dramatic Decline of Concentrated Poverty in the 1990s. Washington, District of Columbia: the Brookings Institution; May 2003. Available at: http://www.brookings.edu/es/urban/publications/jargowskypoverty.pdf. Accessed June 24, 2005.
Guagliardo MF, Ronzio CR, Cheung I, Chacko E, Joseph JG. Physician accessibility: an urban case study of pediatric providers. Health Place. 2004;10(3):273–283.
Abramson AJ, Tobin MS, VanderGoot MR. The changing geography of metropolitan opportunity: the segregation of the poor in U.S. metropolitan areas, 1970 to 1990. Housing Policy Debate. 1995;6(1):45–72.
Iceland J, Weinberg DH, Steinmetz E. Racial and Ethnic Residential Segregation in the United States: 1980–2000. Washington, District of Columbia: USA Government Printing Office; 2002. U.S. Census Bureau Series CENSR-3. Available at: http://www.census.gov/population/www/cen2000/briefs.html.
Sampson RJ, Morenoff JD, Earls F. Beyond social capital: spatial dynamics of collective efficacy for children. Am Soc Rev. 1999;64(633–660).
ArcView [computer program]. Version 3.3. Redlands, California: Environmental Systems Research Institute;1999–2002.
2003 TIGER/Line® Files [database online]. U.S. Census Bureau; 5 Mar 2004. Available at: http://www.census.gov/geo/www/tiger/. Accessed April 7, 2004.
Handy SL, Niemeier DA. Measuring accessibility: an exploration of issues and alternatives. Environment and Planning A. 1997;29:1175–1194.
Talen E. Neighborhoods as service providers: a methodology for evaluating pedestrian access. Environment and Planning B. 2003;30:181–200.
Accessibility Measures (script for use with ArcGIS Desktop) [computer program].Mar 2004. Available at: http://arcscripts.esri.com/.
ArcGIS Desktop [computer program]. Version 8.3. Redlands, California: Environmental Systems Research Institute;1999–2002.
Snap and Split Program [computer program].Dec 2003. Available at: http://arcscripts.esri.com/.
Chicago Transportation Authority CTA Trip Planner [interactive program online]. Available at: http://www.yourcta.com/maps/tripplanner.html. Accessed March 29, 2005.
Chicago Area Transportation Study. Conformity Analysis Documentation Appendix B: Travel Demand Modeling for the Conformity Process in Northeastern Illinois [documentation online]. Chicago Area Transportation Study; Aug 2003. Available at: http://www.catsmpo.com/prog/conformity/prog-conformity-appendixB.pdf. Accessed July 7, 2005.
US Census Bureau. Census 2000 Summary File 3 (SF 3)—Sample Data [database online]. Available: http://factfinder.census.gov/home/saff/main.html?_lang=en. Washington,DC: US Census Bureau; 2005.
Vasiliev IR. Visualization of spatial dependence: an elementary view of spatial autocorrelation. In: Arlinghaus SL, Griffith DA, Arlinghaus WC, Drake WD, Nysteun JD, eds. Practical Handbook of Spatial Statistics. Boca Raton, Florida: CRC; 1995:17–30.
Anselin L. Lagrange multiplier test diagnostics for spatial dependence and spatial heterogeneity. Geographical Analysis. 1988;20:1–17.
Anselin L. Spatial Econometrics: Methods and Models. Boston, Massachusetts: Kluwer Academic; 1988.
Hilkevitch J. CTA ride not worth fare in poorer areas, study says. Chicago Tribune. November 22, 2004:Page 1.
McLafferty S. Urban structure and geographical access to public services. Annals of the Association of American Geographers. 1982;72(3):347–354.
Shen Q. Location characteristics of inner-city neighborhoods and employment accessibility of low-wage workers. Environment and Planning A. 1998;25:345–365.
Luo W, Wang FH. Measures of spatial accessibility to health care in a GIS environment: synthesis and a case study in the Chicago region. Environment and Planning B. 2003;30(6):865–884.
McLafferty S, Grady S. Immigration and geographic access to prenatal clinics in Brooklyn, NY: a geographic information systems analysis. Am J Public Health. 2005;95(4):638–640.
Hyndman JC, D'Arcy C, Holman J, Pritchard DA. The influence of attractiveness factors and distance to general practice surgeries by level of social disadvantage and global access in Perth, Western Australia. Soc Sci Med. 2003;56(2):387–403.
Hyndman JC, Holman CD. Accessibility and spatial distribution of general practice services in an Australian city by levels of social disadvantage. Soc Sci Med. 2001;53(12):1599–1609.
LaVeist TA, Wallace JM. Health risk and inequitable distribution of liquor stores in African American neighborhoods. Soc Sci Med. 2000;51:613–617.
Zenk SN, Schulz AJ, Israel BA, James SA, Bao S, Wilson ML. Neighborhood racial composition, neighborhood poverty, and the spatial accessibility of supermarkets in metropolitan Detroit. Am J Public Health. 2005;95:660–667.
Acknowledgement
We would like to thank investigators at the University of Illinois at Chicago Center for Population Health and Health Disparities (5P50CA106743-02), especially Richard B. Warnecke, Richard T. Campbell, and Michael Berbaum, for helpful feedback on the analysis and manuscript. We also wish to thank Claire Bozic for providing and assisting us in using the automobile travel time data from the Chicago Area Transportation Study. This research was supported by: National Cancer Institute Cancer Education and Career Development Program # 5 R25T CA57699-12 (SNZ), The Health Services Research and Development Service Postdoctoral Fellowship Program of the Veterans Health Administration (ET), and the National Cancer Institute (5P50CA106743-02).
Author information
Authors and Affiliations
Corresponding author
Additional information
Zenk is with the Program in Cancer Control and Population Sciences, University of Illinois at Chicago, Chicago, IL 60608, USA; Tarlov is with the Midwest Center for Health Services and Policy Research, Hines VA Hospital, USA; Sun is with the Department of Sociology and Criminal Justice, Texas A&M University-Commerce, USA.
Rights and permissions
About this article
Cite this article
Zenk, S.N., Tarlov, E. & Sun, J. Spatial Equity in Facilities Providing Low- or No-Fee Screening Mammography in Chicago Neighborhoods. JURH 83, 195–210 (2006). https://doi.org/10.1007/s11524-005-9023-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-005-9023-4