
Abstract
Introduction
Medical mistrust is associated with disparities in a variety of health outcomes. The human papillomavirus (HPV) vaccine has the potential to decrease disparities in cervical cancer by preventing infection with the virus that causes these malignancies. No study has examined associations between medical mistrust and preventative health behaviors including the HPV vaccine among young minority women.
Methods
Self-reported racial/ethnic minority students completed a web-based survey in fall of 2011. Wilcoxon and Kruskal-Wallis were used to test differences in medical mistrust scores by demographics and health behaviors.
Results
Medical mistrust varied significantly by race with Black women reporting the highest scores. Women with no regular health-care provider (HCP) or who had difficulty talking to their provider had higher mistrust. Higher medical mistrust was associated with a preference to receive HPV vaccine recommendation from a HCP of the same race or ethnicity among unvaccinated women. Black and Asian women who had not received the HPV vaccine had higher mistrust scores than vaccinated women. Perceived difficulty in talking to a HCP was associated with ever having a Pap smear.
Discussion
Awareness of medical mistrust and the influence on health behaviors may aid in increasing delivery of quality health services for racial and ethnic minority populations. Further research among different populations is needed to elucidate impacts of medical mistrust and provider communication on preventative health behaviors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Human papillomavirus (HPV) is the most common sexually transmitted infection (STI) and is associated with anogenital warts and cancers in men and women. Racial/ethnic minorities are disproportionately affected by HPV-related cancers. Black and Hispanic women have higher rates of HPV prevalence [1] and cervical cancer incidence and mortality compared to Whites [2]. Prevention of cervical cancer previously relied on screening with cytology, the Pap smear [3]. The quadrivalent HPV vaccine is approved for women and men aged 9 to 26 and protects against types 6 and 11 (associated with 90 % of genital warts) and types 16 and 18 (associated with 70 % of cervical cancers). The vaccine is approved to prevent cervical, vaginal, and vulvar cancers/precancerous lesions (in women), genital warts, and anal cancers/precancerous lesions (both sexes). The Centers for Disease Control and Prevention estimates that approximately 26,000 cancers attributable to HPV occur annually in men and women, including virtually all 11,500 cervical cancer cases [4]. HPV 16 is also the most common type found in other HPV-related cancers; thus, the current vaccine has the potential to prevent a substantial number of cancers and the nonavalent vaccine currently in development may prevent an additional 20 % of cervical cancer cases [5].
Recent national and regional data on HPV vaccine utilization among adolescents, the targeted age group for vaccination, have identified disparities in vaccine uptake [6–11]. Emerging data on young adult women, who have the highest rates of HPV infection and HPV-related diseases, show continued disparities in vaccine uptake among this group [11, 10, 12]. In the 2010 adult vaccination coverage report, Hispanics had lower HPV vaccination coverage (15.1 %) compared with non-Hispanic Whites (22.4 %) [13]. The HPV vaccine has the potential to decrease disparities in cervical dysplasia and cancer if available to adolescent and young adult low-income and minority populations [14].
Medical mistrust is associated with disparities in cancer stage at diagnosis [15], breast cancer surgical and postsurgical adjuvant treatment and quality of life [16, 17], underutilization of health services [18], routine health examinations [19, 20], and cancer screening [21–23]. Studies of mistrust in HIV+ populations found associations between HIV conspiracy beliefs and antiretroviral treatment non-adherence [24] and less condom use [25] among Black men.
Few studies have examined associations between medical mistrust with STI preventative behaviors, and studies of medical mistrust and cancer screening have been conducted among older populations [21–23]. No study has examined potential associations between medical mistrust and preventative health behaviors such as cervical cancer screening and HPV vaccination among young racial and ethnic minorities. To begin to address this gap, this analysis examined associations between medical mistrust and provider communication with preventative health behaviors among racial/ethnic college students. We hypothesized that higher mistrust and greater difficulty talking to health-care providers (HCPs) would be associated with lack of preventative health behaviors in this population.
Methods
Participants
Participants were recruited from a large, public university in the Southeastern USA. Self-reported racial and ethnic minority students were sent an email invitation from the university’s registrar’s office with a link asking them to participate in a 15-min web-based survey. Survey items were adapted from previous research of psychosocial HPV studies among men and women [26–29] and were based on constructs from the Health Belief Model [30] and Social Cognitive Theory [31]. Items assessed a range of topics including sociodemographics, sexual behaviors, HPV knowledge and awareness, psychosocial factors, mistrust of health-care providers, HPV vaccine beliefs, acculturation, and HPV vaccination status. Surveys were completed in November and December of 2011 and all responses are self-reported. This study was approved by the University of South Florida’s Institutional Review Board.
Measures
Single items assessed demographic characteristics, how difficult participants find it to talk with a HCP, and health history items including whether participants had ever received a Pap smear, received at least one dose of the HPV vaccine, and when participants were last tested for STIs. Unvaccinated women who reported that they intended to get the HPV vaccine in the next year were asked if they had a place where they could go to get the vaccine and potential barriers to getting the vaccine. Participants were asked to report how they formally identified themselves (i.e., the race specified on a birth certificate, driver’s license, or other identifying record) to assess racial/ethnic group. For this analysis, racial/ethnic group was categorized as White, Black or African American, Hispanic or Latino/Latina, Asian, or Other. The category of 'Other' racial/ethnic group includes women selecting Other; Indian; Native Hawaiian or Other Pacific Islander; Native American, Alaskan Native; or Middle Eastern as very few participants selected these options.
Medical mistrust was defined as an individual’s distrust and suspicion of medical personnel and institutions. The 12-item Group-Based Medical Mistrust Scale (GBMMS), a validated instrument [22] that has been used in samples of racial/ethnic minority men and women [32], was used to assess medical mistrust in the current study. All responses for this instrument are on a 5-point Likert scale ranging from strongly disagree (0) to strongly agree (4). Factor analyses indicated a two-factor solution including eight of the original items as the most valid indicators of the medical mistrust latent construct [33]. Responses to these eight items were summed to create a medical mistrust score with higher scores indicating greater medical mistrust (theoretical range = 0 to 32). Knowledge of the HPV vaccine was assessed via seven true/false/not sure items. Attitudes toward the HPV vaccine were assessed via eight agree/disagree/neutral items.
Data Analysis
Mean and standard deviation (SD) of medical mistrust scores were calculated, and Wilcoxon and Kruskal-Wallis tests were employed to test differences by demographic and health behaviors. For difficulty talking to a health-care provider, responses were categorized as Not difficult (including “Not difficult at all” and “Not very difficult” response options) and Difficult (including “Somewhat difficult” and “Very difficult” response options). Participants who reported that they do not have a regular provider were excluded from analyses examining associations between health behaviors and provider communication. Chi-squared and Fisher’s exact tests were employed to examine differences by demographic and health behaviors. Analyses were conducted on the total sample (n = 711), Hispanic women (n = 329), and Black women (n = 189). Few women reported their race as Asian (n = 85), Other (n = 76), or White (n = 32); therefore, we did not conduct separate analyses among these subpopulations. All analyses were conducted using SAS version 9.3® software (Cary, NC).
Results
Demographics
Medical mistrust varied significantly by race (p < 0.01); Black women had the highest scores (mean = 12.0, SD = 5.2), followed by Asian women (mean = 8.6, SD = 5.7), Hispanic women (mean = 8.2, SD = 5.1), Other women (mean = 8.4, SD = 4.9), and White women (mean = 7.5, SD = 4.3). Mistrust varied significantly by age only among Black women (Table 1), with higher mistrust scores among women age 27 or older.
Medical Mistrust and Preventative Health Behaviors
Mistrust was associated with difficulty talking to a HCP (Table 1). Higher scores were found among women with no regular provider and women who had difficulty talking to their provider (p < 0.05 in total sample and Hispanic women). Among women who had not received the HPV vaccine, higher mistrust scores were observed among women who reported that they would be more likely to get the vaccine in the future if the HCP who offered it was of the same ethnicity (p < 0.05 in total sample and Hispanic women; Fig. 1) or gender (p < 0.05 in total sample) as them. Among unvaccinated women who reported that they intended to get the HPV vaccine in the next year, those who did not have a place to get the vaccine had higher mistrust scores than women who reported that they had a place they could go to get the vaccine (p < 0.05 in total sample and Hispanic women). Women who reported that “moral or religious reasons,” “side effects,” and “fear of what people would think” might prevent them from getting the vaccine had higher mistrust than women who did not report these barriers (p < 0.05 in total sample). Cost, getting three shots over 6 months, fear of vaccines, fear of needles, fear of what family might think, getting time off, transportation to a clinic, belief that the vaccine would not work, and belief that they were not at risk for HPV were not significantly associated with mistrust.
Among Black women, there were trends toward higher mistrust among those who had ever received a Pap smear (p = 0.09) and had a longer time since their most recent STI test (p = 0.07). There was a trend toward higher mistrust among women who had not received the HPV vaccine (Fig. 2). Further examination of this association among each of the racial and ethnic groups showed lower mistrust among vaccinated Black and Asian women, but not among Hispanic, White, or Other women. Medical mistrust mean and SD was 9.4 (5.9) among those who were not vaccinated compared to 7.2 (5.2) among vaccinated Asian women.

Mean medical mistrust scores by preference for a recommendation of the HPV vaccine by a health-care provider of the same ethnicity. Survey item asked, “I would be more likely to get the HPV vaccine if the doctor or health care provider who recommended it to me was of the same ethnicity as me.”

Mean medical mistrust scores by HPV vaccination status among the total sample and each racial and ethnic group
Medical Mistrust and HPV Vaccine Knowledge and Attitudes
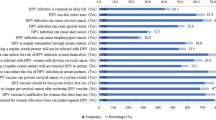
Women who agreed to the statement, “Once vaccinated, women no longer have to be screened for cervical cancer,” had higher mistrust scores among the total sample and Black women. Higher mistrust scores were observed among women who disagreed that the HPV vaccine is a safe vaccine (p < 0.05 in total sample). Women who agreed or were neutral to the statement “The HPV vaccine costs a lot of money” also had higher mistrust (p < 0.05 in total sample) (see Online Resource 1 for results of all knowledge and attitudes items).
Difficulty Talking to a Health-care Provider and Preventative Health Behaviors
Women who found talking to a HCP not difficult were more likely to report that they had ever had a Pap smear (p < 0.05 in Hispanic women) (Table 2). Women who did not have a regular provider were more likely to report difficulty talking to a provider (p < 0.05 in total sample and Hispanic women). Among women who intended to get the HPV vaccine in the next year, those who found talking to a HCP difficult were more likely to report that they would be more likely to get the vaccine if the HCP recommending it were of the same ethnicity (p < 0.05 in total sample and Black women). Barriers to HPV vaccination were not significantly associated with difficulty talking to a HCP.
Discussion
This exploratory research study describes associations between preventative health behaviors and medical mistrust among young, educated racial and ethnic minorities. A goal of the Healthy People 2020 Initiative in the area of access to health services is to “improve access to comprehensive, quality health-care services” as “access to comprehensive, quality health-care services is important for the achievement of health equity and for increasing the quality of a healthy life for everyone” [34]. Awareness of medical mistrust and the influence it may have on health behaviors may aid in increasing delivery of quality health services for racial and ethnic minority populations.
In this sample, women with higher mistrust were less likely to have engaged in preventative health behaviors such as HPV vaccination and STI screening. Associations between health behaviors differed by racial/ethnic group. Further refinement of racial/ethnic groups such as Puerto Rican, Mexican, or South American rather than a single Hispanic category may reveal differences in population subgroups.
A factor associated with higher trust among minority populations is racial concordance between the HCP and patient. According to the American Association of Medical Colleges, Hispanics and Blacks made up 13.2 and 12.2 % of the US population in 2002, but only 2.8 and 3.3 % of physicians, respectively. Increasing physician diversity may influence health-care disparities by improving access, increasing patient satisfaction, and ensuring culturally competent care [35]. A study of medication adherence among Black hypertensive patients reported that among patients in race-concordant relationships, provider communication was not significantly associated with adherence. However, among patients in race-discordant relationships, more collaborative communication was associated with better medication adherence [36]. Among unvaccinated women in this sample, those who preferred a provider of the same ethnicity and gender had higher mistrust scores. Increasing health-care provider diversity may increase participation in preventative health behaviors such as HPV vaccination among populations with higher mistrust of health-care providers and institutions. However, all health-care providers and institutions must be sensitized and given guidance regarding potential medical mistrust as a part of caring for all patients.
Barriers to HPV vaccination associated with medical mistrust included moral/religious reasons, side effects, and fear of what other people would think. Barriers to HPV vaccination include cost, logistics of obtaining the vaccine, side effects and safety, discomfort, and low perceptions of needing the vaccine [37]. Although cost may be an important barrier to vaccination, it was not related to mistrust. Women concerned with side effects of the HPV vaccine had higher mistrust than women who did not report this as a potential barrier. Previous studies have examined framing of HPV vaccine information such as loss-framed vs gain-framed [38] and tailoring based on an individual’s specific self-reported barriers vs non-tailored information [37]; however, mistrust has not been incorporated into studies examining the most effective manner to frame educational information on the HPV vaccine. Among a sample of adult African Americans, the manner in which colon cancer educational information is presented has been associated with positive emotions and willingness for screening [39]. Information framed to present progress (Blacks were doing better over time) and focused on increased colon cancer screening and decreased mortality were associated with positive emotional reactions and an increased interest in screening regardless of medical mistrust. When information is framed to present the impact of screening or the disparity between Blacks and Whites, interest in screening differs by medical mistrust with lower intentions among those with higher mistrust. Thus, how public health education information is framed may increase participation in preventative health behaviors regardless of medical mistrust. Future research on barriers to HPV vaccination and framing of health information related to HPV and the vaccine may benefit from including measures of mistrust.
Limitations
This was a convenience sample of minority college students. All participants were enrolled at the university, took classes in English, and had access to health care through the student health clinic; thus, results may not be generalizable to all young, minority women. All items were self-reported and there is the potential for recall bias and social desirability bias. Although the total sample was relatively large, there were only adequate samples of Black and Hispanic women to examine associations within these subgroups. There were fewer Black women, and failure to detect statistical significance for some variables could be due to the smaller sample size. Associations among Asian and Other minority women could not be evaluated due to the limited samples of these racial and ethnic groups in this study and may differ from Black and Hispanic women. Associations between mistrust and receipt of the HPV vaccine were only found among Black and Asian women and not Hispanic women. Further investigation among these subgroups is needed to elucidate factors that influence health behaviors among different racial and ethnic groups.
Previous research has shown that provider communication and endorsement of the HPV vaccine is associated with receipt among young women [10, 40, 41]; however, these factors have not been examined in relation to mistrust of health-care providers. Further research among different populations of young men and women with adequate sample sizes is needed to elucidate the impact of medical mistrust and provider communication on various preventative health behaviors including HPV vaccination and STI screening. The results of this study indicate that medical mistrust, provider communication, and racial/ethnic patient-provider concordance may be factors associated with health behaviors among young racial and ethnic minorities, a population which has not been a focus of previous research. The level of mistrust varies by population and associations with health behaviors may also differ; thus, it is important to examine these factors among different racial and ethnic groups of men and women.
References
Hariri S, Unger ER, Sternberg M, Dunne EF, Swan D, Patel S, et al. Prevalence of genital human papillomavirus among females in the United States, the National Health and Nutrition Examination Survey, 2003–2006. J Infect Dis. 2011;204(4):566–73.
SEER Stat Fact Sheets: cervix uteri. National Cancer Institute. 2010. http://seer.cancer.gov/statfacts/html/cervix.html. Accessed July 3 2010.
Wheeler CM. Natural history of human papillomavirus infections, cytologic and histologic abnormalities, and cancer. Obstet Gynecol Clin N Am. 2008;35(4):519–36.
Wu X, Watson M, Wilson R, Saraiya M, Cleveland JL, Markowitz L. Human papillomavirus-associated cancers—United States, 2004–2008. Morb Mortal Wkly Rep. 2012;61(15):258–61.
Drolet M, Laprise J-F, Boily M-C, Franco EL, Brisson M. Potential cost-effectiveness of the nonavalent human papillomavirus (HPV) vaccine. Int J Cancer. 2014;134(9):2264–8.
Pampel FC. Differences in the influence of family background and social activities on smoking of minority and white high school seniors, 1976–2004. J Immigr Minor Health Cent Minor Public Health. 2008;10(6):507–15.
Pruitt SL, Schootman M. Geographic disparity, area poverty, and human papillomavirus vaccination. Am J Prev Med. 2010;38(5):525–33.
Kennedy B, Valdimarsdóttir U, Sundström K, Sparén P, Lambe M, Fall K, et al. Loss of a parent and the risk of cancer in early life: a nationwide cohort study. Cancer Causes Control. 2014;25(4):499–506.
Balsam KF, Molina Y, Beadnell B, Simoni J, Walters K. Measuring multiple minority stress: the LGBT people of color microaggressions scale. Cult Divers Ethn Minor Psychol. 2011;17(2):163–74.
Conroy K, Rosenthal SL, Zimet GD, Yan J, Bernstein DI, Glynn S, et al. Human papillomavirus vaccine uptake, predictors of vaccination, and self-reported barriers to vaccination. J Women’s Health. 2009;18(10):1679–86.
Neubrand TPL, Radecki Breitkopf C, Rupp R, Breitkopf D, Rosenthal SL. Factors associated with completion of the human papillomavirus vaccine series. Clin Pediatr. 2009;48(9):966–9.
CDC. Adult vaccination coverage—United States, 2010. JAMA. 2012;307(11):1130–3.
Dorell C, Stokley S, Yankey D, Cohn A, Markowitz L. National, state, and local area vaccination coverage among adolescents aged 13–17 years—United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(32):1018–23.
Jeudin P, Liveright E, del Carmen MG, Perkins RB. Race, ethnicity and income as factors for HPV vaccine acceptance and use. Hum Vaccines Immunotherapeutics. 2013;9(7):1413–20.
Bergamo C, Lin JJ, Smith C, Lurslurchachai L, Halm EA, Powell CA, et al. Evaluating beliefs associated with late-stage lung cancer presentation in minorities. J Thorac Oncol. 2013;8(1):12–8. doi:10.1097/JTO.0b013e3182762ce4.
Maly RC, Stein JA, Umezawa Y, Leake B, Anglin MD. Racial/ethnic differences in breast cancer outcomes among older patients: effects of physician communication and patient empowerment. Health Psychol. 2008;27(6):728–36.
Bickell NA, Weidmann J, Fei K, Lin JJ, Leventhal H. Underuse of breast cancer adjuvant treatment: patient knowledge, beliefs, and medical mistrust. J Clin Oncol. 2009;27(31):5160–7.
LaVeist TA, Isaac LA, Williams KP. Mistrust of health care organizations is associated with underutilization of health services. Health Serv Res. 2009;44(6):2093–105.
Hammond WP, Matthews D, Corbie-Smith G. Psychosocial factors associated with routine health examination scheduling and receipt among African American men. J Natl Med Assoc. 2010;102(4):276–89.
Hammond W, Matthews D, Mohottige D, Agyemang A, Corbie-Smith G. Masculinity, medical mistrust, and preventive health services delays among community-dwelling African-American Men. J Gen Intern Med. 2010;25(12):1300–8.
Purnell JQ, Katz ML, Andersen BL, Palesh O, Figueroa-Moseley C, Jean-Pierre P, et al. Social and cultural factors are related to perceived colorectal cancer screening benefits and intentions in African Americans. J Behav Med. 2010;33(1):24–34.
Thompson HS, Valdimarsdottir HB, Winkel G, Jandorf L, Redd W. The Group-Based Medical Mistrust Scale: psychometric properties and association with breast cancer screening. Prev Med. 2004;38(2):209–18.
Shelton R, Winkel G, Davis S, Roberts N, Valdimarsdottir H, Hall S, et al. Validation of the group-based medical mistrust scale among urban black men. J Gen Intern Med. 2010;25(6):549–55.
Bogart LM, Wagner G, Galvan FH, Banks D. Conspiracy beliefs about HIV are related to antiretroviral treatment nonadherence among African American Men with HIV. JAIDS J Acquir Immune Defic Syndr. 2010;53(5):648–55. doi:10.1097/QAI.0b013e3181c57dbc.
Bogart LM, Galvan FH, Wagner GJ, Klein DJ. Longitudinal association of HIV conspiracy beliefs with sexual risk among black males living with HIV. AIDS Behav. 2011;15(6):1180–6.
Daley EM, Perrin KM, McDermott RJ, Vamos CA, Rayko HL, Packing-Ebuen JL, et al. The psychosocial burden of HPV. J Health Psychol. 2010;15(2):279–90.
Daley EM, Buhi ER, Baldwin J, Lee JH, Vadaparampil S, Abrahamsen M, et al. Men’s responses to HPV test results: development of a theory-based survey. Am J Health Behav. 2009;33(6):728–44.
Gerend MA, Lee SC, Shepherd JE. Predictors of human papillomavirus vaccination acceptability among underserved women. Sex Transm Dis. 2007;34(7):468–71.
Wheldon CW, Daley EM, Buhi ER, Nyitray AG, Giuliano AR. Health beliefs and attitudes associated with HPV vaccine intention among young gay and bisexual men in the southeastern United States. Vaccine. 2011;29(45):8060–5.
Janz NK, Champion VL, Strecher VJ. The health belief model. In: Glanz K, Rimer BK, Lewis FM, editors. Health behavior and health education: theory, research and practice. San Francisco: Jossey-Bass; 2002.
Coreil J. Chapter 4: Behavioral and social science theory. In: Coreil J, editor. Social and behavioral foundation of public health. 2nd ed. Thousand Oaks: Sage Publications; 2010. p. 67–90.
Halbert CH, Weathers B, Delmoor E, Mahler B, Coyne J, Thompson HS, et al. Racial differences in medical mistrust among men diagnosed with prostate cancer. Cancer. 2009;115(11):2553–61.
Kolar SK, Wheldon C, Hernandez N, Daley EM, Young L, Chandler R, et al. Evaluation of the factor structure and validity of the Group-Based Medical Mistrust Scale (GBMMS) among a racially and ethnically diverse sample of college students American Public Health Association 140th Annual Meeting & Expo; October 30, 2012. San Francisco: American Public Health Association; 2012.
Healthy People 2020 Framework. U.S. Department of Health and Human Services. http://www.healthypeople.gov/2020/default.aspx. Accessed Oct 6 2013.
America needs a more diverse physician workforce. American Association of Medical Colleges. 2012. Accessed Oct 7 2013.
Schoenthaler A, Allegrante J, Chaplin W, Ogedegbe G. The effect of patient–provider communication on medication adherence in hypertensive black patients: does race concordance matter? Ann Behav Med. 2012;43(3):372–82.
Gerend MA, Shepherd MA, Lustria MLA. Increasing human papillomavirus vaccine acceptability by tailoring messages to young adult women’s perceived barriers. Sex Transm Dis. 2013;40(5):401–5. doi:10.1097/OLQ.0b013e318283c8a8.
Gerend MA, Shepherd JE. Using message framing to promote acceptance of the human papillomavirus vaccine. Health Psychol. 2007;26(6):745–52.
Nicholson RA, Kreuter MW, Lapka C, Wellborn R, Clark EM, Sanders-Thompson V, et al. Unintended effects of emphasizing disparities in cancer communication to African-Americans. Cancer Epidemiol Biomark Prev. 2008;17(11):2946–53.
Cropsey KL, Jackson DO, Hale GJ, Carpenter MJ, Stitzer ML. Impact of self-initiated pre-quit smoking reduction on cessation rates: results of a clinical trial of smoking cessation among female prisoners. Addict Behav. 2011;36(1–2):73–8.
Daley EM, Vamos CA, Buhi ER, Kolar SK, McDermott RJ, Hernandez N, et al. Influences on human papillomavirus vaccination status among female college students. J Wom Health. 2010;19(10):1885–91.
Ethical Standard Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). Informed consent was obtained from all patients for being included in the study.
Funding Source
This research was funded by the University of South Florida, College of Public Health, Department of Community and Family Health, Student Research Award.
Conflict of Interest
Stephanie K. Kolar, Christopher Wheldon, Natalie D. Hernandez, Lauren Young, and Nancy Romero-Daza have no conflicts of interest to declare. Ellen M. Daly is a member of Merck’s National HPV Vaccine Advisory Board.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Online Resource 1
(PDF 36 kb)
Rights and permissions
About this article

Cite this article
Kolar, S.K., Wheldon, C., Hernandez, N.D. et al. Human Papillomavirus Vaccine Knowledge and Attitudes, Preventative Health Behaviors, and Medical Mistrust Among a Racially and Ethnically Diverse Sample of College Women. J. Racial and Ethnic Health Disparities 2, 77–85 (2015). https://doi.org/10.1007/s40615-014-0050-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-014-0050-2