
Abstract
Purpose of Review
Hundreds of millions of people worldwide are exposed to arsenic via contaminated water. The goal of this study was to identify whether arsenic-associated lung function deficits resemble obstructive- or restrictive-like lung disease, in order to help illuminate a mechanistic pathway and identify at-risk populations.
Recent Findings
We recently published a qualitative systematic review outlining the body of research on arsenic and non-malignant respiratory outcomes. Evidence from several populations, at different life stages, and at different levels of exposure showed consistent associations of arsenic exposure with chronic lung disease mortality, respiratory symptoms, and lower lung function levels. The published review, however, only conducted a broad qualitative description of the published studies without considering specific spirometry patterns, without conducting a meta-analysis, and without evaluating the dose-response relationship.
Summary
We searched PubMed and Embase for studies on environmental arsenic exposure and lung function. We performed a meta-analysis using inverse-variance-weighted random effects models to summarize adjusted effect estimates for arsenic and forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio. Across nine studies, median water arsenic levels ranged from 23 to 860 μg/L. The pooled estimated mean difference (MD) comparing the highest category of arsenic exposure (ranging from > 11 to > 800 μg/L) versus the lowest (ranging from < 10 to < 100 μg/L) for each study for FEV1 was – 42 mL (95% confidence interval (CI) − 70, − 16) and for FVC was – 50 mL (95% CI − 63, − 37). Three studies reported effect estimates for FEV1/FVC, for which there was no evidence of an association; the pooled estimated MD was 0.01 (95% CI − 0.005, 0.024). This review supports that arsenic is associated with restrictive impairments based on inverse associations between arsenic and FEV1 and FVC, but not with FEV1/FVC. Future studies should confirm whether low-level arsenic exposure is a restrictive lung disease risk factor in order to identify at-risk populations in the USA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Arsenic exposure, through the consumption of naturally contaminated groundwater or food, threatens the health of millions of people in countries throughout the world [1]. Prior research shows that chronic arsenic exposure has adverse health effects in several organ systems, including the cardiopulmonary system [2]. The International Agency for Research on Cancer classifies arsenic in drinking water as a type 1 lung carcinogen, meaning there is sufficient evidence that arsenic in water causes lung cancer [3]. There is also growing evidence that arsenic is associated with non-malignant respiratory disease [4]. Evidence from several populations, at different life stages, and at different levels of exposure (generally comparing levels higher than 100 μg/L versus lower exposures) showed consistent associations of chronic arsenic exposure with chronic lung disease mortality [5,6,7,8], respiratory symptoms [9, 10], and lower lung function levels [11,12,13]. Although these epidemiologic observations provide supportive evidence of a link between arsenic and chronic lung disease morbidity and mortality, the specific pattern of lung disease associated with arsenic remains unclear. We recently published a qualitative systematic review outlining the body of research on arsenic and non-malignant respiratory outcomes [4]. The published review, however, only conducted a broad qualitative description of the published studies without considering specific spirometric patterns, without conducting a meta-analysis, and without evaluating the dose-response relationship.
Spirometry is an accurate and frequently used method for assessing pulmonary function. Some of the most important spirometry measures include the total volume of air forcefully expelled after a full inhalation, the forced vital capacity (FVC), the forced expiratory volume in the first second of exhalation (FEV1), and the ratio of FEV1 to FVC (FEV1/FVC). Although pulmonary function tests do not diagnose specific lung diseases, different lung diseases are associated with different patterns of abnormalities in pulmonary function tests [14]. Obstructive lung diseases, like chronic bronchitis and asthma, are associated with chronic inflammation and, thus, obstruction of the airways. An obstructive pattern lung function test is characterized by a reduced FEV1/FVC and FEV1, but a preserved FVC. Alternatively, restrictive lung disease, like pulmonary fibrosis, may develop from increased formation of scar tissue in the lung and, thus, restricted lung expansion. A restrictive pattern lung function test is generally characterized by a reduced FEV1 and FVC, but a stable or higher FEV1/FVC. Linking arsenic-associated lung function deficits to a specific spirometry pattern (i.e., obstruction or restriction) may further elucidate relevant pathophysiologic pathways for environmentally related lung disease [15].
The goal of this analysis was to evaluate whether the patterns of association between arsenic exposure and lung function measures from previously published observational epidemiologic research are suggestive of restrictive deficits.
Methods
Search Strategy and Data Abstraction
This review followed the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines [16] (Supplementary Table 1). We attempted to identify all observational studies assessing the association between arsenic exposure and lung function. Using keyword and MeSH/emtree terms (search terms: arsenic OR arsenicals AND respiratory function OR lung function OR forced expiratory volume OR vital capacity OR Pulmonary function), we searched PubMed and Embase through January 2017 with no language restrictions. In addition, we reviewed the references from all relevant original research and review articles. Two investigators (TRS and MP) screened each article using the study selection criteria (Fig. 1). Epidemiologic studies with data on arsenic exposure and lung function endpoints were included. We excluded non-peer-reviewed studies, non-original reports, animal studies, case reports and case studies, and studies without adequate measures of arsenic exposure or lung function. For arsenic exposure markers, eligible studies were included if they measured arsenic in water, blood, or urine. We excluded studies for which urinary arsenic was the only measure of exposure that did not account for seafood arsenical levels, as nontoxic seafood arsenicals may be a major source of bias among study populations with moderate seafood consumption [17]. We excluded studies that used the presence or absence of arsenical skin lesions without another measure of arsenic exposure from our primary analysis, as skin lesions, though strongly associated with high levels of arsenic exposure, may also be influenced by susceptibility and not exclusively a result of arsenic exposure alone. We also excluded studies where arsenic exposure occurred chemotherapeutically [18]. For lung function endpoints, we included all spirometry measures assessed in the individual studies but we only analyzed the measures that were reported in at least three publications. Two investigators (TRS, MP) independently abstracted study data, including design, study population (location, age, and sex distribution), sample size, arsenic assessment and exposure levels, lung function outcomes, study results (measures of association), and other variables adjusted for in the statistical analysis. Discrepancies were resolved by a third investigator (AN). For studies with regression models with multiple levels of adjustment, we abstracted the measure of association obtained from the regression model that was adjusted for the most variables (fully adjusted model) after confirming the fully adjusted model did not have markedly different findings compared to the more parsimonious model. Quality of individual studies (Supplementary Table 2) was assessed using similar methods as in a published systematic review on arsenic [19].

Study identification and inclusion/exclusion criteria for study selection
Statistical Methods
Measures of association (comparisons of means, linear regression coefficients), their standard errors, and sample size were abstracted or derived from published data [20]. For studies only reporting group means and standard deviations of the relevant outcome [13, 21], we constructed crude coefficient estimates using the linear discriminant function method [20]. All analyses were performed using Stata software, version 14.1 (StataCorp, College Station, TX, USA). Figures were created using R, version 3.4.0.
For our main analysis, we used an inverse-variance-weighted random effects model to summarize (pool) the measure of association comparing mean lung function level in the highest category of arsenic exposure versus the lowest category of exposure for each study. When available, we used measures of association for water arsenic. If water arsenic was not reported, we used measures of association for urinary arsenic (total urinary arsenic). For studies only reporting stratified measures of association (i.e., by sex or smoking status) [22, 23], we pooled the measures of association from each stratum (males/females or smoking/non-smoking) using a separate inverse-variance-weighted random effects model before including one summary measure per study in our overall analysis [24].
For studies which reported measures of association using arsenic as a categorical and continuous variable [11, 25], we confirmed that both approaches (categorical or continuous) were consistent with one another by using measures of association for continuous arsenic rather than categorical arsenic, again using a random effects model. Although most of the included studies used water arsenic as their main marker of exposure, two studies only had urinary arsenic [13, 26, 13, 25] and another study reported measures of association for both [11]. To confirm results using water arsenic or urine arsenic were generally consistent with one another, we stratified studies by exposure measure (water and urine). Consistency was determined as the confidence intervals for categorical and continuous approaches overlapped.
We used the I2 statistic to quantify heterogeneity, which describes the proportion of total variation in summary estimates due to heterogeneity. To examine the relative influence of each study on summary estimates, we omitted one study at a time. We also assessed publication bias graphically using funnel plots [27] and statistically using Egger’s [27] and Begg’s test [28].
There was a wide range of arsenic exposure levels and cut points between and within studies. Although we were unable to conduct a formal dose-response meta-analysis [29] due to limitations in reported data (lack of information on means and standard deviations for all levels of exposure including the reference group), we assessed the exposure-response relationship graphically. First, we identified the mean/median within each exposure category of a given study. If a measure of central tendency was not available for exposure categories and the category was bounded, we used the midpoint, and for upper categories with unbound maxima, we estimated what the median would be by assuming the category had the same width as the category immediately below it. Next, we organized all measures of association (i.e., using all exposure categories from every study) into one of the three different exposure groups: low exposure (< 100 μg/L), moderate exposure (100–400 μg/L), and high exposure (> 400 μg/L). We used an inverse-variance-weighted random effects model to produce summary estimates for each category.
We conducted subgroup analyses by sex, smoking status, and early life exposure (looking at early life exposure and lung function in children and early life exposure and lung function in adults). For studies with measures of association stratified by sex or smoking status, we first used an inverse-variance-weighted random effects model to summarize the association between arsenic and lung function stratified by sex or smoking status, and second, used meta-regression to test whether stratified summary estimates were different from each other. Meta-regression is used to examine the extent to which statistical heterogeneity between results of multiple studies can be related to one or more characteristics of the studies [30]. We evaluated whether sex, smoking status, or timing of exposure were significant effect modifiers using the metareg command in STATA (Supplementary Figure 3 and Supplementary Table 4).
Results
Study Characteristics
After screening titles, abstracts, and/or full texts of 807 unique references identified in the literature search, nine publications met the inclusion criteria (Fig. 1). Studies were conducted in five countries, including Bangladesh, Chile, India, Mexico, and Pakistan, and they were published between 2005 and 2017 (Table 1). The sample size of individual studies ranged from 97 to 942 participants, and across studies, the total number of participants was 4699. Participants ranged from 7 to 65 years of age and included both men and women, except one study that only included men [21]. By study design, there were two prospective cohort studies [11, 26], three retrospective studies [12, 23, 25], which reconstructed early life arsenic exposure from historical measures of water arsenic, and four cross-sectional studies [13, 21, 22, 31]. Studies were characterized by a wide range of arsenic exposure, although in most studies the majority of the arsenic-exposed population was exposed to water arsenic levels above 100 μg/L. Five studies assigned exposure based on the levels of arsenic in the public water supply for the town or city in which the subjects lived [12, 21,22,23, 31] and two studies assigned exposure based on the arsenic level measured in each participant’s primary well [11, 25]. Three studies included exposure based on participants’ total urinary arsenic levels [11, 13, 26]. One used maternal urinary arsenic levels during gestation as a proxy for in utero exposure and lung function among children 9 years of age [26]. For the study outcomes, nine studies reported FEV1 and FVC. Three studies also reported measures of association between arsenic and FEV1/FVC. Two studies reported measures of association for arsenic and the forced expiratory flow between 25 and 75% of FVC and the peak expiratory flow rate.
Most studies adjusted for sex, age, and height. One study, however, did not adjust for any potential confounders [21]. Although spirometry is an effort-dependent test, all except one study [22] explicitly stated they performed lung function tests in accordance with international guidelines set forth jointly by the American Thoracic Society and the European Respiratory Society, which facilitate spirometry maneuver standardization (Table 1) [32, 31]. Most studies also controlled for established lung function risk factors including smoking status and education.
Summary Estimates and Sensitivity Analyses
Forest plots illustrate the summary (pooled) estimates for the mean FEV1 and FVC levels comparing the highest to the lowest arsenic exposure categories from individual studies (Fig. 2). The pooled estimated mean difference comparing arsenic exposure categories was – 42 mL (95% confidence interval (CI): − 70, − 16) for FEV1 and – 50 mL (95% CI − 63, − 37) for FVC. Statistical heterogeneity was relatively high for FEV1 (I2 = 80%) but moderate for FVC (I2 = 34%) but the direction of the association between arsenic and FEV1 and FVC for all nine studies was consistent (mean differences for all nine studies were less than zero). Of the three studies that reported a measure of association for arsenic and FEV1/FVC, the pooled estimated mean difference for FEV1/FVC was 0.01 (95% CI − 0.005, 0.024). Statistical tests of publication bias were non-significant (Supplementary Figure 1).

Mean difference (MD) in forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC) comparing the highest to lowest categories of arsenic exposure, organized by year of publication. The size of each filled square was calculated using inverse-variance weighting. Horizontal lines represent 95% confidence intervals. Diamonds represent summary estimates from inverse-variance-weighted random effects models. Open diamonds represent summary estimate including all nine publications. Filled diamonds represent summary estimate excluding two influential studies
In sensitivity analyses, there were two studies that influenced the results of our meta-analysis. After removing the two studies [13, 21] for which we had calculated the standard error from unadjusted group means and standard deviations as the original publications did not report adjusted mean differences and standard errors, the pooled estimated mean difference comparing arsenic exposure categories was – 58 mL (95% CI − 99, − 17) for FEV1 and was – 87 mL (95%CI − 151, − 23) for FVC (n = 7 studies). Test for publication bias for FEV1 was P = 0.04 and for FVC was P = 0.06, if we excluded those two studies. Stratifying pooled estimates by exposure medium (i.e., water/urine) resulted in similar findings. Using arsenic as a continuous predictor rather than categorical predictor attenuated the associations (Supplementary Figure 2 and Supplementary Table 3).
Exposure-Response Analysis
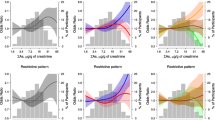
Six of the nine included studies reported measures of association at multiple exposure levels for FEV1 and FVC; however, the available data for FEV1/FVC was insufficient for an exposure-response evaluation due to the lack of reported data for FEV1/FVC at multiple arsenic exposure levels. For FEV1, the pooled estimated mean difference was – 30 mL (95% CI − 55, − 6, n = 4 studies) for the low exposure group (< 100 μg/L), − 36 mL (95% CI − 68, − 4, n = 6 studies) for the moderate exposure group (100–400 μg/L), and – 54 mL (95% CI − 147, 38, n = 5 studies) for the high exposure group (> 400 μg/L). For FVC, the pooled estimated mean difference was – 29 mL (95% CI − 75, 18, n = 4 studies) for the low exposure group, − 50 mL (95% CI − 94, − 5, n = 6 studies) for the moderate exposure group, and – 123 mL (95% CI − 257, 10, n = 5 studies) for the high exposure group (Fig. 3).

Mean difference (MD) in forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC) organized into three arsenic exposure subgroups (high > 400, moderate 100–400, low < 100 μg/L) compared to the lowest exposure category of each study, including measures of association from all exposure categories from all studies using an inverse-variance-weighted random effects model. Exposure subgrouping was determined by the mean/median within each exposure category of a given study. If a measure of central tendency was not available for exposure categories, the midpoint was used if the category was bounded or the lower bound was used for categories with unbound maxima. The size of each square represents the overall weight of the observation via inverse-variance weighting. Horizontal lines represent 95% confidence intervals. Open diamonds represent subgroup summary estimates from inverse-variance-weighted random effects models. Closed black diamonds represent overall summary estimates
Subgroup Analyses
Several studies reported measures of association on arsenic and lung function (FEV1 and FVC only) stratified by sex [11, 12, 22, 26] or smoking status [11, 12, 22, 23]. Half of the studies also examined early life exposure [12, 13, 23, 25, 26] (Supplementary Table 4). Stratifying by sex, the pooled estimated mean differences comparing arsenic exposed versus unexposed for FEV1 was – 8 mL (95% CI − 22, 5) for females and – 67 mL (95% CI − 129, − 5) for males, and for FVC it was – 12 mL (95% CI − 31, 7) for females and – 47 mL (95% CI − 102, 7) for males (subgroup differences: FEV1 P = 0.33, FVC P = 0.55, n = 4 studies). Stratifying by smoking status, the pooled estimated mean difference comparing arsenic-exposed group versus the reference group for FEV1 was – 56 mL (95% CI − 164, 52) for smokers and – 51 mL (95% CI − 97, − 5) for non-smokers, and for FVC it was – 50 mL (95% CI − 155, 55) for smokers and – 92 mL (95% CI − 187, 2) for non-smokers (subgroup differences: FEV1 P = 0.86, FVC P = 0.63, n = 4 studies). Categorizing studies by timing of exposure, the pooled estimated mean difference for FEV1 was – 14 mL (95% CI − 25, − 5, n = 5 studies) for studies of early life exposure and – 66 mL (95% CI − 106, − 25, n = 4 studies) for studies with exposure in adulthood, and for FVC it was – 46 mL (95% CI − 56, − 36, n = 5 studies) for early life exposure studies and – 95 mL (95% CI − 172, − 19, n = 4 studies) for studies with exposure in adulthood (subgroup differences: FEV1 P = 0.01, FVC P = 0.58). Stratifying by age at lung function test yielded results similar to stratifying by early life exposure.
Discussion
In this meta-analysis of lung function spirometry outcomes, arsenic exposure was associated with lower FEV1 and FVC levels but not with FEV1/FVC. These findings support that arsenic exposure is associated with restrictive lung deficits. A dose-response relationship between increasing arsenic exposure levels and decreasing FEV1 and FVC was strongly suggested, although the information available did not allow the conduction of a formal dose-response meta-analysis. The results held in several sensitivity analyses and we found limited evidence of differential association by sex or smoking status, although the associations were stronger among men.
The consistent negative relationships between arsenic and decrements in FVC support that arsenic exposure is likely associated with a restrictive pattern lung disease; however, given the small number of studies reporting data on FEV1/FVC, we are unable to entirely rule out whether arsenic-associated lung function deficits also resemble obstruction, which can be characterized by a reduced FEV1/FVC. Two studies that were excluded from the meta-analysis discussed findings for the association of arsenic with FEV1/FVC. One study was conducted among 2460 adults from the Wuhan cohort across China [33] and it was excluded because the only measure of arsenic exposure, total urinary arsenic, was not adjusted for seafood intake (the primary source of nontoxic seafood arsenicals) among a population for which seafood consumption is common and could have resulted in major exposure misclassification [17]. In that study (mean urinary arsenic = 29.1 μg/L), arsenic was not associated with FVC, and there was an association with increased FEV1 and increased FEV1/FVC [33]. The other study was conducted among 159 adults in West Bengal, India, and it was excluded because skin lesion status was the only measure of arsenic exposure. In that study, participants with arsenic-induced skin lesions had lower mean FEV1, FVC, and FEV1/FVC compared to participants without lesions [34]. This study was consistent with our findings indicating a mixed or restrictive pattern lung disease.
Biological Plausibility
Evidence suggests that pulmonary fibrosis, a restrictive lung disease, is preceded by lung injury, inflammation, altered wound repair, and extracellular matrix remodeling [35]. These mechanisms have also been linked to arsenic exposure [36,37,38]. Cystic fibrosis and arsenic have both shown to be associated with bronchiectasis, a rare lung disease [6, 39], suggesting that arsenic may act through similar mechanisms. Cystic fibrosis is an autosomal recessive genetic lung disease caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. As the CFTR protein regulates fluid transport in the lungs, CFTR dysregulation can result in an insufficient clearance of lung pathogens and airway inflammation. Interestingly, an epidemiologic study from Bangladesh found elevated sweat chloride levels (the diagnostic test for cystic fibrosis) among persons exposed to arsenic but who lacked a genetic diagnosis of cystic fibrosis [40••]. Cell studies have also found that arsenic exposure promotes multiubiquitination of CFTR resulting in CFTR degradation [41]. Further, toxicological studies also show that when tracheal epithelial cells and alveolar macrophages are exposed to arsenite, cellular injury is induced by reactive oxygen species generation and synthesis of stress proteins [42, 43]. Clara cell 16 (CC16) is one of the 20 proteins secreted by Clara cells in the lung’s alveolar epithelium that protects the respiratory tract against oxidative stress and inflammation [44]. In humans, urine arsenic levels have been associated with decreased serum levels of CC16 [45]. Evidence also shows that arsenic exposure activates inflammatory markers. For instance, human and in vivo studies have found that arsenic exposure is inked to increased levels of matrix metalloproteinase-9 [36, 46], a biomarker of lung inflammation and airway remodeling [47].
Smoking, another environmental exposure associated with lung inflammation and interstitial lung disease [48], may modify the relationship between arsenic and the respiratory system. Previous epidemiologic studies examining the interaction between smoking, arsenic, and lung cancer generally support the presence of a synergistic interaction [49, 50]. Less is known, however, for non-malignant lung disease. In our subgroup meta-analysis, among the four studies that stratified their results by smoking status, the association between arsenic and FVC was slightly stronger among non-smokers than smokers. It is, however, unclear why the association between arsenic and FEV1 was comparable among smokers and non-smokers while the magnitude of the association between arsenic and FVC was greater among non-smokers. None of the studies reported the association between arsenic and FEV1/FVC by smoking status.
In our subgroup meta-analysis among the four studies that stratified their results by sex, men appeared to have stronger pooled effect estimates for FEV1 and FVC compared to women. The findings are consistent with more general evidence from the 2015 Global Burden of Disease that shows males are more likely than females to be affected by chronic lung disease, both in terms of disability-adjusted life years and deaths [51].
There is increasing recognition of the importance of early life arsenic exposure to disease in adulthood [52, 53]. Prenatal arsenic exposure may influence the lungs through altered wound repair and extracellular matrix remodeling. Mice exposed to 100 μg/L arsenic prenatally showed increased airway smooth muscle, decreased collagen content, and increased airway reactivity [37]. An increase in smooth muscle is associated with an altered expression of extracellular matrix components, including collagen and elastin [54], leading to a more disorganized and expanded matrix around the airways and blood vessels in the lining of the lung [55•]. Mice prenatally exposed to much lower levels of arsenic (10 μg/L in maternal drinking water) also showed impaired parenchymal lung mechanics and function during infancy; however, alterations to lung mechanics recovered by adulthood [56], supporting the possibility that early respiratory dysfunction associated with arsenic exposure may be reversible if exposure is eliminated. In our subgroup meta-analysis categorizing studies by timing of arsenic exposure (i.e., early life versus adulthood), pooled effect estimates showed that while early life arsenic exposure had a lasting influence on lung function, arsenic exposure in adulthood was also important. Although this subgroup analyses could not rule out the possibility that in some studies children were not only exposed in early life but also exposed chronically, results were similar for our subgroup meta-analysis categorizing studies by age at lung function test, with adults again showing larger FEV1 deficits than children. This finding could support the relative importance of chronic exposure or the possibility that even if exposure occurs early in life, the respiratory consequences associated with arsenic may be at least partially reversible if exposure is eliminated.
Together, the toxicological evidence supports the biological plausibility of the observed associations in this meta-analysis and indicates that the lung is sensitive to arsenic. Further, our findings are suggestive of a dose-response relationship between arsenic and both FEV1 and FVC. While the included studies characterized a wide range of arsenic exposure levels, in most studies, the majority of the population was exposed to water arsenic levels ten times higher than the current World Health Organization guideline and U.S. Environmental Protection Agency standard of 10 μg/L.
Limitations
Only nine publications on arsenic exposure and lung function met the inclusion criteria. The included studies were mostly among populations exposed to high levels of arsenic exposure (> 100 μg/L). Less is thus known about the relation between arsenic and lung function at exposure levels common in the USA (< 10 μg/L). Our analysis was also limited by the selective reporting of outcomes within studies, particularly the lack of reporting a measure of association for FEV1/FVC and the different approaches used to analyze and interpret lung function data across studies. As such, comparing point estimates for arsenic to other lung toxicants, like smoking, was complicated by the lack of an acceptable spirometry reference equation for each of the populations studied. Further, the summary estimates of this meta-analysis should be used in a descriptive rather than in an inferential manner since all studies included in this meta-analysis were observational and highly heterogeneous. As with all systematic reviews, our study may be subject to publication bias. After visually assessing funnel plots, there was a suggestion of publication bias but statistical tests of publication bias were non-significant (Supplementary Figure 1). Most studies controlled for potential confounders, including age, sex, height, smoking, and education; however, residual confounding may have affected our meta-analysis and contributed to the statistical heterogeneity between studies. Only three of the included studies provided some information on participants’ existing disease status and/or medication use. In a study in Chile, the few participants who reported having physician-diagnosed emphysema or bronchiectasis were included [23]. In a study in Bangladesh, only participants with respiratory symptoms, including chronic cough shortness of breath or blood in the sputum during 5 years of follow-up, were included [11]. In a study in Mexico, participants with asthma were excluded [13]. These differences may also explain the heterogeneity of our results.
Conclusions
This meta-analysis evaluated the relationship between arsenic exposure and lung function spirometry measures. We identified an inverse association between arsenic exposure and both FEV1 and FVC, but no association for FEV1/FVC. These findings show that arsenic exposure may be associated with a restrictive pattern lung disease. However, an obstructive or a mixed pattern lung function deficit cannot entirely be ruled out as our analysis is limited by the small number of studies reporting measures of association with FEV1/FVC. Identifying a specific lung function deficit pattern associated with arsenic exposure, like restriction, and potential effect measure modifiers, like smoking and sex, can guide future research aimed at understanding relevant pathophysiological pathways and at-risk populations.
Abbreviations
- ATS:
-
American Thoracic Society
- CFTR:
-
Cystic fibrosis transmembrane conductance
- ERS:
-
European Respiratory Society
- FEV1/FVC:
-
Ratio of FEV1 to FVC
- FEV1 :
-
Forced expiratory volume in one second
- FVC:
-
Forced vital capacity
- PFT:
-
Pulmonary function test
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
World Health Organization. Exposure to arsenic: a major public health concern. http://www.who.int/ipcs/features/arsenic.pdf. Published 2010. Accessed November 15, 2016.
National Research Council. Critical aspects of EPA’s IRIS assessment of inorganic arsenic: interim report. Washington, DC: The National Academies Press; 2014.
Straif K, Benbrahim-Tallaa L, Baan R, Grosse Y, Secretan B, el Ghissassi F, et al. A review of human carcinogens—part C: metals, arsenic, dusts, and fibres. Lancet Oncol. 2009;10(5):453–4. https://doi.org/10.1016/S1470-2045(09)70134-2.
Sanchez TR, Perzanowski M, Graziano JH. Inorganic arsenic and respiratory health, from early life exposure to sex-specific effects: a systematic review. Environ Res. 2016;147:537–55. https://doi.org/10.1016/j.envres.2016.02.009.
Smith AH, Marshall G, Yuan Y, Liaw J, Ferreccio C, Steinmaus C. Evidence from Chile that arsenic in drinking water may increase mortality from pulmonary tuberculosis. Am J Epidemiol. 2011;173(4):414–20. https://doi.org/10.1093/aje/kwq383.
Smith AH, Marshall G, Yuan Y, Ferreccio C, Liaw J, von Ehrenstein O, et al. Increased mortality from lung cancer and bronchiectasis in young adults after exposure to arsenic in utero and in early childhood. Environ Health Perspect. 2006;114(8):1293–6.
Tsai SM, Wang TN, Ko YC. Mortality for certain diseases in areas with high levels of arsenic in drinking water. Arch Environ Health. 1999;54(3):186–93. https://doi.org/10.1080/00039899909602258.
Argos M, Parvez F, Rahman M, Rakibuz-Zaman M, Ahmed A, Hore SK, et al. Arsenic and lung disease mortality in Bangladeshi adults. Epidemiology. 2014;25(4):536–43. https://doi.org/10.1097/EDE.0000000000000106.
Pesola GR, Parvez F, Chen Y, Ahmed A, Hasan R, Ahsan H. Arsenic exposure from drinking water and dyspnoea risk in Araihazar, Bangladesh: a population-based study. Eur Respir J. 2012;39(5):1076–83. https://doi.org/10.1183/09031936.00042611.
Rahman A, Vahter M, Ekstrom EC, Persson LA. Arsenic exposure in pregnancy increases the risk of lower respiratory tract infection and diarrhea during infancy in Bangladesh. Environ Health Perspect. 2011;119(5):719–24. https://doi.org/10.1289/ehp.1002265.
Parvez F, Chen Y, Yunus M, Olopade C, Segers S, Slavkovich V, et al. Arsenic exposure and impaired lung function. Findings from a large population-based prospective cohort study. Am J Respir Crit Care Med. 2013;188(7):813–9. https://doi.org/10.1164/rccm.201212-2282OC.
Dauphine DC, Ferreccio C, Guntur S, et al. Lung function in adults following in utero and childhood exposure to arsenic in drinking water: preliminary findings. Int Arch Occup Environ Health. 2011;84(6):591–600. https://doi.org/10.1007/s00420-010-0591-6.
Recio-Vega R, Gonzalez-Cortes T, Olivas-Calderon E, Lantz RC, Gandolfi AJ, De Alba CG. In utero and early childhood exposure to arsenic decreases lung function in children. J Appl Toxicol. 2015;35(4):358–66. https://doi.org/10.1002/jat.3023.
Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948–68. https://doi.org/10.1183/09031936.05.00035205.
Steele MP, Schwartz DA. Molecular mechanisms in progressive idiopathic pulmonary fibrosis. Annu Rev Med. 2012;64(1):120928131129008–276. https://doi.org/10.1146/annurev-med-042711-142004.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology a proposal for reporting. JAMA. 2000;283(15):2008–12. https://doi.org/10.1001/jama.283.15.2008.
Navas-Acien A, Francesconi KA, Silbergeld EK, Guallar E. Seafood intake and urine concentrations of total arsenic, dimethylarsinate and arsenobetaine in the US population. Environ Res. 2011;111(1):110–8. https://doi.org/10.1016/j.envres.2010.10.009.
Ho JC, Au WY, Han L, Kwong YL, Ip MS. Effect of therapeutic arsenic exposure on pulmonary function. Respir Med. 2013;107(9):1423–30. https://doi.org/10.1016/j.rmed.2013.06.012.
Navas-Acien A, Sharrett AR, Silbergeld EK, Schwartz BS, Nachman KE, Burke TA, et al. Arsenic exposure and cardiovascular disease: a systematic review of the epidemiologic evidence. Am J Epidemiol. 2005;162(11):1037–49. https://doi.org/10.1093/aje/kwi330.
Greenland S. Quantitative methods in the review of epidemiologic literature. Epidemiol Rev. 1987;9:1–30.
Das D, Bindhani B, Mukherjee B, Saha H, Biswas P, Dutta K, et al. Chronic low-level arsenic exposure reduces lung function in male population without skin lesions. Int J Public Health. 2014;59(4):655–63. https://doi.org/10.1007/s00038-014-0567-5.
von Ehrenstein OS, Mazumder DNG, Yuan Y, Samanta S, Balmes J, Sil A, et al. Decrements in lung function related to arsenic in drinking water in West Bengal, India. Am J Epidemiol. 2005;162(6):533–41. https://doi.org/10.1093/aje/kwi236.
Steinmaus C, Ferreccio C, Acevedo J, Balmes JR, Liaw J, Troncoso P, et al. High risks of lung disease associated with early-life and moderate lifetime arsenic exposure in northern Chile. Toxicol Appl Pharmacol. 2016;313:10–5. https://doi.org/10.1016/j.taap.2016.10.006.
Egger M, Davey-Smith G, Altman D (eds). Systematic reviews in health care: meta-analysis in context, 2nd edition. London: BMJ Publishing Group; 2001. https://doi.org/10.1002/9780470693926.
Smith AH, Yunus M, Khan AF, Ercumen A, Yuan Y, Smith MH, et al. Chronic respiratory symptoms in children following in utero and early life exposure to arsenic in drinking water in Bangladesh. Int J Epidemiol. 2013;42(4):1077–86. https://doi.org/10.1093/ije/dyt120.
Ahmed S, Akhtar E, Roy A, von Ehrenstein OS, Vahter M, Wagatsuma Y, et al. Arsenic exposure alters lung function and airway inflammation in children: a cohort study in rural Bangladesh. Environ Int. 2017;101:108–16. https://doi.org/10.1016/j.envint.2017.01.014.
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ, 1997;315(7109):629–34. https://doi.org/10.1136/bmj.315.7109.629.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Crippa A, Orsini N. Dose-response meta-analysis of differences in means. BMC Med Res Methodol. 2016;16:91. https://doi.org/10.1186/s12874-016-0189-0.
Harbord RM, Higgins JPT. Meta-regression in Stata. Stata J. 2008;8(4):493–519.
Nafees AA, Kazi A, Fatmi Z, Irfan M, Ali A, Kayama F. Lung function decrement with arsenic exposure to drinking groundwater along River Indus: a comparative cross-sectional study. Environ Geochem Health. 2011;33(2):203–16. https://doi.org/10.1007/s10653-010-9333-7.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–38. https://doi.org/10.1183/09031936.05.00034805.
Feng W, Huang X, Zhang C, et al. The dose–response association of urinary metals with altered pulmonary function and risks of restrictive and obstructive lung diseases: a population-based study in China. BMJ Open. 2015;1(5):1–24. https://doi.org/10.1017/CBO9781107415324.004.
De BK, Majumdar D, Sen S, Guru S, Kundu S. Pulmonary involvement in chronic arsenic poisoning from drinking contaminated ground-water. J Assoc Physicians India. 2004;52:395–400.
Selman M, Pardo A. Alveolar epithelial cell disintegrity and subsequent activation. Am J Respir Crit Care Med. 2012;186(2):119–21. https://doi.org/10.1164/rccm.201206-0997ED.
Olsen CE, Liguori AE, Zong Y, Lantz RC, Burgess JL, Boitano S. Arsenic upregulates MMP-9 and inhibits wound repair in human airway epithelial cells. Am J Physiol Lung Cell Mol Physiol. 2008;295(2):L293–302. https://doi.org/10.1152/ajplung.00134.2007.
Lantz RC, Chau B, Sarihan P, Witten ML, Pivniouk VI, Chen GJ. In utero and postnatal exposure to arsenic alters pulmonary structure and function. Toxicol Appl Pharmacol. 2009;235(1):105–13. https://doi.org/10.1016/j.taap.2008.11.012.
Choudhury S, Gupta P, Ghosh S, Mukherjee S, Chakraborty P, Chatterji U, et al. Arsenic-induced dose-dependent modulation of the NF-κB/IL-6 axis in thymocytes triggers differential immune responses. Toxicology. 2016;357-358:85–96. https://doi.org/10.1016/j.tox.2016.06.005.
Mazumder DN, Steinmaus C, Bhattacharya P, et al. Bronchiectasis in persons with skin lesions resulting from arsenic in drinking water. Epidemiology. 2005;16(6):760–5.
•• Mazumdar M, Christiani DC, Biswas SK, Ibne-Hasan OS, Kapur K, Hug C. Elevated sweat chloride levels due to arsenic toxicity. N Engl J Med. 2015;372(6):582–3. https://doi.org/10.1056/NEJMc1413312. This study shows evidence that arsenic is associated with elevated sweat chloride levels among persons exposed to arsenic in the absence of a genetic diagnosis of cystic fibrosis.
Bomberger JM, Coutermarsh BA, Barnaby RL, Stanton BA. Arsenic promotes ubiquitinylation and lysosomal degradation of cystic fibrosis transmembrane conductance regulator (CFTR) chloride channels in human airway epithelial cells. J Biol Chem. 2012;287(21):17130–9. https://doi.org/10.1074/jbc.M111.338855.
Han SG, Castranova V, Vallyathan V. Heat shock protein 70 as an indicator of early lung injury caused by exposure to arsenic. Mol Cell Biochem. 2005;277(1–2):153–64. https://doi.org/10.1007/s11010-005-5874-y.
Cohen DS, Palmer E, Welch WJ, Sheppard D. The response of guinea pig airway epithelial cells and alveolar macrophages to environmental stress. Am J Respir Cell Mol Biol. 1991;5(2):133–43.
Broeckaert F, Clippe A, Knoops B, Hermans C, Bernard A. Clara cell secretory protein (CC16): features as a peripheral lung biomarker. Ann N Y Acad Sci. 2000;923:68–77. https://doi.org/10.1111/j.1749-6632.2000.tb05520.x.
Parvez F, Chen Y, Brandt-Rauf PW, Bernard A, Dumont X, Slavkovich V, et al. Nonmalignant respiratory effects of chronic arsenic exposure from drinking water among never-smokers in Bangladesh. Environ Health Perspect. 2008;116(2):190–5. https://doi.org/10.1289/ehp.9507.
Olivas-Calderon E, Recio-Vega R, Gandolfi AJ, et al. Lung inflammation biomarkers and lung function in children chronically exposed to arsenic. Toxicol Appl Pharmacol. 2015;287:161–7. https://doi.org/10.1016/j.taap.2015.06.001.
Atkinson JJ, Senior RM. Matrix metalloproteinase-9 in lung remodeling. Am J Respir Cell Mol Biol. 2003;28(1):12–24. https://doi.org/10.1165/rcmb.2002-0166TR.
Lederer DJ, Enright PL, Kawut SM, Hoffman EA, Hunninghake G, van Beek EJR, et al. Cigarette smoking is associated with subclinical parenchymal lung disease: the Multi-Ethnic Study of Atherosclerosis (MESA)-lung study. Am J Respir Crit Care Med. 2009;180(5):407–14. https://doi.org/10.1164/rccm.200812-1966OC.
Ferreccio C, Gonzalez C, Milosavjlevic V, Marshall G, Sancha AM, Smith AH. Lung cancer and arsenic concentrations in drinking water in Chile. Epidemiology. 2000;11(6):673–9. https://doi.org/10.1097/00001648-200011000-00010.
Hertz-Picciotto I, Smith AH, Holtzman D, Lipsett M, Alexeeff G. Synergism between occupational arsenic exposure and smoking in the induction of lung cancer. Epidemiology. 1992;3(1):23–31.
IHME. Epi visualization. http://ghdx.healthdata.org/gbd-results-tool?params=querytool-permalink/fc7c45515025010a96c2a7dd49ed751f. Published 2016. Accessed October 27, 2016.
Carlin DJ, Naujokas MF, Bradham KD, Cowden J, Heacock M, Henry HF, et al. Arsenic and environmental health: state of the science and future research opportunities. Environ Health Perspect. 2015;124:890–9. https://doi.org/10.1289/ehp.1510209.
Farzan SF, Korrick S, Li Z, Enelow R, Gandolfi AJ, Madan J, et al. In utero arsenic exposure and infant infection in a United States cohort: a prospective study. Environ Res. 2013;126:24–30. https://doi.org/10.1016/j.envres.2013.05.001.
Araujo BB, Dolhnikoff M, Silva LFF, Elliot J, Lindeman JHN, Ferreira DS, et al. Extracellular matrix components and regulators in the airway smooth muscle in asthma. Eur Respir J. 2008;32(1):61–9. https://doi.org/10.1183/09031936.00147807.
• Sherwood CL, Lantz RC. Lung cancer and other pulmonary disease. In: States JC, ed. Arsenic: exposure sources, health risks, and mechanisms of toxicity. John Wiley & Sons, Inc.; 2015:137–162. https://doi.org/10.1002/9781118876992.ch7. This chapter reviews possible mechanisms for arsenic-associated lung disease, both malignant and non-malignant.
Ramsey KA, Larcombe AN, Sly PD, Zosky GR. In utero exposure to low dose arsenic via drinking water impairs early life lung mechanics in mice. BMC Pharmacol Toxicol. 2013;14:13. https://doi.org/10.1186/2050-6511-14-13.
Funding
This work was supported by the National Institute of Environmental Health Sciences at the National Institutes of Health (grant numbers R01ES021367, 1R01ES025216, 5P30ES009089, and P42ES010349).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Water and Health
Electronic Supplementary Material
ESM 1
(DOCX 250 kb)
Rights and permissions
About this article

Cite this article
Sanchez, T.R., Powers, M., Perzanowski, M. et al. A Meta-analysis of Arsenic Exposure and Lung Function: Is There Evidence of Restrictive or Obstructive Lung Disease?. Curr Envir Health Rpt 5, 244–254 (2018). https://doi.org/10.1007/s40572-018-0192-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40572-018-0192-1