
Abstract
Background
Since oral organs function in the first stage of the swallowing process, it is possible that decline in swallowing function can be partly related to oral frailty.
Aims
The purpose of this study was to investigate the association between swallowing function and oral function among community-dwelling elderly Japanese and to propose cut-off values for screening of decline in swallowing function.
Methods
A total of 188 participants were included in the analysis. The number of present teeth and functioning teeth were counted. Bacteria counts in tongue coat, oral wettability, tongue pressure, oral diadochokinesis (ODK), masticatory ability and bite force were examined. Swallowing function was assessed using the 10-item Eating Assessment Tool (EAT-10). Receiver operating characteristic curves were used to determine the cut-off points of each oral function parameter. A logistic regression model was performed to determine the combination of parameters with the highest accuracy for differentiating decline in swallowing function from normal.
Results
Subjects with ODK /pa/ sound < 6.2 times/second had higher prevalence of swallowing problems than those with 6.2 times/second or more. EAT-10 scores of one or more were significantly related to older age (≥ 71 years old; odds ratio [OR] 4.321) and reduced ODK /pa/ sound (< 6.2 times/second; OR 2.914).
Conclusions
Among community-dwelling elderly Japanese, those who were suspected of having decline in swallowing function had lower oral function than those who did not, and the cut-off values were 71 years of age and ODK /pa/ sound 6.2 times/s.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Swallowing is an event in which a bolus is sent to the pharynx. A swallowing reflex occurs when the bolus enters the pharynx, and the bolus then enters the esophagus without entering the airway [1]. Swallowing is a critical process for life, and allowing food and fluid to be ingested safely and efficiently [2].
Difficulty swallowing (dysphagia) is a pathophysiologic status characterized by taking more time and effort to move food or liquid from the pharynx to the stomach. There are many causes of dysphagia such as achalasia [3], esophageal stricture [4], neurological disorders [5] and neurological damages [6]. The main risk factor for dysphagia is aging. Due to natural aging and normal wear on the esophagus, and a greater risk of certain conditions such as stroke or Parkinson’s disease, older adults are at higher risk of swallowing difficulties.
Dysphagia affects nutritional deterioration [7] and frailty [8]. In the field of geriatric dentistry, the concept of oral frailty representing a decline in oral function has been proposed [9, 10]. Oral frailty is considered one of the early stages of frailty, and shows a mild decline in oral function with symptoms such as reduced tongue function, spilling foods, and slight choking.
Since oral organs function in the first stage of the swallowing process, it is possible that dysphagia can be partly related to oral frailty. We hypothesized that decreased swallowing function was associated with oral function. The purpose of this study was to investigate the association between swallowing function and oral function among community-dwelling elderly Japanese and to propose cut-off values for screening of decline in swallowing function.
Materials and methods
Participants
The present study used a cross-sectional design. We estimated the sample size using SamplePower version 3.0 statistical software (IBM, Tokyo, Japan). This software computed the power for a test of the null hypothesis in which the event rate in the two groups was identical. According to our preliminary study, the minimum sample size required to detect significant differences in decline in swallowing function in both positive and negative groups was 170 with an event rate (oral diadochokinesis [ODK] /pa/ sound ≥ 6.2 times/second; 0.59 and < 6.2 times/s; 0.81) of 80% power and a two-sided significance level of 5% (SamplePower ver. 3).
Inclusion criteria for the participants were age 60 years and older and having visited Preventive Dentistry Clinic at Okayama University Hospital between November 2017 and June 2018. Exclusion criteria were inability to answer the questionnaire independently and inability to walk independently. All participants provided written informed consent for study participation. The STROBE guidelines were followed and the study protocol was approved by the Ethics Committee of the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences (No. 1708-028).
Assessment of swallowing function
For the assessment of swallowing function, the 10-item Eating Assessment Tool (EAT-10) (Nestle Nutrition Institute, Vevey, Switzerland) was used. EAT-10 is a dysphagia screening questionnaire composed of ten questions. Each question is answered on a 5-point scale from 0 (no problem) to 4 (severely problematic), with total scores ranging from 0 to 40 points.
Assessment of oral function
The number of present teeth and functioning teeth were counted. This included the number of functioning teeth present and the number of functioning artificial teeth of dental prosthesis. Teeth with severe decay and stump teeth were not considered functioning teeth [11].
Next, we examined bacteria counts in tongue coat, oral wettability, tongue pressure, ODK, bite force, and masticatory ability [12]. Each test was performed twice and the average value was calculated.
Bacteria counts in tongue coat
The central part of the back of the tongue was rubbed with a sterilized cotton swab three times at a distance of 1 cm to prepare a specimen. The rubbing pressure was set to 20 gf using a constant-pressure sample collection device (Bacterial-counter, Panasonic Healthcare, Osaka, Japan). Thereafter, the total number of microorganisms in the specimen was measured using a bacterial counter (Panasonic Healthcare).
Oral wettability
The degree of wetness of the mucous membrane was measured at the center of the back of the tongue about 10 mm from the tongue tip and the left and right buccal mucosa. The oral moisture meter (Mucus®, LIFE, Tokyo, Japan) was used for measurement. The sensor of the meter was pressed on the mucosa with a pressure of approximately 200 g so that it contacts the surface to be measured uniformly, and the measured value was displayed within approximately 2 s.
Tongue pressure
Maximum tongue pressure was measured using a tongue pressure measuring device (JMS tongue pressure measuring instrument, JMS, Hiroshima, Japan). The balloon of the tongue pressure probe was set at the front part of the palate. The tongue pressure was measured by optionally crushing the balloon between the tongue and the palate with the maximum tongue force.
ODK
The ODK test evaluates the speed and regularity of articulatory organs by making the alternating syllables move as fast as possible. It is widely used to evaluate motor dysarthria. In Japan, three types of syllables, i.e., /pa/, /ta/, and /ka/ are often used. Of these, /pa/ evaluates the function of the lips, /ta/ evaluates the function of the tongue tip, and /ka/ evaluates the function of the tongue dorsum. Participants were asked to repeat each given syllable—/pa/, /ta/, /ka/—sequentially as fast as possible for 5 s using a device (KENKOU-KUN handy. Takei Scientific Instruments Co., Ltd., Niigata, Japan). The number of repetitions per second was calculated as the repetition speed of the syllables.
Masticatory ability
Participants chewed 2 g of gummy jelly (Gurucolum, GC, Tokyo, Japan) freely for 20 s. After gargling with 10 mL of water, gummy and water were discharged into a filter mesh, and the amount of glucose dissolved in the solution that passed through the mesh was determined using a glucose sensor (GS-II, GC).
Bite force
Bite force was measured with pressure-sensitive films (Dental Prescale II, GC), analytical software (Bite force analyzer, GC) and a precalibrated scanning device (GT-X830, Seiko Epson Corp., Suwa, Japan). All participants were asked to bite a film with their maximum strength for 3 s after it was confirmed that it was in the position of centric dental occlusion.
Questionnaire
Participants were asked for their age, gender, type of medicine they were taking.
Statistical analysis
An EAT-10 score of 0 indicated no problems with swallowing function, and a score of 1 or more indicated reduced swallowing function.
Receiver operating characteristic (ROC) curves were used to determine the cut-off points of each oral function parameter with calculation of the area under the curve (AUC) for accuracy, sensitivity, and specificity. The p value was considered significant if ≤ 0.05 at the 95% confidence interval. A logistic regression model was performed to determine the combination of parameters with the highest accuracy for differentiating slightly declined swallowing function from normal. All data were analyzed by IBM Statistical Package for the Social Sciences (SPSS, Tokyo, Japan) version 21.
Results
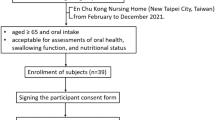
Of the 219 people who agreed to participate in this study, 212 were evaluated for oral function. Swallowing function was not evaluated in 7 participants and 24 participants had missing data. Finally, 188 subjects were included in the analysis (Fig. 1).

Flowchart of study participants
Table 1 shows the characteristics of the participants. The number (%) of participants without any swallowing problems (i.e., EAT-10 score of 0) was 141 (75.0%), and the number with swallowing problems was 47 (EAT-10 score of 1 or 2, n = 26, 13.8%; EAT-10 score of ≥ 3, n = 21, 11.2%). Of the 188 participants, 148 (78.7%) were taking medicine. The most common was medicine for hypertension (41.5%) and hyperlipidemia (22.3%). There were no significant differences in oral wettability between the participants with and without each medicine for hypertension, hyperlipidemia, diabetes mellitus, kidney disease and others (data not shown). Nobody was taking any medicine that affected tongue and jaw motor function.
ROC curve analyses were used to evaluate the values of bacterial counts in tongue coat, oral wettability, tongue pressure, ODK, masticatory ability, bite force, number of present teeth, number of functional teeth and age to predict swallowing function. The optimal cut-off value was an age of ≥ 71 years, giving a sensitivity of 85.1%, a specificity of 44.7%, positive predictive value of 33.9% and negative predictive value of 90.0% in predicting declining swallowing function. The second best parameter was ODK /pa/ sound with an AUC of 0.638. Bacteria counts in tongue coat, oral wettability, tongue pressure, ODK /ka/ sound and number of functional teeth did not significantly correlate with declining swallowing function (p ≥ 0.05) (Table 2).
Table 3 shows the results of binomial logistic regression analysis with these items as independent variables and EAT-10 score of 0 or > 1 as the dependent variable. The EAT-10 score was significantly related to age (odds ratio [OR] 4.321, 95% confidence interval [CI] 1.743–10.710) and ODK /pa/ sound (OR 2.914, 95% CI 1.103–7.695).
Discussion
Our hypothesis was that decreased swallowing function was associated with decreased oral function. In this study among community-dwelling elderly Japanese, those with oral ODK /pa/ sound of < 6.2 times/s were more likely to show dysphagia as assessed by the EAT-10 than those with ODK /pa/ sound of ≥ 6.2 times/second (OR 2.914, 95% CI 1.103–7.695). To the best of our knowledge, this is the first study to show an association between decreased swallowing function and articulatory oral motor skills among independent elderly.
The ODK /pa/ sound represents lip motor function. Some cross-sectional studies reported an association between lip motor function and swallowing function. ODK using the syllables /pataka/ was significantly associated with aspiration risk [13]. Lip-closure power in patients with dysphagia was significantly lower than that in healthy participants [14]. In many cases, sending a bolus from the oral cavity to the pharynx involves not only the tongue, but also oral functions such as lip closure and jaw position stability [1]. Swallowing requires the coordinated activity of many nerves and muscles of mouth, lips, pharynx, and larynx. All of these muscles work in a coordinated way. Lips play a major role in forming the bolus of food that is to be swallowed. Lips also help to create a tight seal which prevents food and liquids from leaking during the swallowing reflex. Proper lip motor function reflects well-controlled nerve and muscle abilities, leading to normal swallowing. Our findings support the association between decreased swallowing function and the ODK /pa/ sound.
The gold standard method for evaluating swallowing function is swallowing contrast examination using video fluoroscopy [15]. However, it requires special equipment and technology and is difficult to administer in elderly facilities or at home. The development of swallowing evaluation by the questionnaire method has been introduced, and its usefulness has been recognized [16]. Various questionnaires are used in surveys of elderly people at home. EAT-10 is a simple swallowing state evaluation form that allows evaluation of swallowing function. The reliability and validity of the Japanese version of EAT-10 have been verified. Therefore, EAT-10 was used for epidemiological studies in Japan and we also used EAT-10 in this study.
We set 6.2 times/s as the new cut-off value for ODK /pa/ sound based on the ROC curve results to detect early stage reductions in swallowing function as assessed by EAT-10. EAT-10 score is based on subjective symptoms related to swallowing. According to the present results, the negative predictive value of ODK /pa/ is 86.7%, which means that nearly 90% of the participants with > 6.2 times/s of ODK/pa/ sound had no subjective dissatisfaction with swallowing. It might be useful to estimate the proportion of such residents in the population with low prevalence of subjective swallowing difficulty and to predict a subclinical level of swallowing difficulty at an early stage. Various cut-off values have been reported for ODK. In the definition of hypo-oral function proposed by the Japan Geriatric Dental Society, if the ODK is less than 6.0 times/s, the function is considered to be impaired. There were other reports with a cut-off value of 4.0 times/s [17] or 5.0 times/s [18] to investigate the association between ODK and frailty. Although these cut-off values may be useful depending on the purpose, further studies are required to seek appropriate values of ODK.
ODK can be improved by implementing an oral function improvement program in which oral training exercises and oral care are continuously performed at home for about 3 months without using instruments [19]. Furthermore, the score of the repeated saliva swallowing test (RSST) of participants with decrease in swallowing function can be improved through the oral function improvement program as home exercise [19]. Thus, improving ODK by home exercise may contribute to prevent a slight decline in swallowing function among independent elderly.
Bacteria counts in tongue coat, oral wettability, tongue pressure, masticatory ability, bite force, number of present teeth, and number of functional teeth were not related to the suspected swallowing function. Surprisingly, we did not expect that factors related to mastication would be insignificant. If hard food is difficult to chew, the meal content or preparation can be changed so that it is easy to chew, such as chopping into smaller pieces or simmering until softened. Contrary to our results, previous studies reported that tongue pressure [20, 21], masticatory ability [22] and number of present teeth [23] were related to decreased swallowing function among dependent elderly or inpatients. The reason for this discrepancy may depend on the characteristics of the participants. Participants in the previous studies were dysphagia patients [20] or amyotrophic lateral sclerosis patients [21] whereas our participants were independent elderly with regular dental visits, and many of them had better oral function than those in the previous studies.
Each medicine for hypertension, hyperlipidemia, diabetes mellitus, kidney disease can cause dry mouth [24]. However, there was no significant association between these medicines and dry mouth in this study. Therefore, the effect of the medicine on our results may be small.
There are limitations in our study. Firstly, participants of this study were elderly who had regular dental visits at a single clinic. Those who received regular dental check-ups had better dental health behavior and a higher awareness of dental health than those who did not [25]. Because the condition of the oral cavity may have been better than the general population of elderly Japanese, selection bias is possible and caution should be exercised when generalizing the results. Secondly, items reported to be related to swallowing function include posture during eating [26], muscle strength throughout the body [27], social life function, cognitive function [28], and lip-closing force, but these were not considered in this study. Thirdly, this was a cross-sectional study and longitudinal studies are required to confirm the results.
Conclusion
Community-dwelling elderly Japanese who were suspected of having decreased swallowing function had lower oral function than those who did not, and the cut-off values were 71 years of age and ODK /pa/ sound of 6.2 times/s.
Availability of data and material
The anonymized data are available.
References
Pitts T (2014) Airway protective mechanism. Lung 192:27–31
Sasegbon A, Hamdy S (2017) The anatomy and physiology of normal and abnormal swallowing in oropharyngeal dysphagia. Neurogastroenterol Motil. https://doi.org/10.1111/nmo.13100
Pandolfino JE, Gawron AJ (2015) Achalasia: a systematic review. JAMA 313:1841–1852
Forti E, Bonato G, Dioscoridi L et al (2018) A smooth esophageal stricture causing dysphagia. Dysphagia 33:399–402
Kertscher B, Speyer R, Palmieri M et al (2014) Bedside screening to detect oropharyngeal dysphagia in patients with neurological disorders: an updated systematic review. Dysphagia 29:204–212
Takizawa C, Gemmell E, Kenworthy J et al (2016) A systematic review of the prevalence of oropharyngeal dysphagia in stroke, Parkinson’s disease, Alzheimer’s disease, head injury, and pneumonia. Dysphagia 31:434–441
Sura L, Madhavan A, Carnaby G et al (2012) Dysphagia in the elderly: management and nutritional considerations. Clin Interv Aging 7:287–298
Lorenzo-López L, Maseda A, Labra C et al (2017) Nutritional determinants of frailty in older adults: a systematic review. BMC Geriatr. https://doi.org/10.1186/s12877-017-0496-2
Iijima K (2015) Upstream preventive strategy for age-related sarcopenia in the elderly: why do the elderly fall into inadequate nutrition? Ann Jpn Prosthodont Soc 7:92–101 (Japanese)
Kera T, Kawai H, Yoshida H et al (2017) Classification of frailty using the Kihon checklist: a cluster analysis of older adults in urban areas. Geriatr Gerontol Int 17:69–77
Watanabe Y, Hirano H, Arai H et al (2017) Relationship between frailty and oral function in community-dwelling elderly adults. J Am Geriatr Soc 65:66–76
Japanese Society of Gerodontology Academic Committee (2016) Deterioration of oral function in the elderly the position paper from Japanese Society of Gerodontology in 2016. Jpn J Gerodontology 31:81–99 (Japanese)
Hara S, Miura H, Kawanishi K et al (2015) The relationship between articulation and probability of aspiration in the rural community-dwelling elderly. Jpn J Gerodontology 30:97–102 (Japanese)
Reddy NP, Costarella BR, Grotz RC et al (1990) Biomedical measurement to characterize the oral phase of dysphagia. IEEE Trans Biomed Eng 37:392–397
Cook IJ, Kahrilas PJ (1999) Aga technical review on management of oropharyngeal dysphagia. Gastroenterology 116:455–478
Belafsky PC, Mouadeb DA, Rees CJ et al (2008) Validity and reliability of the Eating Assessment Tool (EAT-10). Ann Otol Rhinol Laryngol 117:919–924
Matsuo K, Taniguchi H, Nakagawa K et al (2016) Relationships between deterioration of oral functions and nutritional status in elderly patients in an Acute Hospital. Jpn J Gerodontology 31:123–133 (Japanese)
Suzuki A, Kaneko H (2017) Relationship between voluntary cough intensity and the respiratory, physical, oral and swallowing functions of the community-dwelling elderly. J Phys Ther Sci 32:521–525 (Japanese)
Sakayori T, Maki Y, Hirata S et al (2013) Evaluation of a Japanese “Prevention of long-term care” project for the improvement in oral function in the high-risk elderly. Geriatr Gerontol Int 13:451–457
Aoki Y, Oota K (2014) The relationship between tongue pressure and swallowing function in dysphagic patients. Jpn J Dysphagia Rehabil 18:239–248 (Japanese)
Hiraoka A, Yoshikawa M, Nakamori M et al (2017) Maximum tongue pressure is associated with swallowing dysfunction in ALS patients. Dysphagia 32:542–547
Fukada J, Kamlakura Y, Kitake T (2002) Factors related to swallowing function of elderly persons living at home. Jpn J Dysphagia Rehabil 6:38–48 (Japanese)
Okamoto N, Morikawa M, Komatsu M et al (2016) Relationship between loss of teeth and dysphagia, serum albumin, and all-cause mortality in independent elderly-Fujiwara-kyo study. Pre Symptomatic Med Anti Aging 25:28–33 (Japanese)
Tan ECK, Lexomboon D, Sandborgh-Englund G et al (2018) Medicines that cause dry mouth as an adverse effect in older people: a systematic review and meta-analysis. J Am Geriatr Soc 66:76–84
Ando A, Kishi M, Aizawa F et al (2003) The relationship between regular dental check-up and oral health behavior. J Dent Health 53:3–7 (Japanese)
Tanoue H, Ohta K, Kokubo A et al (2008) The influence of a change of posture on swallowing function-change of swallowing function with posture of neck, trunk and lower limbs. Jpn J Dysphagia Rehabil 12:207–213 (Japanese)
Nishiyama K, Sugimoto R, Ebisumoto K et al (2014) A clinical study of the relationship between the swallowing function and physical strength. Deglutition 3:67–74 (Japanese)
Yamaguchi S, Wakayama N, Hideka K et al (2017) Influence of cognitive function on swallowing function. J Jpn Bronchoesophagol Soc 65:441–446 (Japanese)
Acknowledgements
The authors specially thank all participants of the study.
Funding
This work was supported by Japan Society for the Promotion of Science, JSPS KAKENHI grant number 17K12046 and 17H04421.
Author information
Authors and Affiliations
Contributions
NT and MM designed the study, and wrote the initial draft of the manuscript. NT and DE contributed to analysis and interpretation of data, and assisted in the preparation of the manuscript. NS have contributed to data collection. All authors have approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
The study protocol was approved by the Ethics Committee of the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences (No. 1708-028).
Informed consent
All participants provided written informed consent for study participation.
Consent for publication
I confirm that all authors agree with publication in the journal.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Takeuchi, N., Sawada, N., Ekuni, D. et al. Oral diadochokinesis is related to decline in swallowing function among community-dwelling Japanese elderly: a cross-sectional study. Aging Clin Exp Res 33, 399–405 (2021). https://doi.org/10.1007/s40520-020-01547-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-020-01547-7