
Abstract
Purpose
Hand grip strength (HGS) can predict physical function in next year when it is positively associated with nutritional and health status. This study aimed to determine the relationship between the healthy eating index (HEI)-2015 and hand grip strength.
Methods
This cross-sectional study was conducted on data from 4010 participants in the Ravansar non-communicable disease (RaNCD) cohort study. HGS was measured using a hand-held hydraulic hand grip dynamometer. HEI-2015 was calculated using data from the food frequency questionnaire.
Results
The mean of total HEI-2015 score was significantly higher in participants with an optimal HGS than in participants with a weak HGS (P = 0.006). Higher adherence to healthy eating was associated with optimal muscle strength (OR 1.26; CI 95% 1.02–1.62). This association was remained after being adjusted for potential confounders (P = 0.01). Among the HEI-2015 components, we only found association between whole fruit, added sugar, and HGS (P = 0.01, 0.019).
Conclusions
Our findings indicated that adherence to HEI-2015 could promote muscle strength. Among the HEI-2015 components, higher intake of whole fruit and lower adherence to added sugar had significantly positive effects on HGS.
Level of evidence
Level V, descriptive cross-sectional study.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hand grip strength (HGS) is defined as the total flexor muscles strength versus palmar muscles as well as extensor muscles, playing a secondary role in this contraction [1]. Evidence suggests that increased muscle strength is associated with improving health and reducing non-communicable diseases (NCDs) such as cardiovascular disease, diabetes, and overall mortality [2, 3]. In addition, poor muscle strength can increase the risk of fall, fractures, and disability in the years to come [4]. HGS is a simple, reliable, and noninvasive tool applied in many epidemiological studies to measure muscle strength [5, 6] and can predict overall muscle strength [1]. Inappropriate lifestyle such as sedentary behaviors and adherence to unhealthy dietary can accelerate the process of low muscle mass and strength [6, 7].
Healthy eating index (HEI) is developed to assess diet quality based on the Dietary Guidelines for Americans (DGA) that is updated every 5 years [8]. HEI-2015 emphasizes adequacy and moderation. Components of adequacy part include total fruits, whole fruits, total vegetables, greens and beans, whole grains, dairy, total protein foods, seafood and plant proteins, and fatty acids, and the other part emphasizes the limitation of the consumption of refined grains, sodium, added sugars, and saturated fats [9]. Adherence to a Mediterranean diet as a healthy diet can strengthen muscle strength [6, 10]. This dietary pattern is associated with high intake of whole grains, fruits, vegetables, nuts, legumes, olive oil, low-fat dairy, moderate consumption of poultry and fish, and low consumption of red meat, processed meat, and sweets [6]. Additionally, a Nordic diet with low intake of added sugar, dietary fat, and high fiber intake and sea foods has protective effects on muscle strength and mobility [4, 10]. To the best of our knowledge, there is no any study on HEI-2015 and muscle strength. Since recognition and screening of the muscle status and nutritional quality of the community are important to prevent NCDs, this study aimed to assess HEI-2015 and muscle strength in the Ravansar non-communicable diseases (RaNCDs) cohort study.
Methods
Study design and population
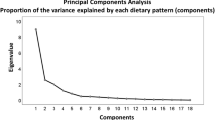
This cross-sectional study was conducted using the baseline data from the RaNCD cohort study. Since 2014, this study is the first Kurdish population-based study on 10,059 Kurdish participants aged 35–65 years living in Ravansar city, Kermanshah province, Western Iran. The RaNCD is one of 18 studies developed by the PERSIAN (Prospective Epidemiological Research Studies in Iran) mega-cohort study that was approved by the Ethics Committees in the Ministry of Health and Medical Education, the Digestive Diseases Research Institute, Tehran University of Medical Sciences, Iran. The protocol of the RaNCD cohort study was described in previous studies [11, 12]. The cohort study was given ethical approval by the Ethics Committee of Kermanshah University of Medical Sciences (ethics approval number: KUMS.REC.1394.318).
In the current study, we included the participants with an available dynamometry status at the baseline. Owing to loss of muscle mass in CVDs [13], cancer [14], and thyroid disorders [15, 16], we did not include participants with these disease as well as participants with pregnancy. Furthermore, the participants consuming energy intake less than 800 kcal/day and more than 4200 kcal/day were considered under and over energy intake reporter, respectively; therefore, they were not included in this study. Fourteen participants, who did not have complete information to calculate the HEI, were excluded from the study (Fig. 1).

Flowchart of the study
Data collection
We included the demographic data, anthropometric indices, nutritional assessments, and HGS measurement collected by well-trained interviewers in the study site in Ravansar.
Anthropometric indices
In the RaNCD cohort study, height was measured by the automatic stadiometer BSM 370 (Biospace Co., Seoul, Korea) in a standing position without shoes and with the precision of 0.1 cm. Weight was measured using the InBody 770 device (InBody Co, Seoul, Korea) with at least clothing and without shoes. Body mass index (BMI) was calculated by dividing the weight (kg) by the square of the height (meter).
Hand grip strength
HGS was determined using a hand-held hydraulic hand grip dynamometer (model SH5003; Saehan Corporation, Masan, Korea). Calibration of this dynamometer was carried out according to the manufacturers’ manual. The measurement was taken with the dominant hand when the participant was sitting and the elbow was at 90º of flexion. The participant was asked to squeeze the handle with maximal effort for 10 s. The measurement was repeated after 30 s, and the latter was recorded as hand grip strength. Based on the guidelines of this device, we considered optimal and weak muscle strength for each age group and gender [17].
Dietary assessment and Healthy eating index 2015
A total of the 130-item food frequency questionnaire was completed to assess dietary intake in the previous year that consisted of ten parts as follows: bread and grains, beans, meat and its products, dairies, vegetables, fruits, oils, oilseeds and butter, added sugar, and spices. The validity and reliability of this questionnaire were assessed in previous studies [18]. We obtained the dietary information of this questionnaire and then calculated HEI-2015, based on the last revised HEI available in the Department of Agriculture, Center for Nutrition Policy and Promotion [19]. This index has two sections: adequacy and moderation. The adequacy was related to the adequate intake of total fruits, whole fruits, total vegetables, greens and beans, whole grains, dairies, total protein foods, seafood and plant proteins, and fatty acids. Moderation intake of refined grains, sodium, added sugars, and saturated fats was evaluated using this index (Table 1).
Statistical analysis
Statistical analyses were conducted using Stata, version 14 (Stata Corp, College Station, TX). All quantitative variables were presented as mean ± standard deviation. Qualitative variables were reported using frequency (%). Comparison of baseline characteristics was assessed according to the HEI-2015 quartiles using ANOVA and Chi-square tests. In addition, comparison of components of HEI-2015 between participants with weak and optimal muscle strength was made using the ANOVA test. Radar graphs were constructed using the Excel software (Microsoft Office 2010) to show difference in the obtained score of HEI-2015 components between participants with weak and optimal muscle strength. Binary logistic regression was used in crude and adjusted models. In adjusted Model 1, we controlled the variables of age, gender, smoking, and alcohol use. Furthermore, in adjusted Model 2, in addition to the variables of Model 1, we controlled the variables of physical activity and diabetes. First, the quartile of HEI-2015 was considered the reference category in all binary logistic regression analyses. P-values were considered significant at the level of < 0.05.
Results
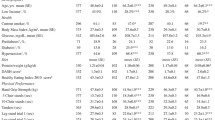
In the current study, the mean of total HEI-2015 score was significantly higher in participants with an optimal HGS than in participants with a weak HGS (P = 0.006) (Table 1). In addition, the mean of HGS was significantly increased with the increase in the HEI-2015 score (P < 0.001). Table 2 presents the baseline characteristics according to HEI-2015 quintiles.
Our findings indicated that higher adherence to healthy eating was associated with optimal muscle strength (OR 1.26; CI 95% 1.02–1.62). This association was remained after being adjusted for potential confounders (P = 0.01) (Table 3).
Although totally all HEI-2015 components were higher than in participants with an optimal HGS than in participants with a weak HGS, this difference was only significant for whole fruit and added sugar components.
In this study, we found that higher intake of whole fruits was associated with an optimal HGS (OR 1.01; CI 95% 1.02–1.18). In addition, participants who consumed less added sugar had an optimal HGS (OR 1.06; CI 95% 1.01–1.12) (Table 4).
Discussion
This study highlights that higher adherence to healthy eating is associated with an optimal HGS. Epidemiological studies have indicated that proper nutrition can prevent the progression of frailty during aging, which is characterized by a low HGS [6, 7]. Since low muscle strength is associated with decreased physical function [20], increased fractures [21], worsening cardiometabolic status [3], and all-cause mortality [22], identification of dietary components is an effective strategy to prevent low muscle strength. To the best of our knowledge, this study is the first study evaluating HEI-2015 and its components using HGS.
Stress oxidative and inflammation contribute to development of low muscle strength and its subsequence frailty [23, 24]. The HEI-2015 confirms an adequate intake of fruits, vegetables, whole grain, seafood, plant protein, dairy, and essential fatty acid. In addition, consumption of refined grain, added sugar, sodium, and saturated fatty acid should be moderate [8]. Fruits and vegetables are high in antioxidants and play a key role in systemic inflammation [25]. Furthermore, omega-3 fatty acid had beneficial effects on decreasing inflammation [26]. Dairy products, sea food, and plant protein spatially soy protein can promote muscle strength and muscle mass [27,28,29]. Moreover, dairy products are rich in high biological value protein and important minerals, including calcium and phosphorus [30]. In addition to high biological value protein, seafood can provide omega-3 fatty acid, contributing to reduction in inflammation [31, 32].
Among the HEI-2015 components, higher adherence to whole fruits intake was related to better muscle strength. In the components, all fruits were considered without fruits juice. In one study by Barrea et al. [6], fruits consumption more than three times per day in women was associated with a better HGS. The higher intake of fruits as a component of the Mediterranean diet had positive effects on muscle strength and fat-free mass [33,34,35]. Lima Ribeiro et al. [36] indicated that intake of the fruits juice worsened muscle strength. Fruits are rich in vitamins having anti-oxidative and anti-inflammatory effects. They can also prevent muscle atrophy owing to the effect of fruits on the gut microbiota in animal models [33, 37].
In this study, the other component contributing to calculation of HEI-2015 was added sugar in which its lower intake was associated with optimal muscle strength. In animal models, no change in strength was shown after drinking sugar-sweetened beverages [38]. Cameron et al. [39] did not observe any association between dietary carbohydrates and fat-free mass; however, high protein intake can predict high fat-free mass. Additionally, Hashemi et al. did not find any association between adherence Western diet and sarcopenia; in this case, Western diet was introduced by high sugar, fat, desserts, and fast food [40]. Since reduction in simple carbohydrates intake is accompanied by an increase in the intake of complex carbohydrates and proteins to provide energy, it seems that this relationship was owing to an increase in intake of complex carbohydrates, not necessarily a decrease in added sugar intake.
This study had several limitations; HEI-2015 was calculated based on FFQ. Although it is considered an appropriate nutritional assessment tool in large epidemiological studies, it can be affected by the recall bias. Furthermore, this study design was cross sectional in which a causal relationship maybe is inferred.
In conclusion, our findings indicated that adherence to HEI-2015 could enhance muscle strength. Although the score of all HEI-2015 components was higher in participants with an optimal HGS than in participants with a weak HGS, these associations were significant only between two HEI-2015 components (including whole fruits and added sugar) and HGS. Therefore, these results reflect that higher adherence to HEI-2015, especially adequate intake of whole fruits and moderation intake of added sugar, is an appropriate strategy to improve muscle strength.
What is already known on this subject?
Over 80% of the study participants had poor muscle strength. Previous studies have shown that weak muscle strength is associated with decreased mobility, increased fractures, and increased risk of cardiometabolic diseases. Identification and screening of nutritional factors affecting muscle strength can play a crucial role in muscle strength improvement.
What does this study add?
The study findings indicated that adherence to the HEI-2015 guidelines enhanced HGS, especially an adequate intake of whole fruits and a moderation intake of added sugar.
Availability of data and materials
Data will be available upon request from the corresponding author.
References
de Lima TR, Silva DAS, de Castro JAC, Christofaro DGD (2017) Handgrip strength and associated sociodemographic and lifestyle factors: a systematic review of the adult population. J Bodyw Mov Ther 21(2):401–413. https://doi.org/10.1016/j.jbmt.2016.08.017
Li JJ, Wittert GA, Vincent A, Atlantis E, Shi Z, Appleton SL, Hill CL, Jenkins AJ, Januszewski AS, Adams RJ (2016) Muscle grip strength predicts incident type 2 diabetes: population-based cohort study. Metabolism 65(6):883–892. https://doi.org/10.1016/j.metabol.2016.03.011
Peterson MD, Zhang P, Saltarelli WA, Visich PS, Gordon PM (2016) Low muscle strength thresholds for the detection of cardiometabolic risk in adolescents. Am J Prev Med 50(5):593–599. https://doi.org/10.1016/j.amepre.2015.09.019
Perälä M-M, von Bonsdorff MB, Männistö S, Salonen MK, Simonen M, Kanerva N, Rantanen T, Pohjolainen P, Eriksson JG (2017) The healthy Nordic diet predicts muscle strength 10 years later in old women, but not old men. Age Ageing 46(4):588–594. https://doi.org/10.1093/ageing/afx034
Wakayo T, Belachew T, Whiting SJ (2018) Serum vitamin D level associates with handgrip muscle strength among Ethiopian schoolchildren: a cross-sectional study. Food Nutr Bullet 39(1):54–64. https://doi.org/10.1177/0379572117724545
Barrea L, Muscogiuri G, Di Somma C, Tramontano G, De Luca V, Illario M, Colao A, Savastano S (2019) Association between Mediterranean diet and hand grip strength in older adult women. Clin Nutr 38(2):721–729. https://doi.org/10.1016/j.clnu.2018.03.012
Bruce S (2017) Healthy diet and better muscle function and quality in older women. Oxford University Press, Oxford. https://doi.org/10.1093/ageing/afx036
Krebs-Smith SM, Pannucci TE, Subar AF, Kirkpatrick SI, Lerman JL, Tooze JA, Wilson MM, Reedy J (2018) Update of the healthy eating index: HEI-2015. J Acad Nutr Diet 118(9):1591–1602. https://doi.org/10.1016/j.jand.2018.05.021
Panizza C, Shvetsov Y, Harmon B, Wilkens L, Le Marchand L, Haiman C, Reedy J, Boushey C (2018) Testing the predictive validity of the healthy eating index-2015 in the multiethnic cohort: is the score associated with a reduced risk of all-cause and cause-specific mortality? Nutrients 10(4):452. https://doi.org/10.3390/nu10040452
Perälä M-M, von Bonsdorff MB, Männistö S, Salonen MK, Simonen M, Pohjolainen P et al (2019) The healthy nordic diet and mediterranean diet and incidence of disability 10 years later in home-dwelling old adults. J Am Med Dir Assoc 20(5):511-5.e1. https://doi.org/10.1016/j.jamda.2018.09.001
Pasdar Y, Najafi F, Moradinazar M, Shakiba E, Karim H, Hamzeh B, Nelson M, Dobson A (2019) Cohort profile: Ravansar non-communicable disease cohort study: the first cohort study in a Kurdish population. Inter J Epidemiol. https://doi.org/10.1093/ije/dyy296
Poustchi H, Eghtesad S, Kamangar F, Etemadi A, Keshtkar A-A, Hekmatdoost A, Mohammadi Z, Mahmoudi Z, Shayanrad A, Roozafzai F (2017) Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): rationale, objectives, and design. Amer J Epidemiol 187(4):647–655. https://doi.org/10.1093/aje/kwx314
Lipkin DP, Jones DA, Round JM, Poole-Wilson PA (1988) Abnormalities of skeletal muscle in patients with chronic heart failure. Int J Cardiol 18(2):187–195. https://doi.org/10.1016/0167-5273(88)90164-7
Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL et al (2011) Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 12(5):489–495. https://doi.org/10.1016/S1470-2045(10)70218-7
Brennan MD, Powell C, Kaufman KR, Sun PC, Bahn RS, Nair KS (2006) The impact of overt and subclinical hyperthyroidism on skeletal muscle. Thyroid 16(4):375–380. https://doi.org/10.1089/thy.2006.16.375
Reuters VS, Patrícia de Fátima ST, Vigário PS, Almeida CP, Buescu A, Ferreira MM et al (2009) Functional capacity and muscular abnormalities in subclinical hypothyroidism. Am J Med Sci 338(4):259–263. https://doi.org/10.1097/MAJ.0b013e3181af7c7c
Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Rogers S (1985) Grip and pinch strength: normative data for adults. Arch Phys Med Rehabil 66(2):69–74
Moradi S, Pasdar Y, Hamzeh B, Najafi F, Nachvak SM, Mostafai R, Niazi P, Rezaei M (2018) Comparison of 3 nutritional questionnaires to determine energy intake accuracy in Iranian adults. Clin Nutr Res 7(3):213–222. https://doi.org/10.7762/cnr.2018.7.3.213
SOURCES: Data—National Center for Health Statistics WWEiANHaNES, 2013-2014. Healthy Eating Index-2015, Scores—U.S. Department of Agriculture, Center for Nutrition Policy and Promotion
Xu B, Houston DK, Locher JL, Ellison KJ, Gropper S, Buys DR, Zizza CA (2011) Higher Healthy Eating Index-2005 scores are associated with better physical performance. J Gerontol A Biol Sci Med Sci 67(1):93–99. https://doi.org/10.1093/gerona/glr159
Selakovic I, Dubljanin-Raspopovic E, Markovic-Denic L, Marusic V, Cirkovic A, Kadija M, Tomanovic-Vujadinovic S, Tulic G (2019) Can early assessment of hand grip strength in older hip fracture patients predict functional outcome? PLoS ONE 14(8):e0213223. https://doi.org/10.1371/journal.pone.0213223
Lera L, Albala C, Leyton B, Márquez C, Angel B, Saguez R, Sánchez H (2018) Reference values of hand-grip dynamometry and the relationship between low strength and mortality in older Chileans. Clin Interv Aging 13:317. https://doi.org/10.2147/CIA.S152946
Can B, Kara O, Kizilarslanoglu MC, Arik G, Aycicek GS, Sumer F, Civelek R, Demirtas C, Ulger Z (2017) Serum markers of inflammation and oxidative stress in sarcopenia. Aging Clin Exp Res 29(4):745–752. https://doi.org/10.1007/s40520-016-0626-2
Namioka N, Hanyu H, Hirose D, Hatanaka H, Sato T, Shimizu S (2017) Oxidative stress and inflammation are associated with physical frailty in patients with Alzheimer’s disease. Geriatr Gerontol Int 17(6):913–918. https://doi.org/10.1111/ggi.12804
Almeida-de-Souza J, Santos R, Lopes L, Abreu S, Moreira C, Padrão P, Mota J, Moreira P (2018) Associations between fruit and vegetable variety and low-grade inflammation in Portuguese adolescents from LabMed Physical Activity Study. Euro J Nutr 57(6):2055–2068. https://doi.org/10.1007/s00394-017-1479-y
Buoite Stella A, Gortan Cappellari G, Barazzoni R, Zanetti M (2018) Update on the impact of omega 3 fatty acids on inflammation, insulin resistance and sarcopenia: a review. Int J Mol Sci 19(1):218. https://doi.org/10.3390/ijms19010218
Hanach NI, McCullough F, Avery A (2019) The impact of dairy protein intake on muscle mass, muscle strength, and physical performance in middle-aged to older adults with or without existing sarcopenia: a systematic review and meta-analysis. Adv Nutr 10(1):59–69. https://doi.org/10.1093/advances/nmy065
Fernandes L (2016) Fish intake and strength in the elderly. In: Fish and fish oil in health and disease prevention. Elsevier, pp 137–142. https://doi.org/10.1016/B978-0-12-802844-5.00011-7
Thomson RL, Brinkworth GD, Noakes M, Buckley JD (2016) Muscle strength gains during resistance exercise training are attenuated with soy compared with dairy or usual protein intake in older adults: a randomized controlled trial. Clin Nutr 35(1):27–33. https://doi.org/10.1016/j.clnu.2015.01.018
Bridge A, Brown J, Snider H, Nasato M, Ward WE, Roy BD, Josse AR (2019) Greek yogurt and 12 weeks of exercise training on strength, muscle thickness and body composition in lean, untrained, University-Aged Males. Frontier Nutr. https://doi.org/10.3389/fnut.2019.00055
Gray SR, Mittendorfer B (2018) Fish oil-derived n-3 polyunsaturated fatty acids for the prevention and treatment of sarcopenia. Curr Opin Clin Nutr Metab Care 21(2):104–109. https://doi.org/10.1097/MCO.0000000000000441
Smith GI, Julliand S, Reeds DN, Sinacore DR, Klein S, Mittendorfer B (2015) Fish oil–derived n − 3 PUFA therapy increases muscle mass and function in healthy older adults. Am J Clin Nutr 102(1):115–122. https://doi.org/10.3945/ajcn.114.105833
Kelaiditi E, Jennings A, Steves C, Skinner J, Cassidy A, MacGregor A, Welch A (2016) Measurements of skeletal muscle mass and power are positively related to a Mediterranean dietary pattern in women. Osteoporos Int 27(11):3251–3260. https://doi.org/10.1007/s00198-016-3665-9
Samadi M, Moradi S, Moradinazar M, Mostafai R, Pasdar Y (2019) Dietary pattern in relation to the risk of Alzheimer’s disease: a systematic review. Neurol Sci. https://doi.org/10.1007/s10072-019-03976-3
Pasdar Y, Moradi S, Moludi J, Darbandi M, Niazi P, Nachvak SM, Abdollahzad H (2019) Risk of metabolic syndrome in non-alcoholic fatty liver disease patients. Med J Nutr Metabol. https://doi.org/10.3233/MNM-190290
Ribeiro SML, Morley J, Malmstrom T, Miller D (2016) Fruit and vegetable intake and physical activity as predictors of disability risk factors in African-American middle-aged individuals. J Nutr Health Aging 20(9):891–896. https://doi.org/10.1007/s12603-016-0780-4
Pasdar Y, Hamzeh B, Moludi J, Mehaki B, Darbandi M, Moradi S (2019) Dietary intake and risk of depression among male and female with HIV/AIDS. Eat Weight Disord. https://doi.org/10.1007/s40519-019-00726-4
Tsanzi E, Light HR, Tou JC (2008) The effect of feeding different sugar-sweetened beverages to growing female Sprague-Dawley rats on bone mass and strength. Bone 42(5):960–968. https://doi.org/10.1016/j.bone.2008.01.020
Cameron JD, Sigal RJ, Kenny GP, Alberga AS, Prud’homme D, Phillips P, Doucette S, Goldfield G (2016) Body composition and energy intake—skeletal muscle mass is the strongest predictor of food intake in obese adolescents: the HEARTY trial. Appl Physiol Nutr Metab 41(6):611–617. https://doi.org/10.1139/apnm-2015-0479
Hashemi R, Motlagh AD, Heshmat R, Esmaillzadeh A, Payab M, Yousefinia M, Siassi F, Pasalar P, Baygi F (2015) Diet and its relationship to sarcopenia in community dwelling Iranian elderly: a cross sectional study. Nutrition 31(1):97–104. https://doi.org/10.1016/j.nut.2014.05.003
Acknowledgments
RaNCD is part of PERSIAN national cohort, and we would like to thank Professor Reza Malekzadeh, Deputy of Research and Technology at the Ministry of Health and Medical Education of Iran and Director of the PERSIAN cohort, and also Dr. Hossein Poustchi Executive Director of PERSIAN cohort for all their supports during design and running of RaNCD.
Funding
This study was supported by Ministry of Health and Medical Education of Iran and Kermanshah University of Medical Science (Grant No: 92472).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Committee of Kermanshah University of Medical Sciences (ethics approval number: KUMS.REC.1394.318).
Informed consent
Written informed consent was obtained from each studied subject after explaining the purpose of the study. The right of subjects to withdraw from the study at any time and subjects information is reserved and will not be published.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Pasdar, Y., Moradi, S., Moradinazar, M. et al. Better muscle strength with healthy eating. Eat Weight Disord 26, 367–374 (2021). https://doi.org/10.1007/s40519-020-00863-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-00863-1