
Abstract
Functional communication training (FCT) typically consists of determining the function(s) of challenging behaviors and teaching the child an appropriate communicative behavior that serves the same function. This review used quality indicators to evaluate FCT studies and determine the level of evidence for children with autism spectrum disorder (ASD) from birth to 8. Based on the authors’ evaluation of six studies located from a previous review, FCT showed potential as an evidence-based practice. After evaluating nine more studies located from literature searches, a moderate level of evidence was established for FCT for children with ASD from birth to 8. Implications for research and practice are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Children with autism spectrum disorder (ASD) often have severe deficits in social, language, and communication skills (American Psychiatric Association 2013). According to Centers for Disease Control and Prevention (CDC), 1 in 59 children is identified with ASD (CDC 2014). A study suggested 25.6% of individuals with ASD have difficulty in communicating (National Longitudinal Transition Study 2 2009). Additionally, a more recent study found 30% of children with ASD may never develop fluent speech (Wodka et al. 2013). Researchers continue to find a strong relation between the lack of communication skills and the presence of challenging behaviors (Kaiser et al. 2002; Park et al. 2012). In other words, children who do not have a functional system of communication are more likely to exhibit challenging behaviors as means of communicating their needs and wants (Chiang 2008).
Challenging behaviors must be a treatment priority (O’Reilly et al. 2010) as they can impede the child from learning and social integration in school and community (Sigafoos et al. 2003). One way to address challenging behaviors in children with ASD is functional communication training (FCT, Carr and Durand 1985). FCT is a behavioral intervention based on differential reinforcement procedures that consists of two steps: (a) assessing the communicative function(s) of the child’s challenging behavior(s), and (b) teaching the child an appropriate communicative response that results in accessing the same reinforcer maintaining the challenging behavior (Carr and Durand 1985). Functional behavior assessments (FBAs) can be used to determine the maintaining variables (e.g., access to attention, tangible, escape from demands) of the challenging behaviors (Cooper et al. 2007). These assessments include interviews with teachers and caregivers, direct observations, and systematic functional analyses (Brady and Halle 1997). After assessing the function(s) of the challenging behavior through FBAs, a communicative response is chosen for the child. The new response has to be easy for the child to learn, produce the same consequences as quickly as the challenging behavior, and easily noticed by communicative partner(s) (Dunlap and Duda 2004). The communicative response could be through an unaided system such as manual signs, spoken words, or an aided system such as picture exchange (PE; e.g., Frea et al. 2001), picture exchange communication system (PECS; Frost and Bondy 2002), and speech-generating devices such as iPads (e.g., Muharib et al. in press). The new communicative response is taught to the child as an alternative to his or her challenging behavior (Carr and Durand 1985).
Identification of the empirical support for interventions targeting children with ASD from birth to age 8 is crucial as federal laws require the implementation of evidence-based practices (EBPs) for students with developmental disabilities (Individuals with Disabilities Education Improvement Act [IDEIA] 2004; No Child Left Behind [NCLB] 2001). Kurtz et al. (2011) evaluated the extent to which FCT is an evidence-based practice for individuals with intellectual disabilities (ID) from birth to 18 years. They used American Psychological Association (APA) criteria with adaptations developed by Jennett and Hagopian (2008) to evaluate 29 studies published between 1985 and 2009. Criteria included a clear description of participants, independent variables, and dependent variables, a demonstration of experimental control, and a demonstration of treatment efficacy. Using those criteria, the authors indicated that FCT was a well-established practice for individuals with ID from birth through 18 years.
In a more recent review, Andzik et al. (2016) evaluated whether FCT is a practice that could be implemented with fidelity by practitioners. Andzik et al. evaluated 12 single-case studies published through 2015 that targeted individuals with developmental disabilities from 3 to 18 years. The Council for Exceptional Children (CEC 2014) criteria were used to assess the quality of the included studies. These criteria were related to descriptions of participants and setting(s), interventionist, dependent variable(s), treatment fidelity, internal validity, outcomes of the dependent variables, and data analysis. FCT was found to be a practice that could generally be implemented effectively by practitioners. However, none of the 12 studies met all the quality indicators developed by CEC (2014).
Wong et al. (2013) conducted a review of 27 practices for individuals with ASD. Of these practices, FCT was evaluated for individuals with ASD from birth to 22 years. They evaluated studies published between 1990 and 2011. Wong et al. indicated that FCT was an evidence-based practice for children and youth with ASD based on Horner et al.’s (2005) indicators and the selected criteria from What Works Clearinghouse ([WWC]; Kratochwill et al. 2010).
Communication skills are critical in a child’s development (Kaiser and Roberts 2011). Early intervention in communication skills (e.g., FCT) is often a priority and can greatly impact children with ASD and their families (American Academy of Pediatrics 2007; Landa 2007; Lorah and Parnell 2017; National Research Council 2001; Tager-Flusberg and Kasari 2013). Previous reviews of FCT evaluated studies with a broader age range of students with ASD or other developmental disabilities (birth to age 18, Kurtz et al. 2011; birth to age 21, Wong et al. 2013; ages 3 to 18, Andzik et al. 2016); therefore, the extent to which FCT is an evidence-based practice for a smaller age range of children and younger students with ASD remains unclear.
Since communication is critical for young children, the purpose of this review was twofold: (a) to evaluate the studies reviewed by Wong et al. (2013) that targeted children with ASD from 0 to 8 years, and (b) to evaluate recent studies conducted on the use of FCT that targeted children with ASD from 0 to 8 years. This range of ages was chosen based on the definition of young children provided by the CEC’s Division for Early Childhood (Division for Early Childhood [n.d.]). Thus, the research questions were:
-
(a)
What level of evidence does functional communication training as a practice have based on studies reviewed by Wong et al. (2013) that targeted children with ASD from birth to age 8?
-
(b)
What level of evidence does functional communication training as a practice have based on reviewing additional studies that targeted children with ASD from birth to age 8?
Method
Article Selection
Article selection was conducted in three steps. First, the authors located all studies on FCT in the Wong et al.’s (2013) review, published between 1990 and 2011, that targeted children with ASD ages 0–8. This process yielded a total of six studies.
Second, the authors did an independent search of studies on FCT that targeted children with ASD ages 0–8 published between 1990 and 2011 to ensure that they were no studies overlooked in Wong et al.’s (2013) review. The authors used Google Scholar, Academic Search Complete, Academic Search Premier, Education Research Complete, ERIC, PsycINFO, and the Psychology and Behavioral Sciences Collection databases. While Wong et al. (2013) used comprehensive search terms (e.g., treatment, therapy, package) to locate studies for 27 different practices, search terms used for this review were specific to only FCT. The search terms were functional communication training, functional communication, functional analysis communication, differential reinforcement of alternative, autism, and autism spectrum disorder.
Third, another independent search was conducted for articles published between 2012 and 2017 using Google Scholar, Academic Search Complete, Academic Search Premier, Education Research Complete, ERIC, PsycINFO, and the Psychology and Behavioral Sciences Collection databases. The search terms were functional communication training, functional communication, functional analysis communication, differential reinforcement of alternative, autism, and autism spectrum disorder. The authors also reviewed the reference lists of the included studies as well as past reviews (Kurtz et al. 2011; Andzik et al. 2016) to further find other relevant studies.
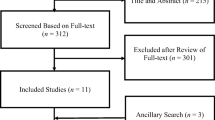
The independent searches, completed in January 2018, yielded 12,827 articles (12,799 articles from the second step, and 28 articles from the third step of the selection process). Abstracts were initially reviewed to determine whether the studies met the inclusion criteria: (a) used a single-case experimental design, (b) employed FCT as an intervention, (c) targeted children ages 0–8 years that exhibited challenging behaviors that were either aggressive (e.g., hitting), self-injurious (e.g., head banging), and/or disruptive (e.g., crying), and (d) children were diagnosed with autism spectrum disorder (ASD), Asperger syndrome, pervasive developmental disorder (PDD), or pervasive developmental disorder-not otherwise specified (PDD-NOS). If participants were diagnosed with a co-occurring condition (e.g., intellectual disability, Rett syndrome), the study was included. In cases where the abstract did not state the ages, disability, and challenging behaviors of participants, the authors read the participant description in the method section. When the abstract did not clearly describe the intervention as FCT, the authors read the independent variable(s) in the method section to determine whether the intervention was FCT. FCT was operationally defined as determining the function(s) of the challenging behavior by using at least one functional behavior assessment, and teaching the child an alternative communicative response that matched the function(s) of the challenging behavior (Carr and Durand 1985).
A study was excluded if (a) it did not include participants with ASD, (b) it included participants with ASD but all were older than 8 years, (c) participants received FCT to replace prelinguistic behaviors (e.g., pointing, reaching), (d) it employed FCT in a combination with other practices, (e) it was not published in a peer-reviewed journal, or (f) it was not a single-case study. Out of the 12,827 articles found, nine met the inclusion criteria (three studies from 1990 to 2011, and six studies from 2012 to 2017). The interrater agreement for the selection process was calculated point-by-point (i.e., applying the selection procedure and yielding the same studies) by dividing the number of agreements by the number of agreement and disagreements multiplied by 100. The agreement for the study selection was 100%.
Coding Procedure
The authors used Horner et al.’s (2005) quality indicators to evaluate the 15 studies (six studies located from Wong et al. (2013), and nine studies from independent searches). The definition of each quality indicator can be found in Table 1. The coding procedures consisted of two steps: (a) the first author independently evaluated the quality of each of the six studies located from Wong et al.’s (2013) review using the 21-item quality indicator criteria developed by Horner et al. (2005), and (b) the first author independently evaluated the quality of the nine studies found from the independent literature searches using the same quality indicator criteria. These quality indicators were used due to the level of rigor compared to other indicators of single-case studies (e.g., Council for Exceptional Children 2014; WWC, Kratochwill et al. 2010). These quality indicators pertained to (a) participants, (b) setting, (c) dependent measures, (d) intervention, (e) procedures, (f) internal validity, (g) external validity, and (h) social validity. In evaluating each study, dichotomous decisions were made in terms of whether a quality indicator was present or absent (see Table 2).
After evaluating all studies, the level of evidence of FCT was determined. The authors determined the evidence of FCT twice: (a) after evaluating the six studies included from Wong et al.’s study, and (b) after evaluating the nine studies added from independent literature searches. The authors evaluated the evidence of FCT twice because they sought to find out whether the results of a large-scale review (i.e., Wong et al. 2013) could have a strong level of evidence when the age of participants was restricted to children from birth to 8.
The authors used the levels of evidence provided by National Technical Assistance Center on Transition ([NTACT]; Test et al. 2009). As opposed to the standards proposed by Horner et al. (2005) which classify a practice as either evidence-based or not evidence-based, NTACT standards allow for classifying a practice into one of three levels: strong, moderate, or potential. Adopted from NTACT, strong evidence was established if the practice had five high-quality studies, conducted by three different groups of researchers in three different geographical locations, demonstrated functional relations, and showed no contradictory results. Moderate evidence was established if the practice had three high-quality studies, data showed functional relations, were conducted by one or two different groups of researchers, and showed no contradictory results. Potential evidence was established if the practice had two high-quality studies, data showed functional relations, were conducted by one or two different groups of researchers, and showed no contradictory results. A high-quality study had to meet all the quality indicators from 1 to 17, and three out of the four indicators related to social validity (i.e., 18, 19, and 21). In this review, original criteria have been altered as it was not expected for every study to report on cost-effectiveness of intervention (indicator 20). For a study to meet a certain quality indicator, it had to meet the definition of the quality indicator as shown in Table 1.
Interrater Agreement
Interrater agreement data were collected on a total of five randomly selected studies (33%) from both groups of studies (i.e., previously reviewed studies by Wong et al. (2013), and studies added from independent searches). The second rater (second author) coded each study independently applying the same quality indicator criteria developed by Horner et al. (2005). The authors then compared each independently coded study item-by-item to record their agreements and disagreements. The interrater agreement was calculated item-by-item using the formula of number of agreements divided by number of agreements plus disagreement multiplied by 100. Interrater agreement across all five randomly interrated studies was 100%.
Results
Table 3 provides a summary of study characteristics in terms of age of participants, settings, intervention agents, type of functional behavior assessments, and experimental designs in each of the 15 reviewed studies. The 15 studies provided an FCT intervention to a total of 29 participants ages 2 to 8. Sixty-three percent of the studies included children between 3 and 5 years old, 36% included children between 6 and 8 years old, and 1% included children between birth and 2 years old. Forty-percent of the studies were conducted in clinical settings while the remaining were conducted in more natural settings such as school (33%), home (20%), or a combination of the two to facilitate generalization (7%).
Over half the studies were implemented by a therapist or researcher (60%). On the other hand, 40% of studies were conducted by typical interventionists such as teachers, teaching assistants, and parents. Studies that involved coaching typical interventionists on the implementation of FCT in natural settings also reported results of the fidelity of the implementation by these interventionists with the exception of Sigafoos and Meikle’s (1996) study. Overall, typical interventionists were able to implement FCT with fidelity. Parents were able to master fidelity at 93 to 100% (Olive et al. 2008; Schindler and Horner 2005; Simacek et al. 2017), and teachers/teaching assistants were able to master fidelity of implementation of FCT at 90 to 100% (Gibson et al. 2010; Schindler and Horner 2005). Interestingly, while the majority of studies conducted in natural settings reported results on procedural fidelity, none of the studies conducted in clinical settings reported results on procedural fidelity (Betz et al. 2013; Falcomata et al. 2010, 2013; Fisher et al. 2015; Greer et al. 2016; Mancil et al. 2006; Volkert et al. 2009).
In terms of behavioral assessments, the vast majority of the studies (87%) conducted functional analysis alone or combined with other procedures to assess the functions of participants’ challenging behaviors. In studies where functional analysis was combined with other forms of behavioral assessments, functional analyses were conducted subsequent to observations and/or interviews. For example, Simacek et al. (2017) conducted interviews with caregivers and observations during free play. Subsequently, a functional analysis verified the results obtained from the interviews and observations. Functional analyses were conducted by a researcher/therapist in eight studies (53%). In five studies, parents and teachers were coached to conduct functional analyses (33%). In four studies (27%), parents and teachers conducted functional analyses with fidelity (Gibson et al. 2010; Olive et al. 2008; Simacek et al. 2017; Suess et al. 2014). In Sigafoos and Meikle’s (1996) study, a teacher conducted FAs. However, the researchers reported no data on the fidelity of implementation. Functional analyses were not conducted in two studies (13%). Braithwaite and Richdale (2000) conducted antecedent-behavior-consequences observations and interviews with teachers. Schindler and Horner (2005) only conducted interviews with teachers to determine the function(s) of the target behaviors.
In addition, studies in this review were conducted using several single-case designs. Forty-seven percent used a multiple baseline/multiple probe design, 33% used a reversal design, 7% used a multi-element design, and 13% of studies used two designs combined such as multiple baseline with embedded reversal design.
Evaluation of Previously Reviewed Studies
A total of six studies located from Wong et al.’s (2013) review met the inclusion criteria. All these studies employed FCT as an intervention for children with ASD between 4 and 8 years old who displayed challenging behaviors. Only two studies met all 21 quality indicators developed by Horner et al. (2005) (Olive et al. 2008; Schindler and Horner 2005). The other four studies failed to meet at least one quality indicator related to treatment fidelity, external validity, and/or social validity. For instance, three studies (Falcomata et al. 2010; Mancil et al. 2006; Volkert et al. 2009) did not include measures of procedural fidelity. One study did not replicate the intervention effects across participants, conditions, or settings (Gibson et al. 2010). In addition, two out of the six studies did not meet the three quality indicators pertaining to social validity (Falcomata et al. 2010; Volkert et al. 2009).
Based on the application of quality indicators for single-case research (Horner et al. 2005), two studies demonstrated a high level of quality (Olive et al. 2008; Schindler and Horner 2005). It is worth noting that all the six studies were conducted by independent groups of researchers and showed functional relations. However, as only two studies met all quality indictors from 1 to 17, and the three indicators pertaining to social validity (indicators 18, 19, and 21), a potential level of evidence was established for FCT for children with ASD based on the studies located from the review by Wong et al. (2013).
Evaluation of Additional Studies
Nine additional studies were evaluated to explore whether stronger empirical support existed for the use of FCT for children with ASD. FCT was used as a treatment procedure in all the nine studies for children with ASD between 2 and 8 years old who displayed challenging behaviors. None of the studies met all 21 quality indicators developed by Horner et al. (2005). However, one study met the quality indicators from 1 to 17 and the three indicators on the social validity measures (Simacek et al. 2017). This study reflected a high level of quality. On the other hand, four studies did not demonstrate a high level of quality because they did not report data on procedural fidelity, and did not meet the three quality indicators pertaining to social validity (Betz et al. 2013; Falcomata et al. 2013; Fisher et al. 2015; Greer et al. 2016). Additional four studies (Braithwaite and Richdale 2000; Franco et al. 2009; Sigafoos and Meikle 1996; Suess et al. 2014) failed to meet three or more quality indicators such as describing the participants with sufficient detail (Braithwaite and Richdale 2000), describing the intervention with replicable precision (Franco et al. 2009), and establishing a design control for threats of internal validity (Suess et al. 2014).
As stated previously, one study reflected a high level of quality based on the quality indicators applied. Based on the evaluation of this study (Simacek et al. 2017) as well as the previous two high-quality studies (Olive et al. 2008; Schindler and Horner 2005) located from Wong et al. (2013), a moderate level of evidence was established for FCT treatment for children with ASD.
Discussion
The purpose of this review was to determine the quality of research and level of evidence for FCT use with children with ASD. After evaluating 15 studies both from Wong et al.’s (2013) review and independent literature searches, a moderate level of evidence was established for FCT for children 0–8 years old with ASD. This is consistent with previous reviews (e.g., Kurtz et al. 2011; Wong et al. 2013). However, our data suggest there still is a need for more research to bring the evidence level of FCT for children with ASD from moderate to strong. This can be achieved by reporting data on procedural fidelity and describing the participants and intervention procedures in a replicable manner. Additionally, the finding of this review adds to the body of literature as it supports the use of FCT specifically for children with ASD from 0 to 8 years. Another finding was that parents and teachers can successfully implement FCT with children with ASD at home and school (Gibson et al. 2010; Olive et al. 2008; Schindler and Horner 2005; Simacek et al. 2017; Suess et al. 2014).
A limitation to this review should be taken into consideration. Horner et al. (2005) recommended 21 quality indicator criteria for high-quality single-case research. However, these criteria have been adapted in this review so that a study had to meet 17 indicators and three indicators related to social validity to be considered as high quality. The authors altered the criteria as it was not expected for each study to have a report on the cost-effectiveness of intervention. However, future evidence-based practice reviews should consider applying all 21 indicators to evaluate practices for children with ASD.
Other suggestions for future research examining practices for children with ASD include the need for having teachers or paraprofessionals serve as interventionists. Based on this review, only three studies (Gibson et al. 2010; Schindler and Horner 2005; Sigafoos and Meikle 1996) were implemented by teachers. Andzik et al. (2016) found practitioners could effectively implement FCT with children with developmental disabilities from 3 to 18 years old. Therefore, future research should evaluate FCT studies to determine whether FCT can be effectively implemented by practitioners working with children with ASD from birth to 8 years old.
In addition, future research investigating FCT and other practices for children with ASD should measure procedural fidelity. Sixty-seven percent of the studies reviewed did not provide data on procedural fidelity. Providing such data adds to the credibility of the results and enhances the quality of single-case research. Without data on procedural fidelity, conclusions about the effects of intervention may be questionable as there are no data to determine the extent in which the intervention procedures were followed and whether the intervention procedures were responsible for the behavior change.
Although studies that collected procedural fidelity data suggested parents and teachers can implement FCT with fidelity (e.g., Gibson et al. 2010; Olive et al. 2008), only one study—in which a teacher was the interventionist—reported data on maintenance (Sigafoos and Meikle 1996). The data showed that the teacher continued to use FCT and that challenging behaviors of children remained at a zero level. Nevertheless, Sigafoos and Meikle (1996), as previously discussed, did not report data on fidelity. Thus, additional studies are needed to examine the extent to which parents and teachers can continue to use FCT with fidelity over time.
An implication for practice drawn from this review is the need to include FCT procedures in professional development trainings provided for practitioners working with children with ASD from birth to 8 years old. Although three studies only were implemented by teachers in this review, teachers were able to implement FCT procedures with ease and fidelity. Teachers also expressed their satisfaction with FCT as it improved the challenging behaviors of targeted children with ASD (Gibson et al. 2010; Schindler and Horner 2005).
Virtual videoconferencing such as telehealth has been used as a service-delivery mechanism to coach parents on the implementation of FCT at home (Gibson et al. 2010; Simacek et al. 2017; Suess et al. 2014). This mechanism may be a viable option to address the shortage of professionals trained in ASD (Wise et al. 2010). Such technology may also serve families who live in remote rural areas (Simacek et al. 2017). As parents have shown that they can implement FCT with fidelity when provided coaching (Olive et al. 2008; Simacek et al. 2017; Suess et al. 2014; Wacker et al. 2011), professionals should coach parents on how to implement FCT at home. Videoconferencing could be one mechanism to conduct coaching.
The findings of this review showed parents and teachers alike can benefit from coaching to implement functional analysis and FCT with fidelity. Whether coaching was provided face-to-face or virtually, researchers employed similar strategies to deliver training to parents or teachers. The strategies included modeling, role-play, and descriptive feedback (e.g., Gibson et al. 2010).
Because this review intended to evaluate FCT as a stand-alone intervention, it included studies that examined FCT only. However, it is noteworthy that procedures involving thin schedules of reinforcement may be necessary. After the child has acquired and maintained the functional communication response, teaching the child to tolerate delay of reinforcement may be important. In natural situations, a specific reinforcer that the child is requesting (e.g., asking to watch a favorite cartoon in the lunchroom) may not be available in the environment. Thus, teaching the child to wait for reinforcement may come as a next step to FCT (e.g., Falcomata et al. 2012).
While this review was not intended to be a meta-analysis, a meta-analytic procedure may be conducted in future research to evaluate whether FCT combined with specific components (e.g., FCT with response blocking) result in different effect sizes for children with ASD ages 0 to 8.
FCT has been researched since 1985 when it was first introduced by Carr and Durand. This review evaluated FCT studies to determine the level of evidence for its use with children with ASD from birth to 8. After evaluating 15 studies, FCT was established as a practice with a moderate level of evidence for children with ASD. Thus, more research is still needed to establish a strong level of evidence to support FCT as an evidence-based practice for children with ASD ages 0 to 8.
References
American Academy of Pediatrics. (2007). Management of children with autism spectrum disorder. Pediatrics, 120, 1162–1182. https://doi.org/10.1542/peds.2007-2362.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington: American Psychiatric Publishing.
Andzik, N. R., Cannella-Malone, H. I., & Sigafoos, J. (2016). Practitioner-implemented functional communication training: A review of the literature. Research and Practice for Persons with Severe Disabilities, 41, 79–89. https://doi.org/10.1177/1540796916633874.
Betz, A. M., Fisher, W. W., Roane, H. S., Mintz, J. C., & Owen, T. M. (2013). A component analysis of schedule thinning during functional communication training. Journal of Applied Behavior Analysis, 46, 219–241.
Brady, N. C., & Halle, J. W. (1997). Functional analysis of communicative behaviors. Focus on Autism and Other Developmental Disabilities, 12, 95–104.
Braithwaite, K. L., & Richdale, A. M. (2000). Functional communication training to replace challenging behaviors across two behavioral outcomes. Behavioral Interventions, 15, 21–36.
Carr, E. G., & Durand, V. M. (1985). Reducing problem behaviors through functional communication training. Journal of Applied Behavior Analysis, 18, 111–126.
Centers for Disease Control and Prevention. (2014). CDC estimates 1 in 68 children has been identified with autism spectrum disorder. Retrieved from https://www.cdc.gov/media/releases/2014/p0327-autism-spectrum-disorder.html.
Chiang, H. M. (2008). Expressive communication of children with autism: The use of challenging behaviour. Journal of Intellectual Disability Research, 52(11), 966–972.
Cooper, J. O., Heron, T. E., & Heward, W. L. (2007). Applied behavior analysis (2nd ed.). Upper Saddle River: Merrill.
Council for Exceptional Children. (2014). Council for exceptional children standards for evidence-based practices in special education. Retrieved from http://www.cec.sped.org/~/media/Files/Standards/Evidence%20based%20 Practices%20and%20Practice/CECs%20Evidence%20Based%20Practice%20Standards.pdf.
Division for Early Childhood. (n.d.). Retrieved from http://www.dec-sped.org/.
Dunlap, G., & Duda, M. (2004). Using functional communication training to replace challenging behavior. What works brief. Retrieved from http://csefel.vanderbilt.edu/briefs/wwb11.pdf.
Falcomata, T. S., Roane, H. S., Feeney, B. J., & Stephenson, K. M. (2010). Assessment and treatment of elopement maintained by access to stereotypy. Journal of Applied Behavior Analysis, 43(3), 513–517. https://doi.org/10.1901/jaba.2010.43-513.
Falcomata, T. S., Roana, H. S., Muething, C. S., Stephenson, K. M., & Ing, A. D. (2012). Functional communication training and chained schedules of reinforcement to treat challenging behavior maintained by terminations of activity interruptions. Behavior Modification, 36, 630–649. https://doi.org/10.1177/0145445511433821.
Falcomata, T. S., Wacker, D. P., Ringdahl, J. E., Vinquist, K., & Dutt, A. (2013). An evaluation of generalization of mands during functional communication training. Journal of Applied Behavior Analysis, 46, 444–454.
Fisher, W. W., Greer, B. D., Fuhrman, A. M., & Querim, A. C. (2015). Using multiple schedules during functional communication training to promote rapid transfer of treatment effects. Journal of Applied Behavior Analysis, 48, 713–733.
Franco, J. H., Lang, R. L., O’Reilly, M. F., Chang, J. M., Sigafoos, J., & Rispoli, M. (2009). Functional analysis and treatment of inappropriate vocalizations using a speech-generating device for a child with autism. Focus on Autism and Other Developmental Disabilities, 24, 146–155.
Frea, W. D., Arnold, C. L., & Vittimberga, G. L. (2001). A demonstration of the effects of augmentative communication on the extreme aggressive behavior of a child with autism within an integrated preschool setting. Journal of Positive Behavior Interventions, 3, 194–198. https://doi.org/10.1177/109830070100300401.
Frost, L., & Bondy, A. (2002). Picture exchange communication system training manual (2nd ed.). Newark: Pyramid Education Products.
Gibson, J. L., Pennington, R. C., Stenhoff, D. M., & Hopper, J. S. (2010). Using desktop videoconferencing to deliver interventions to a preschool student with autism. Topics in Early Childhood Special Education, 29, 214–225. https://doi.org/10.1177/0271121409352873.
Greer, B. D., Fisher, W. W., Saini, V., Ownes, T. M., & Jones, J. K. (2016). Functional communication training during reinforcement schedule thinning: An analysis of 25 applications. Journal of Applied Behavior Analysis, 49, 105–121.
Horner, R., Carr, E., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The use of single subject research to identify evidence-based practice in special education. Exceptional Children, 71, 165–180.
Individuals with Disabilities Education Improvement Act of 2004, 20 U.S.C. § 1400 et seq. (2004) (reauthorization of the Individuals with Disabilities Education Act of 1990).
Jennett, H. K., & Hagopian, L. P. (2008). Identifying empirically supported treatments for phobic avoidance in individuals with intellectual disabilities. Behavior Therapy, 39, 151–161.
Kaiser, A. P., & Roberts, M. Y. (2011). Advances in early communication and language intervention. Journal of Early Intervention, 33, 298–309.
Kaiser, A. P., Cai, X., Hancock, T. B., & Foster, E. M. (2002). Teacher reported behavior problems and language delays in boy and girls enrolled in head start. Behavioral Disorders, 28, 23–39.
Kratochwill, T. R., Hitchcock, J., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M & Shadish, W. R. (2010). Single-case designs technical documentation. Retrieved from What Works Clearinghouse website: http://ies.ed.gov/ncee/wwc/pdf/wwc_scd.pdf.
Kurtz, P. F., Boelter, E. W., Jarmolowicz, D. P., Chin, M. D., & Hagopian, L. P. (2011). An analysis of functional communication training as an empirically supported treatment for problem behavior displayed by individuals with intellectual disabilities. Research in Developmental Disabilities, 32, 2935–2942. https://doi.org/10.1016/j.ridd.2011.05.009.
Landa, R. (2007). Early communication development and intervention for children with autism. Mental Retardation and Developmental Disabilities Research Reviews, 13, 16–25.
Lorah, E. R., & Parnell, A. (2017). Acquisition of tacting using a speech-generating device in group learning environments for preschoolers with autism. Journal of Developmental and Physical Disabilities, 29, 597–609. https://doi.org/10.1007/s10882-017-9543-3.
Mancil, G. R., Conroy, M. A., Nakao, T., & Alter, P. J. (2006). Functional communication training in the natural environment: A pilot investigation with a young child with autism spectrum disorder. Education and Treatment of Children, 29, 615–633.
Muharib, R., Correa, V. I., Wood, C. L., & Haughney, K. L. (in press). Effects of functional communication training using GoTalk Now iPad application on challenging behavior of children with autism spectrum disorder. Journal of Special Education Technology.
National Longitudinal Transition Study 2: Wave 5. (2009). Retrieved from https://nlts2.sri.com/data_tables/tables/14/np5B5bfrm.html.
National Research Council. (2001). Educating children with autism. Washington, DC: National Academy Press.
No Child Left Behind (NCLB) Act of 2001, 20 U.S.C.A. § 6301 et seq.
O’Reilly, M., Rispoli, M., Davis, T., Machalicek, W., Lang, R., Sigafoos, J., … Didden, R. (2010). Functional analysis of challenging behavior in children with autism spectrum disorders: A summary of 10 cases. Research in Autism Spectrum Disorders, 4, 1–10.
Olive, M. L., Lang, R. B., & Davis, T. N. (2008). An analysis of the effects of functional communication and a voice output communication aid for a child with autism spectrum disorder. Research in Autism Spectrum Disorders, 2, 223–236. https://doi.org/10.1016/j.rasd.2007.06.002.
Park, C., Yelland, G., Taffe, J., & Gray, K. (2012). Brief report: The relationship between language skills, adaptive behavior, and emotional and behavior problems in preschoolers with autism. Journal of Autism and Developmental Disorders, 42, 2761–2766. https://doi.org/10.1007/s10803-012-1534-8.
Schindler, H. R., & Horner, R. H. (2005). Generalized reduction of problem behavior of young children with autism: Building trans-situational interventions. American Journal on Mental Retardation, 110, 36–47.
Sigafoos, J., & Meikle, B. (1996). Functional communication training for the treatment of multiply determined challenging behavior in two boys with autism. Behavior Modification, 20, 60–84.
Sigafoos, J., Arthur, M., & O’Reilly, M. (2003). Challenging behavior and developmental disability. London: Whurr Publishers.
Simacek, J., Dimian, A. F., & McComas, J. J. (2017). Communication intervention for young children with severe neurodevelopmental disabilities via telehealth. Journal of Autism and Developmental Disorders, 47, 744–767. https://doi.org/10.1007/s10803-016-3006-z.
Suess, A. N., Romani, P. W., Wacker, D. P., Dyson, S. M., Kuhle, J. L., Lee, J. F., … & Waldron, D. B. (2014). Evaluating the treatment fidelity of parents who conduct in-home functional communication raining with coaching via telehealth. Journal of Behavioral Education, 23, 34–59, doi:https://doi.org/10.1007/s10864-013-9183-3.
Tager-Flusberg, H., & Kasari, C. (2013). Minimally verbal school-aged children with autism spectrum disorder: The neglected end of the spectrum. Autism Research, 6(6), 468–478.
Test, D. W., Fowler, C. H., Richter, S. M., White, J., Mazzotti, V, Walker, A. R., … & Kortering, L. (2009). Evidence based practices in secondary transition. Career Development for Exceptional Individuals, 32, 115–128.
Volkert, V. M., Lerman, D. C., Call, N. A., & Trosclair Lasserre, N. (2009). An evaluation of resurgence during treatment with functional communication training. Journal of Applied Behavior Analysis, 42, 145–160. https://doi.org/10.1901/jaba.2009.42-145.
Wacker, D. P., Harding, J. W., Berg, W. K., Lee, J. F., Schieltz, K. M., Padilla, Y. C., … Shahan, T. A. (2011). An evaluation of persistence of treatment effects during long-term treatment of destructive behavior. Journal of the Experimental Analysis of Behavior, 96, 261–282. https://doi.org/10.1901/jeab.2011.96-261.
Wise, M. D., Little, A., Holliman, J. B., Wise, P. D., & Wang, C. J. (2010). Can state early intervention programs meet the increased demand of children suspected of having autism spectrum disorders? Journal of Developmental and Behavioral Pediatrics, 31, 469–476. https://doi.org/10.1097/DBP.0b013e3181e56db2.
Wodka, E. L., Mathy, P., & Kalb, L. (2013). Predictors of phrase and fluent speech in children with autism and severe language delay. Pediatrics, 131, 1128–1134.
Wong, C., Odom, S. L., Hume, K., Cox, A. W., Fettig, A., Kucharczyk, S., et al. (2013). Evidence-based practices for children, youth, and young adults with autism spectrum disorder. Chapel Hill: The University of North Carolina, Frank Porter Graham Child Development Institute, Autism Evidence-Based Practice Review Group.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights
This research involves no human or animal participants.
Rights and permissions
About this article

Cite this article
Muharib, R., Wood, C.L. Evaluation of the Empirical Support of Functional Communication Training for Children with Autism Spectrum Disorders. Rev J Autism Dev Disord 5, 360–369 (2018). https://doi.org/10.1007/s40489-018-0145-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40489-018-0145-5