
Abstract
Functional communication training (FCT) is one of the most common treatments for challenging behavior and is considered an empirically supported practice for children and adolescents with autism spectrum disorder (ASD). However, no previous systematic review has evaluated the quality of FCT for adults with ASD, and the empirical support for this practice among adults is unknown. The purpose of the current review was to synthesize the extant research, including a quality appraisal of the literature on the use of FCT to treat challenging behavior for adults with ASD. We identified 20 studies that evaluated the efficacy of FCT in reducing challenging behavior for adults with ASD. The quality of each article was evaluated based on the What Works Clearinghouse design and evidence standards. Following the quality and evidence evaluations, eight studies, including eight experiments, were found to have moderate or strong evidence of effectiveness. The current body of literature provides some evidence for the efficacy of FCT in reducing challenging behavior for adults with ASD, but additional research in this area is warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Individuals diagnosed with autism spectrum disorder (ASD) are more likely to engage in challenging behavior than individuals diagnosed with other intellectual or developmental disabilities (IDD; Holden and Gitlesen 2006; Matson and Rivet 2008; McClintock et al. 2003). Challenging behavior is chronic and often persists into and throughout adulthood (Holden and Gitlesen 2006; Matson and Rivet 2008). However, due to limited financial resources, inadequate staff training, and a paucity of research-supported interventions (Manente et al. 2010; Sullivan 2007), adults with ASD have access to fewer services than children with ASD (Turcotte et al. 2016). Without adequate intervention, challenging behavior is unlikely to improve. Adults with IDD, including ASD, who engage in challenging behavior are prone to social isolation, seclusion from the community, and have an overall lower quality of life (Emerson et al. 2000; Gerber et al. 2011; Holden and Gitlesen 2006). In addition, individuals with challenging behavior are more likely to be served in restrictive settings, prone to injury, and treated with restrictive interventions (Cooper et al. 2007; Yang 2003).
However, previous research has shown that adults with IDD, including ASD, who receive treatment for challenging behavior based on the principles of behavior analysis can experience reductions in challenging behavior and improvements in quality of life (Gerber et al. 2011). Functional communication training (FCT) is one of the most researched function-based behavioral interventions for the treatment of challenging behavior (Tiger et al. 2008). Within FCT, a functional behavior assessment (FBA) is conducted to determine the variable(s) maintaining challenging behavior (Carr and Durand 1985). Next, the individual is taught an appropriate communicative response that produces the same reinforcer(s) as the challenging behavior (Carr and Durand 1985).
The quality and empirical support for FCT have been evaluated in a number of systematic and quality reviews (Chezan et al. (2018); Gerow et al. 2018a; Heath et al. 2015; Wong et al. 2014). In a recent review, Gerow et al. (2018a) evaluated the FCT literature to determine the strength of evidence across 13 disability categories using the What Works Clearinghouse (WWC) standards. Of the 216 studies included in the review, FCT resulted in a decrease in challenging behavior for 136 participants indicating that FCT meets standards to be considered an evidence-based practice for individuals with ASD, intellectual disability, other health impairment, and multiple disabilities. The review conducted by Gerow et al. (2018a) represents the most comprehensive review of the FCT literature to date. However, similar to other systematic and quality reviews concerning FCT, data on the quality and characteristics of individual treatment studies for adults with ASD were not disaggregated from the broader FCT literature. Thus, less is known about the empirical support for FCT specifically for adults with ASD.
Evaluating the empirical support for behavioral interventions for adults with ASD is critically important. While the number of adolescents with ASD approaching adulthood continues to rise, the number of research-supported interventions for this population is limited (Howlin and Moss 2012). It has been suggested that the lack of evidence-based practices may contribute to poorer outcomes for this population (Gerhardt and Lainer 2011). Given the efficacy of FCT and the paucity of research on empirically supported practices for adults with ASD, there is a need for a research synthesis of FCT for this population. Thus, the purpose of the current review was to evaluate the quality and evidence of FCT for adults with ASD using the WWC design and evidence standards. Additionally, we sought to summarize the characteristics of the available high-quality research to identify areas of future research and implications for practitioners. Specifically, we addressed the following two research questions:
- 1.
What is the available research evidence on FCT for adults with ASD?
- 2.
What are the characteristics of treatment studies that met the WWC quality and evidence standards?
Method
Article Identification
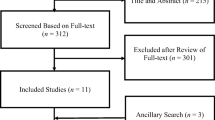
In October of 2018, a systematic search was conducted in two electronic databases, ERIC and PsychINFO using the search terms “functional communication training” and “functional equivalence training.” The initial database search yielded 483 articles. Duplicates were removed, and the remaining 400 articles were evaluated against a set of nine inclusion criteria. To be included in the present review, studies had to meet the following criteria: (a) include at least one participant with ASD (including Rett syndrome, pervasive developmental disorder, autistic disorder, and Asperger syndrome); (b) include at least one participant 18 years or older; (c) implement FCT as the primary intervention, or a component of an intervention package; (d) report the effects of FCT on challenging behavior; (e) provide an original evaluation of FCT efficacy; (f) use experimental single-case or group design methodology; (g) display outcome data on a line graph (single-case experimental studies only); (h) be published in a peer-reviewed journal; and (i) be published in English. Studies that did not disaggregate FCT data from other intervention components (excluding extinction and response blocking) were excluded from the present review. Each article was scored as 1 (yes) or 0 (no) for meeting all inclusion criteria. If an article failed to meet one or more of the inclusion criteria, it was given a score of 0 (no), indicating that it would not be included in the review. An ancestral search of the reference lists of the included studies was conducted to identify additional articles not captured during the database searches.
Additionally, hand searches of articles published online first were conducted in Behavioral Interventions, Journal of Positive Behavior Interventions, Journal of Autism and Developmental Disabilities, and Behavior Modification. A more extensive hand search of the Journal of Applied Behavior Analysis (all issues published between 2003 and 2018) was conducted, given that a majority of included studies were published in this outlet. From these searches, a total of 20 studies met inclusion for the current review.
Quality and Evidence Appraisal
The methodological quality of the 20 studies that met inclusion for this review was evaluated against the Basic Design Standards (DS) described by the WWC (Kratochwill et al 2010) and adapted by Maggin et al. (2013). The purpose of the design evaluation was to determine the methodological quality of each of the included studies. Two standards were adapted based on procedures described in previous quality reviews. DS 2B was adapted according to the procedures described by Hong et al. (2016). This modification requires that a study reports interobserver agreement (IOA) data on a minimum of 20% of data points per study phase (baseline and intervention). DS 3 was adapted based on the procedures described by Gerow et al. (2018a). The modification requires a minimum of three attempts to demonstrate an intervention effect between baseline and FCT phases (for reversal and multiple-baseline designs). For the purposes of this study, we defined baseline as a phase in which no treatment was in place. For alternating treatments and multielement designs, studies were required to demonstrate a minimum of three alterations between FCT and the other treatment(s). A more detailed description of the coding procedures is displayed in Table 1.
Studies that met the minimum quality thresholds as determined by the WWC advanced to the evidence evaluation. The purpose of the evidence evaluation was to determine the presence of a functional relation between FCT and challenging behavior, and the strength of that relation. Each study was coded using the procedures described by the WWC and Maggin et al. (2013). Specific coding procedures for the evidence evaluation are displayed in Table 2.
Descriptive Evaluation
Studies demonstrating high methodological quality may increase the believability that a functional relation was demonstrated between FCT and challenging behavior. Therefore, only methodologically sound studies that demonstrated moderate or strong evidence were coded for specific descriptive information. Data were extracted using a researcher-developed coding manual (available from the first author upon request). The manual contained 30 descriptive variables across 11 categories, totaling 240 coded items across studies. Categories included: (a) participant demographics, (b) intervention setting, (c) intervention agent, (d) FBA components, (e) operant function of challenging behavior, (f) mode of communication, (g) schedule thinning, (h) maintenance, (i) generalization, (j) treatment fidelity, and (k) social validity. Participant demographics consisted of seven variables including gender, age, race, primary diagnosis, secondary diagnosis, and tertiary diagnosis. Participant gender was coded as 1 (male) or 0 (female). The remaining five variables were coded descriptively based on author report. Variables included under the intervention setting, intervention agent, and FBA components categories were coded as either 1 (yes) or 0 (no).
Intervention setting was coded as natural or clinical. Natural settings were defined as settings the participant attended during his or her typical routines (e.g., home, school, place of employment). Intervention agent was coded as natural or researcher. Natural intervention agents were defined as individuals who interacted with the participant during his or her typical routines (e.g., direct support staff, teacher, caregiver). Interventionists described as a trainer or therapist were coded as researcher. Operant function of challenging behavior and mode of communication were coded descriptively based on author report. Variables in the schedule thinning category included delay schedules, chained schedules, multiple schedules, response restriction, or other and were scored as 1 (yes) or 0 (no). Variables in the remaining categories (i.e., maintenance, generalization, treatment fidelity) were coded as 1 (yes) or 0 (no).
Interrater Agreement
Inclusion Criteria
Second raters, two undergraduate students in Special Education and Speech-Language Pathology, independently scored each article against the inclusion criteria. Agreement was defined as both raters assigning the same score to an article. Disagreements were discussed until a consensus on the inclusion of the article was reached. The first author trained each rater on the rating procedures. Training was considered complete when each rater reached a minimum of 80% agreement with the first author across three consecutive articles. Initial agreement between raters was 97%. After disagreements were discussed, final agreement was 100%.
Quality and Evidence Evaluations
The first author read and coded each article against the quality and evidence appraisal rubrics. A second rater independently read and coded each article to achieve reliability. A faculty member in special education with experience conducting quality evaluations evaluated each article against the WWC standards. The second rater was trained by the first author on the scoring procedures using a researcher-developed training protocol (available from first author upon request). Three articles were randomly selected for training purposes. During training, the rater independently read and scored each article using a researcher-developed coding spreadsheet. Training was considered complete when the second rater reached at least 80% agreement with the first author across three articles. After training, the first author and the second rater evaluated the remaining 17 articles independently. Interrater agreement (IRA) was calculated as percentage agreement by dividing the number of agreements by the total number of coding variables and multiplying by 100. Training articles were not included in overall IRA scores. Mean IRA for the WWC DS and evidence standards was 86%, and 93%, respectively, before disagreements were discussed. After consensus on disagreements was reached, final agreement was 100% across appraisal rubrics.
Descriptive Evaluation
A second rater independently read and coded each article for specific descriptive information. IRA was calculated as percentage agreement by dividing the number of agreements by the number of agreements plus disagreements and multiplying by 100. Agreements were defined as instances when both raters provided the same score or description for each variable. When disagreement occurred, raters met to discuss discrepancies until consensus was reached. IRA was 91% before disagreements were discussed. After reaching consensus on disagreements, IRA was 100%.
Results
Twenty studies were included for review and evaluated against the WWC design and evidence standards. In this section, we present the results of the quality and evidence evaluations and provide a descriptive summary of the studies that demonstrated evidence of a strong or moderate effect based on the WWC evidence standards.
Quality Evaluation
The results of the quality evaluation are presented with respect to the WWC’s descriptions of evaluation procedures. Results of the design evaluation are displayed in Table 3.
Design Standard 1
All 20 studies systematically manipulated the independent variable and met DS 1.
Design Standard 2
All 20 studies reported IOA data (DS 2A). Four studies (20%) reported IOA data for at least 20% of data points per study phase, and 14 studies (70%) reported collecting IOA data on at least an average of 20% of data points across all study phases (DS 2B). The remaining two studies (10%) did not report the percentage of sessions in which IOA data were collected and did not meet DS 2B. All 20 studies reported adequate IOA (i.e., ≥ 80%; DS 2C). Overall, 18 (90%) studies met DS 2 with or without reservations.
Design Standard 3
Twelve studies (60%) met DS 3 and made at least three attempts to demonstrate an experimental effect at three different points in time between baseline and FCT phases.
Design Standard 4
Four studies (20%) met DS 4 without reservations, providing five or more data points per phase. Fourteen studies (70%) met DS 4 with reservations (i.e., at 3–4 data points per phase). Two studies (10%) included less than three data points in at least one study phase.
Overall
Overall, 10 studies (50%) met the Basic Design Standards. One study (5%) met standards without reservations, and nine studies (45%) met standards with reservations and were deemed high quality. Ten studies (50%) did not meet standards.
Evidence Evaluation
Studies that met the DS with or without reservations were evaluated against the WWC evidence standards. Results of the evidence evaluation are described below and displayed in Table 4.
Evidence Standards
The 10 studies that met the DS with or without reservations included a total of 12 experiments. Each experiment was evaluated against the WWC evidence standards. One study, including one experiment, was found to have strong evidence (Slaton et al. 2017). Seven studies, including seven experiments, were found to have moderate evidence of effectiveness (Adami et al. 2017; Byiers et al. 2014; Kunnavatana et al. 2018a, b; Lehardy et al. 2013; Lindauer et al. 2002; Rehfeldt and Chambers 2003), and four studies, including four experiments, were found to have no evidence of effectiveness (Byiers et al. 2014; Chezan et al. 2014; Fisher et al. 2000; Horner and Day 1991; Kunnavatana et al. 2018b). Two articles included in this review (Byiers et al. 2014; Kunnavatana et al. 2018a) contained two experiments. For both studies, one experiment received a score of moderate evidence of effectiveness, and another received a score of no evidence of effectiveness.
Descriptive Evaluation
Eight studies, including eight experiments, met the WWC evidence standards with moderate or strong evidence and were summarized across 11 categories of descriptive information. Results of the descriptive evaluation are described below and displayed in Table 5.
Participant Demographics
A total of eight participants were included across the eight studies (6 male; 2 female). In addition to ASD, four participants had additional diagnoses including intellectual disability, Lennox–Gastaut syndrome, and Landau–Kleffner syndrome. Ages of the participants ranged from 18 to 47 years, with most participant ages between 18 and 26 years (i.e., early adulthood). One study included a participant in middle adulthood (i.e., 40–60 years), and no studies included participants in late adulthood (i.e., 60 years or older).
Intervention Setting
FCT was implemented in a variety of settings across studies. While most of the settings were classified as natural (63%), many were congregate facilities that traditionally serve individuals with IDD (e.g., sheltered workshops, private schools, group homes, adult day programs).
Intervention Agent
All of the included studies utilized skilled research personnel as the primary intervention agent.
FBA Components
All eight studies reported conducting a pretreatment FBA. Six studies (75%) conducted traditional functional analyses (TFA) based on the procedures described by Iwata et al. (1994). Two studies (25%) exposed participants to variations of the TFA. Lehardy et al. (2013) modified TFA conditions to identify the function of elopement for a 26-year-old male. During test conditions, the assessment room was divided into two sections. Before all sessions, the participant was directed to stay on one side of the room. At the beginning of the session, the participant was given access to a preferred item for 30 s. The tangible item was then removed and placed on the opposite side of the room. If the participant eloped (i.e., moved to the other side of the room), he was given brief access to his preferred item. In addition to a TFA, Slaton et al. (2017) also conducted a variation of the TFA termed the interview-informed synthesized contingency analysis (IISCA; Hanley et al. 2014). Unlike a TFA in which reinforcement contingencies are evaluated in isolation (Fisher et al. 2016), the IISCA combines multiple reinforcement contingencies into an isolated test condition, which is compared against a matched control (Fisher et al. 2016; Hanley et al. 2014). During control conditions, each participant was given access to all putative reinforcers. In the test condition, all putative reinforcers were removed and reinstated contingent on challenging behavior. One study reported conducting a functional analysis prior to treatment but did not describe specific assessment procedures.
Operant Function of Challenging Behavior
The operant function of challenging behavior was identified for all eight participants. Tangibly maintained challenging behavior was reported most frequently across studies (37%). Escape from task demands and access to attention were reported as the function of challenging behavior in one study each (13%). Two studies (25%) reported multiply maintained challenging behavior in the form of access to attention and preferred leisure items or access to tangibles and escape from aversive activities. Based on the results of the IISCA, one study (13%) found that challenging behavior was sensitive to synthesized reinforcement contingencies in the form of escape from instructional demands to preferred items.
Mode of Communication
Card exchange and vocal responses were the most commonly reported modes of communication across studies (25% of studies each). Two studies (25%) reported speech-generating devices as the primary mode of communication. One study (13%) reported using a microswitch as the primary mode of communication, and one study reported multiple modes of communication.
Data on schedule thinning, maintenance, generalization, treatment fidelity, and social validity were not reported across any of the studies.
Discussion
The purposes of the current review were to evaluate the quality and evidence of the literature on FCT among adults with ASD and to summarize the studies meeting minimal methodological thresholds. Results of a quality and evidence appraisal identified eight studies, including eight experiments that demonstrated moderate or strong evidence of effectiveness for FCT. Major findings of the quality, evidence, and descriptive evaluations and future directions for research are discussed below.
Quality and Evidence Evaluations
Of the total 20 studies included in this review, 10 (50%) met the DS with or without reservations. The most common reason studies failed to meet standards was providing less than three demonstrations of experimental effect between baseline and FCT phases (DS 3). It is important to note that some of the included studies may not have met DS 3 as a result of the study’s primary research question (Campos et al. 2017; Horner and Day 1991; Tincani et al. 1999). For example, the purpose of the study by Campos et al. (2017) was to evaluate the effects of a multiple schedule on communication and challenging behavior within the context of FCT using a multiple-baseline design with an embedded reversal. In this case, experimental control was demonstrated between the various multiple schedule phases, rather than between baseline and intervention. Therefore, caution should be used when interpreting the methodological quality of these studies. Overall, the limited number of studies meeting basic methodological standards indicates an urgent need for more high-quality research examining the effects of FCT among adults with ASD.
The 10 studies that met the DS with or without reservations included a total of 12 experiments. Of those experiments, eight (67%) demonstrated moderate or strong evidence of effectiveness, indicating that FCT can be an effective treatment for challenging behavior among adults with ASD. The most common reason experiments were deemed as having moderate instead of strong evidence, was the number of data points included across phases. Of the eight experiments found to have evidence of moderate or strong effectiveness, seven included 3–4 data points per study phase, resulting in a score of moderate evidence of effectiveness. Overall, the majority of high-quality studies (67%) demonstrated the efficacy of FCT as a treatment of challenging behavior among adults with ASD.
Descriptive Evaluation Outcomes
The descriptive evaluation identified several important gaps within the current literature base. None of the included studies that demonstrated moderate or strong evidence of effectiveness included a natural change agent (e.g., direct service provider, teacher, parent) as the FCT interventionist. However, previous experimental studies and research syntheses have demonstrated the efficacy of natural change agent-implemented FCT (Andzik et al. 2016; Gerow et al. 2018b). Research on the efficacy of natural change agent-implemented FCT for adults is warranted, given that many service providers working with adults with ASD lack adequate training in behavior management (Mills and Rose 2011).
Although it has been shown to produce immediate effects, less research has examined maintenance and generalization of FCT (Falcomata and Wacker 2013; Neely et al. 2018). Of the eight studies that demonstrated moderate or strong evidence, none reported maintenance or generalization data. Therefore, the results of these studies should be interpreted within the context of immediate behavior change. Based on the available literature, we were unable to conclude that reductions in challenging behavior for adults with ASD would extend beyond the treatment conditions described in the included studies.
Directions for Future Research
The results of the current review identified several directions for future research. The studies that employed multiple-baseline designs included both child and adult participants. Although the mechanisms of FCT are consistent regardless of participant demographics, the effects of FCT have been shown to be different for children and adults (Heath et al. 2015). Adults have a longer history of challenging behavior that may be more resistant to extinction, which is a common component of FCT interventions (Heath et al. 2015). Therefore, more between-participant replications for adults with ASD are necessary to understand the differences in treatment outcomes for children and adults.
Of the initial 400 studies identified from the database searches, only 20 met inclusion for this review. This highlights a significant gap in the overall literature on FCT. Although the number of individuals with ASD approaching adulthood continues to rise, there remains a lack of empirically supported practices for this population (Sullivan 2007). Given that FCT is the most common and most empirically supported treatment for challenging behavior, there is a need for additional empirical evaluations of this procedure for adults with ASD.
Limitations
The current review has several limitations that should be noted. First, none of the authors of this review were certified reviewers by the WWC. Therefore, it is unclear whether our results would align with those of certified reviewers. Second, while the WWC standards permit systematic evaluation of internal validity, they do not include variables related to external validity (e.g., description of intervention agent, description of study procedures). Thus, the extent to which these variables influence the methodological quality of this literature base is unknown. Future studies should consider examining variables related to external validity for a more comprehensive evaluation of the literature concerning FCT as a treatment for challenging behavior among adults with ASD. Third, this review excluded studies that did not disaggregate FCT data from other treatment components (e.g., punishment, differential reinforcement of other behavior, choice), which limited the number of studies included in this review. Finally, the search terms used may have limited the number of studies obtained. It is possible that studies could have implemented FCT but used other terminology to describe the intervention (i.e., differential reinforcement of alternative behavior, DRA). Therefore, it is possible that articles which included a function-based differential reinforcement procedure were not included.
Conclusions and Implications for Practice
The findings of the current study align with previous reviews and demonstrate the efficacy of FCT as a treatment for challenging behavior among individuals with ASD (Chezan et al. 2018; Gerow et al. 2018a; Heath et al. 2015; Wong et al. 2014). Specifically, the high-quality literature identified in the current review indicates that FCT can be an effective treatment for challenging behavior among the population of adults with ASD. Although the limited number of participants included across studies demonstrates minimal external validity, the available evidence does demonstrate that FCT can be an effective treatment for a diverse group of adults with ASD.
First, the available evidence shows that FCT can be used to effectively treat all forms of socially maintained challenging behavior (i.e., escape, attention, and access tangibles). Second, the literature demonstrates FCT can be used for adults whose communicative repertoires vary in complexity. Studies included in this review taught the FCR using multiple modes of communication including verbal requests for participants who were verbal and high-tech AAC (e.g., SGD) and low-tech AAC (e.g., picture exchange) for participants who had complex communication needs. These findings indicate that FCT may be an effective treatment for adults with ASD who have varying levels of support needs. However, due to the paucity of high-quality research for this population, practitioners should closely monitor behavior change when implementing FCT as an intervention. Practitioners should also carefully evaluate fidelity of FCT implementation to make informed decisions regarding treatment choice.
In summary, there is some evidence to support the efficacy of FCT as a treatment for challenging behavior among adults with ASD. However, there is still a dearth of research for adults as the target population compared to the extensive literature involving FCT and young children with ASD. Additional research in this area is necessary for the continued identification of empirically supported practices for adults with ASD.
References
References marked with an asterisk indicate studies included in the review.
*Adami, S., Falcomata, T. S., Muething, C. S., & Hoffman, K. (2017). An evaluation of lag schedules of reinforcement during functional communication training: Effects on varied mand responding and challenging behavior. Behavior Analysis in Practice. https://doi.org/10.1007/s40617-017-0179-7.
Andzik, N. R., Cannella-Malone, H. I., & Sigafoos, J. (2016). Practitioner-implemented functional communication training: A review of the literature. Research and Practice for Persons with Severe Disabilities, 41(2), 79–89. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=eric&AN=EJ1099223&site=ehost-live
*Bird, F., Dores, P. A., Moniz, D., & Robinson, J. (1989). Reducing severe aggressive and self-injurious behaviors with functional communication training. American Journal on Mental Retardation,94(1), 37–48.
*Byiers, B. J., Dimian, A., & Symons, F. J. (2014). Functional communication training in Rett syndrome: A preliminary study. American Journal on Intellectual and Developmental Disabilities,119(4), 340–350. https://doi.org/10.1352/1944-7558-119.4.34.
*Campos, C., Leon, Y., Sleiman, A., & Urcuyo, B. (2017). Further evaluation of the use of multiple schedules for behavior maintained by negative reinforcement. Behavior Modification,41(2), 269–285. https://doi.org/10.1177/0145445516670838.
Carr, E. G., & Durand, V. M. (1985). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis,18(2), 111–126. https://doi.org/10.1901/jaba.1985.18-111.
*Chezan, L. C., Drasgow, E., & Martin, C. A. (2014). Discrete-trial functional analysis and functional communication training with three adults with intellectual disabilities and problem behavior. Journal of Behavioral Education,23(2), 221–246. https://doi.org/10.1007/s10864-013-9192-2.
Chezan, L. C., Wolfe, K., & Drasgow, E. (2018). A meta-analysis of functional communication training effects on problem behavior and alternative communicative responses. Focus on Autism and Other Developmental Disabilities,33(4), 195–205. https://doi.org/10.1177/1088357617741294.
Cooper, J. O., Heron, T. E., & Heward, W. L. (2007). Applied behavior analysis (2nd ed.). Upper Saddle River: Pearson.
Emerson, E., Robertson, J., Gregory, N., Hatton, C., Kessissoglou, S., Hallam, A., et al. (2000). Treatment and management of challenging behaviours in residential settings. Journal of Applied Research in Intellectual Disabilities,13(4), 197–215. https://doi.org/10.1046/j.1468-3148.2000.00036.x.
*Fahmie, T. A., Iwata, B. A., & Mead, S. C. (2016). Within-subject analysis of a prevention strategy for problem behavior. Journal of Applied Behavior Analysis,49(4), 915–926. https://doi.org/10.1002/jaba.343.
Falcomata, T. S., & Wacker, D. P. (2013). On the use of strategies for programming generalization during functional communication training: A review of the literature. Journal of Developmental and Physical Disabilities,25(1), 5–15. https://doi.org/10.1007/s10882-012-9311-3.
Fisher, W. W., Greer, B. D., Romani, P. W., Zangrillo, A. N., & Owen, T. M. (2016). Comparisons of synthesized and individual reinforcement contingencies during functional analysis. Journal of Applied Behavior Analysis,49(3), 596–616. https://doi.org/10.1002/jaba.314.
*Fisher, W. W., Thompson, R. H., Hagopian, L. P., Bowman, L. G., & Krug, A. (2000). Facilitating tolerance of delayed reinforcement during functional communication training. Behavior Modification,24(1), 3–29. https://doi.org/10.1177/0145445500241001.
Gerber, F., Bessero, S., Robbiani, B., Courvoisier, D. S., Baud, M. A., Traore, M., et al. (2011). Comparing residential programmes for adults with autism spectrum disorders and intellectual disability: Outcomes of challenging behaviour and quality of life. Journal of Intellectual Disability Research,55(9), 918–932. https://doi.org/10.1111/j.1365-2788.2011.01455.x.
Gerhardt, P. F., & Lainer, I. (2011). Addressing the needs of adolescents and adults with autism: A crisis on the horizon. Journal of Contemporary Psychotherapy,41(1), 37–45. https://doi.org/10.1007/s10879-010-9460-2.
Gerow, S., Davis, T., Radhakrishnan, S., Gregori, E., & Rivera, G. (2018a). Functional communication training: The strength of evidence across disabilities. Exceptional Children. https://doi.org/10.1177/0014402918793399.
Gerow, S., Hagan-Burke, S., Rispoli, M., Gregori, E., Mason, R., & Ninci, J. (2018b). A systematic review of parent-implemented functional communication training for children with ASD. Behavior Modification,42(3), 335–363. https://doi.org/10.1177/0145445517740872.
*Ghaemmaghami, M., Hanley, G. P., & Jessel, J. (2016). Contingencies promote delay tolerance. Journal of Applied Behavior Analysis,49(3), 548–575. https://doi.org/10.1002/jaba.333.
Hanley, G. P., Jin, C. S., Vanselow, N. R., & Hanratty, L. A. (2014). Producing meaningful improvements in problem behavior of children with autism via synthesized analyses and treatments. Journal of Applied Behavior Analysis,47(1), 16–36. https://doi.org/10.1002/jaba.106.
Heath, A. K., Ganz, J. B., Parker, R., Burke, M., & Ninci, J. (2015). A meta-analytic review of functional communication training across mode of communication, age, and disability. Review Journal of Autism and Developmental Disorders,2(2), 155–166. https://doi.org/10.1007/s40489-014-0044-3.
Holden, B., & Gitlesen, J. P. (2006). A total population study of challenging behaviour in the county of Hedmark, Norway: Prevalence, and risk markers. Research in Developmental Disabilities,27(4), 456–465. https://doi.org/10.1016/j.ridd.2005.06.001.
Hong, E. R., Ganz, J. B., Neely, L., Gerow, S., & Ninci, J. (2016). A review of the quality of primary caregiver-implemented communication intervention research for children with ASD. Research in Autism Spectrum Disorders,25, 122–136. https://doi.org/10.1016/j.rasd.2016.02.005.
*Horner, R. H., & Day, H. M. (1991). The effects of response efficiency on functionally equivalent competing behaviors. Journal of Applied Behavior Analysis,24(4), 719–732. https://doi.org/10.1901/jaba.1991.24-719.
Howlin, P., & Moss, P. (2012). Adults with autism spectrum disorders. The Canadian Journal of Psychiatry/La Revue Canadienne De Psychiatrie,57(5), 275–283. https://doi.org/10.1177/070674371205700502.
Iwata, B. A., Dorsey, M. F., Slifer, K. J., Bauman, K. E., & Richman, G. S. (1994). Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis,27(2), 197–209. https://doi.org/10.1901/jaba.1994.27-197.
*Jensen, C. C., Mcconnachie, G., & Pierson, T. (2001). Long-term multicomponent intervention to reduce severe problem behavior: A 63-month evaluation. Journal of Positive Behavior Interventions,3(4), 225–236. https://doi.org/10.1177/109830070100300404.
Kratochwill, T. R., Hitchcock, J. H., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., & Shadish, W. R. (2013). Single-case intervention research design standards. Remedial and Special Education, 34, 26–38. https://doi.org/10.1177/0741932512452794.
*Kunnavatana, S. S., Bloom, S. E., Samaha, A. L., Slocum, T. A., & Clay, C. J. (2018a). Manipulating parameters of reinforcement to reduce problem behavior without extinction. Journal of Applied Behavior Analysis,51(2), 283–302. https://doi.org/10.1002/jaba.443.
*Kunnavatana, S. S., Wolfe, K., & Aguilar, A. N. (2018b). Assessing mand topography preference when developing a functional communication training intervention. Behavior Modification,42(3), 364–381. https://doi.org/10.1177/0145445517751437.
*Langdon, N. A., Carr, E. G., & Owen-DeSchryver, J. S. (2008). Functional analysis of precursors for serious problem behavior and related intervention. Behavior Modification,32(6), 804–827. https://doi.org/10.1177/0145445508317943.
*Lehardy, R. K., Lerman, D. C., Evans, L. M., O’Connor, A., & LeSage, D. L. (2013). A simplified methodology for identifying the function of elopement. Journal of Applied Behavior Analysis,46(1), 256–270. https://doi.org/10.1002/jaba.22.
*Lindauer, S. E., Zarcone, J. R., Richman, D. M., & Schroeder, S. R. (2002). A comparison of multiple reinforcer assessments to identify the function of maladaptive behavior. Journal of Applied Behavior Analysis,35(3), 299–303. https://doi.org/10.1901/jaba.2002.35-299.
Maggin, D. M., Briesch, A. M., & Chafouleas, S. M. (2013). An application of the What works clearinghouse standards for evaluating single-subject research: Synthesis of the self-management literature base. Remedial and Special Education,34(1), 44–58. https://doi.org/10.1177/0741932511435176.
Manente, C. J., Maraventano, J. C., LaRue, R. H., Delmolino, L., & Sloan, D. (2010). Effective behavioral intervention for adults on the autism spectrum: Best practices in functional assessment and treatment development. Behavior Analyst Today,11(1), 36–48. https://doi.org/10.1037/h0100687.
Matson, J. L., & Rivet, T. T. (2008). Characteristics of challenging behaviours in adults with autistic disorder, PDD-NOS, and intellectual disability. Journal of Intellectual and Developmental Disability,33(4), 323–329. https://doi.org/10.1080/13668250802492600.
McClintock, K., Hall, S., & Oliver, C. (2003). Risk markers associated with challenging behaviours in people with intellectual disabilities: A meta-analytic study. Journal of Intellectual Disability Research,47(6), 405–416. https://doi.org/10.1046/j.1365-2788.2003.00517.x.
Mills, S., & Rose, J. (2011). The relationship between challenging behaviour, burnout and cognitive variables in staff working with people who have intellectual disabilities. Journal of Intellectual Disability Research,55(9), 844–857. https://doi.org/10.1111/j.1365-2788.2011.01438.x.
Neely, L., Garcia, E., Bankston, B., & Green, A. (2018). Generalization and maintenance of functional communication training for individuals with developmental disabilities: A systematic and quality review. Research in Developmental Disabilities. https://doi.org/10.1016/j.ridd.2018.02.002.
*Petursson, P. I., & Eldevik, S. (2018). Functional analysis and communication training to reduce problem behavior and time in restraint: A case study. Behavior Analysis: Research and Practice. https://doi.org/10.1037/bar0000139.
*Rehfeldt, R. A., & Chambers, M. R. (2003). Functional analysis and treatment of verbal perseverations displayed by an adult with autism. Journal of Applied Behavior Analysis,36(2), 259–261. https://doi.org/10.1901/jaba.2003.36-259.
*Sigafoos, J., & Tucker, M. (2000). Brief assessment and treatment of multiple challenging behaviors. Behavioral Interventions,15(1), 53–70. https://doi.org/10.1002/(SICI)1099-078X(200001/03)15:1%3c53:AID-BIN43%3e3.0.CO;2-V.
*Slaton, J. D., Hanley, G. P., & Raftery, K. J. (2017). Interview-informed functional analyses: A comparison of synthesized and isolated components. Journal of Applied Behavior Analysis,50(2), 252–277. https://doi.org/10.1002/jaba.384.
Sullivan, R. C. (2007). Position paper on the national crisis in adult services for individuals with autism: A call to action (pp. 1–16). Bethesda: Autism Society of America.
Tiger, J. H., Hanley, G. P., & Bruzek, J. (2008). Functional communication training: A review and practical guide. Behavior Analysis in Practice,1(1), 16–23. https://doi.org/10.1007/BF03391716.
*Tincani, M. J., Castrogiavanni, A., & Axelrod, S. (1999). A comparison of the effectiveness of brief versus traditional functional analyses. Research in Developmental Disabilities,20(5), 327–338. https://doi.org/10.1016/S0891-4222(99)00014-1.
Turcotte, P., Mathew, M., Shea, L. L., Brusilovskiy, E., & Nonnemacher, S. L. (2016). Service needs across the lifespan for individuals with autism. Journal of Autism and Developmental Disorders,46(7), 2480–2489. https://doi.org/10.1007/s10803-016-2787-4.
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., et al. (2014). Evidence-based practices for children, youth, and young adults with autism spectrum disorder: A comprehensive review. Journal of Autism and Developmental Disorders,45(7), 1951–1966.
Yang, L. J. (2003). Combination of extinction and protective measures in the treatment of severely self-injurious behavior. Behavioral Interventions,18(2), 109–121. https://doi.org/10.1002/bin.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and Animal Rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gregori, E., Wendt, O., Gerow, S. et al. Functional Communication Training for Adults with Autism Spectrum Disorder: A Systematic Review and Quality Appraisal. J Behav Educ 29, 42–63 (2020). https://doi.org/10.1007/s10864-019-09339-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10864-019-09339-4