
Abstract
Background
Uncertainty remains about the optimum step count per day for health promotion.
Objective
We aimed to investigate the association between step count per day and all-cause mortality risk.
Methods
PubMed, Scopus, and ISI Web of Science were searched to January 2021 to find prospective cohort studies of the association between device-based step count per day and all-cause mortality risk in the general population. Two reviewers extracted data in duplicate and rated the certainty of evidence using the GRADE approach. Study-specific hazard ratios (HRs) were pooled using a random-effects model.
Results
Seven prospective cohort studies with 175,370 person-years and 2310 cases of all-cause mortality were included. The HR for each 1000 steps per day was 0.88 (95% CI 0.83–0.93; I2 = 79%, n = 7) in the overall analysis, 0.87 (95% CI 0.78–0.97; I2 = 59%, n = 3) in adults older than 70 years, and 0.92 (95% CI 0.89–0.95; I2 = 37%, n = 2) in studies controlled for step intensity. Dose–response meta-analysis indicated a strong inverse association, wherein the risk decreased linearly from 2700 to17,000 steps per day. The HR for 10,000 steps per day was 0.44 (95% CI 0.31–0.63). The certainty of evidence was rated strong due to upgrades for large effect size and dose–response gradient.
Conclusions
Even a modest increase in steps per day may be associated with a lower risk of death. These results can be used to develop simple, efficient and easy-to-understand public health messages.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The optimum step count per day for health promotion has not been yet determined. |
The present meta-analysis suggested evidence of high certainty for a strong inverse association between step count per day and risk of mortality. |
There was an inverse linear association within step counts of 2700 to 17,000 steps per day. |
1 Introduction
Being physically active is a healthy lifestyle considered a core part of the health promotion recommendations in both general and diseased populations [1]. There is convincing evidence that higher physical activity, measured with valid tools, is associated with a lower risk of all-cause mortality [2, 3] and in contrast, sitting time and sedentary lifestyle are associated with unfavorable adverse events [4,5,6]. Interventional studies suggested that increasing physical activity can improve levels of traditional cardiometabolic risk factors [7,8,9,10].
Although several types of physical activity are available, walking is a core feature of exercise recommendations that can be easily performed by people [11, 12]. However, the optimum step count per day for health promotion has not yet been determined. The 2018 Physical Activity Guidelines Advisory Committee stated that there is not sufficient evidence regarding the dose–response association of step count per day with multiple health outcomes [13]. The report asserted that step count per day is a simple public health message that can be easily translated to develop simple and effective public health recommendations [13]. There is a public health message that recommends people achieve a goal of 10,000 steps per day, but there is not sufficient scientific evidence behind this recommendation [14].
A recent systematic review indicated that a greater number of steps per day was associated with a lower risk of all-cause mortality and cardiometabolic events and abnormalities [15]. However, a dose–response association between step counts per day and all-cause mortality risk was not determined. In addition, two population-based prospective cohort studies have published new findings [16, 17]. We therefore aimed to perform a systematic review and dose–response meta-analysis of prospective cohort studies investigating the association between step count per day, measured by device-based approaches, and the risk of all-cause mortality in the general population.
2 Methods
This systematic review has been reported according to the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) checklist [18].
2.1 Data Sources and Searches
The systematic search was conducted by one author using pre-defined search terms in PubMed, Scopus, and Web of Science to December 2020, with an updated search to January 2021. Keywords used for the systematic search were [“step count” OR “step per day” OR “steps per day” OR “step/day” OR “steps/day” OR “step/d” OR steps/d”] AND [mortality OR death OR deaths OR survival]. Titles and abstracts were screened according to the pre-defined inclusion and exclusion criteria to identify potential eligible studies. In the next step, full texts were retrieved and independently assessed for eligibility by two review authors (AJ and SSB). Any disagreements were resolved by consensus. Reference lists of all relevant articles and reviews were checked to find potentially relevant studies. We restricted the systematic search to articles written in English. We did not include abstracts or unpublished data in the present meta-analysis.
2.2 Study Selection and Eligibility Criteria
Published prospective cohort studies with all of the following criteria were considered eligible for inclusion in the present meta-analysis: prospective observational studies that (i) included a general population aged 18 years or older; (ii) reported device-based step count per day as exposure; (iii) considered all-cause mortality as the outcome; (iv) reported relative risk, hazard ratio (HR) or rate ratio with 95% confidence intervals (CIs) for three or more quantitative categories of step count per day; and (v) reported the numbers of cases and noncases or person-years in each category of step count. Studies reporting continuous estimation from the associations (e.g., for each 1000 steps per day) were also eligible. Review studies, interventional studies, and studies conducted in diseased populations were excluded.
2.3 Data Extraction
Two independent researchers (AJ and SSB) recorded the following data from each prospective cohort study: first author’s name, date of publication, country, age range, sex, number of participants and cases, duration of follow-up, baseline daily step count, and variables used for statistical control in the multivariable model. The following data were also extracted for data analysis: median point of each category of step count per day, number of events (mortality) and person-years, and the reported effect estimates for each category.
2.4 Risk of Bias (Quality) Assessment
Quality of prospective cohort studies included in the meta-analysis was evaluated by using a 9-point Newcastle–Ottawa Scale [19]. Accordingly, studies with 1–3, 4–6, and 7–9 points were rated low, moderate, and high quality, respectively. Two independent investigators (AJ and SSB) performed the quality assessment to determine whether there was evidence of bias in each included study. Potential disagreements were resolved through consensus.
2.5 Data Synthesis and Analysis
We selected the HR and its 95% CI as the effect size in the present meta-analysis. We performed a dose–response meta-analysis to estimate the HRs of all-cause mortality for each 1000 steps per day increase in each prospective cohort study [20, 21]. For this purpose, median points, the number of cases and person-years, and corresponding HRs and their 95% CIs across categories of step count per day in each study were extracted. For studies reporting step count per day in each category as a range, we considered the midpoint of the upper and lower bounds. Open-ended categories were considered to have the same widths as the closest category. Study-specific HRs were meta-analyzed by a random-effects model [22]. Sensitivity analysis was performed by step-by-step exclusion of each study from the main analysis. Subgroup analyses were conducted according to geographical location, follow-up duration, age, number of participants, adjustment for step intensity, and devices used for counting steps. The Cochrane Q [23] and I2 statistics [24] were used to test for heterogeneity. Potential publication bias was not checked due to the low number of studies (n < 10) [23]. We also tested for a non-linear dose–response association by using a one-stage weighed mixed effects meta-analysis, which is a more precise, flexible, and efficient method than the traditional two-stage method [25]. The analyses were performed using STATA software version 15.0. P values < 0.05 were considered statistically significant.
2.6 Grading the Evidence
The certainty of the evidence was assessed by using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) tool [26]. This tool rates the evidence as high, moderate, low, or very low quality. Prospective cohort studies start as low-quality evidence. Several pre-specified criteria have been considered for downgrading or upgrading the evidence. The criteria used to downgrade the evidence include study limitations, inconsistency, indirectness, imprecision, and publication bias. The criteria used to upgrade the certainty of the evidence include a large magnitude of association, a dose–response gradient, and attenuation by plausible confounding.
3 Results
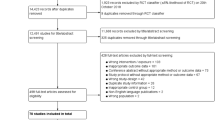
The systematic search and study selection processes are outlined in Fig. 1. The systematic search initially found 8118 records; of those, 2158 records were duplicates. We screened titles and abstracts of 5960 remaining records and found 5914 records were not eligible. We read full texts of the remaining 46 articles and, ultimately, seven population-based prospective cohort studies with 28,141 participants, 175,370 total person-years, and 2310 cases of all-cause mortality were included in the present meta-analysis [16, 17, 27,28,29,30,31].

Literature search and study selection process
3.1 Characteristics of Prospective Cohort Studies
All studies were published after 2015. Two prospective cohort studies were conducted in the US [17, 30], two in the UK [28, 29], and three studies in Japan [31], Norway [16], and Australia [27]. One study was conducted in men [29], one in women [30], and the remainder in both sexes [16, 17, 27, 28, 31]. One study was a pooled analysis of three prospective cohort studies in Australia [27]. Three studies were conducted in older adults aged > 70 years [28, 29, 31], one in women older than 60 years [30], and three other studies in the general population of adults [16, 17, 27]. Three studies had follow-up durations of < 5 years [28,29,30], one had a follow-up duration of 9 years [16], and three other studies continued for 10 years [17, 27, 31].
All studies controlled for body mass index. All but one study [28] controlled for smoking status and alcohol drinking, and all studies controlled for comorbidities except for one study conducted in Australia [27]. One study in Japanese older adults did not control for age in the multivariable analyses [31]. To measure step count per day, five studies used an accelerometer [16, 17, 28,29,30] and two studies used a pedometer [27, 31]. All studies used waist- or hip-mounted devices. All studies measured baseline steps per day, except for one study that made two repeated measurements [27]. Six studies measured step count per day on 7 consecutive days [16, 17, 28,29,30,31], and one study measured step count for a duration of < 7 days [27]. Two studies controlled for step intensity in their multivariable analyses [17, 30], and five other studies did not control for step intensity [16, 27,28,29, 31]. Three studies were rated as being of high quality [17, 30, 31], and four other studies were rated moderate quality [16, 27,28,29] (Electronic Supplementary Material [ESM] Table S1). Detailed procedures used to measure steps per day in each study are described in ESM Table S2. Characteristics of the studies included in the present meta-analysis are indicated in Table 1.
3.2 Meta-analysis
The HR of all-cause mortality for each 1000 steps per day increase was 0.88 (95% CI 0.83–0.93), with substantial heterogeneity, I2 = 79%, Pheterogeneity < 0.001 (Fig. 2). All studies reported significant inverse association, except for one study that reported a non-significant inverse association [31]. The significant inverse association ranged from 0.87 (95% CI 0.81–0.93) to 0.90 (95% CI 0.86–0.94), with step-by-step exclusion of each cohort study from the analysis.

Hazard ratio of all-cause mortality for each 1000 steps per day. HR hazard ratio
The HR was 0.87 (95% CI 0.78–0.97, I2 = 59%, n = 3) in adults older than 70 years, and 0.88 (95% CI 0.82–0.95; I2 = 86%, n = 4) in the general population of adults (p subgroup difference = 0.11). The association was weaker in studies that continued for 10 years (HR 0.93, 95% CI 0.92–0.94; I2 = 0%, n = 3) compared with studies with follow-up < 10 years (HR 0.83, 95% CI 0.80–0.87; I2 = 8%, n = 4) (p subgroup difference < 0.001). The HRs across geographical location were 0.85 (95% CI 0.78–0.92; I2 = 19%, n = 3) in European countries, 0.88 (95% CI 0.77–0.99; I2 = 95%, n = 2) in the US, and 0.91 (95% CI 0.86–0.97; I2 = 0%, n = 2) in Asia (p subgroup difference = 0.04). The HR was 0.81 (95% CI 0.56–1.15; I2 = 74%) in two studies with < 1000 participants, compared with 0.88 (95% CI 0.82–0.93; I2 = 84%) in five studies with > 1000 participants (p subgroup difference = 0.77). In addition, the association was relatively stronger in studies that used an accelerometer (HR 0.86, 95% CI 0.79–0.93; I2 = 86%, n = 5) than in studies that used a pedometer (HR 0.91, 95% CI 0.86–0.97; I2 = 0%, n = 2) for steps assessment (p subgroup difference = 0.71). A subgroup analysis by adjustment for step intensity indicated that the HR was 0.86 (95% CI 0.82–0.91; I2 = 50%, n = 5) in studies that did not take step intensity into account, compared with 0.92 (95% CI 0.89–0.95; I2 = 37%, n = 2) in studies that controlled for step intensity (p subgroup difference < 0.001). Geographical location, devices used for measuring step counts, and age were the potential sources of the heterogeneity.
Dose–response meta-analysis indicated a strong inverse association between step count per day and all-cause mortality risk (Pnon-linearity = 0.24, Pdose–response < 0.001; Fig. 3). In the non-linear dose–response meta-analysis, the HRs for 10,000 and 16,000 steps per day were, respectively, 0.44 (95% CI 0.31–0.63) and 0.34 (95% CI 0.29–0.39) compared with 2700 steps per day (Table 2).

Dose–response association between step count per day and risk of all-cause mortality. Solid line represents non-linear dose response and broken lines represent 95% confidence interval. Circles represent hazard ratio point estimates for steps per day categories from each study with circle size proportional to inverse of standard error. Small vertical black lines are baseline steps per category in each study
3.3 Grading the Evidence
The certainty of evidence was rated strong with upgrades for large effect size (HR < 0.50) and dose–response gradient (Table 3).
4 Discussion
In the present meta-analysis of seven prospective cohort studies, we found that each 1000 steps per day increment was associated with a 12% lower risk of all-cause mortality in the general adult population, and a 13% lower risk in adults older than 70 years. The inverse association persisted in the subgroups defined by age, geographical location, follow-up duration and devices used for counting steps, as well as after adjustments were made for important confounders including body mass index, alcohol drinking, smoking status, step intensity, and pre-existing comorbidities. The association was still significant, albeit of lesser magnitude, in two studies that controlled for step intensity. Dose–response meta-analysis indicated a strong inverse association between step count per day and all-cause mortality risk. The certainty of evidence was rated strong on the basis of the GRADE approach. The strong evidence found in the present meta-analysis suggests that there can be considerable confidence that the estimated effect is similar to the true effect and further research is unlikely to change the confidence in the effect estimate.
The findings of the present meta-analysis are in accordance with those of previous systematic reviews that reported similar inverse associations [13, 15, 32]. However, the existing evidence has not been quantitatively synthesized. In addition, two population-based prospective cohort studies have published new findings. We therefore updated the evidence and rated the certainty of evidence, which indicated that there was strong evidence for beneficial effects of walking on health. Other prospective cohort studies have also indicated that greater number of steps per day was associated with a lower risk of cardiovascular events [33,34,35,36] and type 2 diabetes mellitus [37,38,39]. Another cohort study indicated that greater number of steps per day was associated with better insulin sensitivity [40]. These findings were supported by the findings of intervention studies wherein increasing steps per day resulted in significant improvement in cardiometabolic risk factors [41, 42].
Dose–response meta-analysis indicated a sharp linear inverse association, wherein the risk of mortality decreased proportionally with the increase in steps per day from 1500 to 17,000. However, there were only three categories involving 200 cases of all-cause mortality that reported effect estimates for more than 12,000 steps per day. In the National Health and Nutrition Examination Survey [17], compared with 4000 steps per day, the HRs of mortality were 0.34 (95% CI 0.28–0.45) and 0.34 (95% CI 0.21–0.56) for 14,000 and 16,000 steps per day, respectively. The Australian Tasped prospective cohort study reported an HR of 0.38 (95% CI 0.30–0.46) for 17,000 steps per day compared with 2750 steps per day [27]. Although limited evidence is available for > 12,000 steps per day, the summary HR of all-cause mortality for 12,000 steps per day in our meta-analysis, compared with 2700 steps per day, was 0.41 (95% CI 0.30–0.51), which was still stronger than the proposed threshold to define strong association using the GRADE approach (effect estimate < 0.50 or > 2 for binary outcomes).
Our results indicated that even a modest increase in physical activity, such as an increase of 1000 steps per day, was associated with a 12% lower risk of all-cause mortality. Dose–response analysis indicated that low levels of steps per day, even below the commonly accepted goal of 10,000 steps per day, were associated with a lower risk of mortality [15]. Dose–response analysis also indicated that the risk of death decreased proportionally along with the increase in steps per day. The HR of death, compared with 2700 steps per day, was 0.44 (95% CI 0.31–0.63) for 10,000 steps per day and 0.34 (95% CI 0.29–0.39) for 16,000 steps per day, suggesting that increasing steps per day may confer additional protection against premature death. However, due to the low number of participants, the results for 16,000 steps per day should be interpreted with caution.
There is inter-person variability in step intensity, which may confound the association between step count and mortality. Of seven studies included in the present review, only two cohorts controlled for step intensity. The Women’s Health Study indicated that the association between step count per day and mortality became weaker after controlling for step intensity [30], suggesting that step intensity should be considered when evaluating the association between step count and mortality. However, subgroup analyses in two relatively large cohort studies [17, 30] indicated that step intensity was no longer associated with mortality after controlling for step count per day, suggesting that step count per day may be more important than step intensity for health promotion. Although the subgroup of studies that controlled for step intensity in our review indicated consistently significant inverse association, only two studies were included in that subgroup, thus highlighting a need for more research in the field.
Our review has several strengths. For the first time, we clarified the shape of the dose–response association between step count per day and all-cause mortality risk, wherein the risk of mortality decreased proportionally with the increase in steps per day. This finding confirmed the hypothesis that more steps per day is better for health. The non-linear dose–response meta-analysis suggested the HRs of < 0.50 for > 10,000 steps per day, which surpassed the threshold defined by the GRADE approach (< 0.50 or > 2.0) to define strong association. In addition, our results indicated that even a modest increase in steps per day was significantly associated with a lower risk of death. Furthermore, all studies controlled for body mass index, and six controlled for age, alcohol drinking, smoking status, and pre-existing comorbidities. Although six studies measured baseline steps per day and did not perform repeated measurements during follow-up, there is evidence that steps per day remain stable in short-term follow-up [43, 44]. We included studies conducted in three continents including US, Europe, Asia, and Australia, thus improving the generalizability of the findings. Finally, of seven studies, five studies used an accelerometer to measure step count per day, which is a valid and reliable tool for counting steps [45, 46]. Although different devices are available for counting steps and the number of steps per day measured by different devices may vary up to 20% [47, 48], there are still strong correlations between step volume measured by different tools (r > 0.80) [48,49,50].
There are also limitations for consideration. This is a meta-analysis of observational studies and thus, the results are likely to be affected by residual confounding. Lower step count per day may reflect poor health status and higher presence of comorbidities, and thus, our effect estimate may have been overestimated due to reverse causality bias. Although six studies in the present review controlled for baseline pre-existing comorbidities, these confounding effects cannot be completely controlled by statistical control. However, a subgroup analysis by health status (poor, good, excellent) within the NHANES study indicated that greater steps per day, regardless of health status, was strongly inversely associated with a lower risk of death [17]. In addition, a population-based prospective cohort study in Norway indicated that the results did not change after exclusion of deaths that occurred in the first 2 years of follow-up [16]. Of seven studies included in the present review, four studies had a follow-up duration ≤ 5 years [16, 28,29,30], and two studies included < 1000 participants [28, 31]. The subgroup analyses of studies with longer follow-up duration (10 years, n = 3) and higher number of participants (> 1000 participants, n = 5) showed consistent significant associations. However, there was a limited number of studies in the subgroups. The results also displayed substantial heterogeneity. However, of seven studies in the present review, six studies reported a significant inverse association, and one study showed a marginally significant inverse association. This suggests that the observed heterogeneity is due to differences in the magnitude of the associations rather than differences in the direction of the association. In addition, the association remained significant in the sensitivity analysis and in all subgroups apart from studies with < 1000 participants. Furthermore, three studies in the present review were conducted in individuals older than 70 years, which limits the generalizability of the findings. However, the general population of adults subgroup showed a similar inverse association. A subgroup analysis by age within the National Health and Nutrition Examination Survey [17] indicated that the association did not change materially across categories of age from 40 years to > 65 years. Steps measured by some accelerometers may be due to other types of physical activity such as dancing and housework and thus, the number of steps per day measured by these tools may have been overestimated. Finally, our results reflect the association in the general population of adults and cannot be generalized to diseased populations. There is some evidence of a U-shaped association between step count per day and risk of death in patients with a history of stroke and chronic bronchitis [17].
5 Conclusions
Overall, our findings indicated that greater steps per day was strongly inversely associated with risk of all-cause mortality. Even a modest increase in steps per day was associated with a significantly lower risk of mortality. The risk of death decreased proportionally with the increase in steps per day, suggesting that greater steps per day is better for health. However, there is limited evidence for > 12,000 steps per day. Steps per day is a simple public health message that is easy to understand and implement, and thus our results may help to create effective public health recommendations for health promotions, taking into account step intensity and baseline health status.
References
World Health Organization. Global recommendations on physical activity for health: World Health Organization; 2010.
Ekelund U, Tarp J, Fagerland MW, Johannessen JS, Hansen BH, Jefferis BJ, et al. Joint associations of accelero-meter measured physical activity and sedentary time with all-cause mortality: a harmonised meta-analysis in more than 44 000 middle-aged and older individuals. Br J Sports Med. 2020;54(24):1499–506.
Ekelund U, Tarp J, Steene-Johannessen J, Hansen BH, Jefferis B, Fagerland MW, et al. Dose–response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ. 2019;366:l4570.
Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, Mitchell MS, et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med. 2015;162(2):123–32.
Patterson R, McNamara E, Tainio M, de Sá TH, Smith AD, Sharp SJ, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Berlin: Springer; 2018.
Stamatakis E, Gale J, Bauman A, Ekelund U, Hamer M, Ding D. Sitting time, physical activity, and risk of mortality in adults. J Am Coll Cardiol. 2019;73(16):2062–72.
Alizaei Yousefabadi H, Niyazi A, Alaee S, Fathi M, Mohammad Rahimi GR. Anti-inflammatory effects of exercise on metabolic syndrome patients: a systematic review and meta-analysis. Biol Res Nurs. 2021;23(2):280–92. https://doi.org/10.1177/1099800420958068.
Jadhav RA, Maiya GA, Hombali A, Umakanth S, Shivashankar K. Effect of physical activity promotion on adiponectin, leptin and other inflammatory markers in prediabetes: a systematic review and meta-analysis of randomized controlled trials. Acta Diabetol. 2021;58(4):419–29. https://doi.org/10.1007/s00592-020-01626-1.
Wang S-T, Zheng J, Peng H-W, Cai X-L, Pan X-T, Li H-Q, et al. Physical activity intervention for non-diabetic patients with non-alcoholic fatty liver disease: a meta-analysis of randomized controlled trials. BMC Gastroenterol. 2020;20(1):1–12.
Yarizadeh H, Eftekhar R, Anjom-Shoae J, Speakman JR, Djafarian K. The effect of aerobic and resistance training and combined exercise modalities on subcutaneous abdominal fat: a systematic review and meta-analysis of randomized clinical trials. Adv Nutr (Bethesda, MD). 2021;12(1):179–96.
Harris T, Limb ES, Hosking F, Carey I, DeWilde S, Furness C, et al. Effect of pedometer-based walking interventions on long-term health outcomes: prospective 4-year follow-up of two randomised controlled trials using routine primary care data. PLoS Med. 2019;16(6):e1002836.
U.S. Department of Health and Human Services. Step it up! The surgeon general’s call to action to promote walking and walkable communities. Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General; 2015.
Health UDo, Services H. Physical activity guidelines advisory committee. 2018 physical activity guidelines advisory committee scientific report. 2018.
Lobelo F, Rohm Young D, Sallis R, Garber MD, Billinger SA, Duperly J, et al. Routine assessment and promotion of physical activity in healthcare settings: a scientific statement from the American Heart Association. Circulation. 2018;137(18):e495–522.
Hall KS, Hyde ET, Bassett DR, Carlson SA, Carnethon MR, Ekelund U, et al. Systematic review of the prospective association of daily step counts with risk of mortality, cardiovascular disease, and dysglycemia. Int J Behav Nutr Phys Act. 2020;17(1):1–14.
Hansen BH, Dalene KE, Ekelund U, Wang Fagerland M, Kolle E, Steene-Johannessen J, et al. Step by step: association of device-measured daily steps with all-cause mortality—a prospective cohort Study. Scand J Med Sci Sports. 2020;30(9):1705–11.
Saint-Maurice PF, Troiano RP, Bassett DR, Graubard BI, Carlson SA, Shiroma EJ, et al. Association of daily step count and step intensity with mortality among US adults. JAMA. 2020;323(12):1151–60.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA. 2000;283(15):2008–12.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Appl Eng Agric. 2014;18(6):727–34.
Greenland S, Longnecker MP. Methods for trend estimation from summarized dose–response data, with applications to meta-analysis. Am J Epidemiol. 1992;135(11):1301–9.
Orsini N, Bellocco R, Greenland S. Generalized least squares for trend estimation of summarized dose–response data. Stata J. 2006;6(1):40–57.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. New York: Wiley; 2019.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Crippa A, Discacciati A, Bottai M, Spiegelman D, Orsini N. One-stage dose–response meta-analysis for aggregated data. Stat Methods Med Res. 2019;28(5):1579–96.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6.
Dwyer T, Pezic A, Sun C, Cochrane J, Venn A, Srikanth V, et al. Objectively measured daily steps and subsequent long term all-cause mortality: the tasped prospective cohort study. PLoS ONE. 2015;10(11):e0141274.
Fox KR, Ku P-W, Hillsdon M, Davis MG, Simmonds BA, Thompson JL, et al. Objectively assessed physical activity and lower limb function and prospective associations with mortality and newly diagnosed disease in UK older adults: an OPAL four-year follow-up study. Age Ageing. 2015;44(2):261–8.
Jefferis BJ, Parsons TJ, Sartini C, Ash S, Lennon LT, Papacosta O, et al. Objectively measured physical activity, sedentary behaviour and all-cause mortality in older men: does volume of activity matter more than pattern of accumulation? Br J Sports Med. 2019;53(16):1013–20.
Lee I-M, Shiroma EJ, Kamada M, Bassett DR, Matthews CE, Buring JE. Association of step volume and intensity with all-cause mortality in older women. JAMA Intern Med. 2019;179(8):1105–12.
Yamamoto N, Miyazaki H, Shimada M, Nakagawa N, Sawada SS, Nishimuta M, et al. Daily step count and all-cause mortality in a sample of Japanese elderly people: a cohort study. BMC Public Health. 2018;18(1):540.
Kraus WE, Janz KF, Powell KE, Campbell WW, Jakicic JM, Troiano RP, et al. Daily step counts for measuring physical activity exposure and its relation to health. Med Sci Sports Exerc. 2019;51(6):1206–12.
Cochrane SK, Chen SH, Fitzgerald JD, Dodson JA, Fielding RA, King AC, et al. Association of accelerometry-measured physical activity and cardiovascular events in mobility-limited older adults: the life (lifestyle interventions and independence for elders) study. J Am Heart Assoc. 2017;6(12):e007215.
Huffman KM, Sun J-L, Thomas L, Bales CW, Califf RM, Yates T, et al. Impact of baseline physical activity and diet behavior on metabolic syndrome in a pharmaceutical trial: results from NAVIGATOR. Metabolism. 2014;63(4):554–61.
Jefferis BJ, Parsons TJ, Sartini C, Ash S, Lennon LT, Papacosta O, et al. Does total volume of physical activity matter more than pattern for onset of CVD? A prospective cohort study of older British men. Int J Cardiol. 2019;278:267–72.
Yates T, Haffner SM, Schulte PJ, Thomas L, Huffman KM, Bales CW, et al. Association between change in daily ambulatory activity and cardiovascular events in people with impaired glucose tolerance (NAVIGATOR trial): a cohort analysis. Lancet. 2014;383(9922):1059–66.
Ballin M, Nordström P, Niklasson J, Alamäki A, Condell J, Tedesco S, et al. Daily step count and incident diabetes in community-dwelling 70-year-olds: a prospective cohort study. BMC Public Health. 2020;20(1):1–10.
Kraus WE, Yates T, Tuomilehto J, Sun J-L, Thomas L, McMurray JJ, et al. Relationship between baseline physical activity assessed by pedometer count and new-onset diabetes in the NAVIGATOR trial. BMJ Open Diabetes Res Care. 2018;6(1):e000523.
Ponsonby A-L, Sun C, Ukoumunne OC, Pezic A, Venn A, Shaw JE, et al. Objectively measured physical activity and the subsequent risk of incident dysglycemia: the Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care. 2011;34(7):1497–502.
Dwyer T, Ponsonby A-L, Ukoumunne OC, Pezic A, Venn A, Dunstan D, et al. Association of change in daily step count over five years with insulin sensitivity and adiposity: population based cohort study. BMJ. 2011;342:c7249.
Herzig K, Ahola R, Leppäluoto J, Jokelainen J, Jämsä T, Keinänen-Kiukaanniemi S. Light physical activity determined by a motion sensor decreases insulin resistance, improves lipid homeostasis and reduces visceral fat in high-risk subjects: PreDiabEx study RCT. Int J Obes. 2014;38(8):1089–96.
Yates T, Davies M, Gorely T, Bull F, Khunti K. Effectiveness of a pragmatic education program designed to promote walking activity in individuals with impaired glucose tolerance: a randomized controlled trial. Diabetes Care. 2009;32(8):1404–10.
Keadle SK, Shiroma EJ, Kamada M, Matthews CE, Harris TB, Lee I-M. Reproducibility of accelerometer-assessed physical activity and sedentary time. Am J Prev Med. 2017;52(4):541–8.
Saint-Maurice PF, Sampson JN, Keadle SK, Willis EA, Troiano RP, Matthews CE. Reproducibility of accelerometer and posture-derived measures of physical activity. Med Sci Sports Exerc. 2020;52(4):876–83.
Bassett DR, Toth LP, LaMunion SR, Crouter SE. Step counting: a review of measurement considerations and health-related applications. Sports Med. 2017;47(7):1303–15.
Strath SJ, Kaminsky LA, Ainsworth BE, Ekelund U, Freedson PS, Gary RA, et al. Guide to the assessment of physical activity: clinical and research applications: a scientific statement from the American Heart Association. Circulation. 2013;128(20):2259–79.
Rosenberger ME, Buman MP, Haskell WL, McConnell MV, Carstensen LL. 24 hours of sleep, sedentary behavior, and physical activity with nine wearable devices. Med Sci Sports Exerc. 2016;48(3):457.
Toth LP, Park S, Springer CM, Feyerabend MD, Steeves JA, Bassett DR. Video-recorded validation of wearable step counters under free-living conditions. Med Sci Sports Exerc. 2018;50(6):1315–22.
Campos C, DePaul VG, Knorr S, Wong JS, Mansfield A, Patterson KK. Validity of the ActiGraph activity monitor for individuals who walk slowly post-stroke. Top Stroke Rehabil. 2018;25(4):295–304.
Feito Y, Bassett DR, Thompson DL. Evaluation of activity monitors in controlled and free-living environments. Med Sci Sports Exerc. 2012;44(4):733–41.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
Ahmad Jayedi, Ali Gohari, and Sakineh Shab-bidar declare that they have no conflict of interest.
Availability of data and material
Available upon request.
Code availability
Available upon request.
Ethics approval
Not required.
Author contributions
The authors’ responsibilities were as follows—AJ and SS-B: designed research; AJ and SS-B: performed the literature search, screened articles, extracted data, and wrote the paper; AJ: analyzed data and interpreted the results; SS-B and AG: revised the subsequent draft for important intellectual content; SS-B is the guarantor; and all authors have read and approved the final manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Jayedi, A., Gohari, A. & Shab-Bidar, S. Daily Step Count and All-Cause Mortality: A Dose–Response Meta-analysis of Prospective Cohort Studies. Sports Med 52, 89–99 (2022). https://doi.org/10.1007/s40279-021-01536-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-021-01536-4