
Abstract
The aim of the current study was to perform a systematic review and meta-analysis to evaluate the relationship between step count and changes in blood pressure (BP). Studies involving healthy adults and an intervention in the form of brisk walking with a pedometer were included. Net changes in BP and step count in each trial were calculated and pooled. In addition, the pooled net changes of two categories (trials that achieved walking 10,000 steps a day and those that did not) were compared. A meta-regression analysis was performed to examine the relationship between net changes in BP and step count. Fourteen trials were analyzed. Pooled net changes in BP improved significantly (systolic BP, −3.1 mm Hg; diastolic BP, −1.6 mm Hg). When the trials were categorized depending on whether they achieved walking 10,000 steps a day, the pooled net change in systolic BP and diastolic BP did not differ significantly between both groups of subjects. The meta-regression analyses indicated that net change in systolic BP was significantly associated with an increased step count (e.g., systolic BP is expected to decrease approximately 4 mm Hg if increased step count by 2000 steps a day). However, net change in systolic BP was not associated with the step count in an intervention group following the intervention. At present, there is presumably no evidence that walking 10,000 steps a day lowers the BP to any marked degree. In order to reduce systolic BP by walking with a pedometer, one should be mindful of increasing one’s step count.
Similar content being viewed by others
Introduction
Hypertension causes arteriosclerosis and can lead to the development of cerebrovascular or coronary artery disease [1]. The effects of hypertension also place a burden on the national budget. In Japan, national health care costs due to hypertension amount to 1.8 trillion yen every year [2]. Hypertension accounts for approximately 40% of the costs of cardiovascular disease; together with cerebrovascular disease and coronary artery disease, the three diseases cost 4.4 trillion yen, which is approximately 2% of the national budget [2]. Furthermore, if blood pressure (BP) rises a few mm Hg, it can greatly affect an individual’s prognosis [3, 4]. Conversely, preventing or alleviating hypertension benefits health. For example, a meta-analysis of pharmacotherapy for hypertension recently estimated that a change of −10 mm Hg in systolic BP reduced the risk of developing cardiovascular disease by 20%, the risk of developing coronary artery disease by 17%, the risk of suffering a stroke by 27%, the risk of developing heart failure by 28%, and overall mortality by 13% [5]. Therefore, lowering BP should limit medical expenses and improve health.
The risk factors for hypertension depend heavily on lifestyle [6,7,8,9,10,11,12]. As with pharmacotherapy, management of hypertension with lifestyle modifications is linked to a lower BP [13,14,15,16,17,18,19,20]. A lack of physical activity (PA) is a major factor for development of hypertension. Meta-analyses of randomized controlled trials have indicated that regular aerobic exercise in all forms, such as walking, bicycle, or jogging, had a positive effect on BP, with an estimated change in systolic BP of approximately −3.5 mm Hg and an estimated change in diastolic BP of approximately −2.5 mm Hg [16,17,18,19,20]. Walking is a form of aerobic exercise that can be performed at moderate or vigorous intensity (approximately 3 to 6 METs) [21] and is preferred among sedentary adults who want to combat their lack of PA [22]. A meta-analysis that was limited to randomized controlled trials involving walking indicated that the change in systolic BP was approximately −3.6 mm Hg and the change in diastolic BP was approximately −1.5 mm Hg, but most of the analyzed randomized controlled trials involved supervised walking [20]. Recently, various guidelines have often recommended walking 10,000 steps a day to promote health [23]. A meta-analysis indicated that an intervention to increase PA involving the use of a pedometer facilitated an increased step count and an improved BP [24], providing important evidence on the effectiveness of walking. However, that meta-analysis included few randomized controlled trials that sought to lower BP [24]. In addition, the step count needed to lower the BP and the effect of walking 10,000 steps a day on BP are unclear. Recent systematic reviews and meta-analyses evaluated the association between step count and clinical outcomes such as hemoglobin A1c, body mass index, lipid profile, or BP, and they reported that the step count increased significantly following the intervention that involved walking, but the found no significant improvement in all clinical outcomes [25, 26]. In addition, the analyzed studies involved patients with type 2 diabetes [25, 26], and few randomized controlled trials evaluated BP [26].
The aim of the current study was to perform a systematic review and meta-analysis to evaluate the effects of an intervention that involved walking with a pedometer on BP and to evaluate the relationship between step count and changes in BP.
Methods
This systematic review and meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [27].
Data sources and study selection
Databases were searched by a Boolean search for literature published until September 2017. MEDLINE, SPORTDiscus, the Cochrane library, and Google Scholar were searched using terms: hypertension, blood pressure, exercise, exercise therapy, physical fitness, walking, and pedometer (Supplementary Table 1). In addition, listed references of original articles, review, and textbooks were also searched. Studies that were included in the meta-analysis were those that (1) involved healthy adults ≥ 18 years of age with no cardiovascular or other diseases except for lifestyle-related diseases such as hypertension, type 2 diabetes, dyslipidemia, obesity, and metabolic syndrome; (2) a PA group that walked briskly with a pedometer (the intervention) without performing any other exercise and that measured the daily step count; (3) a non-intervention control group in which the daily step count was only measured with a pedometer; (4) both groups being instructed to continue their usual routine; (5) neither group receiving any other intervention; (6) subjects being randomly assigned to one of two groups (i.e., a randomized controlled trial); and (7) recording of the mean systolic BP and diastolic BP at the baseline and after intervention plus the standard deviation (SD) in those measurements and the mean step count (steps per day) following the intervention.
The identified articles were first screened by title and abstract, and full-text of the article was obtained if the study included an intervention involving walking with a pedometer. Once these articles were identified, two authors (YI and NA) determined whether or not they should be included in this meta-analysis. If the two authors disagreed, a third author (SM) made a final decision as to whether or not to include the study.
Data extraction and assessment of the risk of bias
The date and details of the intervention (mean systolic BP or diastolic BP, mean step count, SD in those data, number of subjects, detail on the intervention group and the control group, and the duration of the intervention) were extracted from the studies for the meta-analysis.
The risk of bias in each trial was assessed using the Cochrane Risk of Bias tool, which consisted of six domains: (1) random sequence generation, (2) allocation concealment, (3) blinding, (4) incomplete outcome data, (5) selective reporting, and (6) other bias [28]. Each domain was ranked in one of three categories: low risk, high risk, or unclear.
Two authors (YI and NA) independently extracted and checked the aforementioned data and assessed the risk of bias using the Cochrane Risk of Bias tool.
Statistical analyses
The baseline BP and step count weighted by the sample size were expressed as the mean ± SD and the differences between the PA group and the control group were evaluated using the Mann–Whitney test.
Net changes in the BP for each trial were calculated as follows: (mean value at post-intervention in PA group – mean value at baseline in PA group) – (mean value at post-intervention in control group – mean value at baseline in control group). Crossover studies were calculated as follows: (mean value at post-intervention in PA group – mean value at post-intervention in control group). Pooled net changes were calculated by a random effects model and were weighted by the inverse variance of differences from baseline to post-intervention in each trial [29]. If the SD of the differences in baseline and post-intervention was not reported but each SD in baseline and post-intervention was reported, we assumed that the correlation coefficient between baseline and post-intervention was 0.50 and imputed it as such [30]. In addition, net changes in the step count were defined as the difference in the mean step count per day for the PA group and the control group following the intervention and pooled. Results of net changes were expressed as 95% confidence intervals (95% CI). Cochran Q statistics and I2 value were calculated to evaluate whether or not the pooled net change showed heterogeneity among trials. The level of heterogeneity was assessed using the I2 statistic: low risk (<25%), moderate risk (25 to 75%), and high risk (>75%) [31].
A subgroup analysis was performed by limiting trials that achieved walking 10,000 steps a day (i.e., a mean step count ≥ 10,000 steps a day for the PA group following the intervention) and those that did not. The net change in BP was then pooled, and those changes of the two categories were compared. In addition, a sensitivity analysis was used to evaluate the influence of a risk of bias according to the Cochrane Risk of Bias tool [28]. Trials falling into one or more domains of a high risk of bias were excluded and the net change in BP was then pooled.
A meta-regression analysis was performed using the method of moments weighted by the sample size in order to examine the relationship between net changes in BP and the step count. Four explanatory variables on step count were selected: (i) step count in the PA group, defined as the mean step count per day in the PA group following the intervention; (ii) increased step count, defined as the difference in the mean step count per day for the PA group and the control group following the intervention; (iii) cumulative step count in the PA group following the intervention, defined as (i) × the period of intervention (days); and (iv) cumulative increased step count following the intervention, defined as (ii) × the period of intervention (days). The regression coefficient (β) and coefficient of determination (R2) were calculated for each explanatory variable. In addition, when the relationship between net changes in BP and age was examined, mean age served as a secondary explanatory variable.
Publication bias was evaluated by assessing the symmetry of funnel plots produced by net changes in BP (x-axis) and inverse standard errors (y-axis) using Egger’s regression test [32, 33]. In addition, the number of missing trials was estimated using the trim and fill method of Duval and Tweedie [34]. If results suggested that trials were missing, then pooled net changes in BP were adjusted in light of the effect of those studies.
In all statistical tests, P < 0.05 was considered statistically significant. Comprehensive Meta-Analysis (Version 2.2; Biostat, Inc., Englewood, NJ) was used to perform the meta-analysis and meta-regression analysis and to assess publication bias. Other statistical tests were performed using SPSS (Version 21.0; IBM Inc, Armonk, NY).
Results
Study selection
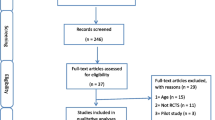
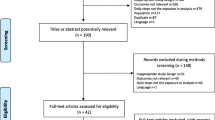
A literature search resulted in 66 full-text articles that described studies involving intervention in the form of walking regularly with a pedometer and indicated BP. Of these 66 articles, 53 were excluded (Fig. 1). As a result, 14 trials described in 13 articles [35,36,37,38,39,40,41,42,43,44,45,46,47] were analyzed.

PRISMA flow diagram regarding article selection for the meta-analysis
Study characteristics
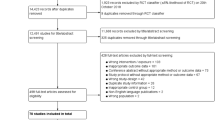
Twelve trials [35,36,37,38,39,40,41,42,43, 45, 47] had a parallel design, and two trials [44, 46] had a crossover design. Table 1 shows the details for each article. The trials included a total of 746 subjects (PA group: n = 356; control group: n = 390). The number of male and female subjects was not reported in three trials [37, 38, 40], but the remaining trials included 251 males (38.0%) and 410 females (62.0%). The mean age ranged 21 to 63 years of age (median: 50 years of age). The duration of intervention ranged from 4 to 24 weeks (median: 8 weeks). Figure 2 shows overall results for a risk of bias. Five trials [35, 36, 40, 46, 47] included one or more domains with the high risk of bias (Supplementary Table 2).

Overall results for risk of bias. Numbers of each bar show the number of trials within each judgment for attribute in the Cochrane Risk of Bias tool
The baseline mean systolic BP and diastolic BP did not differ significantly between the PA group and the control group. In addition, ten trials [35,36,37,38,39, 42, 43, 45, 47] reported the baseline mean step count. The baseline mean step count was 5547 ± 1540 steps per day (5731 ± 2385 steps per day in the PA group and 5388 ± 2104 steps per day in the control group), and the baseline mean step count did not differ significantly between the two groups. Five trials [37, 39, 41, 43, 46] achieved a mean step count ≥ 10,000 steps a day in the PA group following the intervention. Figures 3 and 4 show respective baseline systolic BP and diastolic BP in each trial. Both the baseline systolic BP and diastolic BP did not differ significantly between trials that achieved walking 10,000 steps a day and those that did not.

Baseline systolic BP and forest plot for the net changes in systolic BP. Each trial is represented with black squares (net change) and widths (95% CI); the size of the black squares is in proportion to the weighting by inverse variance in each trial. The pooled net changes are represented by black rhombuses (net change) and widths (95% CI)

Baseline diastolic BP and forest plot for the net changes in diastolic BP. Each trial is represented with black squares (net change) and widths (95% CI); the size of the black squares is in proportion to the weighting by inverse variance in each trial. The pooled net changes are represented by black rhombuses (net change) and widths (95% CI)
Pooled net change
Figures 3 and 4 also show respective forest plots of the net changes in systolic BP and diastolic BP in each trial. The pooled net changes indicated significant decreases in systolic BP and diastolic BP. The pooled net change in systolic BP and diastolic BP did not contain significant heterogeneity.
In addition, these figures show pooled net changes in systolic BP and diastolic BP in a subgroup analysis of two categories: achieved walking 10,000 steps a day and those that did not. In each category of trials, the pooled net change in systolic BP decreased significantly and did not contain significant heterogeneity. The pooled net change in diastolic BP in trials that achieved walking 10,000 steps a day did not decrease significantly and did not contain significant heterogeneity. In trials that did not achieve walking 10,000 steps a day, the pooled net change in diastolic BP did not decrease significantly but it contained significant heterogeneity. The pooled net changes in systolic BP and diastolic BP did not contain significant heterogeneity between the two categories of trials.
When five trials included one or more domains with a high risk of bias were excluded, results of sensitivity analysis revealed that, pooled net change in systolic BP decreased significantly (−2.9 mm Hg; 95% CI, −5.3 to −0.5) and that it did not contain significant heterogeneity (I2 = 0.7%). Results also revealed that pooled net change in diastolic BP decreased significantly (−2.1 mm Hg; 95% CI, −4.1 to −0.1) but that it contained significant heterogeneity (I2 = 54.2%).
Meta-regression analyses
Figures 5 and 6 show the relationship between net changes in BP and step count according to a meta-regression analysis. The net change in systolic BP was significantly associated with two explanatory variables: (ii) increased step count (P < 0.01) and (iv) cumulative increased step count (P < 0.01). When the regression coefficients were used in calculations, the net change in systolic BP, for example, was estimated to decrease approximately 2 mm Hg if the step count increased by 1000 steps a day. Similarly the net change in systolic BP was estimated to decrease approximately 7 mm Hg if the step count increased by 1000 steps a day for 48 weeks. However, the net change in systolic BP was not significantly associated with (i) step count in the PA group or (iii) cumulative step count in the PA group. The net change in diastolic BP was not significantly associated with any explanatory variables.

The relationship between changes in the systolic BP and step count. Four explanatory variables were selected, as follows: (i) step count in the PA group, defined as the mean step count per day in the PA group following the intervention; (ii) increased step count, defined as the difference in the mean step count per day for the PA group and the control group following the intervention; (iii) cumulative step count in the PA group, defined as (i) × the period of intervention; and (iv) cumulative increased step count, defined as (ii) × the period of intervention

The relationship between changes in the diastolic BP and step count. Four explanatory variables were selected, as follows: (i) step count in the PA group, defined as the mean step count per day in the PA group following the intervention; (ii) increased step count, defined as the difference in the mean step count per day for the PA group and the control group following the intervention; (iii) cumulative step count in the PA group, defined as (i) × the period of intervention; and (iv) cumulative increased step count, defined as (ii) × the period of intervention
In addition, the net change in systolic BP was not significantly associated with mean age (β = 0.15, P = 0.11; R2 = 0.09), but the net change in diastolic BP was significantly associated with mean age (β = 0.19, P < 0.001; R2 = 0.41).
Publication bias
Based on Egger’s regression test, the intercept for systolic BP was −1.04 (P = 0.13), the intercept for diastolic BP was −0.64 (P = 0.56). Thus, the funnel plots were not significantly asymmetrical. Duval and Tweedie’s trim and fill suggested that two trials were missing for the systolic BP and that one trial was missing for the diastolic BP (Supplementary Figs. 1 and 2). After adjusting for the effects of those missing trials, the pooled net change in systolic BP was estimated to be −2.8 mm Hg (95% CI, −4.8 to −0.7) and the pooled net change in diastolic BP was −1.5 mm Hg (95% CI, −3.0 to −0.1).
Discussion
The current study performed a meta-analysis to evaluate the effects of walking with a pedometer on BP. A search of the literature identified 14 trials (746 subjects). The pooled net changes in BP were significant reductions (systolic BP, −3.1 mm Hg; diastolic BP, −1.6 mm Hg) and did not contain significant heterogeneity. In nine trials that did not achieve a mean step count ≥ 10,000 steps a day for the PA group following the intervention, the pooled net change in diastolic BP contained significant heterogeneity. A subgroup analysis indicated that the pooled net change in systolic BP and diastolic BP did not differ significantly between trials that achieved walking 10,000 steps a day and trials that did not achieve walking 10,000 steps a day. When trials were limited to those of low and unclear risk of bias, systolic and diastolic BP decrease significantly but diastolic BP contained significant heterogeneity. A meta-regression analysis was performed assuming that differences in reduced BP were due to walking a certain number of steps per day. Results indicated that the net change in systolic BP was associated with an increased step count and a cumulative increased step count.
Epidemiological studies and meta-analyses have revealed that walking daily or generally exercising by walking lowers BP and reduces the risk of developing hypertension [17, 19, 20, 48, 49]. A recent meta-analysis of randomized controlled trials reported that the pooled net change in systolic BP was −3.6 mm Hg and that the pooled net change in diastolic BP was −1.5 mm Hg as a result of walking [20], which is similar to the current findings. However, most of the trials analyzed in previous meta-analyses have involved supervised intervention [17, 19, 20]. Measuring the step count with a pedometer is often used to ascertain the volume of walking or to set a goal for subjects, and the intervention can be performed without supervision [50]. A previous meta-analysis found that an intervention in the form of walking enhanced with pedometer feedback increased the step count and thus increased PA [24]. A target step count can be, for example, 10,000 steps a day [23, 37, 40, 41, 43,44,45,46]. Guidelines to promote health often recommend walking 10,000 steps a day since this step count is considered to be an ideal level of PA to remain healthy [23]. The recent National Health and Nutrition Survey in Japanese reported that the mean step count was 6670 steps per day in 2015 [51], so Japanese are undoubtedly not walking enough to stay healthy. In current study, five trials [37,39,41,43,46] achieved a mean step count ≥ 10,000 steps a day in the PA group following the intervention. However, the change in systolic BP and diastolic BP did not differ significantly between trials that achieved walking 10,000 steps a day and those that did not. Thus, doubts remain as to whether or not walking 10,000 steps a day will lower systolic and diastolic BP. Furthermore, a meta-regression analysis indicated that the change in systolic BP was not associated with the step count in the PA group or the cumulative step count in the PA group. In contrast, however, a meta-regression analysis indicated that the change in systolic BP was associated with an increased step count following intervention. If an inactive adult, for example, increases his or her step count by 2000 steps a day (roughly equivalent to 20 min a day of moderate-intensity exercise [52]) in comparison to a sedentary lifestyle, the adult’s systolic BP is estimated to decrease approximately 4 mm Hg. If the individual walks keeping his or her step count by plus 2000 steps a day for 48 weeks, the individual’s systolic BP is estimated to decrease approximately 13 mm Hg. In order to lower BP by walking with a pedometer, the ideal method may involve focusing on increasing one’s step count per day rather than focusing on an exact step count target (e.g., 10,000 steps a day). Incidentally, when adults with impaired glucose tolerance walked an additional 2000 steps (as mentioned earlier) and modified their lifestyle for 48 weeks (12 months), they had an 8% lower risk of developing cardiovascular disease 6 years later [53]. Taken together, the current findings indicate that an increased step count should lead to a lower BP and greatly help to subsequently decrease the incidence of cardiovascular disease.
The current study had several limitations. First, in trials that did not achieve walking 10,000 steps a day, the pooled net change in diastolic BP contained significant heterogeneity and was deemed to represent a moderate risk of bias. In addition, current study resulted that the net change in diastolic BP was not significantly associated with step count. The current study was unable to directly ascertain those reasons. However, age bias might have influenced the changes in diastolic BP since subjects in the analyzed trials had a mean age of 21 to 63 years. The diastolic BP decreased or remained the same with age according to the Framingham Heart Study [54], while a cross-sectional study reported that functional vasodilatation decreased with age [55]. A recent meta-analysis reported that the net change in the diastolic BP as a result of regular aerobic exercise was related to age [56]. In the current study, a meta-regression analysis similarly indicated that the net change in diastolic BP was significantly associated with mean age. Therefore, the heterogeneity noted might be the result of changes in functional vasodilatation with age. Additional analysis of the relationship between changes in diastolic BP and step count should be performed in the future. A second limitation of the current study is that while our meta-regression analysis considered the step count following the intervention as an explanatory variable, it could not consider the baseline step count. This was because all of the trials indicated the mean step count following the intervention, but four trials did not indicate the baseline mean step count [40, 41, 44, 46]. In addition, four trials did not statistically compare the step count in the PA group and the control group at baseline [36, 42, 43], and one trial [35] indicated that the step count was significantly greater in the control group than in the PA group at the baseline [35]. The effects of the baseline step count may need to be considered in the future. A third limitation of the current study is the influence of publication bias. The current study found that two trials were missing systolic BP data, and one trial was missing diastolic BP data. When the effects of these missing trials were considered, the pooled net changes in systolic BP and diastolic BP did not change significantly. This publication bias was presumably due to the small samples in the trials. Therefore, these issues need to be examined in the future.
In conclusion, the currents results substantiate the claim that an intervention involving walking with a pedometer lowers BP (systolic BP, −3.1 mm Hg; diastolic BP, −1.6 mm Hg). Systolic BP should decrease in proportion to the increased step count. If, for example, an individual increases his or her step count by 2000 steps a day in comparison to a sedentary lifestyle, the individual’s systolic BP is expected to decrease approximately 4 mm Hg according to current calculations. However, the step count itself was not associated with any change in BP. At present, there seems to be no hard evidence that achieving 10,000 steps a day appreciably lowers BP. In order to reduce BP by walking with a pedometer, one should be mindful of increasing one’s step count rather than focusing on the step count per day.
Summary
What is known about this topic?
-
Various guidelines have often recommended walking 10,000 steps a day to promote health.
-
Meta-analyses reported that the pooled change in blood pressure was the reductions as a result of supervised walking.
What this study adds?
-
An intervention involving walking with a pedometer lowers blood pressure.
-
Systolic blood pressure will decrease in proportion to the increased step count.
-
At present, there is presumably no evidence that walking 10,000 steps a day lowers the blood pressure to any marked degree.
References
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospective studies collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–13.
Health Statistics Office, Director-General for Statistics and Information Policy, Ministry of Health, Labour and Welfare of Japan. Estimates of National Medical Care Expenditure, FY 2015. Tokyo, Japan: Statistical Surveys conducted by Ministry of Health, Labour and Welfare; 2017.
He J, Gu D, Chen J, Wu X, Kelly TN, Huang JF, et al. Premature deaths attributable to blood pressure in China: a prospective cohort study. Lancet. 2009;374:1765–72.
Takashima N, Ohkubo T, Miura K, Okamura T, Murakami Y, Fujiyoshi A, et al. Long-term risk of BP values above normal for cardiovascular mortality: a 24-year observation of Japanese aged 30 to 92 years. J Hypertens. 2012;30:2299–306.
Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–67.
Intersalt Cooperative Research Group. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24 h urinary sodium and potassium excretion. BMJ. 1988;297:319–28.
Hashimoto T, Fujita Y, Ueshima H, Kagamimori S, Kasamatsu T, Morioka S, et al. Urinary sodium and potassium excretion, body mass index, alcohol intake and blood pressure in three Japanese populations. J Hum Hypertens. 1989;3:315–21.
Forman JP, Stampfer MJ, Curhan GC. Diet and lifestyle risk factors associated with incident hypertension in women. JAMA. 2009;302:401–11.
Colin BA, Adair LS, Popkin BM. Ethnic differences in the association between body mass index and hypertension. Am J Epidemiol. 2002;155:346–53.
Crump C, Sundquist J, Winkleby MA, Sundquist K. Interactive effects of physical fitness and body mass index on the risk of hypertension. JAMA Intern Med. 2016;176:210–6.
Sawada S, Tanaka H, Funakoshi M, Shindo M, Kono S, Ishiko T. Five year prospective study on blood pressure and maximal oxygen uptake. Clin Exp Pharmacol Physiol. 1993;20:483–7.
Ishizaka N, Ishizaka Y, Toda E, Koike K, Yamakado M, Nagai R. Impacts of changes in obesity parameters for the prediction of blood pressure change in Japanese individuals. Kidney Blood Press Res. 2009;32:421–7.
Dickinson HO, Mason JM, Nicolson DJ, Campbell F, Beyer FR, Cook JV, et al. Lifestyle interventions to reduce raised blood pressure: a systematic review of randomized controlled trials. J Hypertens. 2006;24:215–33.
Xin X, He J, Frontini MG, Ogden LG, Motsamai OI, Whelton PK. Effects of alcohol reduction on blood pressure: a meta-analysis of randomized controlled trials. Hypertension. 2001;38:1112–7.
Graudal NA, Hubeck-Graudal T, Jürgens G. Effects of low-sodium diet vs. high-sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride (Cochrane Review). Am J Hypertens. 2012;25:1–15.
Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure: a meta-analysis of randomized, control trial. Ann Intern Med. 2002;136:493–503.
Kelley GA, Kelley KS, Tran ZV. Walking and resting blood pressure in adults: a meta-analysis. Prev Med. 2001;33:120–7.
Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc. 2013;2:e004473.
Hanson S, Jones A. Is there evidence that walking groups have health benefits? A systematic review and meta-analysis. Br J Sports Med. 2015;49:710–5.
Murtagh EM, Nichols L, Mohammed MA, Holder R, Nevill AM, Murphy MH. The effect of walking on risk factors for cardiovascular disease: an updated systematic review and meta-analysis of randomised control trials. Prev Med. 2015;72:34–43.
Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR Jr, Tudor-Locke C, et al. 2011 Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43:1575–81.
Williams PT. Advantage of distance- versus time-based estimates of walking in predicting adiposity. Med Sci Sports Exerc. 2012;44:1728–37.
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–59.
Bravata DM, Smith-Spangler C, Sundaram V, Gienger AL, Lin N, Lewis R, et al. Using pedometers to increase physical activity and improve health: a systematic review. JAMA. 2007;298:2296–304.
Qiu S, Cai X, Chen X, Yang B, Sun Z. Step counter use in type 2 diabetes: a meta-analysis of randomized controlled trials. BMC Med. 2014;12:36.
Baskerville R, Ricci-Cabello I, Roberts N, Farmer A. Impact of accelerometer and pedometer use on physical activity and glycaemic control in people with type 2 diabetes: a systematic review and meta-analysis. Diabet Med. 2017;34:612–20.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647.
Higgins JPT, Green S (eds). Cochrane handbook for systematic reviews of interventions version 5.1.0. [updated March 2011]. London, UK: The Cochrane Collaboration; 2011. Available from http://handbook.cochrane.org/
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol. 1992;45:769–73.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
Cooper H, Hedges LV. The handbook of research synthesis. New York, NY: Russell Safe Foundation; 1994.
Egger M, Davey G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56:455–63.
Moreau KL, Degarmo R, Langley J, McMahon C, Howley ET, Bassett DR, et al. Increasing daily walking lowers blood pressure in postmenopausal women. Med Sci Sports Exerc. 2001;33:1825–31.
Tudor-Locke C, Bell RC, Myers AM, Harris SB, Ecclestone NA, Lauzon N, et al. Controlled outcome evaluation of the First Step Program: a daily physical activity intervention for individuals with type II diabetes. Int J Obes Relat Metab Disord. 2004;28:113–9.
Araiza P, Hewes H, Gashetewa C, Vella CA, Burge MR. Efficacy of a pedometer-based physical activity program on parameters of diabetes control in type 2 diabetes mellitus. Metabolism. 2006;55:1382–7.
Murphy MH, Murtagh EM, Boreham CA, Hare LG, Nevill AM. The effect of a worksite based walking programme on cardiovascular risk in previously sedentary civil servants [NCT00284479]. BMC Public Health. 2006;6:136.
Baker G, Gray SR, Wright A, Fitzsimons C, Nimmo M, Lowry R, et al. The effect of a pedometer-based community walking intervention “Walking for Wellbeing in the West” on physical activity levels and health outcomes: a 12-week randomized controlled trial. Int J Behav Nutr Phys Act. 2008;5:44.
Bell GJ, Harber V, Murray T, Courneya KS, Rodgers W. A comparison of fitness training to a pedometer-based walking program matched for total energy cost. J Phys Act Health. 2010;7:203–13.
Uchikawa Y, Miyai N, Ito K, Yabu M, Ishii A, Shibata M, et al. Effects of walking exercise on cardiovascular risk parameters and arterial stiffness in middle-aged and elder subjects. Jpn J Appl Physiol. 2010;40:185–92. (Japanese)
Serwe KM, Swartz AM, Hart TL, Strath SJ. Effectiveness of long and short bout walking on increasing physical activity in women. J Women’s Health (Larchmt). 2011;20:247–53.
Tully MA, Cupples ME. UNISTEP (university students exercise and physical activity) study: a pilot study of the effects of accumulating 10,000 steps on health and fitness among university students. J Phys Act Health. 2011;8:663–7.
Uchikawa Y, Nakamura C, Miyai N, Ito K, Ishii A, Utsumi M, et al. Effects of walking in sand-beach on novel risk factors of cardiovascular disease in metabolic syndrome - randomized control design. Heart. 2012;44:799–804. (Japanese)
Suboc TB, Strath SJ, Dharmashankar K, Coulliard A, Miller N, Wang J, et al. Relative importance of step count, intensity, and duration on physical activity’s impact on vascular structure and function in previously sedentary older adults. J Am Heart Assoc. 2014;3:e000702.
Ohta Y, Kawano Y, Minami J, Iwashima Y, Hayashi S, Yoshihara F, et al. Effects of daily walking on office, home and 24-h blood pressure in hypertensive patients. Clin Exp Hypertens. 2015;37:433–7.
Phing CH, Saad HA, Nisak MYB, Nasir MTM. Effectiveness of physical activity intervention among government employees with metabolic syndrome. J Exerc Sci Fit. 2017;15:55–62.
Laverty AA, Mindell JS, Webb EA, Millett C. Active travel to work and cardiovascular risk factors in the United Kingdom. Am J Prev Med. 2013;45:282–8.
Sun Q, Townsend MK, Okereke OI, Franco OH, Hu FB, Grodstein F. Physical activity at midlife in relation to successful survival in women at age 70 years or older. Arch Intern Med. 2010;170:194–201.
Huang B, Wu X. Pedometer algorithm research based-matlab. Adv Comput Sci Inform Eng. 2012;168:81–6.
Health Service Division, Health Servuce Bureau, Ministry of Health, Labour and Welfare of Japan. National Health and Nutrition Survey. Tokyo, Japan: Statistical Surveys conducted by Ministry of Health, Labour and Welfare; 2016.
Tudor-Locke C, Bassett DR Jr. How many steps/day are enough? Preliminary pedometer indices for public health. Sports Med. 2004;34:1–8.
Yates T, Haffner SM, Schulte PJ, Thomas L, Huffman KM, Bales CW, et al. Association between change in daily ambulatory activity and cardiovascular events in people with impaired glucose tolerance (NAVIGATOR trial): a cohort analysis. Lancet. 2014;383:1059–66.
Franklin SS, Gustin W 4th, Wong ND, Larson MG, Weber MA, Kannel WB, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation. 1997;96:308–15.
Avolio AP, Chen SG, Wang RP, Zhang CL, Li MF, O’Rourke MF. Effects of aging on changing arterial compliance and left ventricular load in a northern Chinese urban community. Circulation. 1983;68:50–8.
Igarashi Y, Akazawa N, Maeda S. Regular aerobic exercise and blood pressure in East Asians: A meta-analysis of randomized controlled trials. Clin Exp Hypertens. 2018;40:378–89.
Acknowledgements
A special thanks to the staff of Osaka University of Health and Sports Sciences Library collecting literatures for our analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Igarashi, Y., Akazawa, N. & Maeda, S. The required step count for a reduction in blood pressure: a systematic review and meta-analysis. J Hum Hypertens 32, 814–824 (2018). https://doi.org/10.1038/s41371-018-0100-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41371-018-0100-z
- Springer Nature Limited