
Abstract
Background
Evidence suggests that physical self-concept is associated with physical activity in children and adolescents, but no systematic review of this literature has been conducted.
Objective
The primary aim of this systematic review and meta-analysis was to determine the strength of associations between physical activity and physical self-concept (general and sub-domains) in children and adolescents. The secondary aim was to examine potential moderators of the association between physical activity and physical self-concept.
Methods
A systematic search of six electronic databases (MEDLINE, CINAHL, SPORTDiscus, ERIC, Web of Science and Scopus) with no date restrictions was conducted. Random effects meta-analyses with correction for measurement were employed. The associations between physical activity and general physical self-concept and sub-domains were explored. A risk of bias assessment was conducted by two reviewers.
Results
The search identified 64 studies to be included in the meta-analysis. Thirty-three studies addressed multiple outcomes of general physical self-concept: 28 studies examined general physical self-concept, 59 examined perceived competence, 25 examined perceived fitness, and 55 examined perceived appearance. Perceived competence was most strongly associated with physical activity (r = 0.30, 95 % CI 0.24–0.35, p < 0.001), followed by perceived fitness (r = 0.26, 95 % CI 0.20–0.32, p < 0.001), general physical self-concept (r = 0.25, 95 % CI 0.16–0.34, p < 0.001) and perceived physical appearance (r = 0.12, 95 % CI 0.08–0.16, p < 0.001). Sex was a significant moderator for general physical self-concept (p < 0.05), and age was a significant moderator for perceived appearance (p ≤ 0.01) and perceived competence (p < 0.05). No significant moderators were found for perceived fitness.
Conclusion
Overall, a significant association has been consistently demonstrated between physical activity and physical self-concept and its various sub-domains in children and adolescents. Age and sex are key moderators of the association between physical activity and physical self-concept.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
The results of this meta-analysis indicate a medium effect size relationship between general physical self-concept, perceived competence and perceived fitness and physical activity in young people |
General physical self-concept, perceived competence and perceived fitness may act as both determinants and outcomes of physical activity behaviour in youth |
Strategies to enhance physical self-perceptions in children and adolescents may assist in efforts to promote physical activity |
1 Introduction
The physical health benefits of physical activity are extensive and include reduced risk of coronary heart disease, type II diabetes, some cancers and osteoporosis, as well as improved physical fitness and bone strength [1, 2]. In addition, participation in physical activity may improve psychological health and help prevent and treat the development of mental health disorders such as depression and anxiety [3–5]. Mental health disorders represent a significant public health burden [6, 7], yet mental health is not only the absence of a mental disorder but a state of psychological well-being in which individuals realise their own ability and potential [8]. The self-concept construct is vital to psychological well-being [9] and is the term used to describe an individual’s awareness of their qualities and limitations [10]. Individuals who feel good about themselves and their abilities are resilient to the challenges of life, and self-concept facilitates other aspects of well-being, including happiness, motivation, and anxiety [9]. A hierarchical organisation of general self-concept has been posited by Shavelson et al. [10], with general self-concept at the apex that includes academic and non-academic sub-domains. Academic self-concept consists of subject-specific facets of self (e.g. english, history and mathematics) [11], while the non-academic sub-domain is further divided into social, emotional and physical self-concepts. Physical self-concept (sometimes referred to as physical self-perceptions) is then separated into perceived physical ability and perceived physical appearance [10].
Although known by different names, perceived physical ability (or competence) is considered to be a central determinant of behaviour and is included in prominent social cognitive theories, including competence motivation theory (perceived competence) [12], self-determination theory (competence) [13], social cognitive theory (self-efficacy) [14] and theory of planned behaviour (perceived behavioural control) [15]. In the physical activity domain, perceived competence is generally operationalised as confidence to perform sport and outdoor games [16], while perceived behavioural control and self-efficacy are defined as confidence to overcome barriers to participation. Self-efficacy, perceived competence and perceived behavioural control are three of the most commonly measured psychological correlates of physical activity and there is evidence for their utility as determinants of behaviour [17–20]. Indeed, in a recent review of reviews, Bauman et al. [17] described health status and self-efficacy as the ‘clearest correlates’ of physical activity in adults. The same authors concluded that perceived behavioural control and self-efficacy were the strongest psychological determinants of physical activity in adolescents, but did not find sufficient evidence that perceived competence was a determinant of behaviour.
In contrast to social cognitive models, the exercise and self-esteem model (EXSEM) [21] was developed to explore the pathways by which self-esteem is influenced by physical training. Based on Shavelson’s hierarchical organisation of general self-concept [10], the model proposes that confidence in one’s abilities to perform specific exercises and sports-related activities generalise to a broader perceived physical competence [22]. Therefore, in this model, self-efficacy to complete specific exercise-related tasks is considered an outcome rather than a determinant of activity. More recently, Stodden et al. proposed a conceptual model that positioned perceived competence as a mediator of the association between motor skill competence and physical activity [23]. In their model, motor skill competence was considered to be the “primary underlying mechanism that promotes engagement in physical activity”, with perceived competence playing an increasingly important role as children develop the cognitive skills to accurately differentiate between actual and perceived motor competence [24, 25].
In summary, it is not clear if general physical self-concept and sub-domains are outcomes, mediators or moderators of physical activity in young people [26]. Numerous studies have modelled physical self-concept and sub-domains as determinants of physical activity [27–32], while others have explored the impact of exercise and physical activity programmes on physical self-perceptions [33, 34]. However, no previous review has systematically evaluated the evidence for the association between physical activity and physical self-concept in children and adolescents. Providing a summary of existing studies may assist in the design of physical activity interventions and/or provide evidence for the positive effects of physical activity on well-being. Therefore, the primary aim of this systematic review and meta-analysis was to determine the association between physical activity and physical self-concept in young people by reviewing cross-sectional, experimental and longitudinal studies. The secondary aim of this review was to examine potential moderators of the association between physical activity and physical self-concept.
2 Methods
2.1 Eligibility Criteria
A study was considered eligible for this review if it met the following inclusion criteria: (a) study included quantitative assessment of leisure-time physical activity. Physical activity was defined as “body movement produced by the skeletal muscles which results in a substantial increase over the resting energy expenditure” [35]; (b) study included the quantitative assessment of physical self-concept or sub-domains; (c) study included a quantitative assessment of the association between physical activity and physical self-concept or sub-domains; (d) study participants were school-aged children or adolescents (i.e. aged 4–20 years); (e) published full text and peer reviewed. For a study to be included in the meta-analysis it was required to report a correlation coefficient or standardised regression coefficient for the association between physical activity and physical self-concept or sub-domains (studies that did not provide this information but examined the association between physical activity and physical self-concept are included in the electronic supplementary material [ESM] Table S1).
Excluded studies were those which (a) were published in languages other than English; (b) reported only qualitative data; (c) included participants who were targeted groups from special populations (e.g. people with mental illness, psychiatric disorders, developmental delays and developmental co-ordination or eating disorders); and (d) conference abstracts, dissertations, thesis or non-peer-reviewed studies. Finally, studies examining the impact of physical activity programmes on physical self-concept or sub-domains were not included if they did not examine the association between changes in physical activity and changes in self-perceptions.
To allow for the aggregation of findings, scales/questionnaires assessing similar constructs of different names were combined in the meta-analyses. For example, ‘perceived appearance’ was presented in different studies as body image, body attractiveness, body esteem. All of these constructs were considered to represent an individual’s assessment of their body size and/or shape, with a higher score representing a more positive self-evaluation. ‘Perceived competence’ was operationally defined as an individual’s assessment of their ability to perform sports and recreational activities. Although related to perceived confidence, ‘perceived fitness’ was operationalised as an individual’s evaluation of their health-related physical fitness. Validation studies of commonly used scales, including the Physical Self-Perception Profile and the Physical Self-Description Questionnaire (PSDQ) have demonstrated that perceptions of fitness are unique constructs [36, 37]. Scales assessing the different components of physical fitness (i.e. strength, endurance, flexibility) were combined for the meta-analyses.
2.2 Search Strategy
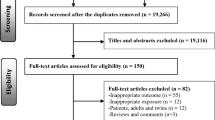
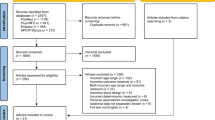
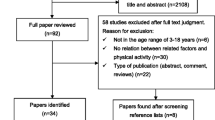
The literature search was conducted on the 3 August 2013. Studies were identified through a structured electronic database search of the following databases: MEDLINE, CINAHL, SPORTDiscus, ERIC, Web of Science and Scopus. Search terms included a combination of key words including: (‘Physical activit*’ OR exercise OR active OR motor*) AND (adolescence OR teenage OR children OR student OR youth OR boy OR girl) AND (Adoles* OR teen* OR child* OR student OR youth OR boy OR girl OR school OR primary OR elementary OR high OR secondary OR grade) AND (‘physical self-concept’ OR ‘physical self-worth’ OR perceived competence OR ‘physical self-perception’ OR ‘physical appearance’ OR body image). The strings were further limited to those aged 5–20 years and English language. Only articles published in peer-reviewed journals were considered. The search was executed by MB with the assistance of a professional librarian; reference lists of included studies were manually cross-referenced for possible additional studies. The literature search was conducted in accordance with the standards applicable in the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analysis’ (PRISMA) statement [38] (Fig. 1). The PRISMA checklist has also been provided (ESM Table S2).

Results of the literature search
2.3 Screening
Two authors (MB and RW) independently assessed each identified study for relevance to the review based on the title, abstract, and full text. In the event of a disagreement, consensus was reached by discussion with a third member (DRL). In the first stage, studies were screened based on title and abstract. Relevant full-text articles were searched and evaluated for inclusion. Reference lists of included studies were reviewed for potential papers.
2.4 Data Extraction
The extracted data included authors, country in which the study was conducted, sample (number, age, and sex), study design, location, measure of physical activity, measure of physical self-concept, reliability of tools, outcomes, the intervention (dose and length), year of publication, sample size, and number/percentages of males/females (where provided). When details of mean age were not available, an average was calculated from the age range provided. If a study used more than one physical activity variable, the variable that was most closely aligned with the following definition: ‘meeting physical activity guidelines during leisure time’ was used [39]. As studies often included multiple statistical analyses (e.g. correlation, multiple regression), the results from the highest level of analysis were used (i.e. multivariate analyses, or analyses that accounted for potential confounders, were favoured over bivariate analyses). For example, if a study reported both bivariate correlations and multiple regression models, results from the regression models were included in the meta-analysis. If a study reported both longitudinal and cross-sectional results, the longitudinal findings were included in the meta-analysis. This was performed to avoid the double counting of studies and because longitudinal study designs are considered to provide a more robust test of theory [40].
2.5 Analytic Strategies
Meta-analyses were conducted using the Comprehensive Meta-Analysis (CMA) Version 2 software program (Englewood, NJ, USA) [41]. Effect sizes for each study were calculated before and after correcting for measurement error. Measurement error procedures were based on the reliabilities of the measures as presented in the study or from prior published literature with the same instrument. In cases with single items or where reliabilities were not reported, we used rxy = 0.70 based on a conservative, yet acceptable, judgement of reliability [42]. In cases where coefficients had already been corrected (e.g. structural equation models), no additional correction procedures were used.
The general aim of a meta-analysis is to provide a more powerful estimate of the effect size (or associations between variables) than what can be achieved in a single study under a specific set of assumptions and conditions. Two types of statistical models are used to create weighted averages when conducting meta-analyses. The fixed-effects model assumes that sampling error accounts for differences in the observed effects, while random-effects models produce within-study (sampling) and between-studies (variance) [43]. Random-effects models are considered more appropriate when data are heterogeneous [43, 44]; however, both models are reported in the current review for comparative purposes. Along with the weighted average effect sizes, we computed the 95 % confidence intervals (CI). If the CI does not include zero, then the effect size is statistically significant at the p < 0.05 level. Correlations between variables were interpreted as follows: 0.1–0.29 (weak), 0.3–0.49 (moderate) and 0.5–1.0 (strong) [1].
Rosenthal’s classic fail-safe N [45] and Duval and Tweedie’s ‘trim and fill’ procedure [46, 47] were used to assess the extent of publication bias. Rosenthal’s classic fail-safe provides an indication of the number of studies needed with a mean effect of zero before the overall effect would no longer be statistically significant. Alternatively, the ‘trim and fill’ procedure selectively removes extreme effect sizes from small studies and replaces them with imputed values to produce a more symmetrical funnel plot, which generates a less biased overall effect size [46, 47].
Separate meta-analyses were carried out for (i) general physical self-concept; (ii) perceived competence; (iii) perceived fitness; and (iv) perceived appearance. Studies that were separated by sex and/or cohort years were treated as separate studies in the meta-analysis. We report the weighted average effect sizes and the 95 % CIs. The Q and I 2 statistics were calculated to determine the heterogeneity of the average effect sizes. Q tests are used to determine if the observed variance in effect sizes is no greater than what is expected by sampling error alone, while the I 2 statistic (I 2 = 100 % × (Q − df)/Q) is used to quantify the degree of heterogeneity [48]. The I 2 value provides the percentage of total variation across studies due to heterogeneity [48] rather than chance. A value of 0 % indicates no observed heterogeneity, while larger values indicate increasing heterogeneity. Based on existing recommendations, I 2 values of 25, 50 and 75 % were considered low, moderate and high, respectively [48].
Subgroup moderator analyses are conducted in meta-analyses to offer an understanding of the strength and/or direction of association between independent and dependent variables [45]. Moderator analyses were also conducted using corrected r’s and random-effects models. The following demographic and methodological variables were tested as potential moderators: (i) sex (i.e. girls only, boys only and mixed); (ii) age (i.e. childhood, early adolescence and late adolescence); and (iii) study design (i.e. cross-sectional, experimental, and longitudinal). Age was categorised according to definitions from the World Health Organisation, childhood (pre 10 years), early adolescence (10–14 years) and late adolescence (15–19 years) [49]. For the moderator analysis, we used Q B to explore the impact of the categorical variables on the effect size. Q B is used for testing the differences between effect sizes.
2.6 Synthesis of Studies Not Included in the Meta-Analysis
A synthesis of studies not included in the meta-analysis was conducted. Results were coded using the method first employed by Sallis et al. [49]. If 0–33.3 % of studies reported a significant association, results were classified as having no association (0). If 34–59 % of studies reported a significant association or if fewer than four studies were included, the results were classified as being inconsistent/uncertain (?). If >60 % of studies found a significant association, the results were classified as positive (+) or negative (−), depending on the direction of the association. If studies employed multiple analyses, only findings from the highest level of analysis (i.e. multivariate) were considered.
2.7 Criteria for Risk of Bias Assessment
The PRISMA statement recommends that systematic reviews include an evaluation of the methodological risks of bias that may have a bearing on the individual study findings [50]. Potential risk of bias will depend upon the study design and objectives. For example, the Cochrane risk of bias tool [51] consists of five items that are known to influence the estimates of an intervention’s effectiveness in randomised controlled trials, and includes items relating to sequence generation, allocation concealment blinding, treatment of outcome data and selective outcome reporting. Two authors (MB and RW) independently assessed the ‘risk of bias’ of the included studies using methodological items and coding. Studies were assessed for ‘risk of bias’ using criteria adapted from research reviewing the associations between sedentary behaviour and health indicators [52]. A ‘risk of bias’ score for each study was completed on a 5-point scale by assigning a ‘✓’ if the study met the criteria or a ‘✗’ if the study failed to meet the criteria (ESM Table S3).
The studies were examined based on criteria which included the following: (a) Study schools and/or participants were randomly selected from the target population (for experimental studies, the process of randomisation was clearly described and adequately carried out). A ‘✓’ was awarded if the sample was randomly selected from the target population or participants were randomly allocated to conditions for experimental studies. A ‘✗’ was given if convenience sampling was used or if the process of randomisation was not adequately described. (b) Adequate description of baseline study sample (individuals entering the study) for key demographic characteristics (number of participants and their mean age (or age range) and sex). A ‘✓’ was awarded if the study reported the proportion of males and females and age range and/or mean for participants. A ‘✗’ was given if the study provided only one or no characteristic(s). (c) Adequate assessment of physical self-concept and sub-domains (if used). A ‘✓’ was awarded if authors reported at least one ‘acceptable’ reliability statistic for all physical self-concept measures (e.g. Cronbach alphas of ≥0.70 or test-retest reliability intraclass correlation coefficient, which describes how strongly units in the same group resemble each other, of ≥0.70), or uses an established method. A ‘✗’ was given if a single-item measure was used or the study did not report reliability statistics. (d) Adequate assessment of physical activity. A ‘✓’ was awarded if objective measures were used (i.e. heart rate monitors, accelerometers, pedometers, direct observations) or if authors cited adequate validity data for self-report measures in the study population. A ‘✗’ was given for self-report measures when authors did not report validity data. A ‘✗’ was also given if the validity being measured was related to fitness and not physical activity. (e) Appropriate adjustment for covariates (i.e. age and sex) in the statistical analysis (exploring the association between physical activity and physical self-concept). A ‘✓’ was awarded if authors adjusted for age or pubertal status, or if authors reported separate findings for boys and girls and different age groups (if students were from the same grade at school this was considered acceptable). A ‘✗’ was given if authors did not adjust for age and sex.
2.8 Description of the Synthesis of Studies Not Included in the Meta-Analysis
A synthesis of studies not included in the meta-analysis was conducted. Of the 47 studies, 29 were cross-sectional, 8 were experimental and 10 were longitudinal. Results were coded using the method employed by Sallis et al. [20]. If 0–33.3 % of studies reported a significant association, results were classified as having no association (0). If 34–59 % of studies reported a significant association or if fewer than four studies were included, the results were classified as being inconsistent/uncertain (?). If >60 % of studies found a significant association, the results were classified as positive (+) or negative (−), depending on the direction of the association. If studies employed multiple analyses, only findings from the highest level of analysis (i.e. multivariate) were considered.
3 Results
The literature search yielded a total of 4,666 potentially relevant citations (Fig. 1). Following screening procedures, 332 full-text articles were retrieved and reviewed. A total of 111 were considered eligible for the review. A total of 64 studies were included in the meta-analysis, consisting of 47 cross-sectional, 12 longitudinal and 5 experimental studies.
3.1 Study/Sample Characteristics
In terms of country the study was conducted, the US provided 17 studies, England 12, Australia 7, Canada 5, UK 4, Spain, Finland and Sweden provided 2 each, and Taiwan, Hong Kong, Mexico, Norway, Germany, Scotland, Cyprus, Poland, Jamaica, Greece, Estonia, Italy and China had a single study included (ESM Table S1). A total of 167 independent samples were used in the meta-analysis, which included data from 24,546 girls, 15,215 boys (the sex of 7,130 participants was not specified).
3.2 Overall Effect Size, Heterogeneity and Significance of Moderators
3.2.1 General Physical Self-Concept
After correcting for measurement error, the random-effects model yielded a weak to moderate effect size of r = 0.25 (95 % CI 0.16–0.34, p < 0.001), suggesting that higher physical activity levels were associated with higher levels of general physical self-concept (ESM Fig. S1). Sex emerged as a statistically significant moderator of effects (p < 0.05). Results by sex category were r = 0.40 (95 % CI 0.32–0.48, p < 0.001) for boys (4 studies), r = 0.26 (95 % CI 0.16–0.36, p < 0.001) for girls (15 studies) and r = 0.20 (95 % CI −0.01 to 0.39, p > 0.05) for the mixed sample (9 studies).
Study design and age were not significant moderators of effects (p > 0.5). This is because the association between general physical self-concept and physical activity was not significantly different between subgroups (e.g. the effect size estimates were similar for cross-sectional, experimental and longitudinal study designs). Results by study design category were r = 0.25 (95 % CI 0.13–0.36, p < 0.001) for cross-sectional designs, r = 0.27 (95 % CI 0.11–0.42, p < 0.001) for longitudinal designs and r = 0.30 (95 % CI 0.12–0.47, p < 0.005) for experimental designs. Results by age category were r = 0.26 (95 % CI 0.15–0.37, p < 0.001) for early adolescence (23 studies) and r = 0.22 (95 % CI 0.04–0.40, p < 0.05) for late adolescence (5 studies).
3.2.2 Perceived Competence
The random-effects model correcting for measurement error revealed a moderate effect size of r = 0.33 (95 % CI 0.27–0.39, p < 0.001) [ESM Fig. S2]. Age emerged as a statistically significant moderator of effects (p < 0.05) and a total of 59 samples were extracted. Of these, 1 involved children, 45 included early adolescents, and 13 studies included late adolescents. Results by age category were r = 0.08 (95 % CI −0.12 to 0.28, p < 0.5) for children, r = 0.35 (95 % CI 0.28–0.42, p < 0.001) for early adolescents and r = 0.31 (95 % CI 0.19–0.41, p < 0.001) for late adolescents.
Sex and study design were not significant moderators of effects (p > 0.5). A total of 59 samples were extracted. Results by sex category were r = 0.32 (95 % CI 0.19–0.45, p < 0.001) for boys, r = 0.33 (95 % CI 0.23–0.42, p < 0.001) for girls and r = 0.35 (95 % CI 0.25–0.43, p < 0.001) for the mixed sample. Results by study design category were r = 0.32 (95 % CI 0.24–0.39, p < 0.001) for cross-sectional designs, r = 0.34 (95 % CI 0.24–0.43, p < 0.001) for longitudinal designs and r = 0.66 (95 % CI 0.31–0.85, p < 0.001) for experimental designs.
3.2.3 Perceived Fitness
Higher levels of perceived fitness were moderately associated with increased physical activity in the random-effects model, r = 0.30 (95 % CI 0.23–0.36, p < 0.001) [ESM Fig. S3]. Sex, age and study design were not moderators of the association (p > 0.05). Results by sex category were r = 0.40 (95 % CI 0.32–0.48, p < 0.001) for boys, r = 0.30 (95 % CI 0.23–0.37, p < 0.001) for girls and r = 0.25 (95 % CI 0.02–0.45, p < 0.05) for the mixed sample. Results by age category were r = 0.31 (95 % CI 0.24–0.37, p < 0.001) for early adolescents and r = 0.28 (95 % CI 0.13–0.42, p < 0.001) for late adolescents. Results by study design category were r = 0.32 (95 % CI 0.25–0.39, p < 0.001) for cross-sectional designs and r = 0.21 (95 % CI 0.07–0.34, p < 0.01) for longitudinal designs.
3.2.4 Perceived Appearance
After correcting for measurement error, the random-effects model revealed a weak association between perceived appearance and physical activity, r = 0.14 (95 % CI 0.09–0.18, p < 0.001) [ESM Fig. S4]. Age emerged as a statistically significant moderator of effects (p < 0.01). A total of 55 samples were extracted and, of these, 33 and 22 involved early adolescents and adolescents, respectively. The effect size for early adolescents was r = 0.19 (95 % CI 0.13–0.24, p < 0.001) and for late adolescents was r = 0.07 (95 % CI 0.01–0.13, p < 0.05).
Sex and study design were not significant moderators of effects (p > 0.5). Results by sex category were r = 0.13 (95 % CI 0.03–0.24, (p < 0.05) for boys, r = 0.13 (95 % CI 0.07–0.19, p < 0.001) for girls and r = 0.16 (95 % CI 0.06–0.25, p < 0.001) for the mixed sample. Results by study design category were r = 0.14 (95 % CI 0.09–0.18, p < 0.001) for cross-sectional designs, r = 0.16 (95 % CI 0.11–0.21, p < 0.001) for longitudinal designs and r = 0.13 (95 % CI −0.09 to 0.33, p > 0.05) for experimental designs.
3.3 Synthesis of Findings Not Included in the Meta-Analysis
Overall, there were consistent positive associations between physical activity and physical self-concept and its sub-domains. The summary of findings is reported in Table 1.
3.4 Risk of Bias Assessment
Inter-rater reliability metrics for the risk of bias assessments indicated adequate percentage of agreement (94 %) for the 320 items (ESM Table S3). Thirteen studies (20 %) provided an adequate description of the random sampling process, 59 studies (92 %) provided an adequate description of the study sample, 63 studies (98 %) provided a valid measure of physical activity, 47 studies (73 %) provided a valid measure of physical self-concept and 17 studies (27 %) adjusted for covariates.
3.5 Testing for Publication Bias
The classic fail-safe N was high for general physical self-concept (N = 3,909), perceived competence (N = 89,188), perceived fitness (N = 3,450) and perceived appearance (N = 2,932). Therefore, a large number of studies with a mean effect of zero would be necessary before the overall effects found in the present study would become not statistically significant. Thus, the significant associations observed in these meta-analyses are likely not the result of publication bias towards significant findings.
In addition, Duval and Tweedie’s ‘trim and fill’ procedure [46, 47] was used to compute a random-effects estimate of the unbiased effect size. No studies were trimmed for either perceived fitness or perceived appearance; however, 2 studies were trimmed for general physical self-concept and 18 were trimmed for perceived competence. The general physical self-concept meta-analysis trimmed for extreme values (2 studies) had little impact on the overall estimate, while the trimmed perceived competence meta-analysis (18 studies) resulted in a weaker effect size of r = 0.22 (95 % CI 0.15–0.29). This finding suggests there is evidence of publication bias that contributed to the observed overall effect size for the association between perceived competence and physical activity.
4 Discussion
4.1 Overview of Findings
The findings from this systematic review and meta-analysis suggest that young people with stronger beliefs about their physical characteristics are more likely to engage in physical activity than those who report lower levels of physical self-concept [96, 97]. However, it is not clear if participation in physical activity leads to improvements in physical self-concept or those with high levels of physical self-concept are attracted to physical activity. Notably, the strength of association between physical activity and physical self-concept (and sub-domains) did not upon depend upon how the data was treated (i.e. whether physical self-concept was the dependent or independent variable) and there is conflicting evidence in the literature regarding associations of this nature. For example, according to the model proposed by Stodden et al. [96, 97], perceived competence is a mediator of the relationship between motor skill competence and physical activity. The model describes two different spirals—one for those who are active with high levels of perceived and actual motor skill competence, and another for those who live sedentary lifestyles and possess low levels of competency. As children grow, the divide increases, with a positive spiral of engagement leading to higher physical activity levels and a negative spiral of disengagement contributing to physical inactivity.
Alternatively, the EXSEM considers self-efficacy or perceived competence in exercise and sport-related tasks as outcomes of participation. Although there is sufficient evidence from our review and previous studies to conclude that there is a bi-directional association between physical activity and physical self-concept, researchers working in this area are encouraged to conduct mediation analyses to assist in unravelling the nature of the association between physical self-concept and physical activity. Furthermore, separate analyses that model the bidirectional nature of general physical self-concept and its sub-domains as both mediators and moderators of physical activity are needed.
The meta-analysis effect sizes from the current review are similar, but slightly smaller, than those found in previous reviews examining the effects of exercise on self-esteem in young people [98] and adults [99]. While it is plausible to suggest that larger associations would be observed between physical activity and physical self-concept, compared with global self-esteem which is both more stable and distal from the impact of physical activity [21], both previous reviews were focused on the effects of participation in structured exercise programmes. Exercise is planned and repetitive bodily movement done to improve or maintain health-related fitness [100] and, according to the EXSEM, individuals who experience improvements in fitness should also experience changes in global self-esteem (via changes in physical self-perceptions which are more proximal to exercise participation). In contrast, the current review was designed to examine the association between leisure-time physical activity and physical self-concept. Physical activity measures capture a range of organised and non-organised activities and, in the case of objective measures such as accelerometers and pedometers, also collect incidental and lifestyle physical activity (e.g. walking and riding for transportation); however, these behaviours (e.g. walking) may not require much in the way of perceived competence. Overall, the findings of this systematic review suggest that physical self-concept is important for physical activity in young people and the sub-domains of physical self-concept may play a unique role.
4.2 Summary of Risk of Bias from Included Studies
The findings of this review should be interpreted with some caution as 54 (84 %) of the included studies were found to have a high risk of bias. It is a concern that the majority of studies assessed physical activity using a self-report measure. Self-report of physical activity can suffer from reporting bias [70], attributable to a combination of social desirability bias and the cognitive challenges associated with estimating frequency and duration of physical activity, especially in children [71]. Furthermore, common method artefact may result in stronger correlation coefficients, when two outcomes are measured using the same method of assessment (i.e. self-report) [101]. In addition, few of the studies included participants who were randomly selected from nationally representative populations, which may limit the generalisability of our findings. Only a small percentage of studies adjusted for relevant covariates, which may confound the association between physical self-concept and physical activity. Finally, most of the studies included in this review were cross-sectional, and while a number of longitudinal studies were included, such studies do not provide the same level of evidence generated from experimental studies.
4.3 Major Findings and Potential Contributors
This is the first systematic review and meta-analysis of studies examining the association between physical activity and physical self-concept in children and adolescents. The findings suggest that general physical self-concept and its sub-domains (i.e. perceived competence, perceived fitness and perceived appearance) are significantly associated with physical activity in young people. Sex was a significant moderator of the association between physical activity and general physical self-concept, with stronger associations found for boys. Age was also a significant moderator of the association between physical activity and perceived competence and perceived appearance. Notably, study design did not emerge as a significant moderator of the association between physical activity and physical self-concept or any of its sub-domains. Due to the small number of experimental studies, it is not possible to determine if the findings from experimental studies were significantly different to cross-sectional and longitudinal studies.
Perceived competence was found to have the strongest association with physical activity, and age emerged as a significant moderator, with the strongest association found in early adolescents. Evidence suggests that young children do not possess the cognitive skills to accurately assess their motor-skill competence. As a result, young children often report inflated levels of perceived competence [24, 25, 54], which may explain the weak associations found among children in our review. Stodden et al. [23] suggest that perceived motor skill competence will not be strongly correlated to actual levels of motor skill competence or physical activity during the early childhood years, but by middle childhood they will develop a “sophisticated cognitive capacity to more accurately compare themselves to their peers”. Alternative explanations for the moderating effects of age should be considered as the association between perceived competence and physical activity was slightly weaker in late adolescents. As children progress into adolescence, traditional team sports become less important as young people are exposed to, and participate in, more lifelong physical activities (e.g. resistance training, walking, aerobics, etc.) [1]. Many lifelong activities are attractive to young people, especially those with low levels of perceived competence, because they do not require competence in fundamental and sports-specific movement skills [102]. As many perceived competence scales include items focused on proficiency in traditional team sports, they may not capture adolescents’ perceptions of their abilities in non-traditional physical activities. Such activities make an increasingly important contribution to adolescents’ leisure-time physical activity [23, 86, 96].
Perceived fitness was found to have the second strongest association with physical activity in children and adolescents. Perceived fitness may be amenable to change, and experimental studies have demonstrated that well-designed physical activity or exercise programmes can increase perceived fitness in adolescents [31, 32, 58]. However, these studies were not included in the meta-analysis because they did not examine the association between changes in physical activity and changes in physical self-perceptions. Studies often report the association between changes in physical self-concept and actual fitness [58]; however, physical activity and fitness are only weakly related in young people [59, 60]. Research examining the association between changes in physical self-concept and changes in both fitness and behaviour is warranted. Increasing perceived fitness may have utility as a strategy for increasing physical activity levels in young people, but further testing of this hypothesis in experimental studies is required. Notably, none of the hypothesised moderators were statistically significant.
Perceived appearance was found to have the weakest association with physical activity in the current review. Age was a significant moderator of this association, with the strongest associations found in young adolescents. A recent longitudinal study found that the association between physical activity and perceived body attractiveness weakened over the 12-month study period in a sample of adolescent girls [61]. This finding suggests an increasing divergence between girls’ perceptions of their appearance and their involvement in physical activity as they progress through adolescence [62]. Such results may be attributable to bodily changes and increases in body fat that occur with maturation (i.e. through puberty) [62]. Although it is possible that perceived appearance becomes less important to adolescent girls over time, it is likely that this finding reflects an increasing dissatisfaction with their bodies and a disconnect between their actual body shape and their perceived body shape [63–65, 103]. For example, a recent nationally representative sample of French adolescents found that one-third of adolescents misperceived their body weight and that girls were more likely to overestimate their body weight than boys. This possibility is alarming and provides further support for the importance of enhancing adolescent girls’ acceptance of their bodies in attempts to promote physical activity [66, 67].
4.4 Practical Implications
Evidence from this systematic review and meta-analysis suggests that physical self-perceptions (both general and sub-domains), are important for physical activity participation in young people. Although it remains unclear if physical self-perceptions are mediators or outcomes, there is sufficient evidence to suggest that physical activity interventions may benefit from strategies designed specifically to enhance physical self-concept. While it may not be possible to specifically target general physical self-concept, learning experiences and teaching styles that promote a mastery climate may assist in developing both perceived and actual motor skill competence [104–106]. Furthermore, exercise programmes that include fitness education, where students learn about the effects of physical activity on fitness and help children link health-related fitness to present and future health status, can improve perceived and actual fitness levels in young people [107, 108]. Fitness testing has an important role to play in this process, but it is important that those administering tests use appropriate methods that minimise adverse reactions to fitness testing and maximise effort, enjoyment and motivation in young people [109].
4.5 Strengths and Limitations of the Review
The strengths of this review include adherence to the PRISMA statement, the large number of studies identified and the inclusion of meta-analyses. Despite these strengths, some limitations should be noted. First, although this review was comprehensive, we did not include studies that were published in languages other than English and we did not include unpublished studies. Second, we did not include studies that examined the association between physical fitness and physical self-concept as this was considered beyond the scope of the already extensive review. Third, the definition and assessment of physical self-concept and sub-domains was not consistent across studies. For example, the global physical self-concept subscale from the PSDQ [110] includes items that require respondents to evaluate how they feel about themselves in the physical domain (e.g. I feel good about who I am and what I can do physically). For the purpose of our review, we did not exclude studies that described their measure as a physical self-concept scale, but included items that measured physical self-esteem. Additionally, most of the studies published to date on this topic are cross-sectional or longitudinal, and such studies do not provide the same level of evidence generated from experimental studies.
5 Conclusions
The results of this systematic review and meta-analysis have demonstrated a significant association between physical activity and physical self-concept in youth. However, due to study heterogeneity and the high risk of bias observed in the included studies, these findings should be interpreted with caution. Although we were unable to establish causality, strategies to increase physical self-concept and sub-domains, particularly perceived physical fitness and competence, may have a role to play in promoting physical activity in young people. In addition, these results highlight the importance of understanding the physical-self and its links to health-related behaviours in youth. Further studies are needed to determine the mechanisms responsible for the effects of physical activity on physical self-concept.
References
Strong WB, Malina RM, Blimkie CJ, et al. Evidence based physical activity for school-age youth. J Pediatr. 2005;146(6):732–7.
Janssen I, LeBlanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7(40):1–16.
Ströhle A. Physical activity, exercise, depression and anxiety disorders. J Neural Transm. 2009;116(6):777–84.
Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. 2011;45(11):886–95.
Brown HE, Pearson N, Braithwaite RE, et al. Physical activity interventions and depression in children and adolescents. Sports Med. 2013;43(3):195–206.
Viner R, Booy R. Epidemiology of health and illness. BMJ. 2005;330(7488):411–4.
Patel V, Flisher AJ, Hetrick S, et al. Mental health of young people: a global public-health challenge. Lancet. 2007;369(9569):1302–13.
World Health Organisation. The world health report 2001: mental health: new understanding, new hope (online). http://apps.who.int/iris/bitstream/10665/42390/1/WHR_2001.pdf (2001). Accessed 15 Feb 2014.
Craven RG, Marsh HW. The centrality of the self-concept construct for psychological wellbeing and unlocking human potential: implications for child and educational psychologists. Educ Child Psychol. 2008;25(2):104–18.
Shavelson RJ, Hubner JJ, Stanton GC. Self-concept: validation of construct interpretations. Rev Educ Res. 1976;46(3):407–41.
Marsh HW. Age and sex effects in multiple dimensions of self-concept: preadolescence to early adulthood. J Educ Psychol. 1989;81(3):417.
Weiss MR. Motivating kids in physical activity. Pres Counc Phys Fit Sports Res Dig. 2000;3(11):1–8.
Deci EL, Ryan RM. Handbook of self-determination research. Rochester: University Rochester Press; 2002.
Bandura A. Social foundations of thought and action: a social cognitive theory. Englewood Cliffs, N.J: Prentice-Hall; 1986.
Ajzen I. From intentions to actions: a theory of planned behavior. Berlin: Springer; 1985.
Harter S. The perceived competence scale for children. Child Dev. 1982;53(1):87–97.
Bauman AE, Reis RS, Sallis JF, et al. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380(9838):258–71. doi:10.1016/S0140-6736(12)60735-1.
Biddle SJH, Whitehead SH, O’Donovan TM, et al. Correlates of participation in physical activity for adolescent girls: a systematic review of recent literature. J Phys Act Health. 2005;2(4):423.
Van der Horst K, Paw M, Twisk JWR, et al. A brief review on correlates of physical activity and sedentariness in youth. Med Sci Sports Exerc. 2007;39(8):1241–50.
Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32(5):963–75.
Sonstroem RJ, Morgan WP. Exercise and self-esteem: rationale and model. Med Sci Sports Exerc. 1989;21(3):329-37.
Sonstroem RJ, Harlow LL, Josephs L. Exercise and self-esteem: validity of model expansion and exercise associations. J Sports Exerc Psychol. 1994;16(1):29–42.
Stodden DF, Goodway JD, Langendorfer SJ, et al. A developmental perspective on the role of motor skill competence in physical activity: an emergent relationship. Quest. 2008;60(2):290–306.
Harter S. The construction of the self: a developmental perspective. New York: Guilford Press; 1999.
Harter S, Pike R. The pictorial scale of perceived competence and social acceptance for young children. Child Dev. 1984;55:1969–82.
Marsh HW, Papaioannou A, Theodorakis Y. Causal ordering of physical self-concept and exercise behavior: reciprocal effects model and the influence of physical education teachers. Health Psychol. 2006;25(3):316–28. doi:10.1037/0278-6133.25.3.316.
Annesi JJ. Relations of physical self-concept and self-efficacy with frequency of voluntary physical activity in preadolescents: implications for after-school care programming. J Psychosom Res. 2006;61(4):515–20.
Annesi JJ, Faigenbaum AD, Westcott WL, et al. Relations of self-appraisal and mood changes with voluntary physical activity changes in African American preadolescents in an after-school care intervention. J Sports Sci Med. 2008;7(2):260–8.
Craft LL, Pfeiffer KA, Pivarnik JM. Predictors of physical competence in adolescent girls. J Youth Adolesc. 2003;32(6):431–8. doi:10.1023/a:1025986318306.
Crocker P, Sabiston C, Kowalski K, et al. Longitudinal assessment of the relationship between physical self-concept and health-related behavior and emotion in adolescent girls. J Appl Sports Psychol. 2006;18(3):185–200.
Crocker PR, Eklund RC, Kowalski KC. Children’s physical activity and physical self-perceptions. J Sports Sci. 2000;18(6):383–94.
Crocker P, Sabiston C, Forrestor S, et al. Predicting change in physical activity, dietary restraint, and physique anxiety in adolescent girls: examining covariance in physical self-perceptions. Can J Public Health. 2003;94(5):332–7.
Lubans DR, Aguiar E, Callister R. The effects of free weights and elastic tubing resistance training on physical self-perception in adolescents. Psychol Sport Exerc. 2010;11(6):497–504.
Velez A, Golem DL, Arent SM. The impact of a 12-week resistance training program on strength, body composition, and self-concept of Hispanic adolescents. J Strength Cond Res. 2010;24(4):1065–73.
Bouchard C, Shephard RJ, Stephens T. Physical activity, fitness, and health: international proceedings and consensus statement. Toronto (ON): Human Kinetics Publishers; 1994.
Fox K, Corbin C. The physical self- perception profile: development and preliminary validation. J Sport Exerc Psychol. 1989;11(1):408–30.
Marsh HW. Physical self-description questionnaire: stability and discriminant validity. Res Q Exerc Sport. 1996;67(3):249–64.
Moher D, Liberati A, Tetzlaff J, et al. Reprint—preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. 2009;89(9):873–80.
Nasuti G, Rhodes RE. Affective judgment and physical activity in youth: review and meta-analyses. Ann Behav Med. 2013;45(3):357–76.
Johnson SL. Research and statistics a question of time: cross-sectional versus longitudinal study designs. Paediatr Rev. 2010;31(6):250–1.
Borenstein M, Hedges L, Higgins J, et al. Comprehensive meta-analysis version 2. Englewood, NJ: Biostat; 2005.
Cohen J, Cohen P. Applied multiple regression/correlation analysis for the behavioral sciences. Hillsdale, NJ: Erlbaum; 1983.
Borenstein M, Hedges LV, Higgins J, et al. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. 2010;1(2):97–111.
Field AP. Is the meta-analysis of correlation coefficients accurate when population correlations vary? Psychol Methods. 2005;10(4):444.
Rosenthal R. The file drawer problem and tolerance for null results. Psychol Bull. 1979;86(3):638.
Duval S, Tweedie R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. J Am Stat Assoc. 2000;95(449):89–98.
Duval S, Tweedie R. Trim and fill: a simple funnel plot based method of adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–63.
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. Br Med J. 2003;327(7414):557.
Sawyer SM, Afifi RA, Bearinger LH, et al. Adolescence: a foundation for future health. Lancet. 2012;379(9826):1630–40.
Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151(4):W65–94.
Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions. Wiley Online Library; 2008.
Rhodes RE, Mark RS, Temmel CP. Adult sedentary behavior: a systematic review. Am J Prev Med. 2012;42(3):e3–28.
Annesi JJ, Tennant G, Westcott WL, et al. Effects of the youth fit for life protocol on physiological, psychological, and behavioral factors at YMCA calgary after-school care sites. Psychol Rep. 2009;104(3):879–95.
Asci HF, Gokment H, Tiryaki G, et al. Self-concept and body image of Turkish high school male athletes and nonathletes. Adolescence. 1997;32(128):959–68.
Balaguer I, Atienza FL, Duda JL. Self-perceptions, self-worth and sport participation in adolescents. Span J Psychol. 2012;15(2):624–30. doi:10.5209/rev_SJOP.2012.v15.n2.38873.
Burgess G, Grogan S, Burwitz L. Effects of a 6-week aerobic dance intervention on body image and physical self-perceptions in adolescent girls. Body Image. 2006;3(1):57–66.
Cuddihy T, Michaud-Tomson L, Jones EK, et al. Exploring the relationship between daily steps, body mass index and physical self-esteem in female Australian adolescents. J Exerc Sci Fit. 2006;4(1):25–35.
Daley AJ. Extra-curricular physical activities and physical self-perceptions in British 14–15-year-old male and female adolescents. Eur Phys Educ Rev. 2002;8(1):37–49. doi:10.1177/1356336X020081003.
Debate RD, Gabriel KP, Zwald M, et al. Changes in psychosocial factors and physical activity frequency among third- to eighth-grade girls who participated in a developmentally focused youth sport program: a preliminary study. J School Health. 2009;79(10):474–84.
Findlay LC, Coplan RJ. Come out and play: shyness in childhood and the benefits of organized sports participation. Can J Behav Sci. 2008;40(3):153–61. doi:10.1037/0008-400x.40.3.153.
Hagger M, Ashford B, Stambulova N. Russian and British children’s physical self-perceptions and physical activity participation. Pediatr Exerc Sci. 1998;10(2):137–52.
Inchley J, Kirby J, Currie C. Longitudinal changes in physical self-perceptions and associations with physical activity during adolescence. Pediatr Exerc Sci. 2011;23(2):237–49.
Jensen CD, Steele RG. Body dissatisfaction, weight criticism, and self-reported physical activity in preadolescent children. J Pediatr Psychol. 2009;34(8):822–6. doi:10.1093/jpepsy/jsn131.
Malete L. Perceived competence and physical activity involvement among youths: an examination of HARTER’s competence motivation theory in Botswana. S Afr J Res Sport Ph. 2004;26(2):91–103.
Morgan CF, McKenzie TL, Sallis JF, et al. Personal, social, and environmental correlates of physical activity in a bi-ethnic sample of adolescents. Pediatr Exerc Sci. 2003;15(3):288–301.
Planinšec J, Fošnarič S. Relationship of perceived physical self-concept and physical activity level and sex among young children. Percept Mot Skills. 2005;100(2):349–53.
Planinsec J, Fosnaric S, Pisot R. Physical self-concept and physical exercise in children. Stud Psychol. 2004;46(2):89–95.
Ransdell LB, Dratt J, Kennedy C, et al. Daughters and mothers exercising together (DAMET): a 12-week pilot project designed to improve physical self-perception and increase recreational physical activity. Women Health. 2001;33(3/4):101–16.
Schneider M, Dunton GF, Cooper DM. Physical activity and physical self-concept among sedentary adolescent females: an intervention study. Psychol Sport Exerc. 2008;9(1):1–14.
Sullivan SO. The physical activity of children: a study of 1,602 Irish school children aged 11-12 years. Ir Med J. 2002;95(3):78–81.
Trautwein U, Gerlach E, Ludtke O. Athletic classmates, physical self-concept, and free-time physical activity: a longitudinal study of frame of reference effects. J Educ Psychol. 2008;100(4):988–1001.
Trew K, Scully D, Kremer J, et al. Sport, leisure and perceived self-competence among male and female adolescents. Eur Phys Educ Rev. 1999;5(1):53–73.
Viira R. Adolescents’ physical self-perception as relate to moderate-to-vigorous physical activity: a one-year longitudinal study. Acta Kinesiologiae Universitatis Tartuensis. 2011;17:199–208.
Asci FH, Kosar SN, Isler AK. The relationship of self-concept and perceived athletic competence to physical activity level and gender among Turkish adolescents. Adolescence. 2001;36(143):499.
Biddle S, Armstrong N. Children’s physical activity: an exploratory study of psychological correlates. Soc Sci Med. 1992;34(3):325–31.
Schmalz DL, Deane GD, Birch LL, et al. A longitudinal assessment of the links between physical activity and self-esteem in early adolescent non-hispanic females. J Adolesc Health. 2007;41(6):559–65. doi:10.1016/j.jadohealth.2007.07.001.
Altintas A, Asci FH. Physical self-esteem of adolescents with regard to physical activity and pubertal status. Pediatr Exerc Sci. 2008;20(2):142–56.
Bagoien TE, Halvari H, Nesheim H. Self-determined motivation in physical education and its links to motivation for leisure-time physical activity, physical activity, and well-being in general. Percept Mot Skills. 2010;111(2):407–32.
Carroll B, Loumidis J. Children’s perceived competence and enjoyment in physical education and physical activity outside school. Eur Phys Educ Rev. 2001;7(1):24–43. doi:10.1177/1356336X010071005.
Moreno JA, Cervello EM. Physical self-perception in Spanish adolescents: effects of gender and involvement in physical activity. J Hum Mov Stud. 2005;48(4):291–311.
Moreno Murcia JA. Goal orientations, motivational climate, discipline and physical self-perception related to the teacher’s gender, satisfaction and sport activity of a sample of Spanish adolescent physical education students. Int J Med Appl Sports Sci. 2005;17(2):44–58.
Papaioannou A. Perceptions of motivational climate, perceived competence, and motivation of students of varying age and sport experience. Percept Mot Skills. 1997;85(2):419–30.
Raustorp A, Mattsson E, Svensson K, et al. Physical activity, body composition and physical self-esteem: a 3-year follow-up study among adolescents in Sweden. Scand J Med Sci Sports. 2006;16(4):258–66.
Spink KS, Shields CA, Chad K, et al. Correlates of structured and unstructured activity among sufficiently active youth and adolescents: a new approach to understanding physical activity. Pediatr Exerc Sci. 2006;18(2):203–15.
Taylor IM, Ntoumanis N, Standage M, et al. Motivational predictors of physical education students’ effort, exercise intentions, and leisure-time physical activity: a multilevel linear growth analysis. J Sport Exerc Psychol. 2010;32(1):99–120.
Gao Z. Perceived competence and enjoyment in predicting students’ physical activity and cardiorespiratory fitness. Percept Mot Skills. 2008;107(2):365–72.
Sollerhed AC, Apitzsch E, Rastam L, et al. Factors associated with young children’s self-perceived physical competence and self-reported physical activity. Health Educ Res. 2008;23(1):125–36. doi:10.1093/her/cym010.
Gísladóttir TL, Matthíasdóttir Á, Kristjánsdóttir H. The effect of adolescents’ sports clubs participation on self-reported mental and physical conditions and future expectations. J Sports Sci. 2013;31(10):1139–45. doi:10.1080/02640414.2013.773402.
Abbott BD, Barber BL. Differences in functional and aesthetic body image between sedentary girls and girls involved in sports and physical activity: does sport type make a difference? Psychol Sport Exerc. 2011;12(3):333–42.
Bohnert AM, Ward AK. Making a difference: evaluating the girls in the game (GIG) after-school program. J Early Adolesc. 2013;33(1):104–30. doi:10.1177/0272431612466174.
Gaspar MJM, Amaral TF, Oliveira B, et al. Protective effect of physical activity on dissatisfaction with body image in children: a cross-sectional study. Psychol Sport Exerc. 2011;12(5):563–9. doi:10.1016/j.psychsport.2011.05.004.
Neumark-Sztainer D, Paxton SJ, Hannan PJ, et al. Does body satisfaction matter? Five-year longitudinal associations between body satisfaction and health behaviors in adolescent females and males. J Adolesc Health. 2006;39(2):244–51.
Monteiro Gaspar MJ, Amaral TF, Oliveira BMPM, et al. Protective effect of physical activity on dissatisfaction with body image in children: a cross-sectional study. Psychol Sport Exerc. 2011;12(5):563–9.
Neumark-Sztainer D, Goeden C, Story M, et al. Associations between body satisfaction and physical activity in adolescents: implications for programs aimed at preventing a broad spectrum of weight-related disorders. Eat Disord. 2004;12(2):125–37.
Shriver LH, Harrist AW, Page M, et al. Differences in body esteem by weight status, gender, and physical activity among young elementary school-aged children. Body Image. 2013;10(1):78–84. doi:10.1016/j.bodyim.2012.10.005.
Barnett LM, Morgan PJ, van Beurden E, et al. Perceived sports competence mediates the relationship between childhood motor skill proficiency and adolescent physical activity and fitness: a longitudinal assessment. Int J Behav Nutr Phys Act. 2008;5(1):40.
Eccles JS, Harold RD. Gender differences in sport involvement: applying the eccles’ expectancy-value model. J Appl Sports Psychol. 1991;3(1):7–35. doi:10.1080/10413209108406432.
Ekeland E, Heian F, Hagen KB. Exercise to improve self-esteem in children and young people. Cochrane Database Syst Rev. 2004;(1):CD003683.
Spence JC, McGannon KR, Poon P. The effect of exercise on global self-esteem: a quantitative review. J Sport Exerc Psychol. 2005;27(3):311–34.
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126.
Dishman RK. The measurement conundrum in exercise adherence research. Med Sci Sports Exerc. 1994;26:1382–90.
Lubans D, Morgan P. Evaluation of an extra-curricular school sport programme promoting lifestyle and lifetime activity for adolescents. J Sports Sci. 2008;26(5):519–29.
Deschamps V, Salanave B, Chan-Chee C, et al. Body-weight perception and related preoccupations in a large national sample of adolescents. Pediatr Obes. 2014;. doi:10.1111/j.2047-6310.2013.00211.x.
Morgan PJ, Barnett LM, Cliff DP, et al. Fundamental movement skill interventions in youth: a systematic review and meta-analysis. Paediatrics. 2013;132(5):e1361–83.
Robinson LE, Goodway JD. Instructional climates in preschool children who are at-risk. Part I: object-control skill development. Res Q Exerc Sport. 2009;80(3):533–42.
Robinson LE, Rudisill ME, Goodway JD. Instructional climates in preschool children who are at-risk. Part II: perceived physical competence. Res Q Exerc Sport. 2009;80(3):543–51.
Eather N, Morgan PJ, Lubans DR. Improving the fitness and physical activity levels of primary school children: results of the fit-4-fun group randomized controlled trial. Prev Med. 2013;56(1):12–9.
Morgan PJ, Saunders KL, Lubans DR. Improving physical self-perception in adolescent boys from disadvantaged schools: psychological outcomes from the physical activity leaders randomized controlled trial. Pediatr Obes. 2012;7(3):e27–32. doi:10.1111/j.2047-6310.2012.00050.x.
Wiersma LD, Sherman CP. The responsible use of youth fitness testing to enhance student motivation, enjoyment, and performance. Meas Phys Educ Exerc Sci. 2008;12(3):167–83.
Marsh HW, Richards GE, Johnson S, et al. Physical self-description questionnaire: psychometric properties and a multitrait-multimethod analysis of relations to existing instruments. J Sport Exerc Psychol. 1994;16(3):270–305.
Acknowledgments
Ronald C. Plotnikoff is supported by a National Health and Medical Research Council (NHMRC) Senior Research Fellowship. Mark J. Babic, Philip J. Morgan, Ronald C. Plotnikoff, Chris Lonsdale, Rhiannon L. White and David R. Lubans have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Babic, M.J., Morgan, P.J., Plotnikoff, R.C. et al. Physical Activity and Physical Self-Concept in Youth: Systematic Review and Meta-Analysis. Sports Med 44, 1589–1601 (2014). https://doi.org/10.1007/s40279-014-0229-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-014-0229-z