
Abstract
Background
Analysis of lower limb exercises is traditionally completed with four distinct methods: (1) 3D motion capture; (2) depth-camera-based systems; (3) visual analysis from a qualified exercise professional; and (4) self-assessment. Each method is associated with a number of limitations.
Objective
The aim of this systematic review is to synthesise and evaluate studies which have investigated the capacity for inertial measurement unit (IMU) technologies to assess movement quality in lower limb exercises.
Data Sources
A systematic review of studies identified through the databases of PubMed, ScienceDirect and Scopus was conducted.
Study Eligibility Criteria
Articles written in English and published in the last 10 years which investigated an IMU system for the analysis of repetition-based targeted lower limb exercises were included.
Study Appraisal and Synthesis Methods
The quality of included studies was measured using an adapted version of the STROBE assessment criteria for cross-sectional studies. The studies were categorised into three groupings: exercise detection, movement classification or measurement validation. Each study was then qualitatively summarised.
Results
From the 2452 articles that were identified with the search strategies, 47 papers are included in this review. Twenty-six of the 47 included studies were deemed as being of high quality.
Conclusions
Wearable inertial sensor systems for analysing lower limb exercises is a rapidly growing field of research. Research over the past 10 years has predominantly focused on validating measurements that the systems produce and classifying users’ exercise quality. There have been very few user evaluation studies and no clinical trials in this field to date.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Inertial measurement unit (IMU) systems have been extensively validated to successfully measure joint angle and temporal features during lower limb exercises. |
It is less understood if IMU systems can validly compute kinetic measures pertaining to lower limb exercises. |
IMU systems, which incorporate machine learning into their data analysis pathways, have also been found to be effective in automated exercise detection and in classifying movement quality across a range of lower limb exercises. |
1 Introduction
Lower limb exercises are used in rehabilitation, performance assessment, injury screening and strength and conditioning (S&C) contexts [1,2,3]. Movement is deemed ‘optimal’ during these exercises when injury risk is minimised and performance is maximised [4]. There are currently four distinct methods of assessing movement during lower limb exercise: (1) 3D motion capture; (2) depth-camera-based systems; (3) visual analysis from a qualified exercise professional; and (4) self-assessment. Each method is associated with a number of limitations. For instance, 3D motion capture systems are expensive and the application of skin-mounted markers may hinder normal movement [5, 6]. Furthermore, data processing can be time intensive and specific expertise is often required to interpret the processed data and to make recommendations on the observed results. Therefore, these systems are not frequently used to assess exercise technique beyond the research laboratory [7]. A cheaper and more accessible alternative is the use of depth-camera systems such as the Microsoft Kinect. In recent times, such systems have been increasingly leveraged for both research and commercial purposes due to their low cost and ease of setup. However, such systems have several key limitations. Depth-camera systems often lack accuracy when compared with gold-standard, marker-based systems. Such systems operate by tracking specific body locations and re-creating body segments based on these locations. As such, confusion and resultant poor accuracy is often caused by crossing over of body segments, unsuitable lighting (outdoors), movement of clothing and movement of other people [8]. As a result, users often must engage in time-intensive manual re-labelling of body segments to ensure an accurate system. Secondly, while these systems are relatively unobtrusive, they do require the user to set up a camera in an empty 2-m2 area. However, depending on the application space (clinic or gym), this may not be possible due to the presence of other people and equipment (squat rack/weight bench) that may confuse the system, resulting in poor accuracy. In clinical and gym-based settings, visual assessment is typically used to assess lower limb exercises. Visual assessment of human biomechanics is subjective and unreliable amongst novices and experts alike, as the need to visually assess numerous constituent components simultaneously is challenging [9]. This issue is compounded by the fact that athletes/clients may not be able to afford the supervision of a qualified professional (such as a physiotherapist, athletic therapist or personal trainer) in many instances. For this reason, individuals largely rely on self-assessment of their exercise technique in gym-based settings. The obvious limitation with this approach is that the individual may lack the knowledge required to assess their movement patterns, and simultaneously completing an exertive movement and assessing it without bias can be difficult [10].
Due to these limitations, in the past 15 years there has been an increase in interest in the automated assessment of lower limb exercises with wearable inertial measurement units (IMUs). Wearable IMUs are small, inexpensive sensing units (≈ €50–1000) that consist of accelerometers, gyroscopes and/or magnetometers. They are able to acquire data pertaining to the inertial motion and 3D orientation of individual limb segments [11, 12]. Self-contained, wireless IMU devices are easy to set up, and allow for the acquisition of human movement data in unconstrained environments [13]. IMU systems can robustly track a variety of postures in the complex environment associated with training in the ‘real-world’, unlike camera-based systems, which are hampered by location, occlusion and lighting issues [14]. IMUs have also been shown to be as effective as marker-based systems at measuring joint angles [7, 15, 16]. Therefore, IMUs have been recently employed for analysing a range of components of lower limb exercises. This includes detecting and quantifying the number of repetitions that are completed of a given exercise [17, 18], computing the range of motion (ROM) at key joints during these repetitions [19, 20], temporal analysis of exercises [21, 22], classifying one’s performance of an exercise as acceptable or as a specific deviation from acceptable [3, 23], or extracting exercise performance measures such as jump height and reactive strength index [24].
In the past decade, a number of reviews have assessed the literature pertaining to exercise analysis with wearable sensors. Fong and Chan reviewed the use of wearable IMUs in lower limb biomechanics studies; however, the focus of this work was broad, and predominantly reviewed gait-based papers [25]. Another early review covered the broad scope of health and wellness, rehabilitation and injury prevention with both wearable and ambient sensor systems [26]. The field has expanded considerably since then. Recently, a systematic review was published by Wang et al. that classified studies involving upper limb wearable systems for rehabilitation [27]. The ‘wearability’ of such systems and evidence supporting the systems’ effectiveness were also reviewed. Prior to this, this group published a review of studies on upper limb rehabilitation systems from 2008 to 2013 [28]. A variety of works have given an in-depth summary of movement measurement and analysis technologies; however, these do not focus on exercise analysis or the lower limb [29,30,31]. Cuesta-Vargas et al. reviewed the use of inertial sensors in human motion analysis and showed their capability for task-specific analysis [32]. Other studies have investigated how feedback affects therapy outcomes; however, these systems did not necessarily involve wearable IMUs and focused predominantly on the upper extremities [33,34,35]. A contemporary systematic review investigating the capacity for IMU technologies to quantify movement quality during lower limb exercises is not available. Therefore, the aim of this systematic review is to synthesise and evaluate studies which have investigated the capacity for IMU technologies to assess movement quality in lower limb exercises such as straight-leg raises, squats and countermovement jumps. In particular, we aim to describe the sensing set-ups used, inclusive of type (accelerometer and/or gyroscope and/or magnetometer), number and position of the sensing units. We also aim to describe the measurements each system extracted from the sensing units (e.g. ROM, power) and how they were validated. We will also establish which exercises were analysed by such systems. This review serves to summarise a rapidly growing field that has not been specifically reviewed in over 7 years [25]. It will identify clear gaps in the literature which are of interest to the research community and can be used as a resource for sports-medicine practitioners to build an understanding of the capabilities of IMU systems in assessing lower limb exercises. We hypothesise that IMU systems may be an effective and affordable tool to analyse components of lower limb exercises objectively and efficiently.
2 Methods
2.1 Literature Search Strategy and Study Selection Process
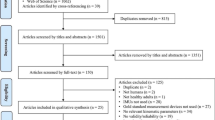
The protocol for this review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [36]. A literature search was completed within the following three databases: PubMed, Scopus and ScienceDirect. Papers regarding the following were selected: exercise, lower body, movement monitoring and IMUs. MeSH (Medical Subject Heading) terms or title/abstract keywords and their synonyms and spelling variations were used in several combinations and modified for every database. Articles published from January 2007 to May 2017 were reviewed. The 2007 start date was chosen to minimise irrelevant search results, as it represents the first known paper published in the field [17]. The general search strategy, including the search terms used, is provided in Table 1. This search includes refereed journal papers and peer-reviewed articles published in conference proceedings. Only articles written in the English language were included. The article selection process consisted of the following steps using the PRISMA [36] guidelines (Fig. 1): (1) a computerised search strategy was performed for the period January 2007 until September 2017; (2) after removal of duplicates, titles and abstracts of the remaining articles were screened; (3) the reviewer read the full texts and selected articles based on the inclusion/exclusion criteria (Table 2). In cases where a journal paper covered the contents reported in the earlier conference publications, the journal paper was preferred over the conference paper. In cases where the overlap was only partial, multiple publications were used as sources. Due to the relative novelty of IMU technologies, the grey literature was not searched; only peer-reviewed scientific articles were eligible for inclusion. We deemed this appropriate due to the non-interventional nature of studies in this field.

PRISMA flowchart of the results from the literature search. IMU inertial measurement unit, HAR human activity recognition
2.2 Data Extraction Process
Data extraction was completed by two authors (MOR and CD). Where discrepancies occurred, these were discussed and the associated papers were reassessed. A standardised data extraction form was utilised. Details about the study design, the exercises investigated, the sensor systems (e.g. accelerometer-only vs accelerometer + gyroscope) and the set-ups (e.g. multi-site vs single-site) used were ascertained. The studies were divided into three categories based on the aims/objectives of this review: exercise detection (ED); movement classification (MC); measurement validation (MV). Each study was then qualitatively summarised (aims, findings and conclusions based on these findings).
2.3 Assessment of Study Quality
Two authors (MOR and CD) evaluated the quality of the studies deemed eligible for inclusion using an adapted version of the STROBE assessment criteria for cross-sectional studies [37], which was devised by author consensus. Specifically, each study was rated on 10 specific criteria which were derived from items 1, 3, 6, 8, 11, 14, 18, 19, 20 and 22 of the original checklist. In cases where the authors completing paper rating (MOR or CD) were an author of a paper included in this review, the paper was instead rated by a different author of this paper (WJ) to minimise the risk of bias. Final study ratings for each reviewer were collated and examined for discrepancies. Any inter-rater disagreement was resolved by consensus decision. Once consensus was reached for all study ratings, overall quality scores were collated by summing those criteria, providing a score out of 10.
Studies were considered to be of high quality when more than seven domains were scored as high (1). If more than three domains were scored as low (0), the study was considered of low quality.
3 Results
3.1 Database Search and Paper Lists
An overview of the results in the different stages of the article selection process is shown in Fig. 1. From the 2452 articles that were identified with the search strategies, 47 papers are included in this review following the selection process.
The quality of the included reviews is displayed in Table 3. Based on our pre-defined criteria, 26 of the 47 included studies were deemed as being of high quality. Briefly, most studies adequately reported the methods of data acquisition (42/47), the outcome variables of interest and the method of statistical analysis employed (43/47). In contrast, many authors did not adequately discuss the limitations of the study (24/47), detail the eligibility criteria of the included sample (19/47) or cite relevant literature when discussing their results (27/47).
3.2 Sensor Set-Ups
Table 4 categorises the included articles based on whether the systems they adopted used multiple/single sensor units, compared sensor units at a variety of anatomical locations, and/or compared multiple sensor set-ups to single sensor set-ups for each application.
There was a large degree of heterogeneity in the included studies’ sensor set-ups. In particular, the types of sensors on board each sensing unit (accelerometer and/or gyroscope and/or magnetometer) and the number of sensing units required to be worn by system users varied. Table 5 demonstrates the distribution of sensors used in the included studies.
3.3 Exercises Investigated Versus Study Design
In the included studies, a total of fifty-three exercises were evaluated using a wearable inertial sensor system (Table 6). The most commonly investigated single-joint, uni-planar exercise was the lying straight leg-raise. There were three single-joint multi-planar exercises investigated. There were also two multi-joint, uni-planar exercises and 26 multi-joint, multi-planar exercises investigated. The most investigated of these were the sit-to-stand and squat exercises.
3.4 Qualitative Review
3.4.1 Measurement Validation
Twenty-eight studies identified for inclusion in this review attempted to validate wearable motion sensor systems [7, 20,21,22, 24, 38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. These 28 studies were categorised as evaluating either concurrent validity (Table 7) or construct validity (Table 8). For the purposes of this review, concurrent validity was defined as when a newly developed tool such as a wearable sensor system is compared with another test which is considered to be the ‘gold standard’ to measure the construct in question [62]. Construct validity compares a new wearable system’s output with another test that measures a similar construct but that is not a ‘gold standard’ (convergent validity), or evaluates the system’s capacity to discriminate between known groups in a cross-sectional (discriminative validity; known groups) or longitudinal (discriminative validity; responsiveness) manner [62].
Concurrent Validity Seventeen of the studies included in this review sought to compare a wearable sensor system’s output with a tool used in current clinical practice (e.g. goniometer for joint angle measurement) or gold standard biomechanical measurement tools (e.g. optoelectronic motion capture systems and force plates) [7, 20, 21, 24, 38,39,40,41,42,43,44,45,46,47,48,49,50]. These studies are summarised in Table 7.
Construct Validity Eleven studies investigated the construct validity of wearable motion systems for specific applications in tracking lower limb exercises. Of these, four assessed convergent validity [51,52,53,54]. Five studies pertained to known-groups validity [22, 55,56,57,58]. Two studies evaluated the longitudinal validity of a lower limb wearable sensor system in assessing joint ROM throughout a rehabilitation programme [60, 61]. All 11 studies which predominantly evaluated construct validity are summarised in Table 8.
3.4.2 Exercise Detection
Ten studies were identified for which automated detection of the exercise being completed was a key objective [14, 17,18,19, 63,64,65,66,67,68]. These studies are summarised in Table 9. It is difficult to directly compare the exercise detection sensitivity, specificity and accuracy across different studies. This is due to the vastly different data sets and cross-validation methods used to compute system accuracy.
3.4.3 Movement Classification
Eleven studies investigated the utilisation of wearable IMU systems for quantifying exercise technique [3, 19, 23, 64, 69,70,71,72,73,74,75]. Table 10 summarises the sensing set-ups, movement measure which was classified, methodology and performance metrics for each system identified in this area.
4 Discussion
4.1 Sensor Set-Ups
Various approaches have been employed when considering sensor set-ups for analysing lower limb exercises. As shown in Table 6, some studies opted solely for using one sensor type (accelerometer, gyroscope or magnetometer), whereas others opted for combinations of these in IMUs. The use of additional on-board sensors will reduce a sensing unit’s battery life, but allows for a greater variety of motion data to be captured from a user [12]. Combining accelerometer, gyroscope and magnetometer data also allows for improved accuracy in computing each unit’s 3D orientation [11]. The authors of this review believe that collecting data with all three inertial sensor types and then comparing system quality (i.e. accuracy or agreement with gold standard measurement) with individual sensor types or reduced combinations is the best approach. This enables a systematic approach to assess the cost–benefit of using additional sensors on board each IMU.
Similarly, the cost–benefit of using wearable sensing set-ups that use multiple sensing units can be compared with reduced sensor sets or single sensing unit set-ups by initially completing data collection with comprehensive set-ups. System efficacy can then be assessed when using data from multiple sensing units and each reduced combination of sensing units. This approach has been applied in movement classification and has shown promising results for single sensor systems in analysing early-stage and late-stage lower limb rehabilitation exercises [3, 70, 71]. Using reduced sensing set-ups potentially reduces the total cost of systems and increases their practicality for end users.
A criticism of the approach to sensor set-up employed by all the included studies in this review is that none reported evidence of engaging target end users when selecting their set-up. As previously mentioned, sensor set-up can influence a system’s cost, usability, battery life, accuracy and functionality. It is likely that the importance of each of these factors would vary across differing types of end users. For instance, a recreational gym goer may prioritise cost, usability and battery life, which may favour a minimal sensor set-up, whereas an elite sports team may prioritise accuracy and functionality, which could favour a comprehensive set-up. It is the authors’ contention that completing relevant qualitative research regarding sensor set-up with the target end users of a system, in advance of its development, could be of great benefit. It could also streamline the process of transferring systems from a research environment into a real-world offering.
4.2 Measurement Validation Studies
The concurrent validity of wearable motion-sensor-based systems to extract useful measures in lower limb exercises has been well investigated. The articles included in this review demonstrate these systems’ validity in measuring joint angle and ROM, in a broad variety of exercises ranging from sit-to-stands [48, 49] to lunges [42]. It is notable that a large proportion of these studies have high paper quality ratings (Table 3). They also used optoelectronic motion capture, a biomechanical research gold-standard measurement tool [20, 39, 50], or goniometry, a clinical gold standard [41,42,43], as the measurement comparator, which adds to the strength of this literature. Therefore, the evidence that IMU systems can validly measure joint angle and ROM is strong. However, for applications requiring maximal accuracy in these measures, an interesting area of further research may be identifying the sensing-unit placement position, for various body segments and exercises, which optimally agrees with an optoelectronic motion capture system. With the exception of Faber et al. [40], this is a widely under-investigated field. Research has also demonstrated the concurrent validity of wearable motion-sensor-based system measures, with force plate and optoelectronic motion capture data, to compute temporal features of exercises. A number of these studies have high quality ratings (Table 3) and analyse exercises ranging from five-times sit-to-stand tests [48], to deadlifts [21] to drop jumps [24, 44]. It is less understood if wearable motion sensor systems are useful in estimating kinetic measures such as peak vertical force and power during exercises. With the exception of Zijlstra et al.’s study on vertical power during the sit-to-stand exercise [49], the ‘high’ quality work to date in this area has shown these measures have a lower agreement with gold-standard biomechanical measurement systems than joint angle or temporal features [44, 46, 48]. Further research is required to investigate if the results are unique to different types of exercises or if they can be improved through employing different signal processing techniques.
The construct validity of wearable motion systems for a range of applications has also been well demonstrated at this point. Longitudinal validity has been shown via progress tracking in ROM through a rehabilitation programme [59, 60]. Known-groups validity has been demonstrated through capturing different movement profiles in specific exercises between injured and non-injured individuals [56, 57]. However, it should be noted these studies involved very small samples. Fitzgerald et al. [56] compared just a single injured and non-injured participant, and Ai et al. [57] compared three non-injured participants with one participant with polymyositis and one participant with lower back pain. Both papers also received a low paper quality rating (Table 3). Therefore, it is currently difficult to conclude that IMU systems can differentiate movement profiles from injured and non-injured groups and that the presented results are not just due to chance. Future validation studies of this fashion would benefit from employing larger participant groups of both injured and non-injured individuals. This would allow for statistical analyses comparing the groups. The results could be further strengthened by demonstrating concurrent validity of the reported measurements with an existing gold-standard measurement tool.
Whilst measurement validation studies are the most researched category in this field, there is still scope for more investigation. It is the authors’ contention that studies which validate temporal feature, joint angle and ROM measurements, computed from multiple sensing units, in lower limb exercises are likely to produce favourable results, but produce little new knowledge for the field. However, creating predictive algorithms for kinetic measurements, such as that in Setuain et al. [46] and Zijlstra et al. [49], or joint angle estimations with a single IMU in [7, 43], are still widely under-investigated areas with much room for advancement. Research that employs larger samples and assesses known-groups validity between injured and non-injured participants could also progress this area of the field.
4.3 Exercise Detection Systems
Ten studies included in this survey have demonstrated the efficacy of wearable inertial sensor systems to automatically identify the exercises being completed by users [14, 17,18,19, 63,64,65,66,67,68]. Exercise classification may serve as a useful input to an automated exercise tracking system or automated exercise logbook system. All studies demonstrated that a machine-learning-based classification approach is an effective data analysis approach for this task. With this in mind, it is interesting to note that only four studies in this area involved > 20 participants [18, 66,67,68]. As with many classification problems, exercise detection results may be improved by collecting larger data sets from more participants [76]. Future work in this area could also consider the practicality of the system for end users. Utilising a single IMU system for exercise detection [14, 18, 66,67,68] may be most desirable for end users. This will also reduce the cost of the exercise detection system. A potential methodological flaw in some of the reviewed studies is the inclusion of repetitions of exercises from the same participant in both training and test data. This can produce unrealistically high accuracy scores following cross-validation on a data set. This may have happened in a number of studies which used cross-validation methods such as leave-one-out-cross-validation (LOOCV), repeated random sub-sampling (RRSS) and K-fold cross-validation where each fold did not represent all of one participant’s data [14, 19, 63, 64]. Future work may also benefit from utilising deep learning techniques for classification such as the convolutional neural networks approach demonstrated by Dominguez Veiga et al. [68]. Such classification methodologies have recently been shown to have many benefits when compared with traditional machine learning classification techniques when analysing time-series data, including reducing the risk of overfitting and improving system accuracy [77, 78]. The method of Dominguez Veiga et al., which uses a machine vision approach within a deep learning context, also has the advantage of allowing interpretability of classification based on the visual appearance of the time series [68].
4.4 Movement Classification Systems
Despite first being investigated in 2010 [23], lower limb wearable movement classification systems are still a relatively under-investigated area. Five of the eleven published papers are relatively small-scale, with ten or fewer participants [19, 23, 64, 69, 75]. Movement classification systems have the potential to augment current clinical practice, providing users with feedback relating to their exercise technique in an unsupervised setting [79]. Most of the published work on movement classification pertains to a limited number of rehabilitation and S&C exercises (Table 10) [3, 19, 23, 64, 70,71,72, 74]. There is therefore potential to investigate movement classification with larger data sets and across a range of other exercises. This work could also compare binary and multi-label classification techniques and comprehensive and minimal sensing set-ups for such exercises, as in the work conducted by Giggins and colleagues [3]. Such work could also compare a variety of classification strategies (e.g. random forests [80], support vector machines [81], k nearest neighbours [82]) and should use appropriate cross-validation techniques to estimate system efficacy (accuracy, sensitivity and specificity). The studies which used leave-one-subject-out-cross-validation (LOSOCV) to validate their global movement classification system report that this is the most appropriate cross-validation method to estimate the efficacy of the system for a new user who is not included in the classifier’s training data [3, 23]. They also warn that including exercise repetitions from the same participant in both training and test data, as in Yurtman and Barshan [19] and Whelan et al. [70], can produce artificially high efficacy scores which do not transfer to real-world systems. Only one study experimentally evaluated the real-world accuracy of a movement classification system [75], which is recommended for future studies where possible as it negates the limitations of cross-validation techniques in assessing system efficacy. The efficacy scores presented by authors included accuracy, sensitivity/precision/true positive rate and specificity/recall/true negative rate. It is best to provide as many metrics as possible to allow a reader to understand a classification system’s strengths and weaknesses.
The general data analysis approach for all studies appears to be first completing signal pre-processing, signal segmentation, computing features from the signals and placing them in feature vectors, which will be used to train and evaluate different classification algorithms [79]. Some recent studies also compared the effectiveness of global and personalised classification systems [73, 74], whereby a personalised classification system is one which is trained from data from an individual and developed specifically for this individual, and a global classification system is trained with data from many individuals and can be used by individuals not included in the training data. Analysis has shown that the personalised systems are more computationally efficient and accurate than global ones [73,74,75], which has enabled movement classification systems to be developed with a single sensing unit rather than multiple sensing units. However, the time required to collect data from and train a classification system for every individual who requires a movement classification system is a significant practical limitation which may hinder the uptake of movement classification systems in clinical practice. Creating tools that streamline this process, as in O’Reilly et al. [75], could be an important avenue of research.
4.5 Review Limitations
Despite the strengths of this systematic review, it is important to consider several limitations when interpreting the results. Studies were not included if they were not published in the English language, which may influence the outcomes of our analyses, despite the probability that authors of high-quality surveys would aim for publication in high-impact journals published in the English language in the pursuit of superior dissemination of output data. Additionally, while the data extraction and paper rating were both completed by two authors (MOR and CD), the initial search, title and abstract screening was only completed by one author (MOR). Therefore, the possibility of erroneous exclusion of a valid study from this review exists. Finally, the protocol for this review was not registered prior to its completion. We deemed pre-registration inappropriate due to the expected heterogeneity in the evidence base. The scientific field of movement detection, classification and feedback using IMU is a burgeoning area that spans a multitude of disciplines, making systematic review and curation using a predefined protocol difficult.
4.6 Practical Implications
The practical implications of these findings deserve consideration. For members of the public or sports-medicine practitioners considering purchase of a commercially available sensing system to support lower-limb exercise completion for themselves or their patient/client, we would recommend a three-step appraisal process to determine the utility of the system under consideration. First, for what purpose is the system designed? Whether the system in question is for exercise detection (e.g. repetition (rep) counting during a deadlift) or classification (e.g. aberrant form during a squat) should be determined. Second, the system’s validity for the stated purpose in the same population should be confirmed. A system that is valid for detection is not commensurate with a system that is valid for classification. Similarly, the validity of a system tested on a healthy population does not necessarily extend to a pathological population. Finally, at what cost does the feature-set come? More expensive systems that incorporate a greater number of sensing units are likely to be more accurate, but the benefit of this increased accuracy should be identified. For instance, sports-medicine practitioners may seek higher accuracies for a system they plan to deploy in a cohort who are at a higher risk of injury, or to detect aberrant exercise technique, than for a cohort in whom they are seeking to quantify exercise load through rep-counting. As such, it may be more appropriate to leverage a more accurate and expensive multi-sensor system in the aberrant exercise cohort than in the rep counting cohort.
The number of commercially available sensing systems for exercise detection, classification and feedback will likely increase in the coming years, and the methods underlying these systems will evolve as the field of research progresses. We believe the appraisal process outlined above will accommodate new developments in the field.
This systematic review has also led to a number of recommendations for researchers developing wearable motion sensor systems for analysing lower limb exercises. A summary of such recommendations can be found in Table 11.
5 Conclusion
Wearable inertial sensor systems for analysing lower limb exercises is a rapidly growing technology. Research over the past 10 years has involved both the development and evaluation of such systems. The research to date has predominantly focused on validating measurements that the systems produce and classifying technique quality in the exercises (Tables 7, 8 and 10). A smaller number of studies have evaluated the ability of the systems to detect exercise type. Table 6 shows the 53 exercises that have currently been incorporated into such systems and highlights gaps in the literature which warrant further research. One such gap is that there are a limited number of studies that classify movement quality in jumping exercises. There exist a vast number of considerations for future research in this field, as outlined in Table 11. Moreover, there have been very few user evaluation studies and no clinical trials evaluating wearable inertial sensor systems for lower limb exercises. Such studies will be essential in producing knowledge that will catalyse the movement of these systems from laboratory-based studies into real-world applications for sports-medicine practitioners and people completing lower limb exercises.
References
Waller M, Gersick M, Holman D. Various jump training styles for improvement of vertical jump performance. Strength Cond J. (Lippincott Williams Wilkins) [Internet]. 2013;35:82–9. http://search.ebscohost.com/login.aspx?direct=true&db=s3h&AN=85709355&lang=pt-br&site=ehost-live.
Whittaker JL, Booysen N, de la Motte S, Dennett L, Lewis CL, Wilson D. Predicting sport and occupational lower extremity injury risk through movement quality screening: a systematic review. Br J Sports Med. 2017;51:580–5. https://doi.org/10.1136/bjsports-2016-096760.
Giggins OM, Sweeney KT, Caulfield B. Rehabilitation exercise assessment using inertial sensors: a cross-sectional analytical study. J Neuroeng Rehabil 2014;11:158. http://www.jneuroengrehab.com/content/11/1/158. Accessed 13 May 2017.
Farrokhi S, Pollard CD, Souza RB, Chen Y-J, Reischl S, Powers CM. Trunk position influences the kinematics, kinetics, and muscle activity of the lead lower extremity during the forward lunge exercise. J Orthop Sports Phys Ther. 2008;38:403–9.
Ahmadi A, Mitchell E, Destelle F, Gowing M, O’Connor NE, Richter C. Automatic activity classification and movement assessment during a sports training session using wearable inertial sensors. In: Proc 11th Int Conf Wearable Implant Body Sens Networks, BSN 2014. 2014. p. 98–103.
Bonnechère B, Jansen B, Salvia P, Bouzahouene H, Omelina L, Moiseev F. Validity and reliability of the Kinect within functional assessment activities: comparison with standard stereophotogrammetry. Gait Posture. 2014;39:593–8.
Bonnet V, Mazza C, Fraisse P, Cappozzo A. An optimization algorithm for joint mechanics estimate using inertial measurement unit data during a squat task. Proc Annu Int Conf IEEE Eng Med Biol Soc, EMBS. 2011. p. 3488–91.
Arulampalam J, Pierrepont J, Kark L. Markerless motion capture: validity of microsoft kinect cameras and ipisoft. Gait Posture. 2018;42:S76. https://doi.org/10.1016/j.gaitpost.2015.06.141 (Elsevier).
Whiteside D, Deneweth JM, Pohorence MA, Sandoval B, Russell JR, McLean SG. Grading the functional movement screenTM: A comparison of manual (real-time) and objective methods. [Internet]. J Strength Cond Res. 2014. http://www.ncbi.nlm.nih.gov/pubmed/25162646.
John OP, Robins RW, Craik KH, Dawes RM, Funder DC, Kemis M. Accuracy and bias in self-perception: individual differences in self-enhancement and the role of narcissism. J Pers Soc Psychol. 1994;66:206–19.
Madgwick SOH, Harrison AJL, Vaidyanathan R. Estimation of IMU and MARG orientation using a gradient descent algorithm. IEEE Int Conf Rehabil Robot. 2011.
Burns A, Greene BR, McGrath MJ, O’Shea TJ, Kuris B, Ayer SM. SHIMMERTM–A wireless sensor platform for noninvasive biomedical research. IEEE Sens J. [Internet]. 2010;10:1527–34. http://ieeexplore.ieee.org/lpdocs/epic03/wrapper.htm?arnumber=5482214.
McGrath D, Greene BR, O’Donovan KJ, Caulfield B. Gyroscope-based assessment of temporal gait parameters during treadmill walking and running. Sport Eng. 2012;15:207–13.
Morris D, Saponas TS, Guillory A, Kelner I. RecoFit: using a wearable sensor to find, recognize, and count repetitive exercises. In: CHI ’14 Proc SIGCHI Conf Hum Factors Comput Syst. [Internet]. ACM; 2014. p. 3225–34. http://dl.acm.org/citation.cfm?id=2557116.
Leardini A, Lullini G, Giannini S, Berti L, Ortolani M, Caravaggi P. Validation of the angular measurements of a new inertial-measurement-unit based rehabilitation system: comparison with state-of-the-art gait analysis. J Neuroeng Rehabil. 2014;11:1–7.
Tang Z, Sekine M, Tamura T, Tanaka N, Yoshida M, Chen W. Measurement and estimation of 3D orientation using magnetic and inertial sensors. Adv Biomed Eng. 2015;4:135–43.
Chang K, Chen MY, Canny J. Tracking free-weight exercises. Ubiquitous Comput. 2007. p. 19–37.
Giggins O, Sweeney KT, Caulfield B. The use of inertial sensors for the classification of rehabilitation exercises. In: Conf Proc IEEE Eng Med Biol Soc. 2014;2965–8.
Yurtman A, Barshan B. Automated evaluation of physical therapy exercises using multi-template dynamic time warping on wearable sensor signals. Comput Methods Programs Biomed. [Internet]. 2014;117:189–207. http://www.sciencedirect.com/science/article/pii/S0169260714002910. Accessed 19 May 2017.
Lin JFS, Kulić D. Human pose recovery using wireless inertial measurement units. Physiol Meas. [Internet]. 2012;33:2099–115. http://www.ncbi.nlm.nih.gov/pubmed/23174667.
Gleadhill S, Lee JB, James D. The development and validation of using inertial sensors to monitor postural change in resistance exercise. J Biomech. [Internet]. 2016;49:1259–63. http://www.sciencedirect.com/science/article/pii/S0021929016302937. Accessed 22 May 2017.
Setuain I, González-Izal M, Alfaro J, Gorostiaga E, Izquierdo M. Acceleration and orientation jumping performance differences among elite professional male handball players with or without previous ACL reconstruction: an inertial sensor unit-based study. PM&R [Internet]. 2015;7:1243–53. http://www.sciencedirect.com/science/article/pii/S1934148215002567. Accessed 13 May 2017.
Taylor PE, Almeida GJM, Kanade T, Hodgins JK. Classifying human motion quality for knee osteoarthritis using accelerometers. In: 2010 Annu Int Conf IEEE Eng Med Biol Soc. 2010. p. 339–43.
Patterson M, Caulfield B. A method for monitoring reactive strength index. Proced Eng. 2010;2:3115–20. https://doi.org/10.1016/j.proeng.2010.04.120.
Fong DTP, Chan YY. The use of wearable inertial motion sensors in human lower limb biomechanics studies: a systematic review. Sensors (Switzerland). 2010. p. 11556–65.
Patel S, Park H, Bonato P, Chan L, Rodgers M. A review of wearable sensors and systems with application in rehabilitation. J Neuroeng Rehabil. [Internet]. 2012;9:21. http://www.jneuroengrehab.com/content/9/1/21. Accessed 27 May 2017.
Wang Q, Markopoulos P, Yu B, Chen W, Timmermans A. Interactive wearable systems for upper body rehabilitation: a systematic review. J Neuroeng Rehabil. [Internet]. London: BioMed Central; 2017;14:20. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5346195/.
Wang Q, Chen W, Markopoulos P. Literature review on wearable systems in upper extremity rehabilitation. Biomed Heal Informatics (BHI), 2014 IEEE-EMBS Int Conf IEEE; 2014. p. 551–5.
Wong WY, Wong MS, Lo KH. Clinical applications of sensors for human posture and movement analysis: a review. Prosthet Orthot Int. 2007;31:62–75. https://doi.org/10.1080/03093640600983949 (SAGE Publications).
Noorkõiv M, Rodgers H, Price CI. Accelerometer measurement of upper extremity movement after stroke: a systematic review of clinical studies. J Neuroeng Rehabil. [Internet]. London: BioMed Central; 2014;11:144. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4197318/.
Howcroft J, Kofman J, Lemaire ED. Review of fall risk assessment in geriatric populations using inertial sensors. J Neuroeng Rehabil. [Internet]. BioMed Central; 2013;10:91. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3751184/.
Cuesta-Vargas AI, Galán-Mercant A, Williams JM. The use of inertial sensors system for human motion analysis. Phys Ther Rev. [Internet]. 2010;15:462–73. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3566464/.
Ribeiro DC, Sole G, Abbott JH, Milosavljevic S. Extrinsic feedback and management of low back pain: a critical review of the literature. Man Ther. 2017;16:231–9. https://doi.org/10.1016/j.math.2010.12.001 (Elsevier).
Subramanian SK, Massie CL, Malcolm MP, Levin MF. Does provision of extrinsic feedback result in improved motor learning in the upper limb poststroke? A systematic review of the evidence. Neurorehabil Neural Repair. 2009;24:113–24. https://doi.org/10.1177/1545968309349941 (SAGE Publications).
Saposnik G, Levin M. Virtual reality in stroke rehabilitation. Stroke [Internet]. 2011;42:1380–6. http://stroke.ahajournals.org/content/42/5/1380.abstract. Accessed 25 May 2017.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–9.
Haladjian J, Hodaie Z, Xu H, Yigin M, Bruegge B, Fink M. KneeHapp: a bandage for rehabilitation of knee injuries. In: Proc 2015 ACM Int Symp Wearable Comput. 2015;181–4.
Bolink SAAN, Naisas H, Senden R, Essers H, Heyligers IC, Meijer K. Validity of an inertial measurement unit to assess pelvic orientation angles during gait, sit–stand transfers and step-up transfers: Comparison with an optoelectronic motion capture system. Med Eng Phys. [Internet]. 2016;38:225–31. http://www.sciencedirect.com/science/article/pii/S1350453315002672. Accessed 13 May 2017.
Faber GS, Chang CC, Kingma I, Dennerlein JT. Lifting style and participant’s sex do not affect optimal inertial sensor location for ambulatory assessment of trunk inclination. J Biomech. 2013;46:1027–30. https://doi.org/10.1016/j.jbiomech.2012.12.007 (Elsevier).
Mehta SP, Barker K, Bowman B, Galloway H, Oliashirazi N, Oliashirazi A. Reliability, concurrent validity, and minimal detectable change for iphone goniometer app in assessing knee range of motion. J Knee Surg. 2016;30:577–84.
Romero Morales C, Calvo Lobo C, Rodríguez Sanz D, Sanz Corbalán I, Ruiz Ruiz B, López López D. The concurrent validity and reliability of the Leg Motion system for measuring ankle dorsiflexion range of motion in older adults. PeerJ [Internet]. San Francisco, USA: PeerJ Inc.; 2017;5:e2820. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214953/.
Bonnet V, Mazza C, Fraisse P, Cappozzo A. Real-time estimate of body kinematics during a planar squat task using a single inertial measurement unit. IEEE Trans Biomed Eng IEEE. 2013;60:1920–6.
Quagliarella L, Sasanelli N, Belgiovine G, Moretti L, Moretti B. Evaluation of standing vertical jump by ankles acceleration measurement. J Strength Cond Res LWW. 2010;24:1229–36.
Gordon D, Mullane SL, Conway PP, West AA. Development of a novel system for monitoring strength and conditioning in elite athletes. Proced Eng. [Internet]. 2012;34:496–501. http://www.sciencedirect.com/science/article/pii/S1877705812016980. Accessed 2 June 2017.
Setuain I, Martinikorena J, Gonzalez-Izal M, Martinez-Ramirez A, Gómez M, Alfaro-Adrián J. Vertical jumping biomechanical evaluation through the use of an inertial sensor-based technology. J Sports Sci. 2016;34:843–51. https://doi.org/10.1080/02640414.2015.1075057.
Rawson ES, Walsh TM. Estimation of resistance exercise energy expenditure using accelerometry. Med Sci Sports Exerc. [Internet]. 2010 [cited 2013 Dec 20];42:622–8. http://www.ncbi.nlm.nih.gov/pubmed/19952824.
Papi E, Osei-Kuffour D, Chen Y-MA, McGregor AH. Use of wearable technology for performance assessment: a validation study. Med Eng Phys. [Internet]. Butterworth-Heinemann; 2015;37:698–704. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4510317/.
Zijlstra W, Bisseling RW, Schlumbohm S, Baldus H. A body-fixed-sensor-based analysis of power during sit-to-stand movements. Gait Posture [Internet]. 2010;31:272–8. http://www.sciencedirect.com/science/article/pii/S0966636209006559. Accessed 23 May 2017.
Charlton PC, Mentiplay BF, Pua YH, Clark RA. Reliability and concurrent validity of a Smartphone, bubble inclinometer and motion analysis system for measurement of hip joint range of motion. J Sci Med Sport Sports Med Aust. 2015;18:262–7. https://doi.org/10.1016/j.jsams.2014.04.008.
Bo APL, Hayashibe M, Poignet P. Joint angle estimation in rehabilitation with inertial sensors and its integration with kinect. Eng Med Biol Soc EMBC. In: 2011 Annu Int Conf IEEE. IEEE; 2011. p. 3479–83.
Pernek I, Hummel KA, Kokol P. Exercise repetition detection for resistance training based on smartphones. Pers Ubiquitous Comput. 2012;17:771–82.
Omkar SN, Vyas K, Vikranth HN. Time-frequency analysis of human motion during rhythmic exercises. Eng Med Biol Soc EMBC, 2011 Ann Int Conf IEEE. IEEE; 2011. p. 1279–82.
Arai T, Obuchi S, Shiba Y, Omuro K, Inaba Y, Kojima M. The validity of an assessment of maximum angular velocity of knee extension (KE) using a gyroscope. Arch Gerontol Geriatr. 2012;54:175–80. https://doi.org/10.1016/j.archger.2011.10.012 (Elsevier).
Chakraborty S, Jamthe A, Ghosh SK, Agrawal DP. Determining athlete’s injury with wireless body area sensor network-based overhead squat testing. Mob Ad-Hoc Sens Syst (MASS), 2013 IEEE 10th Int Conf IEEE; 2013. p. 439–40.
Fitzgerald D, Foody J, Kelly D, Ward T, Markham C, McDonald J. Development of a wearable motion capture suit and virtual reality biofeedback system for the instruction and analysis of sports rehabilitation. Eng Med Biol Soc EMBS. 2007. p. 4870–4.
Ai QS, Chen L, Liu Q, Zou L. Rehabilitation assessment for lower limb disability based on multi-disciplinary approaches. Aust Phys Eng Sci Med. 2014;37:355–65.
Giggins O, Kelly D, Caulfield B. Evaluating rehabilitation exercise performance using a single inertial measurement unit. In: 7th Int Conf Pervasive Comput Technol Healthc Work. [Internet]. 2013 [cited 2014 Nov 13]. p. 49–56. http://eudl.eu/doi/10.4108/pervasivehealth.2013.252061.
Chen K-H, Chen P-C, Liu K-C, Chan C-T. Wearable sensor-based rehabilitation exercise assessment for knee osteoarthritis. Sensors (Basel). [Internet]. Springer; 2015;15:4193–211. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4367405/.
Houmanfar R, Karg M, Kulić D. Movement analysis of rehabilitation exercises: distance metrics for measuring patient progress. IEEE Syst J IEEE. 2016;10:1014–25.
Chen K-H, Tseng W-C, Liu K-C, Chan C-T. Using gyroscopes and accelerometers as a practical rehabilitation monitor system after total knee arthroplasty. In: 2015 IEEE MTT-S 2015 Int Microw Work Ser RF Wirel Technol Biomed Healthc Appl. IEEE; 2015. p. 58–9.
Streiner DL, Norman GR. Health Measurement Scales: a practical guide to their development and use. 5th ed. Oxford: Oxford University Press; 2008.
Tunçel O, Altun K, Barshan B. Classifying human leg motions with uniaxial piezoelectric gyroscopes. Sensors (Basel). [Internet]. MDPI; 2009;9:8508–46. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3260598/.
Chen P, Huang C-N, Chen I, Chan C. A rehabilitation exercise assessment system based on wearable sensors for knee osteoarthritis. In: Int Conf Smart Homes Heal Telemat. Springer; 2013. p. 267–72.
Ahmadi A, Mitchell E, Richter C, Destelle F, Gowing M, O’Connor NE. Automatic activity classification and movement assessment during a sports training session using wearable inertial sensors. IEEE Internet Things J. 2015;2:23–32.
Conger SA, Guo J, Fulkerson SM, Pedigo L, Chen H, Bassett DR. Objective assessment of strength training exercises using a wrist-worn accelerometer. Med Sci Sports Exerc. [Internet]. 2016;48:1847–55. http://europepmc.org/abstract/MED/27054678. Accessed 4 June 2017.
O’Reilly M, Whelan D, Ward TE, Delahunt E, Caulfield B. Technology in S&C: Tracking lower limb exercises with wearable sensors. J Strength Cond Res. [Internet]. 2017;pre-print. http://insights.ovid.com/crossref?an=00124278-900000000-96098. Accessed 17 Apr 2017.
Dominguez Veiga JJ, O’Reilly M, Whelan D, Caulfield B, Ward TE. Feature-free activity classification of inertial sensor data with machine vision techniques: Method, development, and evaluation. JMIR Mhealth Uhealth [Internet]. 2017;5:e115. http://mhealth.jmir.org/2017/8/e115/. Accessed 19 Aug 2017.
Kianifar R, Lee A, Raina S, Kulić D. Classification of squat quality with inertial measurement units in the single leg squat mobility test. In: 38th Annu Int Conf IEEE Eng Med Biol Soc. 2016. p. 6273–6.
Whelan DF, O’Reilly MA, Ward TE, Delahunt E, Caulfield B. Technology in rehabilitation: Evaluating the single leg squat exercise with wearable inertial measurement units. Methods Inf Med. [Internet]. Schattauer Publishers; 2016;55:[Epub ahead of print]. http://dx.doi.org/10.3414/ME16-02-0002.
O’Reilly MA, Whelan DF, Ward TE, Delahunt E, Caulfield B. Classification of lunge biomechanics with multiple and individual inertial measurement units. Sport Biomech. 2017;16:342–60.
O’Reilly MA, Whelan DF, Ward TE, Delahunt E, Caulfield BM. Technology in S&C: Assessing bodyweight squat technique with wearable sensors. J Strength Cond Res. 2017.
O’Reilly MA, Whelan DF, Ward TE, Delahunt E, Caulfield B. Technology in rehabilitation: comparing personalised and global classification methodologies in evaluating the squat exercise with wearable imus. Methods Inf Med. 2017;56:1–9.
O’Reilly MA, Whelan DF, Ward TE, Delahunt E, Caulfield BM. Classification of deadlift biomechanics with wearable inertial measurement units. J Biomech. 2017;58:155–61.
O’Reilly M, Duffin J, Ward T, Caulfield B. Mobile app to streamline the development of wearable sensor-based exercise biofeedback systems: system development and evaluation. JMIR Rehabil Assist Technol [Internet]. 2017;4:e9. http://rehab.jmir.org/2017/2/e9/. Accessed 13 Sept 2017.
Kotsiantis SB. Supervised machine learning: a review of classification techniques. Informatica [Internet]. 2007. http://books.google.com/books?hl=en&lr=&id=vLiTXDHr_sYC&oi=fnd&pg=PA3&dq=survey+machine+learning&ots=CVsyuwYHjo&sig=A6wYWvywU8XTc7Dzp8ZdKJaW7rc%5Cnpapers://5e3e5e59-48a2-47c1-b6b1-a778137d3ec1/Paper/p800%5Cnhttp://www.informatica.si/PDF/31-3/11_Kotsiantis. Accessed 7 July 2017.
Zeng M, Nguyen LT, Yu B, Mengshoel OJ, Zhu J, Wu P. Convolutional neural networks for human activity recognition using mobile sensors. In: Pro 6th Int Conf Mob Comput Appl Serv. [Internet]. 2014. p. 197–205. https://www.computer.org/csdl/proceedings/mobicase/2014/024/00/07026300-abs.html. Accessed 15 June 2017.
Jia Y, Shelhamer E, Donahue J, Karayev S, Long J, Girshick R. Caffe: convolutional architecture for fast feature embedding. ACM Int Conf Multimed. 2014;675–8.
Whelan DF, O’Reilly MA, Huang B, Giggins OM, Kechadi T, Caulfield B. Leveraging IMU data for accurate exercise performance classification and musculoskeletal injury risk screening. In: 38th Annu Int Conf IEEE Eng Med Biol Soc 2016 [Internet]. IEEE; 2016. p. 1–6. http://dx.doi.org/10.3414/ME16-02-0002.
Breiman L. Random forests. Mach Learn. 2001;45:5–32. https://doi.org/10.1023/A:1010933404324.
Hearst MA, Dumais ST, Osman E, Platt J, Scholkopf B. Support vector machines. IEEE Intell Syst. 1998;13:18–28.
Dudani SA. The distance-weighted k-nearest-neighbor rule. IEEE Trans Syst Man Cybern. 1976;6:325–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Martin O’Reilly was partially funded for this work by the Irish Research Council as part of a Postgraduate Enterprise Partnership Scheme with Shimmer (EPSPG/2013/574). Brian Caulfield, Tomas Ward, William Johnston and Cailbhe Doherty were funded and Martin O’Reilly was partially funded by Science Foundation Ireland under their grant for the Insight Centre for Data Analytics (SFI/12/RC/2289). These funding bodies had no influence on the data collection, data analysis, data interpretation or approval/disapproval of publication.
Conflict of interest
Martin O’Reilly, Brian Caulfield, Tomas Ward, William Johnston and Cailbhe Doherty declare that they have no conflicts of interest relevant to the content of this review.
Rights and permissions
About this article

Cite this article
O’Reilly, M., Caulfield, B., Ward, T. et al. Wearable Inertial Sensor Systems for Lower Limb Exercise Detection and Evaluation: A Systematic Review. Sports Med 48, 1221–1246 (2018). https://doi.org/10.1007/s40279-018-0878-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-018-0878-4