
Abstract
Background
An adverse drug reaction (ADR) is a harmful and unintended response to a drug. The Portuguese National Pharmacovigilance System (NPS) receives reports from healthcare professionals and consumers, then analyzes the reports to help prevent, eliminate or minimize the risks of drugs to consumers. Community pharmacy professionals (CPPs) have privileged access to consumers, and throughout their pharmacotherapeutic follow-up and the professional–consumer relationship, they can perceive possible ADRs and encourage consumers to report. The aim of this survey was to evaluate CPPs as role players in improving consumers’ involvement in pharmacovigilance and to describe their attitudes related to the pharmacovigilance system and consumers’ reporting of ADRs.
Methods
An observational study was performed in a group of Portuguese CPPs contacted through e-mail with a link to a web-based survey created in the Google Docs® platform. Data were collected between April and May 2016 and analysed using Spearman’s correlation coefficients and statistical analysis with SPSS® v.23.0 software.
Results
Almost all (96.5%) of respondents declared they knew about the NPS, but only 40.7% had reported an ADR. Half (50.0%) of respondents said they usually encourage consumers to report ADRs. However, 1.2% admitted advising consumers not to report if they solicited help from the CPP. Most CPPs (80.2%) were available to help consumers report ADRs. CPPs are encouraged to report ADRs if they are concerned about the situation caused by the reaction or if the ADR is serious or unexpected. Regarding measures to increase the number of ADRs received by the NPS, 91.9% of respondents advised raising awareness of the NPS and 86.1% advised improving the communication between doctors and patients.
Conclusion
Despite their knowledge of the pharmacovigilance system, only a small percentage of CPPs had reported ADRs, and approximately half did not usually encourage consumers to report possible ADRs. Reporting of ADRs is fundamental to pharmacovigilance, and consumer reporting is a significant contribution to creating useful information on drug safety. Underreporting remains a concern and, in community pharmacies, CPPs can play a major role in pharmacovigilance by reporting ADRs directly or encouraging consumers to report them.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
According to the World Health Organization (WHO), “Pharmacovigilance is the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other possible drug-related problems”, through adverse drug reaction (ADR) reports, which are analysed to prevent, minimize or even eliminate the risk of ADRs associated with certain drugs [1, 2]. An ADR corresponds to a response to a medicinal product that is noxious and unintended, that may arise from the use of the product within or outside the terms of the marketing authorization or from occupational exposure, including off-label use, overdose, misuse, abuse and medication errors [3].
When a drug is introduced on the market, only a part of its activity is known (i.e. some ADRs associated with its pharmacological activity are only discovered after its marketing, since unexpected or low-incidence ADRs are difficult to detect during clinical trials) [4–6]. Therefore, ADR reporting is a useful method for their detection and prevention, as it involves the whole population as well as all marketed drugs [4–6]. The suspicion of an ADR means there is at least a reasonable possibility of a causal relationship between a drug and an adverse event, and it should be a sufficient reason for reporting [3]. Reporting of ADRs to the Portuguese National Pharmacovigilance System (NPS) by both healthcare professionals (HCPs) and the general public is essential to ensure medication safety and minimize the risk to public health in Portugal [7].
The new European legislation of 2010 [3] established that consumers could also be active participants reporting ADRs directly to the National Competent Authorities in all countries of the EU. The implementation of this legislation aimed to increase the number and quality of ADR reports, since the major limitation of spontaneous reporting is usually the lack of reports and the quality of ADRs reported [4, 8–10]. This underreporting appears to be related to the lack of knowledge in the pharmacovigilance field, both by HCPs and consumers [11].
Consumers’ ADR reports may contain incorrect or incomplete clinical information due to a lack of knowledge about pharmacovigilance and ADR reporting [12]. Consumers’ reporting may be of poor quality compared with reports from HCPs. Low-quality reports can be inconclusive and lead to loss of time and additional analysis costs [13]. However, consumer reporting has more advantages than disadvantages: it allows a better collection of ADR-related data and provides more information about the misuse of drugs, contributing to a genuine perception of the ADRs impact in consumers’ lives [8]. Consumers’ reports are usually not focused on clinical information, but reveal complete reports of the signs, symptoms, and consequences related to ADRs and indicate the consumer’s perspective about the subject [14].
In this context, community pharmacy professionals (CPPs) have an important role in encouraging and assisting consumers to report ADRs, since they can track consumers before and during drug treatment and verify the occurrence of ADRs [11, 15, 16]. CPPs can be active not only as reporters, but also as promoters of improving patient reporting [16, 17]. In Portugal, there are two different regulated professionals in the community pharmacy sector, namely pharmacists (5-year curriculum, including a mandatory pharmacovigilance component, resulting in a Master’s degree in Pharmaceutical Sciences) and pharmacy technicians (4-year curriculum, resulting in a Bachelor’s degree in Pharmacy; a pharmacovigilance course is not mandatory, but is included in some syllabuses). These are the professionals who have the most contact with consumers and may be able to perceive possible ADRs and encourage them to report such events [18]. Therefore, reporting from CPPs and consumers can be complementary, building up more reliable and accurate reports.
This study aims to evaluate the role of CPPs as active agents for improving the involvement of consumers in pharmacovigilance and to describe the attitudes and knowledge of these professionals regarding the spontaneous reporting of ADRs.
Material and methods
A cross-sectional descriptive study was designed with the objective of describing the attitudes and knowledge of Portuguese CPPs regarding pharmacovigilance knowledge and ADR reporting by consumers, as well as their opinions regarding the NPS.
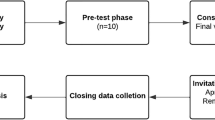
A questionnaire was constructed by the research team and was first tested in a small group of field testers (n = 12), and subsequently sent to the selected respondents through the Google Docs® platform. The individual questionnaire was anonymous, and the data were intended only for the scientific purposes of this study and were stored in agreement with privacy regulations.
The questionnaire was pre-tested to evaluate its major wording problems and improve the quality of the questions. When pre-test was performed, some questions were rewritten to provide a better understanding of the questionnaire.
The questionnaire consisted of 42 items and was divided into the following four parts:
-
Part I collected personal information about the responding CPPs.
-
Part II collected information about the characteristics of the pharmacy at which the responding CPP was employed.
-
Part III contained questions exploring the knowledge of CPPs regarding pharmacovigilance and their attitudes and behaviour regarding ADR reporting.
-
Part IV contained questions regarding the CPP’s relationship with consumers and the position of the CPP with regard to consumer reporting of ADRs.
The questionnaire was sent to all pharmacies in the Coimbra region in Portugal (n = 152) via the general e-mail address of each pharmacy, and asked all respondents to disseminate the questionnaire to other CPPs at the pharmacy, to maximize the number of responses. A reminder was sent 2 and 4 weeks later. Data were collected during a 6-week period in April and May 2016.
Non-probability intentional sampling was used: pharmacy professionals who were employed in community pharmacies in the Coimbra district were surveyed. According to the Medicine and Healthcare Products Statistics (INFARMED, IP), currently, there are 636 CPPs in Coimbra with higher degree education [19]. The data were analysed according to descriptive statistics using SPSS® v.23.0 software. Spearman nonparametric test was used for correlations. The correlation was considered very strong when r ≥ 0.90, strong when 0.90 > r ≥ 0.70, moderate when 0.70 > r ≥ 0.40, weak if 0.40 > r ≥ 0.20 and very weak if r < 0.20 [20].
Results
A total of 90 questionnaires were completed, but four were excluded due to selection criteria, providing 86 valid responses. The response rate of target CPPs was 13.5%. The personal and professional characteristics of the responders are presented in Table 1.
Pharmacies had on average 6.12 ± 2.77 staff members. The pharmacy workforce consisted of pharmacists (3.45 ± 1.46), pharmacy technicians (2.06 ± 1.14) and pharmacy assistants (1.46 ± 0.72). Participants were 35.07 ± 10.32 years old and had 10.90 ± 8.46 years of professional experience.
Professional knowledge and attitudes
Of the 86 respondents, 96.5% (n = 83) knew about the NPS, with these being mostly female (73.5%, n = 61) and with a Master’s degree in Pharmaceutical Sciences (77.1%, n = 64), and 67.4% (n = 58) of respondents stated that they had training in the pharmacovigilance field.
Only 40.7% (n = 35) of respondents said they had reported an ADR, with 71.4% (n = 25) of these being female, 88.6% (n = 31) having a Master’s degree in Pharmaceutical Sciences, and 60% (n = 21) coming from a rural area. Among the 51 CPPs who never reported an ADR, 74.5% (n = 38) were female, 70.6% (n = 36) had a Master’s degree in Pharmaceutical Sciences and 51% (n = 26) were from a rural area. There are no statistical differences between age and length of professional experience and the knowledge of the NPS or previous reporting of an ADR.
Regarding reported ADRs, 51.4% (n = 18) were reported online, 42.9% (n = 15) by sending a letter and 2.3% (n = 2) by telephone. Last year, the average number of reported ADRs was 1.23 (±1.14), and 77.1% (n = 27) of participants had no difficulty during the reporting process.
Table 2 shows the factors that encouraged these CPPs to have previously reported an ADR. The main reason for reporting ADRs among CPPs was the concern about the situation caused by the ADR—“the ADR was considered serious”—and was found to be statistically significant (p = 0.034) with a weak correlation (r = 0.359). The absence of ADRs in the information leaflet of the medicine was the second leading factor encouraging CPPs to report ADRs—“the ADR is not described in the leaflet”—and was found to be statistically significant (p = 0.028) with weak correlation (r = 0.371). The professional concern with the ADR not being described in the leaflet increases with age. In addition, work experience is statistically significant when compared with “the ADR is not described in the leaflet” (p = 0.001), establishing among themselves a moderate correlation (r = 0.522).
Of the 51 respondents who had never reported an ADR, 21.6% (n = 11) admitted that they had experienced a situation where they should have reported an ADR. Table 3 shows the reasons why these CPPs had never reported an ADR. There were no statistically significant differences between the age of CPPs and the reasons mentioned above. The length of work experience was found to be statistically significant with the item “a single case is not relevant to the drug safety knowledge” (p = 0.042), with a weak positive correlation (r = 0.292).
Professional relationship with the consumers
Of the respondents, 50% (n = 43) stated they encourage consumers to report ADRs and 29.1% (n = 25) said that the consumer took part in reporting the ADR to the NPS.
With regard to completing the ADR report, 80.2% (n = 69) of responders would help the consumer and would explain the spontaneous reporting process to him/her, 16.3% (n = 14) would offer to report the ADR for the consumer, 2.3% (n = 2) would explain the procedure of spontaneous reporting to the consumer, and 1.2% (n = 1) would advise consumers not to report the ADR.
Opinions about the national pharmacovigilance system
Table 4 presents some measures that could increase the number of ADR reports.
There is a statistically significant difference between the age of the professional and “increase awareness of NPS”, with a weak negative correlation (r = −0.284), which means that as the length of work experience increases, it becomes less important for professionals. The same happens between this measure and the length of work experience (p = 0.012 and r = −0.274).
With regard to the open-ended question addressing the barriers to reporting to the NPS, 28 responses were received. The major barriers were the bureaucratic level and the lack of exposure. Fourteen responses showed some negative views within the NPS; however, there were also positive responses (n = 9), and some that indicate both positive and negative points (n = 5).
Some of the responses to the open-ended question are shown below (translated from Portuguese by the authors):
-
“NPS cannot expect reports from users when health professionals are not encouraged to report ADR.”
-
“NPS should be more communicative with healthcare professionals and consumers.”
-
“The reporting system is still undeveloped and needs to be closer to healthcare professionals.”
-
“[Reporting system] is unknown by most consumers and not truly fulfills its role … it is something that is good to exist, but not being up [to] the responsibility.”
-
“NPS is still little known and poorly used because people do not know about the possibility of reporting or don’t have the opportunity to do it, especially in rural areas. Regarding healthcare professionals, lack of time and knowledge are, unfortunately, the reasons for the low use of the NPS.”
-
“The system works well despite the poor adherence by health professionals, including the practitioners that sometimes choose not to report.”
-
“The system is not well known in (Portuguese) Central region. The information does not reach the community pharmacies.”
-
“It seems that [they] perform their activities well. However, it should provide greater support and dissemination to HCPs.”
-
“It should have more activities with health professionals and the general population.”
-
“It is an important system to control the side effects of drugs.”
-
“It should be more frequently disseminated among health professionals.”
-
“The NPS is very important. However it is unintuitive and in my experience the site is too slow.”
-
“It is a useful system, well organized and that I value.”
Discussion
This study aimed to assess the knowledge and attitudes of CPPs regarding the Portuguese NPS. Although most respondents declared themselves to be aware of the NPS, only 40.7% had previously reported an ADR. The main reasons for reporting an ADR was the severity of the ADR and a lack of information about the ADR in the medicine leaflet. Both reasons demonstrated a statistically significant relationship with the years of experience of the CPP; the more experienced the CPP, the greater was the concern with ADRs. The fact that the ADR was already known was the most mentioned reason that CPPs did not report the ADR. Respondents also showed a positive agreement with the item “ADR was unexpected” as a factor that encourage CPPs to report (85.7% of respondents agreed or fully agreed).
The biggest concern the NPS faces is the lack of ADR reporting [21]. According to respondents, this can happen due to several reasons, such as the complexity of the NPS and also the attitudes of HCPs [18, 22, 23]. Although the respondents had the opinion that the NPS is favourable and useful for the study of drug safety, they also feel that this pharmacovigilance system was not well known among HCPs and consumers, and needs more exposure. This study showed that as long as work experience increases, the concern about the awareness of NPS decreases, due to the improvement of their knowledge in pharmacovigilance and drug safety issues with working experience. However, ≈90% of respondents identified the need for raising awareness of the NPS, through direct contact with consumers and incorporation of pharmacovigilance topics in HCPs’ graduation curricula.
According to similar studies in Portugal and Europe, there is no agreement about whether gender and workplace of HCPs can influence ADR reporting, whereas their knowledge and attitudes seem to affect the reporting of ADRs [15, 18, 23–25]. Similar to what happened in this study, age and gender did not influence ADR reporting [24]; however, some attitudes could be influenced by these variables.
CPPs commonly only report ADRs if they are sure that these ADRs are associated with medication use [15]. Common reasons for not reporting ADRs included lack of time to report the ADR and uncertainty about the drug causing the ADR. Also, other reasons associated with ADR underreporting were related to method of reporting, fear of legal liability, ignorance, diffidence, complacency and insecurity [15, 18, 22, 24–27]. Inman [22] proposes seven reasons for this high underreporting: three linked to attitudes relating to professional activity (financial incentives, legal aspects and ambition to publish); and the others linked to ADR-related attitudes and knowledge (diffidence, indifference, complacency and ignorance) [22]. Insecurity about causality (i.e. the belief that it is nearly impossible to determine whether or not a medicine is responsible for a particular ADR) is another factor associated with underreporting [23], but was not proposed by Inman [22]. A study in the UK concluded that, despite professionals being aware that consumers are able to report ADRs, there were doubts regarding their ability to identify ADRs and submit a good report [28]. If measures could be taken to change CPPs’ attitudes, underreporting of ADRs could be reduced [15]. The Regional Centers of Pharmacovigilance should take a proactive role in improving communication with the CPPs, for example, performing conferences/training courses, webinars or newsletters, and trying to develop educational tools to discuss the attitudes related to underreporting of ADRs [23–25, 28]. However, other measures, such as the simplification of the reporting process or more exposure of the NPS in a regional or national way may lead to a greater awareness of the importance of this issue [25].
Strengths and limitations
Due to the low response rate to the questionnaire, it was not possible to obtain a statistically significant sample. The response rate could be related to the lack of interest in spontaneous reporting of ADRs and drug safety issues by HCPs. In 2015, the Pharmacovigilance Center of the Central region in Portugal was the centre that had received the lowest amount of ADR reports [29]. The results of this study should be explored further in regional or national studies.
An ADR had already been reported by 40.7% of respondents. This percentage could be even lower across CPPs in general, since most of the respondents had a keen interest in pharmacovigilance, leading them to answer the questionnaire.
Regarding the process of data collection, social interaction between the interviewer and respondent can lead to respondents taking social norms into account when responding, resulting in social desirability bias. Also, a communication barrier could impact the results. There was no direct contact between researchers and respondents. During the data collection, all contacts were performed via e-mail, including the initial invitation to participate in the survey and the reminders. A lack of social contact may have an impact on survey uptake by participants; sample selection bias could also be present, due to the non-randomized method of selection of the sample, which commonly could cause bias in the extrapolation of the results to the population. Selection method might contribute to the exclusion of professionals, since the decision to disseminate the questionnaire to all CPPs in the pharmacy was uncertain, and there were pharmacies where only one response was received, and other pharmacies that ignored the questionnaire and reminders.
One of the major strengths of this study was the input of personal answers of the CPPs regarding the NPS. These views could be useful and should be taken into account to improve the communication between the NPS and professionals in order to create a reporting culture.
Conclusion
Reporting of ADRs is fundamental to pharmacovigilance, and consumer reporting is a significant contribution to creating useful information on drug safety. CPPs can play a major role in pharmacovigilance by reporting ADRs directly or encouraging consumers to report them. Consumer reporting is fundamental for gathering important information in the pharmacovigilance area, as they provide the consumer’s point of view, with a better description of the signs and symptoms. Underreporting of ADRs remains the biggest concern of the NPS. Nevertheless, some measures could be taken to overcome this problem and encourage HCPs and consumers to play an active role in pharmacovigilance, namely continuous education and training should be incorporated to increase the level of risk perception and encourage a better attitude about reporting for both CPPs and consumers.
References
World Health Organization. WHO. The importance of pharmacovigilance: safety monitoring of medicinal products. Geneva: World Health Organization; 2002. p. 1–48.
Härmark L, Van Grootheest AC. Pharmacovigilance: methods, recent developments and future perspectives. Eur J Clin Pharmacol. 2008;64(8):743–52.
EC. Directive 2010/84/EU of the European Parliament and of the Council of 15 December 2010 amending, as regards pharmacovigilance. Directive 2001/83/EC on the Community code relating to medicinal products for human us [online]. Available from URL: http://eur-lex.europa.eu/LexUriServ/LexUriServ.douri=OJ:L:2010:348:0074:0099:EN:PDF. Accessed 30 May 2011; 2010.
Matos C, van Hunsel F, Joaquim J. Are consumers ready to take part in the pharmacovigilance system? A Portuguese preliminary study concerning ADR reporting. Eur J Clin Pharmacol. 2015;71(7):883–90.
Marques J, Ribeiro-Vaz I, Pereira AC, et al. A survey of spontaneous reporting of adverse drug reactions in 10 years of activity in a pharmacovigilance centre in Portugal. Int J Pharm Pract. 2014;22(4):275–82.
Figueiras A, Tato F, Fontaiñas J, et al. Physicians’ attitudes towards voluntary reporting of adverse drug events. J Eval Clin Pract. 2001;7(4):347–54.
Gavaza P, Brown CM, Lawson KA, et al. Influence of attitudes on pharmacists’ intention to report serious adverse drug events to the Food and Drug Administration. Br J Clin Pharmacol. 2011;72(1):143–52.
Leone R, Moretti U, D’Incau P, et al. Effect of pharmacist involvement on patient reporting of adverse drug reactions: first Italian study. Drug Saf. 2013;36(4):267–76.
Van Grootheest AC, Van Puijenbroek EP, de Jong-van den Berg LTW. Contribution of pharmacists to the reporting of adverse drug reactions. Pharmacoepidemiol Drug Saf. 2002;11(3):205–10.
Borg J-J, Aislaitner G, Pirozynski M, et al. Strengthening and rationalizing pharmacovigilance in the EU: where is Europe heading to? Drug Saf. 2011;34(3):187–97.
Steurbaut S, Hanssens Y. Pharmacovigilance: empowering healthcare professionals and patients. Int J Clin Pharm. 2014;36(5):859–62.
Waller PC. Making the most of spontaneous adverse drug reaction reporting. Basic Clin Pharmacol Toxicol. 2006;98(3):320–3.
Blenkinsopp A, Wilkie P, Wang M, et al. Patient reporting of suspected adverse drug reactions: a review of published literature and international experience. Br J Clin Pharmacol. 2007;63(2):148–56.
Anderson C, Krska J, Murphy E, et al. The importance of direct patient reporting of suspected adverse drug reactions: a patient perspective. Br J Clin Pharmacol. 2011;72(5):806–22.
Herdeiro MT, Figueiras A, Polónia J, et al. Influence of pharmacists’ attitudes on adverse drug reaction reporting. Drug Saf. 2006;29(4):331–40.
Parretta E, Rafaniello C, Magro L, et al. Improvement of patient adverse drug reaction reporting through a community pharmacist-based intervention in the Campania region of Italy. Expert Opin Drug Saf. 2014;13(Supp 1):21–9.
Pellegrino ML, Desiderio V, Mores N, et al. The role of the pharmacist in patient reporting of adverse drug reactions: the Italian interregional project [in Italian]. G Ital di Farm e Farm. 2015;7(1):63–74.
Matos C, Joaquim J, Pires T. Attitudes and knowledge of community pharmacy professionals regarding the spontaneous reporting of adverse drug reactions: a preliminary study in Coimbra, Portugal. Drugs Ther Perspect. 2017;33(2):86–92.
Infarmed. Estatística do Medicamento e Produtos de Saúde 2014; 2014.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrance Eribaum Association; 1988.
Herdeiro MT, Ferreira M, Ribeiro-Vaz I, et al. The Portuguese pharmacovigilance system. Acta Médica Port. 2012;25(4):241–9.
Inman WH. Attitudes to adverse drug reaction reporting. Br J Clin Pharmacol. 1996;41(5):434.
Lopez-Gonzalez E, Herdeiro MT, Figueiras A. Determinants of under-reporting of adverse drug reactions. Drug Saf. 2009;32(1):19–31.
Marques JI, Polónia J, Figueiras AG, et al. Nurses’ attitudes and spontaneous adverse drug reaction reporting: a case–control study in Portugal. J Nurs Manag. 2016;24(3):409–16.
Duarte M, Ferreira P, Soares M, et al. Community pharmacists’ attitudes towards adverse drug reaction reporting and their knowledge of the new pharmacovigilance legislation in the southern region of Portugal: a mixed methods study. Drugs Ther Perspect. 2015;31(9):316–22.
Toklu HZ, Soyalan M, Gültekin O, et al. The knowledge and attitude of the healthcare professionals towards pharmacovigilance and adverse drug reaction reporting in northern Cyprus. J Pharmacovigil. 2016;4:193. doi:10.4172/2329-6887.1000193.
Belton KJ. Attitude survey of adverse drug-reaction reporting by health care professionals across the European Union. Eur J Clin Pharmacol. 1997;52(6):423–7.
Krska J. Views of British community pharmacists on direct patient reporting of adverse drug reactions (ADRs). Pharmacoepidemiol Drug Saf. 2013;22(10):1130–3.
INFARMED. Sistema Nacional de Farmacovigilância (SNF): Notificações e Casos de RAM - Ano/2015; 2016.
Acknowledgements
The manuscript has been read and approved by all authors, and all authors agree to the submission of the manuscript to the Journal. The authors would like to thank Clara Rocha, Ph.D., at the Coimbra Health School for her contribution in the data analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Sources of funding
No sources of funding was used to assist in the preparation of this manuscript.
Conflict of interest
Cristiano Matos, Liliana Rodrigues and João José Joaquim have no conflicts of interest that are directly relevant to the content of this study.
Rights and permissions
About this article

Cite this article
Matos, C., Rodrigues, L. & Joaquim, J. Attitudes and opinions of Portuguese community pharmacy professionals towards patient reporting of adverse drug reactions and the pharmacovigilance system. Drugs Ther Perspect 33, 188–194 (2017). https://doi.org/10.1007/s40267-017-0380-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40267-017-0380-3