
Abstract
Albiglutide is a long-acting, glucagon-like peptide-1 receptor agonist for subcutaneous administration with a recommended dose of 30–50 mg once weekly. The aim of this article is to outline the pharmacokinetic and pharmacodynamic properties of albiglutide including the clinical efficacy and safety data underlying the approval of albiglutide for the treatment of type 2 diabetes mellitus in both Europe and USA. Albiglutide is cleared from the circulation (by a mechanism partially dependent on renal function) with an elimination half-life of 5 days, allowing once-weekly administration. In the clinical trial program called HARMONY, albiglutide demonstrated placebo-corrected reductions in glycosylated hemoglobin of 0.8–1.0%. In addition, reductions in fasting plasma glucose in the range of 1.3–2.4 mmol/L compared with placebo were reported. Albiglutide caused weight reductions at a level comparable to placebo in the HARMONY trials, possibly related to limited central nervous system penetration of the large albiglutide molecule. Albiglutide demonstrated a generally favorable safety profile, although with a signal of an increased risk of pancreatitis. The well-known adverse events related to glucagon-like peptide-1 receptor activation such as nausea, diarrhea, and vomiting were less frequent with albiglutide compared with another glucagon-like peptide-1 receptor agonist, liraglutide, but slightly more frequent following treatment with albiglutide than with placebo or active comparators from other classes of anti-hyperglycemic drugs. The full risk-benefit profile for albiglutide used in treating type 2 diabetes will not be clear until reporting of the long-term cardiovascular outcome trial (HARMONY Outcome) with planned completion in 2019.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Albiglutide provides glycemic control and lowers fasting plasma glucose and glycosylated hemoglobin by 0.8–1%, similar to other glucagon-like peptide-1 receptor agonists. |
Compared with other glucagon-like peptide-1 receptor agonists, gastrointestinal adverse effects and weight loss are less frequent with albiglutide. |
1 Introduction
Type 2 diabetes mellitus (T2DM) is an increasing global health problem and a leading cause of microvascular and macrovascular morbidity and mortality. The disease is characterized by a disruption of glucose and lipid metabolism, leading to hyperglycemia in both the fasting and postprandial state. The risk of microvascular complications, such as retinopathy and renal impairment in patients with T2DM, can be reduced by improving glycemic control, and a treatment goal of glycosylated hemoglobin (HbA1c) below 7% should be pursued. However, individual characteristics such as the risk of hypoglycemia, co-morbidities, patient preferences, and life expectancy must be taken into account when deciding on glycemic targets [1, 2]. Furthermore, the treatment of patients with T2DM includes optimal prevention of the potential macrovascular complications and increased mortality in these individuals. This includes a focus on cardiovascular risk factors associated with the diabetic phenotype such as obesity, hypertension, and dyslipidemia. Subjects with T2DM exhibit hepatic and peripheral insulin resistance, deficient insulin secretion, and inappropriately elevated glucagon levels [3, 4]. The reduced β-cell function and chronic hyperglycemia in patients with T2DM is at least partly owing to an impaired incretin effect [5, 6]. The incretin effect is elicited by the gut hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide and has been demonstrated to account for up to 70% of insulin secretion in healthy subjects following oral glucose ingestion [7].
A range of pharmacological GLP-1 receptor agonists (GLP-1RAs) has been developed to use the ability of GLP-1 to counteract the pathophysiological features of T2DM. GLP-1 augments insulin secretion from the pancreatic β cells alongside a suppressive effect on glucagon secretion at normal and elevated glucose levels [8]. These insulinotropic and glucagon-suppressing effects of GLP-1 are both clinically important to reduce the hyperglycemia in patients with T2DM [9]. Additionally, the combination of reduced enteric motility, which delays carbohydrate absorption [10], and the activation of GLP-1 receptors in the central nervous system, which promotes satiety and ultimately weight loss [8, 11], are also beneficial. All of these effects are particularly beneficial in patients with T2DM. It is generally accepted that the initial therapy following T2DM diagnosis should consist of lifestyle changes alongside metformin [1]. However, a lack of data on comparative effectiveness and long-term benefits on micro- and macrovascular outcomes of the available anti-hyperglycemic agents for the treatment of T2DM [sulfonylurea, insulin, GLP-1RAs, α-glucosidase inhibitors, thiazolidinediones, dipeptidyl peptidase-4 (DPP-4) inhibitors, sodium-glucose co-transporter 2 inhibitors, bromocriptine, and bile acid sequestrants] complicate the choice of a preferred add-on treatment to metformin [1]. In addition, the range of established adverse events (AEs), typically hypoglycemia, weight gain, and/or gastrointestinal side effects, but also potential safety risks should be taken into account when deciding on treatment. Furthermore, the price of the drugs may also influence treatment choice.
Albiglutide (Eperzan®/Tanzeum®; GlaxoSmithKline, Brentford, London, United Kingdom) is a long-acting GLP-1RA for subcutaneous administration with a recommended starting dose of 30 mg once weekly (QW). However, up-titration to 50 mg QW is an option in the case of an insufficient glycemic response. Albiglutide was approved in both Europe and USA in 2014 as an add-on to other anti-hyperglycemic drugs including basal insulin. In addition, albiglutide is approved in Europe as monotherapy in patients with contraindications or intolerance towards metformin.
The aim of this article is to outline the pharmacokinetic and pharmacodynamic properties of albiglutide including the clinical efficacy and safety data underlying the approval of albiglutide for the treatment of T2DM. The protocol is based on electronic literature searches in www.pubmed.org with the keywords: ‘albiglutide’, ‘GLP-1 receptor agonist’, ‘HARMONY’, ‘eperzan’, ‘tanzeum’, ‘glucagon-like peptide-1’, and ‘type 2 diabetes’. Furthermore, manual searches including scanning of reference lists in relevant papers, specialist journals, and conference proceedings have been performed. No relevant Cochrane reviews were identified.
2 Pharmacokinetics
2.1 Chemistry
Albiglutide is a large protein molecule weighing 73 kDa and generated by recombinant DNA technology in the yeast species Saccharomyces cerevisiae [12]. The drug is based on two sequential copies of modified human GLP-1 merged in sequence with human albumin (Fig. 1). The N-terminal amino acid sequence of GLP-1 is normally rapidly cleaved (elimination half-life of approximately 1.5 min) by the enzyme DPP-4 [13]. This inactivation of the pharmacologically active GLP-1 moiety in albiglutide is prevented by substituting the GLP-1 sequences at position eight (glycine substituted for alanine) (Fig. 1) [12].

Molecular structures of native human GLP-1 and albiglutide
2.2 Absorption
Albiglutide is predominantly absorbed via the lymphatic circulation after subcutaneous administration. The use of various injection sites (abdomen, leg, or arm) has been demonstrated not to affect the exposure of albiglutide [12].
2.3 Distribution
The apparent volume of distribution (relative to bioavailability, which is not known) for albiglutide is 11 L. A mean peak plasma concentration of 1.7 µg/mL is reached approximately 4 days after single-dose subcutaneous administration of 30 mg albiglutide and steady-state concentrations are obtained following 3–4 weeks of treatment in subjects with T2DM [14]. The ability to cross the blood–brain barrier is limited because of the albumin-based structure and large molecular weight of the albiglutide molecule [15]. In mice, penetration into brain parenchyma was similar to that observed with albumin and no accumulation of albiglutide was observed after 24 h [16].
2.4 Metabolism
Albiglutide undergoes degradation into small peptides and individual amino acids by proteolytic enzymes in plasma and tissues. However, because albiglutide is an albumin fusion protein, it likely follows a metabolic pathway similar to native human serum albumin, which is catabolized primarily in the vascular endothelium [12]. No formal investigations of the metabolism of albiglutide have been reported.
2.5 Elimination
Albiglutide has an elimination half-life of 5 days and a mean apparent clearance of 67 mL/h [12]. Functioning kidneys seem to play a part in the elimination process, perhaps related to the renal blood flow, and a 30–40% increase in exposure to albiglutide is observed in patients with severe renal impairment compared with subjects with normal renal function. This is in line with population pharmacokinetic data suggesting that clearance decreased approximately 30% (from normal) in subjects with severe renal impairment [12]. Age has been reported to correlate with clearance to almost the same degree as the estimated glomerular filtration rate, and this may be based on the close association of these two parameters [12]. In a post-hoc analysis of all clinical studies, albiglutide seemed to be associated with more AEs and had a slightly lower efficacy in patients with moderate renal impairment (i.e., estimated glomerular filtration rate <60 mL/min) compared with patients with normal renal function [17].
Body weight and race have both been found to influence the clearance of albiglutide. Thus, proportional changes in clearance have been reported in subjects with lower (44 kg) and higher (157 kg) body weight compared with subjects with a more typical body weight of 92 kg [12]. Reduced clearance and increased exposure to albiglutide have been demonstrated in both Japanese patients and subjects with African heritage. Thus, Japanese patients have a 30–40% higher exposure to albiglutide than Caucasians, whereas African heritage is associated with a 22% lower clearance compared with other racial groups [12]. No formal studies have been conducted to investigate the pharmacokinetics of albiglutide in patients with hepatic impairment or pediatric patients. No adjustment of dosage is recommended in USA for patients with mild, moderate, or severe renal impairment [18], but the knowledge base on albiglutide treatment in patients with severe renal impairment is at this time still limited. Thus, albiglutide is not recommended in the European Union for this group of patients [19, 20].
2.6 Drug–Drug Interactions
A range of potential drug–drug interactions for albiglutide has been examined in a series of phase I studies (Table 1). No clinical relevant changes in pharmacokinetic or pharmacodynamic properties of digoxin, oral contraceptives, or warfarin were observed in response to concomitant treatment with albiglutide 50 mg QW [21]. However, a study reported albiglutide to cause a 40% decrease in the area under the plasma concentration-time curve (AUC) for simvastatin combined with an 18% increase in maximum plasma concentration. The observed decrease in AUC for simvastatin was seen alongside a similar increase in AUC for the potent active metabolite simvastatin acid, which points to an increased metabolism of simvastatin in relation to concurrent albiglutide treatment [12]. The clinical impact of this drug interaction is not clear and no dosage adjustments have been advised [19].
3 Pharmacodynamics
3.1 Glycemia and Body Weight
An ex vivo study using human embryonic kidney cells has demonstrated albiglutide to function as a GLP-1RA. Other preclinical studies have reported treatment with albiglutide to elicit improvements in insulin secretion, insulin sensitivity, and β-cell mass in addition to reduced body weight and reduced gastric emptying rate and intestinal motility [12].
A phase II study comprising a stepped glycemic clamp setup in patients with T2DM showed glucose-dependent augmentation of insulin secretion after a single dose of albiglutide 50 mg [22]. In this study, a total of 44 subjects with median age of 51 years and duration of T2DM between 6 months and 10 years were equally randomized to either albiglutide (female 12/22) or placebo (female 12/22). Significant C-peptide AUC increments (p = 0.02) were observed at plasma glucose levels above 5 mmol/L in patients treated with albiglutide compared with placebo. During hypoglycemic conditions, no differences with respect to insulin secretion and counter-regulatory hormones (glucagon, epinephrine, norepinephrine, growth hormone, and cortisol) were observed between treatment groups [22].
Acute activation of the GLP-1 receptor has a delaying effect on gastric emptying, but continuous activation of this receptor induces tachyphylaxis to this effect [23, 24]. Albiglutide, as a 100-mg single dose in healthy men, delayed gastric emptying with an increase in time to empty half of the gastric content from 1.1 to 2.2 h (p = 0.01) and from 0.3 to 0.7 h (p = 0.002) for solids and liquids, respectively [25]. It is likely that this effect will wane a few days into the treatment with albiglutide (continuous activation of the GLP-1 receptor) similar to the situation for the other long-acting GLP-1RAs. Nevertheless, the potential effect on gastric emptying should be taken into consideration in relation to the timing of concomitant medications and precaution for use in patients with gastroparesis.
3.2 Cardiovascular System
Ex vivo studies on perfused rat hearts have demonstrated albiglutide to stimulate the insulin-independent glucose uptake with an associated improvement in cardiac glucose utilization. In addition, in vivo studies in rats have reported albiglutide to cause a significant reduction in myocardial infarct size in addition to an improved left ventricular function following myocardial ischemia as compared with placebo [25].
The effects of albiglutide on the human cardiovascular system have also been investigated. As with other GLP-1RAs, an increase in heart rate has been observed. Thus, an integrated analysis of phase III trials for albiglutide has reported an increased mean heart rate of 1–2 beats per minute compared with the all comparators group [12]. Albiglutide treatment has demonstrated no effect on the electrocardiographic QT interval [26] and furthermore, no consistent effect on blood pressure with variations within 1 mmHg of baseline values [12]. A meta-analysis of the cardiovascular events (cardiovascular death, non-fatal myocardial infarction, hospitalization for unstable angina, and stroke) in the clinical trials reported a hazard ratio of 1.00 (0.68; 1.49) for albiglutide vs. the all comparators group [27].
A trial entitled “HARMONY Outcome and further exploring long-term cardiovascular endpoints for albiglutide” is underway (ClinicalTrials.gov identifier: NCT02465515.) This trial is investigating albiglutide in the doses of 30 and 50 mg QW vs. placebo with an estimated enrollment of 9400 patients ≥40 years of age and with pre-established cardiovascular disease including coronary artery disease, cerebrovascular disease, or peripheral arterial disease. The trial will be essential in determining the cardiovascular safety of albiglutide. However, with a final completion date of May 2019, it is likely to be the last large-scale cardiovascular outcome trial to report among the currently marketed (or close to be marketed) GLP-1RAs.
Thus, several trials with acronyms LEADER (trial for liraglutide; reported in 2016) [28], SUSTAIN (for semaglutide; reported in 2016) [29], and ELIXA (for lixisenatide; reported in 2015) [30] have been completed. Furthermore, results from EXSCEL (for exenatide QW; to be completed in 2018) and REWIND (for dulaglutide; to be completed in 2018) will be reported before completion of the HARMONY Outcome study. The EXSCEL trial, with an expected 14,000 subjects (30% of these having no prior history of cardiovascular events), will be the first large cardiovascular outcome study to address the potential role of GLP-1RA treatment in the primary prevention of cardiovascular events in patients with T2DM. To date, the completed trials have reported cardiovascular safety for lixisenatide and cardiovascular benefit for liraglutide and semaglutide, respectively, with respect to major adverse cardiac events. The ELIXA trial reported a placebo-corrected hazard ratio of 1.02 (95% confidence interval 0.89–1.17) for major adverse cardiac events (cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, or hospitalization for unstable angina), whereas placebo-corrected hazard ratios of 0.87 (95% confidence interval 0.78–0.97) and 0.74 (95% confidence interval 0.58–0.95) were reported for major adverse cardiac events (cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke) in the LEADER and SUSTAIN trials, respectively.
3.3 Dosing
The optimal regimen for dosage and administration of albiglutide in the extensive phase III study program was based on several phase II studies. One of these phase II studies reported by Rosenstock et al. included 356 North and South American patients with T2DM and found an apparent advantage of 30-mg QW dosing of albiglutide [31]. In this study, participants were randomized to placebo or eight different treatment arms (three QW [4, 15, and 30 mg], three once biweekly [15, 30, and 50 mg] and two once monthly [50 and 100 mg]) of albiglutide or to an open-label group with exenatide 10 mg twice daily. Dose-dependent reductions in HbA1c were observed with albiglutide. Treatment with 30 mg QW, 50 mg biweekly, or 100 mg monthly for 16 weeks caused similar and statistically significant placebo-corrected reductions in HbA1c of approximately 0.6%. A larger placebo-corrected reduction in fasting plasma glucose (FPG) of 1.38 mmol/L was observed in the 30-mg QW group compared with the 50-mg biweekly and 100-mg monthly groups with reductions of 1.17 and 1.16, respectively [31]. Even more important in this context, larger fluctuations in FPG were reported after treatment with albiglutide 50 mg biweekly and 100 mg monthly compared with 30 mg QW [31].
Seino and colleagues have performed two randomized controlled trials in Japanese patients with T2DM. The first of these studies included 40 participants treated with diet or a single oral anti-hyperglycemic drug other than thiazolidinedione. Participants were randomized to 4 weeks of treatment with albiglutide 15 mg QW, 30 mg QW, 50 mg biweekly, 100 mg monthly, or placebo. All four groups treated with albiglutide had significant placebo-corrected reductions in HbA1c in the range of 0.51–0.63%. FPG was also significantly reduced by 1.74–1.98 mmol/L (31.4–35.7 mg/dL) in the QW and biweekly treatment groups, whereas no significant reduction was observed after treatment with 100 mg monthly compared with placebo [32]. The second study by Seino et al. included 215 participants randomized to four different groups treated for 16 weeks with either albiglutide 15 mg QW, 30 mg QW, 30 mg once biweekly, or placebo. The albiglutide 30-mg QW group had the largest glycemic response with placebo-corrected reductions in HbA1c of 1.6% and FPG of 2.37 mmol/L (42.7 mg/dL) [33]. A longer duration of the second study (16 vs. 4 weeks), combined with a higher baseline HbA1c of 8.5% compared with 7.1–8.3% in the different groups of the first study, could partly account for the remarkable difference in glycemic efficacy between the two studies [32, 33].
Overall, the range of phase II studies have reported a favorable safety profile for the 30 mg QW dosing of albiglutide [32, 33] and furthermore, fewer gastrointestinal AEs have been reported with this dosing regimen compared with 50 mg biweekly and 100 mg monthly [31]. Thus, based on the findings from the phase II studies, a QW dosing of 30 mg with an optional up-titration to 50 mg was chosen for the extensive phase III investigation of the clinical effects of albiglutide. It is worth noting that although the 50-mg QW dose was not included in the dose-finding studies, it was investigated within the phase III studies. More than 50% of the albiglutide-treated subjects across the phase III trials, which allowed optional up-titration based on glycemic control, had their dose up-titrated from 30 to 50 mg QW [12]. Thus, the 30-mg QW dose may not be sufficient in the majority of patients.
4 Clinical Efficacy
4.1 Glycemic Control
The clinical efficacy of albiglutide in patients with T2DM has been evaluated in the phase III study program entitled HARMONY that included eight randomized controlled trials. Albiglutide was examined in dosing regimens of 30 and 50 mg QW, both as monotherapy and in combination with other anti-hyperglycemic agents. An overview of the HARMONY trials can be found in Table 2. All eight studies included changes in HbA1c from baseline as the primary outcome. Furthermore, effects on FPG were also assessed in all HARMONY trials. Any additional composite endpoints regarding glycemic efficacy, such as time to anti-hyperglycemic rescue therapy and proportion of patients meeting specified HbA1c levels, will not be addressed in this article. Table 3 provides an overview of the results from the HARMONY studies. Baseline HbA1c levels were between 8 and 8.5% in the trials. Albiglutide was applied as both monotherapy and as add-on to different combinations of metformin, glimepiride, and pioglitazone in the four trials including placebo arms. Placebo-corrected HbA1c reductions between 0.8 and 1.0% after treatment with albiglutide were reported in these studies [34–37]. The largest reduction in HbA1c was observed in HARMONY 2 following forced up-titration of albiglutide to 50 mg QW [35], which provides further rationale for the optional up-titration from the recommended starting dose of 30 mg QW in clinical practice. Between half and two-thirds of subjects in the HARMONY trials allowing optional up-titration of albiglutide ended up with a final dose of 50 mg QW [36–40].
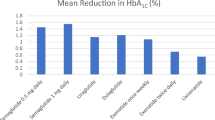
In the trials using active comparators, albiglutide was added to various combinations of metformin, sulfonylureas, glitazones, and insulin glargine [36–41]. Albiglutide led to superior HbA1c reductions compared with both sitagliptin (0.4% [0.5;0.2]) and glimepiride (0.3% [0.5;0.1]) [36]. In addition, the HARMONY 8 trial demonstrated a significant reduction of 0.3% with albiglutide in a combined comparison to three different doses of sitagliptin (25, 50, and 100 mg) applied in patients with severe, moderate, and mild renal impairment, respectively [40]. On the contrary, albiglutide demonstrated smaller reductions in HbA1c as compared with pioglitazone and liraglutide with differences of 0.25% [0.10;0.40] and 0.21% [0.08;0.34], respectively [37, 41]. However, in both cases the observed differences did not exceed the arbitrarily defined non-inferiority margins of 0.3%. Finally, albiglutide has been reported to elicit HbA1c reductions similar to insulin glargine and insulin lispro [38, 39]. No apparent correlation between particular combinations of anti-hyperglycemic drugs and improvements in glycemic control was apparent in the HARMONY trials.
The effects of albiglutide on FPG demonstrated in the HARMONY trials mirror the changes in HbA1c described above (Table 2). Placebo-corrected reductions in the range of 1.3–2.4 mmol/L (23.4–43.2 mg/dL) from a baseline between 8.5 and 9.7 mmol/L (153.2–174.8 mg/dL) were demonstrated [34–37]. Again, treatment with albiglutide 50 mg QW caused the largest reduction [35].
Albiglutide was found to cause superior reductions in FPG of 0.9 mmol/L (16.2 mg/dL) compared with sitagliptin and 0.6 mmol/L (10.8 mg/dL) compared with glimepiride [36]. The HARMONY 8 trial demonstrated a significant reduction of 1.2 mmol/L (21.6 mg/dL) after treatment with albiglutide compared with sitagliptin in patients with renal impairment [40]. Albiglutide elicited smaller reductions in FPG in comparison to pioglitazone and liraglutide with differences of 1.1 mmol/L [0.6; 1.5] (19.8 mg/dL [10.8; 27.0]) and 0.5 mmol/L [0.1; 0.8] (9.0 mg/dL [1.8; 14.4]), respectively [37, 41]. A significant larger reduction in FPG (difference of 1.2 mmol/L (21.6 mg/dL)) was observed after treatment with basal insulin glargine compared with albiglutide [38]. However, albiglutide was shown to cause non-inferior reductions in FPG as compared with prandial insulin lispro [39].
Postprandial glycemia was not reported as an outcome in any of the HARMONY trials. This was most likely owing to an expected limited effect on gastric emptying of this long-acting GLP-1RA [24, 42] as opposed to the short-acting GLP-1RA counterparts lixisenatide and exenatide twice daily [43]. However, the previously described phase II studies by Seino et al. reported significant reductions in postprandial plasma glucose levels after 16 weeks of treatment with albiglutide 30 mg QW. Placebo-corrected reductions of 3.6 mmol/L (64.9 mg/dL) in the 4-h post-breakfast weighted mean AUC and 3.2 mmol/L (57.7 mg/dL) in mean 2-h postprandial glucose were observed in the two studies, respectively [32, 33].
The above-mentioned clinical trials have provided evidence that albiglutide in monotherapy and as add-on to different glucose-lowering therapies confers substantial reductions in HbA1c and FPG.
4.2 Body Weight
Average baseline BMI of participants was above 30 kg/m2 in all of the HARMONY trials (Table 2). Albiglutide resulted in absolute body weight changes between −1.2 and +0.3 kg in the placebo-controlled trials with non-significant placebo-corrected changes in the range of −0.2 to +0.3 kg [34–37]. The absolute changes in body weight after treatment with albiglutide were between −0.7 and −1.2 kg in the trials including insulin and sulfonylureas as active comparators. The albiglutide-treated groups had significant reductions in body weight of 1.5 and 2.6 kg compared with insulin and sulfonylurea-treated groups, respectively [36, 38, 39]—an unsurprising finding owing to the well-established weight-increasing effects of insulin and sulfonylureas [44]. In addition, albiglutide was associated with increased body weight reductions compared with both sitagliptin and pioglitazone with differences of 0.6 and 4.9 kg, respectively [37, 40]. However, the HARMONY 3 trial reported a non-significant difference of 0.4 kg between albiglutide and sitagliptin [36] and the observed difference to pioglitazone could be explained by an increase in body weight of 4.4 kg in patients treated with this drug [37]. Finally, in comparison with liraglutide, less body weight reduction was observed with albiglutide—the absolute difference in weight reduction was 1.5 kg [1.0;2.1] between the two continuous-acting GLP-1RAs [41].
Overall, albiglutide provided no clinically significant weight loss compared with placebo, and the weight-reducing effect was below that reported for exenatide and liraglutide. This is likely owing to the albumin-based molecular size and structure of albiglutide, which might limit the access to and stimulation of GLP-1 receptors in the central nervous system as demonstrated by Hottenstein et al. in mice [16].
5 Safety
5.1 Immunogenicity
Non-neutralizing anti-albiglutide antibodies of low titers were reported in 3–7% of subjects treated with albiglutide [34–41]. Data on immunogenicity from the HARMONY 1-7 trials involved 2098 albiglutide-treated subjects. An analysis investigated the possible correlation between titers of anti-albiglutide antibodies in these patients and changes in HbA1c or FPG [12]. The changes from baseline in both HbA1c and FPG were similar in the groups of antibody-positive and antibody-negative subjects. Furthermore, no correlation between maximum antibody titers and FPG levels at the time of the maximum antibody titer was evident [12].
5.2 Adverse Events
The HARMONY trial program reported overall AE frequencies between 73 and 84% in the groups treated with albiglutide. Serious adverse events (SAEs) after treatment with albiglutide were much less frequent and varied between 3 and 15% (Table 4). Importantly, however, the four placebo-controlled HARMONY studies showed that subjects treated with albiglutide had frequencies of both AEs and SAEs similar to placebo [34–37]. In addition, albiglutide-treated groups overall demonstrated AEs and SAEs in line with the frequencies observed in the groups treated with various active comparators. Withdrawal in relation to treatment with albiglutide was observed in the range of 3–10% of subjects and was comparable to placebo [34, 36, 37]. The majority of reported AEs were injection-site reactions and gastrointestinal AEs such as nausea, diarrhea, and vomiting. Injection-site reactions were reported in 8–17% of subjects treated with albiglutide, which was typically higher than the incidences reported in the placebo groups and the different active comparator groups. Nausea, diarrhea, and vomiting tended to be more frequent following treatment with albiglutide as compared with both placebo and non-GLP-1RA active comparators, which is no surprise considering the well-described link between gastrointestinal AEs and the class of GLP-1RAs. However, the head-to-head trial against liraglutide demonstrated albiglutide to cause significantly less nausea and vomiting, whereas similar frequencies of diarrhea were observed [41]. The direct comparisons of albiglutide vs. exenatide and liraglutide demonstrated incidences of nausea of 26 vs. 40 and 10 vs. 29%, respectively [31, 41].
Monotherapy with albiglutide in the HARMONY 2 trial demonstrated low incidences (0–2%) of symptomatic hypoglycemia [35]. Furthermore, albiglutide as add-on to metformin and pioglitazone resulted in low incidences of symptomatic hypoglycemia in the area of 3% [34, 36]. Frequencies of symptomatic hypoglycemia between 10 and 18% were reported in studies including either sulfonylureas or insulin as add-on to albiglutide [37–41]. As would be expected, treatment with albiglutide caused lower incidences of hypoglycemia in direct comparisons to insulin and glimepiride [36, 38, 39]. Similar frequencies of hypoglycemia were reported after treatment with albiglutide and liraglutide in the HARMONY 7 study [41]. A very limited number of six severe hypoglycemic events in total have been reported with albiglutide in the HARMONY program [34, 37, 38, 40].
Seven cases of clinically diagnosed acute pancreatitis occurred in 3340 patient-years in albiglutide-treated patients compared with no adjudicated cases meeting the same criteria for active comparators or placebo [12]. In addition, the HARMONY program has reported two cases of pancreatic cancer. One albiglutide-treated subject experienced a fatal pancreatic metastatic carcinoma on day 694, and another subject treated with pioglitazone reported an SAE of pancreatic adenocarcinoma [12].
Overall, the majority of discontinuations were owing to withdrawal of consent or AEs. Injection-site reactions were frequent and led to discontinuation in 2% of all patients treated with albiglutide. The most frequent short-term AEs were the group of well-known gastrointestinal AEs. Interestingly, fewer of these seem to be elicited by treatment with albiglutide than other agents from the class of GLP-1RAs. This AE profile could be related to the limited central nervous system penetration of albiglutide and may be an important feature to discern this GLP-1RA from the other available agents.
6 Summary and Conclusion
The HARMONY program demonstrated albiglutide to cause placebo-corrected reductions in HbA1c of 0.8–1.0%. Furthermore, albiglutide was shown to reduce HbA1c to a greater extent than the commonly used oral anti-hyperglycemic medications glimepiride (sulfonylurea) and sitagliptin (DPP-4 inhibitor) [36, 40]. In patients treated with metformin (±sulfonylurea), albiglutide was reported to provide glycemic control comparable to what can be obtained by adding both long- and short-acting insulin [38, 39], whereas both pioglitazone and liraglutide caused larger reductions in HbA1c than albiglutide [37, 41]. Overall, the reported reductions in FPG tended to mimic the changes in HbA1c. The clinical trial program reported weight reductions at the placebo level in relation to treatment with albiglutide [34–37]. In the only study directly comparing albiglutide with another GLP-1RA, weight loss was significantly less with albiglutide 50 mg QW than with liraglutide 1.8 mg once daily—a mean difference of 1.5 kg that may be of clinical relevance for some patients [41].
Overall, in the clinical trials, albiglutide demonstrated a favorable safety profile compared with placebo, non-GLP-1RA comparators, and in particular in both direct and indirect comparison to other members of the GLP-1RA class (i.e., liraglutide and exenatide). Albiglutide caused less gastrointestinal (and other) AEs than liraglutide in the direct comparison [41]. Nonetheless, well-known AEs to treatment with GLP-1RAs such as nausea, diarrhea, and vomiting were in general slightly more frequently observed following treatment with albiglutide than placebo or active comparators from other classes of anti-hyperglycemic drugs. There was a safety signal of increased acute pancreatitis with seven incidences in the albiglutide-treated patients compared with none in the all comparators group. Altogether, there were no signals of increased malignant neoplasms or other critical safety issues, but the trials were in general too short and underpowered to detect a difference in the occurrence of such (unexpected) rare events.
The results of cardiovascular outcome trials are important to establish the safety profile of albiglutide, even more so in the light of the recent favorable cardiovascular outcomes reported with liraglutide and semaglutide treatment and the neutral effect of lixisenatide [28–30]. It is a clear limitation that the cardiovascular outcomes (and a consolidation of the general safety) for albiglutide will not be reported before 2019. Issues concerning convenience factors such as the need for time-consuming reconstitution (albiglutide and exenatide QW) compared with ready-to-use preparations (exenatide twice daily, lixisenatide, liraglutide, and dulaglutide), as well as QW dosing (exenatide QW, dulaglutide, and albiglutide) compared with daily injections (exenatide twice daily, lixisenatide, and liraglutide) might also affect prescriber and patient preference for one GLP-1RA over another. The actual implications of these issues in a real-life situation and whether it may favor the clinical use of and adherence to treatment with albiglutide are not certain. So what should we expect from this anti-hyperglycemic agent. In general, the preserved glycemic efficacy and favorable gastrointestinal effects may pave the way for use in patients not able to tolerate other GLP-1RAs because of gastrointestinal AEs. Likewise, the limited effect on body weight may lead to use in patients, who need glycemic control, but do not need to lose weight. As albiglutide at present ‘only’ offers glycemic control (and has no documented beneficial long-term cardiovascular and pancreatic safety), it is not surprising that this agent in USA is cheaper than the other members of the GLP-1RA class. However, a price even more similar to other drug classes, who offer almost the same, e.g., DPP-4 inhibitors, could be important to enhance the clinical use of albiglutide.
In conclusion, compared with other GLP-1RAs, albiglutide seems clinically non-inferior in terms of effects on glycemia, better in terms of gastrointestinal AEs, but inferior in terms of weight loss. The full risk-benefit profile will not be clear until reporting of the long-term cardiovascular outcome trial, HARMONY Outcome. Thus, despite a quite favorable short-term efficacy-safety profile, the verdict is still out as to whether the actual benefit of albiglutide includes a safe or even improved cardiovascular risk profile.
References
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38:140–9.
Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M, et al. Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: meta-analysis of randomised controlled trials. BMJ. 2011;343:d4169.
Kahn SE, Cooper ME, Del Prato S. Pathophysiology and treatment of type 2 diabetes: perspectives on the past, present, and future. Lancet. 2014;383:1068–83.
Göke B. Islet cell function: alpha and beta cells: partners towards normoglycaemia. Int J Clin Pract Suppl. 2008;159:2–7.
Meier JJ, Nauck MA. Is the diminished incretin effect in type 2 diabetes just an epi-phenomenon of impaired beta-cell function? Diabetes. 2010;59:1117–25.
Holst JJ, Gromada J. Role of incretin hormones in the regulation of insulin secretion in diabetic and nondiabetic humans. Am J Physiol Endocrinol Metab. 2004;287:E199–206.
Nauck MA, Homberger E, Siegel EG, et al. Incretin effects of increasing glucose loads in man calculated from venous insulin and C-peptide responses. J Clin Endocrinol Metab. 1986;63:492–8.
Holst JJ. The physiology of glucagon-like peptide 1. Physiol Rev. 2007;87:1409–39.
Hare KJ, Knop FK. Incretin-based therapy and type 2 diabetes. Vitam Horm. 2010;84:389–413.
Thazhath SS, Marathe CS, Wu T, et al. The glucagon-like peptide-1 receptor agonist exenatide inhibits small intestinal motility, flow, transit, and absorption of glucose in healthy subjects and patients with type 2 diabetes: a randomised controlled trial. Diabetes. 2016;65:269–75.
Flint A, Raben A, Astrup A, Holst JJ. Glucagon-like peptide 1 promotes satiety and suppresses energy intake in humans. J Clin Invest. 1998;101:515–20.
European Medicines Agency. Eperzan (European Public Assessment Report). Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPARPublic_assessment_report/human/002735/WC500165119.pdf. Accessed 2 Aug 2016.
Deacon CF, Nauck MA, Toft-Nielsen M, et al. Both subcutaneously and intravenously administered glucagon-like peptide I are rapidly degraded from the NH2-terminus in type II diabetic patients and in healthy subjects. Diabetes. 1995;44:1126–31.
Trujillo JM, Nuffer W. Albiglutide: a new GLP-1 receptor agonist for the treatment of type 2 diabetes. Ann Pharmacother. 2014;48:1494–501.
Blair HA, Keating GM. Albiglutide: a review of its use in patients with type 2 diabetes mellitus. Drugs. 2015;75:651–63.
Hottenstein CS, Szapacs ME, Maier CC. Investigation of blood-brain barrier penetration of albiglutide in mice. 76th Scientific Sessions of the American Diabetes Association. New Orleans, 10-14 June 2016;1044-P.
Leiter LA, Jones-Leone A, Acusta A, et al. Effects of mild to moderate renal impairment on albiglutide in type 2 diabetes. 76th Scientific Sessions of the American Diabetes Association. New Orleans, 10-14 June 2016;1020-P.
US Food and Drug Administration. Tanzeum (albiglutide): prescribing information. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125431s009lbl.pdf. Accessed 25 Jul 2016.
European Medicines Agency. Eperzan: product information. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_Product_Information/human/002735/WC500165117.pdf. Accessed 25 Jul 2016.
Young MA, Wald JA, Matthews JE, et al. Effect of renal impairment on the pharmacokinetics, efficacy, and safety of albiglutide. Postgrad Med. 2014;126:35–46.
Bush M, Scott R, Watanalumlerd P, et al. Effects of multiple doses of albiglutide on the pharmacokinetics, pharmacodynamics, and safety of digoxin, warfarin, or a low-dose oral contraceptive. Postgrad Med. 2012;124:55–72.
Hompesch M, Jones-Leone A, Carr MC, et al. Albiglutide does not impair the counter-regulatory hormone response to hypoglycaemia: a randomized, double-blind, placebo-controlled, stepped glucose clamp study in subjects with type 2 diabetes mellitus. Diabetes Obes Metab. 2015;17:82–90.
Nauck MA, Kemmeries G, Holst JJ, Meier JJ. Rapid tachyphylaxis of the glucagon-like peptide 1-induced deceleration of gastric emptying in humans. Diabetes. 2011;60:1561–5.
Umapathysivam MM, Lee MY, Jones KL, et al. Comparative effects of prolonged and intermittent stimulation of the glucagon-like peptide 1 receptor on gastric emptying and glycemia. Diabetes. 2014;63:785–90.
US Food Drug Administration, Center for Drug Evaluation and Research. Clinical pharmacology review, albiglutide (GSK716155). Available from: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/125431Orig1s000ClinPharmR.pdf. Accessed 5 Aug 2016.
Darpo B, Zhou M, Matthews J, et al. Albiglutide does not prolong QTc interval in healthy subjects: a thorough ECG study. Diabetes Ther Res Treat Educ Diabetes Relat Disord. 2014;5:141–53.
Fisher M, Petrie MC, Ambery PD, et al. Cardiovascular safety of albiglutide in the HARMONY programme: a meta-analysis. Lancet Diabetes Endocrinol. 2015;3:697–703.
Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375:311–22.
Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–44.
Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med. 2015;373:2247–57.
Rosenstock J, Reusch J, Bush M, et al. Potential of albiglutide, a long-acting GLP-1 receptor agonist, in type 2 diabetes: a randomized controlled trial exploring weekly, biweekly, and monthly dosing. Diabetes Care. 2009;32:1880–6.
Seino Y, Nakajima H, Miyahara H, et al. Safety, tolerability, pharmacokinetics and pharmacodynamics of albiglutide, a long-acting GLP-1-receptor agonist, in Japanese subjects with type 2 diabetes mellitus. Curr Med Res Opin. 2009;25:3049–57.
Seino Y, Inagaki N, Miyahara H, et al. A randomized dose-finding study demonstrating the efficacy and tolerability of albiglutide in Japanese patients with type 2 diabetes mellitus. Curr Med Res Opin. 2014;30:1095–106.
Reusch J, Stewart MW, Perkins CM, et al. Efficacy and safety of once-weekly glucagon-like peptide 1 receptor agonist albiglutide (HARMONY 1 trial): 52-week primary endpoint results from a randomized, double-blind, placebo-controlled trial in patients with type 2 diabetes mellitus not controlled on pioglitazone, with or without metformin. Diabetes Obes Metab. 2014;16:1257–64.
Nauck MA, Stewart MW, Perkins C, et al. Efficacy and safety of once-weekly GLP-1 receptor agonist albiglutide (HARMONY 2): 52 week primary endpoint results from a randomised, placebo-controlled trial in patients with type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetologia. 2016;59:266–74.
Ahrén B, Johnson SL, Stewart M, et al. HARMONY 3: 104-week randomized, double-blind, placebo- and active-controlled trial assessing the efficacy and safety of albiglutide compared with placebo, sitagliptin, and glimepiride in patients with type 2 diabetes taking metformin. Diabetes Care. 2014;37:2141–8.
Home PD, Shamanna P, Stewart M, et al. Efficacy and tolerability of albiglutide versus placebo or pioglitazone over 1 year in people with type 2 diabetes currently taking metformin and glimepiride: HARMONY 5. Diabetes Obes Metab. 2015;17:179–87.
Weissman PN, Carr MC, Ye J, et al. HARMONY 4: randomised clinical trial comparing once-weekly albiglutide and insulin glargine in patients with type 2 diabetes inadequately controlled with metformin with or without sulfonylurea. Diabetologia. 2014;57:2475–84.
Rosenstock J, Fonseca VA, Gross JL, et al. Advancing basal insulin replacement in type 2 diabetes inadequately controlled with insulin glargine plus oral agents: a comparison of adding albiglutide, a weekly GLP-1 receptor agonist, versus thrice-daily prandial insulin lispro. Diabetes Care. 2014;37:2317–25.
Leiter LA, Carr MC, Stewart M, et al. Efficacy and safety of the once-weekly GLP-1 receptor agonist albiglutide versus sitagliptin in patients with type 2 diabetes and renal impairment: a randomized phase III study. Diabetes Care. 2014;37:2723–30.
Pratley RE, Nauck MA, Barnett AH, et al. Once-weekly albiglutide versus once-daily liraglutide in patients with type 2 diabetes inadequately controlled on oral drugs (HARMONY 7): a randomised, open-label, multicentre, non-inferiority phase 3 study. Lancet Diabetes Endocrinol. 2014;2:289–97.
Phillips LK, Rayner CK, Jones KL, et al. Measurement of gastric emptying in diabetes. J Diabetes Complications. 2014;28:894–903.
Petersen AB, Christensen M. Clinical potential of lixisenatide once daily treatment for type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2013;6:217–31.
Hermansen K, Mortensen LS. Bodyweight changes associated with antihyperglycaemic agents in type 2 diabetes mellitus. Drug Saf. 2007;30:1127–42.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No external funding was used in the preparation of this article.
Conflict of interest
Andreas Brønden, Filip K. Knop, and Mikkel Christensen declare that they have no conflicts of interest that might be relevant to the contents of this article.
Rights and permissions
About this article

Cite this article
Brønden, A., Knop, F.K. & Christensen, M. Clinical Pharmacokinetics and Pharmacodynamics of Albiglutide. Clin Pharmacokinet 56, 719–731 (2017). https://doi.org/10.1007/s40262-016-0499-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-016-0499-8