
Abstract
Despite accumulating evidence linking screen-based sedentary behaviours (i.e. screen time) with poorer health outcomes among children and youth <18 years of age, the prevalence of these behaviours continues to increase, with roughly half of children and youth exceeding the public health screen time recommendation of 2 h per day or less. The purpose of this article is to provide an overview of key research initiatives aimed at understanding the associations between screen time and health indicators including physical health, quality of life and psychosocial health. Available evidence suggests that screen time is deleteriously associated with numerous health indicators in child and youth populations, including adiposity, aerobic fitness, quality of life, self-esteem, pro-social behaviour, academic achievement, depression and anxiety. However, few longitudinal or intervention studies have been conducted, with most of these studies focusing on physical health indicators. While most studies have used self-reported assessments of screen time, the availability of more objective assessment methods presents important opportunities (e.g. more accurate and precise assessment of sedentary time and screen time) and challenges (e.g. privacy and participant burden). Novel statistical approaches such as isotemporal substitution modelling and compositional analysis, as well as studies using longitudinal and experimental methodologies, are needed to better understand the health impact of excessive screen time, and to develop strategies to minimise or reverse the negative impacts of these behaviours. The evidence to date suggests a clear need for policy aimed at minimising the hazardous health consequences associated with screen time among children and youth.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
While television and video games are most often key contributors to screen time among children and youth, smartphones and tablets are gaining widespread use among children and youth and are becoming key contributors to screen time. |
Children and youth are engaging in screen time at an alarming rate with most children and youth not meeting the screen time guidelines of <2 h per day. |
Engaging in excessive amounts of screen time is significantly associated with hazardous health consequences including reduced quality of life, and poorer physical and psychosocial aspects of health. |
Given the amount of screen time already engaged in by children and youth away from school, adding to that time by providing tablets in class during school hours may not be prudent. |
1 Introduction
Screen-based sedentary behaviours (i.e. screen time) have recently been recognised as a significant contributor to adverse health (e.g. physical, mental) indicators in children and youth, independent of physical activity and other health-related behaviours [1]. Given the high prevalence of screen time in the paediatric population, this novel risk factor represents an important threat to public health. The purpose of this article is to provide an overview of key research initiatives aimed at understanding the associations between screen time and health indicators including physical health, quality of life (QoL), and psychosocial health. We will also identify gaps in the current research evidence, and suggest areas for future research in this emerging and important field of study.
2 Sedentary Behaviour
Historically, the term sedentary behaviour described a lack of physical activity, including physical activities that were performed at a low intensity and/or frequency [2]. Recent advances in the study and understanding of sedentary behaviour have led to sedentary behaviour now being defined as a distinct behavioural category [3] highlighted by the absence of energy expenditure. The contemporary definition of sedentary behaviour includes activities that are low in energy expenditure and has been conceptualised as any waking behaviour with an energy-expenditure equivalent of <1.5 metabolic equivalents, while in a sitting or reclining position [4]. Sedentary behaviours are not to be confused with physical inactivity (i.e. performing insufficient amounts of moderate- to vigorous-intensity physical activity) [4]. Sedentary behaviour does not include sleep, which has important restorative and health functions. Examples of common sedentary behaviours include watching television or sitting at a computer.
Sedentary behaviour comprises a variety of specific sedentary behaviours, which may include watching television, driving a car, working at a computer, smartphone, or tablet, playing video games, or reading [5]. Screen time is often the major contributor to overall sedentary time among children and youth [6] as transportation and/or work-related sedentary time, which may be prevalent in adult populations, are not necessarily relevant for the child and youth context. Screen time most often includes television viewing, recreational computer use, watching DVDs/videos and playing video games, and may also include smartphone and tablet use (e.g. engaging in social media, gaming, app use). While television and video games (i.e. gaming) were most often key contributors to screen time among children and youth, smartphones and tablets are gaining widespread use among children and youth and may already be key contributors to screen time.
3 Screen Time Recommendations
The American Academy of Pediatrics recommends children limit the amount of total screen time to <1–2 h per day [7]. For children under the age of 2 years, screen time is discouraged altogether. Other countries have adopted similar guidelines. For example, in Canada, the Canadian Society for Exercise Physiology has adopted guidelines for early years (0–4 years), children (5–11 years) and youth (12–17 years) [8]. For children <2 years of age, screen time is not recommended, while for children between the ages of 2 and 4 years, screen time should be limited to under 1 h per day. For children between the ages of 5 and 17 years, recreational screen time should be limited to under 2 h per day. The Australian Government Department of Health recommends children aged 5–12 years and young people aged 13–17 years should minimise the time they spend being sedentary every day [9].
4 Screen Time Prevalence
Screen time is prevalent among children and youth, with an increased volume of overall screen time in recent years [1]. Approximately 50% of school-aged children in North America are currently meeting published guidelines of <2 h per day of recreational screen time [10–12]. Available information suggests that total daily screen time has increased in recent years, as well as a general shift in the prevalence of specific sedentary behaviours [1]. Using the Health Behaviour in School Aged Children survey, Bucksch et al. found that self-reported television viewing increased from 2.2 to 2.6 h per day for 11-year-old boys and 2.4–2.1 h per day for girls between 2002 and 2010 (similar trends were seen in 13 and 15-year olds) [13]. In contrast, they reported that computer use increased from 1.3 to 3.1 h per day amongst 11-year-old boys and from 0.7 to 2.3 h per day for girls over the same period. These findings are consistent with other research, and suggest that the proportion of daily sedentary time spent using computers has increased substantially in recent years, while the proportion spent watching television has decreased [1].
Data in younger children are also now starting to emerge. A recently published systematic review found a few studies examining screen time among children <2 years of age [14]. In this review, Downing et al. reported mean daily television viewing time ranged from 37 to 331 min per day, while the proportion of children meeting the screen time recommendations (0 min of screen time) ranged from 2.3 to 83%. This review further analysed non-television screen time and found 35% of toddlers and 28% of infants used a cell phone the previous day. One study of infants (mean age = 25.7 months) published since this systematic review reported 93% of the sample watched television and 57% had used a computer [15]. In this study, among children <2 years of age, less than 25% met the screen time guidelines (0 min) on weekdays and weekends. Collectively, these studies are concerning and conclude that even children <2 years of age are already engaging in excessive amounts of screen time, which may have both short- and long-term health consequences.
5 Correlates of Screen Time
Screen time activities are correlated with several sociodemographic factors. Self-reported screen time is consistently higher in boys than girls [5, 10, 13, 16], and appears to increase with age. Bucksch et al. recently examined daily screen time across 30 countries and 443,821 participants aged 11–15 years [13]. Across all countries, they reported weekday screen time averaging 5.3 and 4.4 h per day for boys and girls at 11 years of age, 6.1 and 5.4 h per day at 13 years of age, and 6.5 and 5.4 h per day at 15 years of age. These estimates are similar to those in a cohort of 51,922 Canadian students in grades 6–12, who self-reported an average of 7.8 h of daily screen time [10]. Estimates of daily screen time in younger children are substantially lower; Leblanc et al. examined television viewing and computer and video game use in a sample of 5844 children aged 9–11 years in Australia, Brazil, Canada, China, Colombia, Finland, India, Kenya, Portugal, South Africa, the UK and USA [5]. They reported an average total screen time of 2.6 h per day across all sites, with 54% of participants exceeding 2 h per day. The specific screen-based behaviours that children and youth engage in also shift with age, with television viewing accounting for a greater proportion of total screen time in younger children, and computer use accounting for more screen time among older children and youth [10, 13]. Given the more recent widespread use of smartphones and tablets among children, it is currently unknown if there is a shift from computer use to smartphone or tablet use. Screen time is also positively associated with having a television or computer in the bedroom [5], being a current smoker [10], parental age and body mass index [16, 17]. Screen time is negatively associated with sleep [18], parental socioeconomic status, and having rules related to screen time [17]. In addition to the above sociodemographic factors, screen time is also associated with several physical and psychosocial health indicators, as we outline below.
6 Screen Time and Health
6.1 Physical Health Indicators
A wealth of cross-sectional and longitudinal observational studies have examined the relationship between screen time and physical health indicators in children and youth. In general, these studies suggest that increased levels of screen time are associated with worse health indicators, independent of other health behaviours such as diet, sleep and/or physical activity [1, 19].
The health indicator most widely studied with respect to screen time is adiposity [20–22]. In a systematic review and meta-analysis published in 2011 to support the development of the Canadian Sedentary Behaviour Guidelines, Tremblay et al. [12] identified 119 cross-sectional and 33 longitudinal studies examining the relationship between screen time (mostly television viewing) and adiposity in school-aged children and youth. Their results indicate that children who watched more than 2 h of television per day were more likely to be overweight or obese in cross-sectional studies. Further, longitudinal studies indicated a dose-response relationship, in that more daily screen time was associated with an increased risk of becoming overweight or obese. Although less research has been performed in pre-school children, the relationship between screen time and adiposity is similar to those seen in school-aged children and youth [21]. The systematic review by Tremblay et al. [22] was recently updated by Carson et al. [20] with similar results; television viewing and total screen time were associated with unfavourable results irrespective of study design. However, this updated review also identified a greater number of studies examining other forms of screen time, and found no consistent association between adiposity and either video game or computer use.
The relationships between screen time and other physical health indicators are similar to those observed for adiposity [20, 22]. Total screen time, and in particular television time, is positively associated with metabolic risk factors in school-aged children and youth [20, 22, 23]. Of note, these findings appear to be independent of physical activity [19, 23]. Finally, screen time has also been associated with reduced aerobic fitness and muscular strength/endurance in a limited number of studies, although the evidence base for these outcomes is much smaller than for adiposity or metabolic risk factors [20, 22].
Relatively few intervention studies have examined the relationship between screen time and physical health [20, 22]. The few studies that are available have focused primarily on screen time and adiposity [22]. Robinson et al. randomised students in third and fourth grade to receive a 6-month curriculum on reducing television and video game use (intervention) or receive no specific instruction related to screen use (control) [24]. In comparison to the control group, the intervention group experienced a 5.5-h per week reduction in self-reported television viewing and a 2.5-h per week reduction in video game use at study conclusion. These changes were accompanied by significant reductions in both body mass index (0.45 kg/m2) and waist circumference (2.3 cm), although there were no changes in aerobic fitness or self-reported physical activity. These findings are consistent, with a meta-analysis by Tremblay et al. concluding that interventions targeting screen time may result in significant reductions in body mass index in school-aged children [22]. It should be noted that the reductions in adiposity observed in response to reduced screen time do not appear related to increases in physical activity or energy expenditure. Although it is true that prolonged sitting time is associated with lower levels of energy expenditure [25], these findings are more likely owing to reductions in food intake that accompany reduced screen time [26]. This is supported by laboratory-based intervention studies that suggest screen time (especially television viewing) increases ad libitum food intake in paediatric populations [27, 28]. For example, Temple et al. provided 9- to 12-year-old, non-overweight children with 1000 kcal of a favourite snack food. In comparison to participants who ate while sitting quietly, those who ate while watching a continuous television programme consumed roughly twice as many calories [29]. Not surprisingly, televised food advertisements are also likely to play a role. Halford et al. exposed 9- to 11-year-old children to televised food and non-food advertisements, followed by an ad libitum meal [30]. Following the food advertisements, children consumed more food than after seeing the non-food advertisements. Further, overweight and obese children were more likely to recognise food ads, a trait that was itself positively associated with food intake. These and similar results from others [31] suggest that food advertisements result in increased food intake, and this effect may be particularly strong in children at risk for excess weight gain.
6.2 Quality of Life
QoL is defined as a measure of the physical and psychosocial dimension of health [32] and has been associated with a variety of chronic diseases. Studies examining the role of screen time in the QoL context have only emerged within the last 5 years. In one of the first (and largest) studies to examine screen time and QoL, Iannotti et al. examined nationally representative samples of both American (n = 14,818) and Canadian (n = 7266) school-aged children [33]. In both samples, screen time (defined as a) using a computer during free time [excluding homework], and b) watching television) was negatively related with QoL and physical health status (B = − 0.7 and −0.12, respectively). Other studies have recently emerged supporting this contention. For example, in a study of 2353 Australian adolescents (median age = 12.7 years), Gopinath et al. [6] reported on the prevalence on a variety of sedentary behaviours (i.e. reading, homework and screen time [consisting of television viewing, computer use and videogame use]). On average, 2 h per day was spent on reading and homework, and the overwhelming majority of sedentary behaviour time was spent engaged in screen time (~3.3 h per day). While total screen time was negatively associated with QoL, the difference between the first and third tertile was most pronounced for television viewing. These authors suggested that the passive nature of television viewing may be responsible for poorer QoL, while others have suggested the isolation and lack of social interaction that are indicative of television viewing may limit a child or youth’s cognitive and physical capabilities [34].
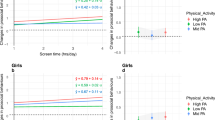
Studies have also explored demographic and health-related factors that may influence associations between screen time and QoL. For example, in a sample of 3040 Australian adolescents (11–18 years of age). Lacy et al. found boys reported significantly more screen time (2.1 h per day) compared with girls (1.4 h per day) [34]. While there were differences in the amount of screen time accrued across boys and girls, associations with QoL were consistent across the groups with those reporting high screen time use, also reporting lower QoL with an increase in 1 h per day in screen time being associated with significantly lower QoL scores (1.3 and 1.8 for boys and girls, respectively). The authors reported no differences in associations across age groups (above and below 15 years of age).
With respect to QoL, some have also suggested that the consequences of excessive screen time may be more pronounced among overweight and obese children and youth. For example, Goldfield et al. examined 358 overweight and obese Canadian adolescents (14–18 years of age) and found screen time duration was associated with reduced overall QoL and psychosocial QoL [35]. However, no association with physical QoL was found. One review of 34 studies examining QoL in overweight and obese children and youth provided early evidence (despite a small sample of studies) that children and youth who engaged in higher amounts of screen time had lower self-reported QoL [36].
6.3 Psychosocial Health
Although the volume of research on screen time and psychosocial health indicators is less than that seen for physical health indicators (especially adiposity), there is still a large body of published evidence dating back to the late 1950s [37]. Broadly speaking, the relationship between screen time and psychosocial health indicators seen in observational studies mirrors that seen for physical health indicators, with more screen time generally associated with worse outcomes [20–22]. Recent systematic reviews of observational studies [3, 38] have concluded that screen time is negatively associated with self-esteem, pro-social behaviour, academic achievement and psychological well-being and positively associated with depression. These reviews have also found positive associations of screen time with sleep problems, musculoskeletal pain, hyperactivity and internalising problems, and negatively associated with social support. In contrast to physical health indicators where television viewing was the only specific type of screen time consistently linked with deleterious outcomes, computer and video game use are consistently and negatively associated with psychosocial health indicators (self-esteem and pro-social behaviour) in the child and youth population [20].
Since the publication of these aforementioned reviews, data have continued to emerge providing convergent evidence on the hazardous consequences of screen time on psychosocial health among children and youth. For example, a large prospective Canadian study examined the relationship between screen time with anxiety and depression during adolescence [39]. Starting at 13 years of age, screen time as well as symptoms of depression and anxiety increased over time. Higher initial levels of anxiety and depression were both significantly associated with higher initial screen time. Research has also started to examine subgroups of children and adolescents, as well as different types of screen behaviour. For example, a recent study of obese adolescents found that time spent playing video games, and recreational computer time, was associated with depressive symptoms, even after controlling for relevant covariates including body mass index, caloric and carbohydrate intake, and intake of sugar-sweetened beverages [40]. Further, in a sample of 2482 Canadian youth in grades 7–12, Maras et al. [41] reported screen time duration was strongly associated with the severity of depression and anxiety, with video game playing and computer use being responsible for more severe depressive symptoms. Finally, new data have examined the possible dose-response association between screen time and depression in children and youth. Liu et al. conducted a meta-analysis of 16 studies (n = 127,714 children and youth) and found overall, those with more daily screen time (compared with no screen time) had a 12% increased risk of depression [42]. The association was not dose dependent (but rather, curvilinear) as 1 h per day of screen time was associated with a reduced risk of depression; however, 2 or more hours of screen time per day was associated with a continuously increasing risk of depression.
To date, only a handful of intervention studies have examined the links between screen time and psychosocial health indicators, most of which have also focused on physical activity [43–45]. In a 12-week randomised controlled trial, Robinson et al. provided the intervention group with dance classes and a series of home-based lessons focused on reducing screen time [44]. Despite no change in physical activity levels, the intervention did result in a significant reduction in household television use and dinners eaten while watching television, as well as a non-significant 5 h per week reduction in screen time. However, the authors observed no significant changes in self-esteem or academic performance. Goldfield et al. [43] provided children aged 8–12 years with an 8-week intervention targeting increased physical activity and reduced screen time. To achieve these dual goals, television viewing was limited by an electronic device, which shut off the television after a prescribed period. Participants in the intervention group could earn increased television viewing time by accumulating higher levels of objectively measured physical activity. The 8-week intervention resulted in nearly a doubling of moderate and vigorous physical activity levels (14 min per day at baseline to 24 min per day at follow-up) and a large reduction in television viewing (161 min per day at baseline and 44 min per day at follow-up) in the intervention group [46]. Further, reductions in television viewing were associated with increased physical and global self-worth [43]. Although these results are promising, broad conclusions on the impact of reductions in screen time and psychosocial indicators are precluded given the paucity of evidence available to date; future studies on this topic are certainly needed.
7 Limitations of the Research
There are several limitations to the body of literature examining screen time and health indicators among children and youth. First, the majority of studies to date have used cross-sectional designs, which do not allow for any causal inferences between screen time and health indicators to be made. For example, it is not possible to determine whether screen time causes depression, or vice versa. For many children and youth, screen time may be used as a coping mechanism to issues they may be facing including stress, anxiety and interpersonal conflict. In other words, it should also be recognised that screen time may function as a form of entertainment, and therefore may not be congruent with speculation that screen time is associated with depression. Very few studies have examined the dose-response association between screen time and health indicators [42], and future studies should design and implement appropriately designed studies that allow for more robust conclusions regarding dose and causality to be made.
Most studies to date have used self-reported measures of screen time, which may not be the most valid and reliable approach to measurement given limited cognitive capacity and unreliable recall in this population (i.e. children and youth) [47, 48]. Self-reported estimates of sedentary behaviour are prone to measurement error that may lead to incorrect inferences about sitting time (and associated outcomes) and thus bias study results [49]. For example, Saunders et al. have noted that some children report implausibly high amounts of daily screen time (e.g. >13.5 h per day) that, if true, would leave little time for school, sleep or other daily activities [48]. One objective method that is emerging that can capture the context within which screen time behaviours emerge is known as life logging and involves the digital capture of life activities through first-person point-of-view images [50]. In particular, wearable cameras have been suggested as one potential method for objectively measuring screen time [50, 51]. One such device that can capture these images is the SenseCam, a digital camera worn around the neck that captures images every 20 s throughout the day. However, this method of surveillance and data collection presents ethical challenges related to privacy and participant burden, as well as a large amount of data processing, when compared with self-reported screen time [52].
In addition to self-reported screen time, the majority of available studies also relied on children and youth self-rating a variety of health indicators such as QoL and depression, which may introduce additional error and bias in the study findings. As several studies summarised in this paper indicate, overall psychosocial health ratings are high. That is, samples of children and youth were already relatively healthy. Another important limitation in the literature that should be recognised is related to multitasking—engaging in multiple screen time behaviours simultaneously. At present, most questionnaires assess each screen time behaviour independently, and then sum the amount of time spent in each behaviour to calculate total screen time. Thus, estimates of total screen time may be inflated for individuals who perform multiple behaviours simultaneously (e.g. watch television while texting and also browsing the Internet on a laptop or tablet). Finally, despite the large number of studies performed to date, the overall quality of evidence linking screen time to health indicators has been identified as being low to very low quality [20], primarily consisting of cross-sectional studies using self- or proxy-report measures of screen time.
8 Future Research Directions
Regarding both physical and psychosocial health indicators, there is a relatively large body of cross-sectional evidence, but a lack of other more robust research designs. Thus, more research is needed using experimental methods, such as randomised interventions, when ethically possible, and longitudinal studies when they are not. To date the vast majority of research has focused on screen-based sedentary behaviours in isolation, ignoring other important health-related behaviours such as physical activity and sleep. However, given that these behaviours are likely to interact with each other, and with health indicators, it is important that future research investigates the health impact of various combinations of screen time and other health behaviours [53].
Novel statistical techniques, such as compositional analyses or isotemporal substitution modelling, may prove useful in this area [54]. Across a 24-h time period, children and youth engage in a combination of sleep, sedentary behaviours (including screen time) and physically active behaviours (of light, moderate or vigorous intensity). Increasing time spent in one of these behaviours results in less time spent in one or more of the other behaviors. That is, a fixed time in one behaviour can be substituted for a fixed time in another behaviour [55]. Isotemporal modelling allows the researcher to explore associations of alternating allocations of time in one behaviour with another while holding total time constant [55, 56]. Opportunities exist to use isotemporal substitution modelling to examine the potential effects of reallocating time between sleep, sedentary (or in particular, screen time) and physical activity behaviours on health outcomes such as QoL in children and youth.
The majority of screen time research was performed before the widespread adoption of tablet and/or smartphones, and accordingly such measures commonly included television and computer use. With the ever-increasing use of smartphones and tablets by children and youth, future research needs to examine whether there are unique health consequences to smartphone or tablet use compared with more traditional forms of screen time such as television or video games. Thus, while the health impact of a smartphone or tablet may be similar to that of a computer or television, this has yet to be examined. Further, it is unclear whether reading physical media (e.g. a book) has a different impact than reading the same text on a screen-based device. These are important questions to distinguish between the health impacts of screen-based devices, in comparison to the behaviours performed using those devices.
Evidence is emerging suggesting health benefits to breaking up prolonged bouts of sitting. For example, among adults, breaking up prolonged sedentary time has been associated with improved cardiometabolic risk factors [57–59]. One recent review identified 16 studies examining health consequences of breaking up prolonged sitting [57] and concluded breaking up prolonged sitting time and replacing with standing and/or light intensity physical activity was associated with metabolic outcomes. To date, only a small number of studies have examined the impact of prolonged sitting in children and youth. While Belcher et al. observed increases in blood sugar and insulin levels in response to uninterrupted sitting [60], others have observed no such changes [59, 61]. To our knowledge, no studies have examined the impact of uninterrupted sitting on QoL or psychosocial health outcomes. More research is therefore needed to determine the impact of sitting per se, in addition to the impact of screen time in children and youth.
9 Policy Implications
The above evidence suggests a clear need for policy aimed at minimising the hazardous health consequences associated with screen time among children and youth. One common approach is to create screen time guidelines and messaging aimed at parents, caregivers, teachers and healthcare workers, as has been done by the American Academy of Pediatrics and the Canadian Society for Exercise Physiology [7, 8]. Although this is an important first step, future research should investigate whether these guidelines are being properly understood and applied by their target audience.
Another approach may be to regulate specific forms of screen-based behaviours [62], such as restricting television food advertisements aimed at young children. The Canadian province of Quebec has banned junk food advertisements to children under the age of 13 years, resulting in an estimated Can$88 million reduction in junk food purchases within the province each year [63]. Though the impact of this programme on obesity rates in Quebec is unclear, it has been suggested that such a policy would reduce American childhood obesity rates by roughly 1% [64]. While such an approach would not reduce total screen time, it may nonetheless reduce the health impact of television viewing among young children.
Finally, individual schools may benefit from a conscious approach to screen time, employing screen-based devices only as needed. This may also improve academic performance, given that off-topic screen use has been found to reduce learning of both individual screen users, as well as other students within view of the screen [65]. Given the amount of screen time engaged in by children and youth away from school, adding to that time by providing tablets and other devices during school hours may not be prudent. While a plethora of literature exists highlighting the advantages of using tablets in the classroom, this literature most often does not recognise the emerging literature suggesting adverse health consequences of the technology. To minimise the potential distraction tablets may cause, teachers at least need to be educated about how best to implement these devices into their classroom so that learning can be maximised. Further, schools may also wish to investigate incorporating sit-stand desks into the classroom environment, which allow students to sit or stand based on their preference. Although this does not have a direct impact on screen time, it has nonetheless been shown to reduce daily sitting time [66], without impacting classroom management, concentration or physical discomfort [67].
10 Conclusion
Children and youth are engaging in screen time at an alarming rate with most children and youth not meeting the screen time guidelines of <2 h per day. Here, we have highlighted some of the hazardous health consequences of engaging in excessive amounts of screen time, which include both physical and psychosocial aspects of health. Well-designed trials that are currently accruing participants are examining innovative and more comprehensive strategies for reducing screen time. For example, Jussila et al. [68] are currently targeting 14 secondary schools in Finland and delivering a health education campaign providing youth feedback on their current screen time, as well as homework exercises, promotional videos and information for parents. In Australia, Babic et al. [69] are using a cluster-randomised design in eight secondary schools to deliver an intervention consisting of interactive seminars, eHealth messaging, behavioural contracts and parental newsletters, to reduce recreational screen time. While these interventions may demonstrate utility and effectiveness, such initiatives will need to be implemented and adopted as policy (e.g. school, community) for any population-based reductions in screen-based behaviours to be realised. Screen-based technology is rapidly changing and it is imperative that researchers recognise and keep pace with the shifts in trends and use of screen-based entertainment devices.
References
Saunders TJ, Chaput JP, Tremblay MS. Sedentary behaviour as an emerging risk factor for cardiometabolic diseases in children and youth. Can J Diabetes. 2014;38:53–61.
Pate RR, O’Neill JR, Lobelo F. The evolving definition of “sedentary”. Exerc Sport Sci Rev. 2008;36:173–8.
Suchert V, Hanewinkel R, Isensee B. Sedentary behavior and indicators of mental health in school-aged children and adolescents: a systematic review. Prev Med. 2015;76:48–57.
Sedentary Behaviour Research Network. Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours”. App Phys Nutr Metab. 2012;37:540–2.
LeBlanc AG, Katzmarzyk PT, Barreira TV, et al. Correlates of total sedentary time and screen time in 9–11 year-old children around the world: the International Study of Childhood Obesity. Lifestyle and the environment. PLoS One. 2015;10:e0129622.
Gopinath B, Hardy LL, Baur LA, et al. Physical activity and sedentary behaviors and health-related quality of life in adolescents. Pediatrics. 2012;130:e167–74.
American Academy of Pediatrics Council on Communications and Media. Children, adolescents, and the media. Pediatrics. 2013;132:958–61.
Tremblay MS, Carson V, Chaput JP, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016;41:S311–7.
Australian Government Department of Health. Australia’s physical activity and sedentary behaviour guidelines. Australian Government Department of Health; 2014.
Leatherdale ST, Ahmed R. Screen-based sedentary behaviours among a nationally representative sample of youth: are Canadian kids couch potatoes? Chronic Dis Inj Canada. 2011;31:141–6.
Fakhouri TI, Hughes JP, Brody DJ, et al. Physical activity and screen-time viewing among elementary school-aged children in the United States from 2009 to 2010. JAMA Pediatrics. 2013;167:223–9.
Tremblay MS, LeBlanc AG, Janssen I, et al. Canadian sedentary behaviour guidelines for children and youth. App Phys Nutr Metab. 2011;36:59–64.
Bucksch J, Sigmundova D, Hamrik Z, et al. International trends in adolescent screen-time behaviors from 2002 to 2010. J Adolesc Health. 2016;58:417–25.
Downing KL, Hnatiuk J, Hesketh KD. Prevalence of sedentary behavior in children under 2 years: a systematic review. Prev Med. 2015;78:105–14.
Vanderloo LM, Tucker P. An objective assessment of toddlers’ physical activity and sedentary levels: a cross-sectional study. BMC Pub Health. 2015;15:969.
Atkin AJ, Sharp SJ, Corder K, van Sluijs EMF. Prevalence and correlates of screen time in youth: an international perspective. Am J Prev Med. 2014;47:803–7.
Hoyos Cillero I, Jago R. Systematic review of correlates of screen-viewing among young children. Prev Med. 2010;51:3–10.
Hale L, Guan S. Screen time and sleep among school-aged children and adolescents: a systematic literature review. Sleep Med Rev. 2015;21:50–8.
Saunders TJ, Tremblay MS, Mathieu ME, et al. Associations of sedentary behavior, sedentary bouts and breaks in sedentary time with cardiometabolic risk in children with a family history of obesity. PLoS One. 2013;8:e79143.
Carson V, Hunter S, Kuzik N, et al. Systematic review of the relationships between sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Phys Nutr Metab. 2016;41:S240–65.
LeBlanc AG, Spence JC, Carson V, et al. Systematic review of sedentary behaviour and health indicators in the early years (aged 0–4 years). Appl Phys Nutr Metab. 2012;37:753–72.
Tremblay M, LeBlanc AG, Kho M, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. 2011;8:98.
Goldfield GS, Saunders TJ, Kenny GP, et al. Screen viewing and diabetes risk factors in overweight and obese adolescents. Am J Prev Med. 2013;44:S364–70.
Robinson TN. Reducing children’s television viewing to prevent obesity: a randomized controlled trial. JAMA. 1999;282:1561–7.
Saunders TJ, Chaput JP, Goldfield GS, et al. Children and youth do not compensate for an imposed bout of prolonged sitting by reducing subsequent food intake or increasing physical activity levels: a randomised cross-over study. Br J Nutr. 2014;111:747–54.
Epstein LH, Roemmich JN, Robinson JL, et al. A randomized trial of the effects of reducing television viewing and computer use on body mass index in young children. Arch Ped Adol Med. 2008;162:239.
Boulos R, Vikre EK, Oppenheimer S, et al. ObesiTV: how television is influencing the obesity epidemic. Phys Behav. 2012;107:146–53.
Saunders TJ, Chaput J-P. Is obesity prevention as simple as turning off the television and having a nap? Br J Nutr. 2012;108:946–7.
Temple JL, Giacomelli AM, Kent KM, et al. Television watching increases motivated responding for food and energy intake in children. Am J Clin Nutr. 2007;85:355–61.
Halford JCG, Boyland EJ, Hughes G, et al. Beyond-brand effect of television (TV) food advertisements/commercials on caloric intake and food choice of 5–7-year-old children. Appetite. 2007;49:263–7.
Harris JL, Bargh JA, Brownell KD. Priming effects of television food advertising on eating behavior. Health Psych. 2009;28:404.
McHorney CA. Health status assessment methods for adults: past accomplishments and future challenges. Ann Rev Pub Health. 1999;20:309–35.
Iannotti RJ, Kogan MD, Janssen I, Boyce WF. Patterns of adolescent physical activity, screen-based media use, and positive and negative health indicators in the US and Canada. J Adol Health. 2009;44:493–9.
Lacy KE, Allender SE, Kremer PJ, et al. Screen time and physical activity behaviours are associated with health-related quality of life in Australian adolescents. Qual Life Res. 2012;21:1085–99.
Goldfield GS, Cameron JD, Murray M, et al. Screen time is independently associated with health-related quality of life in overweight and obese adolescents. Acta Paediatr. 2015;104:e448–54.
Buttitta M, Iliescu C, Rousseau A, Guerrien A. Quality of life in overweight and obese children and adolescents: a literature review. Qual Life Res. 2014;23:1117–39.
Scott LF. Relationships between elementary school children and television. J Educ Res. 1958;52:134–7.
Costigan SA, Barnett L, Plotnikoff RC, Lubans DR. The health indicators associated with screen-based sedentary behavior among adolescent girls: a systematic review. J Adol Health. 2013;52:382–92.
Gunnell KE, Flament MF, Buchholz A, et al. Examining the bidirectional relationship between physical activity, screen time, and symptoms of anxiety and depression over time during adolescence. Prev Med. 2016;88:147–522.
Goldfield GS, Murray M, Maras D, et al. Screen time is associated with depressive symptomatology among obese adolescents: a HEARTY study. Eur J Pediatr. 2016;175:909–19.
Maras D, Flament MF, Murray M, et al. Screen time is associated with depression and anxiety in Canadian youth. Prev Med. 2015;73:133–8.
Liu M, Wu L, Yao S. Dose-response association of screen time-based sedentary behaviour in children and adolescents and depression: a meta-analysis of observational studies. Br J Sports Med. 2015;50:1252–8.
Goldfield GS, Mallory R, Parker T, et al. Effects of modifying physical activity and sedentary behavior on psychosocial adjustment in overweight/obese children. J Pediatr Psychol. 2007;32:783–93.
Robinson TN, Killen JD, Kraemer HC, et al. Dance and reducing television viewing to prevent weight gain in African–American girls: the Stanford GEMS pilot study. Ethnic Dis. 2003;13:S65–77.
Simon C, Wagner A, DiVita C, et al. Intervention centred on adolescents’ physical activity and sedentary behaviour (ICAPS): concept and 6-month results. Int J Obes. 2004;28:S96–103.
Goldfield GS, Mallory R, Parker T, et al. Effects of open-loop feedback on physical activity and television viewing in overweight and obese children: a randomized, controlled trial. Pediatrics. 2006;118:e157–66.
Atkin AJ, Ekelund U, Møller NC, et al. Sedentary time in children: influence of accelerometer processing on health relations. Med Sci Sports Exerc. 2013;45:1097–104.
Saunders TJ, Prince SA, Tremblay MS. Clustering of children’s activity behaviour: the use of self-report versus direct measures. Int J Behav Nutr Phys Act. 2011;8:48 (author reply 49).
Ainsworth BE, Caspersen CJ, Matthews CE, et al. Recommendations to improve the accuracy of estimates of physical activity derived from self report. J Phys Act Health. 2012;9(Suppl 1):S76–84.
Kelly P, Doherty A, Berry E, et al. Can we use digital life-log images to investigate active and sedentary travel behaviour? Results from a pilot study. Int J Behav Nutr Phys Act. 2011;8:44.
Kerr J, Marshall SJ, Godbole S, et al. Using the SenseCam to improve classifications of sedentary behavior in free-living settings. Am J Prev Med. 2013;44:290–6.
Kelly P, Marshall SJ, Badland HM, et al. An ethical framework for automated, wearable cameras in health behavior research. Am J Prev Med. 2013;44:314–9.
Saunders T, Gray C, Poitras V, et al. Combinations of physical activity, sedentary behaviour and sleep: relationships with health indicators in school-aged children and youth. Appl Phys Nutr Metab. 2016;41(6 Suppl 3):S283–93.
Chastin SFM, Palarea-Albaladejo J, Dontje ML, Skelton DA. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: a novel compositional data analysis approach. PLoS One. 2015;10:e0139984.
Mekary RA, Willett WC, Hu FB, Ding EL. Isotemporal substitution paradigm for physical activity epidemiology and weight change. Am J Epidemiol. 2009;170:519–27.
Buman MP, Winkler EA, Kurka JM, et al. Reallocating time to sleep, sedentary behaviors, or active behaviors: associations with cardiovascular disease risk biomarkers, NHANES 2005-2006. Am J Epidemiol. 2014;179:323–34.
Benatti FB, Ried-Larsen M. The effects of breaking up prolonged sitting time: a review of experimental studies. Med Sci Sports Exerc. 2015;47:2053–61.
Healy GN, Matthews CE, Dunstan DW, et al. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06. Eur Heart J. 2011;32:590–7.
Saunders TJ, Chaput JP, Goldfield GS, et al. Prolonged sitting and markers of cardiometabolic disease risk in children and youth: a randomized crossover study. Metabolism. 2013;62:1423–8.
Belcher BR, Berrigan D, Papachristopoulou A, et al. Effects of interrupting children’s sedentary behaviors with activity on metabolic function: a randomized trial. J Clin Endocrin Metab. 2015;100:3735–43.
Sisson SB, Anderson AE, Short KR, et al. Light activity following a meal and postprandial cardiometabolic risk in adolescents. Ped Exerc Sci. 2013;25:347–59.
Handsley E, Mehta K, Coveney J, Nehmy C. Regulatory axes on food advertising to children on television. Aus NZ Health Pol. 2009;6:1.
Dhar T, Baylis K. Fast-food consumption and the ban on advertising targeting children: the Quebec experience. J Market Res. 2011;48:799–813.
Kristensen AH, Flottemesch TJ, Maciosek MV, et al. Reducing childhood obesity through US federal policy: a microsimulation analysis. Am J Prev Med. 2014;47:604–12.
Fried CB. In-class laptop use and its effects on student learning. Comp Educ. 2008;50:906–14.
Clemes SA, Barber SE, Bingham DD, et al. Reducing children’s classroom sitting time using sit-to-stand desks: findings from pilot studies in UK and Australian primary schools. J Pub Health (Oxf). 2015. [Epub ahead of print].
Koepp GA, Snedden BJ, Flynn L, et al. Feasibility analysis of standing desks for sixth graders. Child Obes Nutr. 2012;12:89–92.
Jussila AM, Vasankari T, Paronen O, et al. KIDS OUT! Protocol of a brief school-based intervention to promote physical activity and to reduce screen time in a sub-cohort of Finnish eighth graders. BMC Public Health. 2015;15:634.
Babic MJ, Morgan PJ, Plotnikoff RC, et al. Rationale and study protocol for ‘Switch-off 4 Healthy Minds’ (S4HM): a cluster randomized controlled trial to reduce recreational screen time in adolescents. Contemp Clin Trials. 2015;40:150–8.
Acknowledgements
Jeff Vallance is supported by the Canada Research Chairs Program and a Population Health Investigator Award from Alberta Innovates-Health Solutions. Travis Saunders is supported by a Jeanne and J.-Louis Lévesque Research Professorship.
Author contributions
Jeff Vallance and Travis Saunders equally contributed to conceptualising and drafting the manuscript. Both authors provided critical input and feedback during the manuscript writing process.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Both authors declare that they have no conflicts of interest.
Funding
Travis Saunders is funded by a Jeanne and J.-Louis Levesque Research Professorship. Jeff Vallance is funded by the Canada Research Chairs Program and Alberta Innovates-Health Solutions.
Rights and permissions
About this article

Cite this article
Saunders, T.J., Vallance, J.K. Screen Time and Health Indicators Among Children and Youth: Current Evidence, Limitations and Future Directions. Appl Health Econ Health Policy 15, 323–331 (2017). https://doi.org/10.1007/s40258-016-0289-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-016-0289-3