
Abstract
Isfahan as an important industrial city has faced with air pollution recently. Thus, we assessed the spatial and temporal trends of ambient PM2.5, CO, SO2, and O3 and for estimating their health effect on Isfahan citizens between March 2018 and March 2019 through the AirQ+ software. Our results showed that citizens of Isfahan in almost 240, 167, and 134 of the days in the year has exposure to PM2.5, SO2, and O3 higher than the WHO daily guideline, respectively. Daily variations of PM2.5, CO, and SO2 concentration showed the increasing trend of pollutants in the morning to evening. The maximum concentrations of O3 were observed in the noonday. Also, the concentrations of these pollutants on Friday due to the holiday effect were higher than the weekdays. Except for O3, the PM2.5, CO, and SO2 concentrations in the cold months and cold seasons was higher compared with the hot months and hot seasons. The total number of deaths because of lung cancer, natural mortality, ischemic heart disease, chronic obstructive pulmonary disease,, stroke associated with ambient PM2.5 with the attributable proportion (AP) 11.43%, 11.63%, 15.96%, 15.15%, and 13.1% (95% CI) were 683, 19, 2, 202, and 55 cases, respectively. Therefore, the present study provides additional data for the provincial managers and politicians useful in planning proper strategies of air pollution control to decrease exposure and attributable mortalities.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Air pollution is a considerable environmental issue in cities in metropolitan cities of world [1]. Air pollution includes a variety of gaseous pollutants, particulate matters (PM), heavy metals, and polycyclic aromatic hydrocarbons (PAHs) compounds [2,3,4,5]. Outdoor air pollution and the resulted adverse health impacts cause considerable risk factors, especially in developing countries [6]. According to the pollutant type, level, type, time of exposure and adverse events due to air pollution can be categorized as acute and chronic outcomes [7]. In October 2013, ambient air pollution categorized as Group 1 carcinogenic for human as recommended by the International Agency for Research on Cancer (IARC) [8]. According to the epidemiological investigation done during the recent decades, being exposed to air pollutants is linked to elevated deaths because of ischemic heart disease (IHD), stroke, lung cancer (LC), chronic obstructive pulmonary disease (COPD) and acute lower respiratory infections (ALRI) [9]. About 87% of the world’s population lives in countries where the level of air pollution is higher than the limit recommended by regulatory agencies such as the World Health Organization (WHO) [10]. Based on the WHO report, about 80 present of premature mortalities are because of IHD and stroke, 14% of COPD and 6% of LC are resulted from air pollution [11]. Air pollution in addition to health effects increases the economic burden of countries, whereas, in 2016 the costs of air pollution were as much as the gross domestic product (GDP) in some countries such as India, Canada, and Mexico. In Iran, the economic burden of air pollution is estimated at $ 30 billion, or 2.48% of GDP [12]. Many types of research proved that Short- (acute) and long-term (chronic) exposure to the fine particulate matter (PM2.5) increases mortality and morbidity in humans owing to its chemical characteristics [13]. PM species are among the important air pollutants in urban areas [14, 15]. PM2.5 has natural and anthropogenic origins, thus, in urban areas, traffic is the main cause of release [16, 17]. Thorough the recent decades, increases in respiratory and cardiovascular illnesses (e.g. heart attacks, bronchitis, decrease in lung function, and asthma,) and rate of mortality in the residents of cities are highly associated with atmospheric particulate matter [18]. The epidemiological studies demonstrated a significant correlation between PM2.5 exposure and increased risk of mortality [17, 19]. So that, A 10 μg/m3 elevation in the ambient PM2.5 is because of elevated death risk of all causes (4%), LC (9%), COPD (9%), and IHD (17%) [20, 21]. According to the reports, in 2015 approximated that chronic exposures to outdoor PM2.5 results in 4.2 million early mortality all over the world [22, 23]. Although, PM2.5 is extensively applied for the health effect evaluation of air pollution, the gaseous pollutants, like NO2, CO, O3 and SO2, directly affect the elevated morbidity and mortality rates [13]. The number of deaths or hospitalizations due to exposure to air pollution can be estimated using the Health Impact Assessment (HIA) method. [24]. AirQ+ model has been recently applied for assessing the health effect of outdoor air pollution in different countries [25]. The WHO introduced AirQ+ software, by using outdoor air pollution information, overall and at-risk people of the city, baseline incidence (BI per 105 cases), relative risk (RR) and different epidemiological information, are able to estimate natural mortality as well as other mortalities because of ALRI, COPD, IHD, LC, and stroke [26]. Isfahan is a biggest city of Iran that has faced with serious air pollution because of unsustainable development, densely vehicular traffic and lack of outdoor air quality standards along with high daily consumptions of fossil fuels and associated emissions [27, 28]. Thus, the current study was carried out with the following aims: i) investigating the daily, weekly, monthly and seasonal variation in PM2.5, CO, SO2 and O3 in ambient air of Isfahan, Iran; and ii) estimating all-natural mortality and other mortalities because of COPD, LC (adults ≥30 years), IHD, and stroke (adults ≥25 years) due to short and long-term exposure to PM2.5 and O3 in the Isfahan between March 2018 and March 2019 through WHO AirQ+ software.
Material and method
Study area
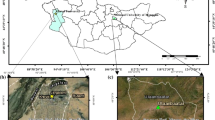
Isfahan city, with a population of more than two million, is the most populous city in central Iran. Isfahan is a large city (551 km2) and is also one of the most beautiful cities worldwide and one of the industrial hubs of Iran. It is between longitude 59°39′E and latitude 32°38’N and 1570 m above sea level [29]. Figure 1 indicates the Isfahan Map and Air quality monitoring stations.

The Map of the study area and Air quality monitoring stations
Data collection and processing
Of 16 Isfahan air pollution monitoring stations, seven ones were related to the Isfahan Department of Environment (IDOE) and nine ones were related to Isfahan Municipality. The hourly PM2.5, CO, SO2 and O3 concentrations were gathered from the stations between March 21, 2018 and March 20, 2019. The PM2.5, CO, SO2 and O3 values were analyzed using Excel software based on the WHO criteria [30, 31]. The 24 h averages for PM2.5 and SO2; and Sum of ozone means more than 35 ppb (SOMO 35) for O3 was calculated based on WHO Guideline [26]. Thus, merely valid values related to the stations were analyzed through AirQ+ software. To process PM2.5, CO, SO2 and O3 data and to construct the graphs, Excel and R software was applied, respectively. Geographic Information System (GIS) (V.10.1) was also employed for the air pollutants spatial distribution level. The IDW method was used for generating maps of annual means.
Baseline mortality and population data
The Isfahan population between 2018 and 2019 regarding the all age groups, ≤5 years, ≥25, and ≥ 30 was achieved from the Statistical Centre of Ministry of Health and Medical Education, Iran. Regarding the death rates according to age in Isfahan between 2018 and 2019 provided by the Isfahan University of Medical Sciences, the BI numbers of natural mortality (because of all-natural reasons) and different mortality causes because of LC, IHD, COPD, and stroke were determined by integrated exposure-response (IER) model.
Health risk assessment (HIA)
The PM2.5 and O3 health outcomes on those at risk was measured using the AirQ+ software based on the WHO through the annual mean of PM2.5 and O3 and at-risk population, BI (per 100,000 population), a cutoff point for consideration (10 μg/m3 reported by WHO) and RR. Therefore, the natural mortality (because of all-natural reasons) and other mortalities because of COPD, LC (adult cases over 30 years), IHD, and stroke (adult cases over 25 years) can be estimated [32]. This method is based on the attributable proportion (AP) considered as the health effect section because of air pollution in people at risk (Eq. (1)) [26]:
RR(c) presents the RR for the health consequences in the cases after exposure to air pollutants (c), and p(c) is the rate of cases in the exposure category (c).
The RR is measurable using Eq. 2.
β indicates the 95% CI, X represents the level of air pollutant, Xo indicates the data of the counterfactual. The health outcomes (per 100,000 population) or (BE), as well as the overall number of AP related to the exposure (NE), are measurable using Eqs. (3) and (4), respectively [33]:
B is the baseline prevalence of the health outcomes (per 100,000 population). NE is measurable using the equation below:
N represents the number of people at risk.
Results and discussion
Temporal and spatial variations of air pollutants concentration
The annual variations
Table 1 summarizes the annual mean, minimum, and maximum levels of PM2.5, CO, SO2, and O3 in the 16 monitoring station of Isfahan from 2018 to 2019. These values for PM2.5 was recorded 2.03, 606 and 30.14 ± 25.02 μg/m3, respectively. The annual mean PM2.5 levels is approximately 3 and 2.5 times higher compared with the WHO recommendation (10 μg/m3) and US-EPA Standards (12 μg/m3), respectively. The CO, SO2, and O3 were analyzed in 14, 12, and 2 stations, respectively. The mean annual concentration of CO, SO2, and O3 in monitoring stations was 2.54 ± 1.76, 24.46 ± 30.68, and 42.2 ± 27.86 μg/m3, respectively. During the study period the residents of Isfahan city about 240 days (65% of the days of the year) were exposed to the daily mean PM2.5 concentration higher compared with the WHO guideline (25 μg/m3). These values in Al-Hemond et al. 2019 and Guo et al. 2017 investigations were 6 and 7 times higher than the WHO guideline, respectively [34, 35].
The count of days with 24 h mean of SO2 and O3 higher than the WHO recommendation (20 and 50 μg/m3) was 167 and 134 days that The number of days with 24 h mean of SO2 and O3 higher than the WHO recommendation (20 and 50 μg/m3) was 167 and 134 days that these values for PM2.5 and O3 in Ahvaz (2014–2015) was 302 and 186 days [36, 37]. The reason for this is the high temperature and solar radiation and the photochemical reactions in the production of O3. Also, the presence of various industries and deserts all over this city and dust storms of the Middle East involved a role in increasing PM2.5 concentrations.
Figure 2 (a, b and c) indicates distribution of PM2.5, SO2 and CO levels in the monitoring stations using ArcGIS software except for O3 (due to lack of data on all stations). The distribution of PM2.5, SO2 and CO approximately follows a similar pattern. According to Fig. 4, the highest PM2.5, SO2 and CO concentration was found for the north, northwest, south and center. The following reasons can be mentioned for the high concentration of PM2.5, SO2 and CO in such areas: i) In the north, because of the highways, bus terminal, and the main line of the city buses; ii) In the northwest because of the monitoring station being near the main squares, and also stone-cutting industries and farming activities; iii) In the south and center because of the high population density, huge administrative and commercial buildings, and high traffic; iv) In the east, owing to the beltway, and the elevated transportation of diesel cars, the airport, and farming and road building activities. High concentrations of Criteria pollutants were reported in areas near main highways and those with terminals, higher traffic volume and population, as well as industrial and farming lands. Thus those living in such regions are more vulnerable against cardiovascular and respiratory disorders [9, 38,39,40,41].

The zoning of the annual concentration of PM2.5, SO2 and CO in urban areas of Isfahan
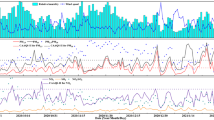
The hourly and daily variations
The mean hourly and daily concentration of PM2.5, CO, SO2, and O3 of all hourly concentration during the study period 2018–2019 are indicated in Fig. 3 (a,b,c and d) and Fig. 4 (a,b,c, and d), respectively. These are the results of the interaction between photochemical reactions, emission sources, and meteorological factors [42, 43]. Fig. 3a illustrates that the hourly concentrations of PM2.5 increases in 4 phases. The first phase begins from 6:00 to 9:00 a.m., the second phase from midday (11:00 a.m. to 13:00), the third phase from 17:00 to 19:00, and the last phase from 21:00 to 22:00. Daily variations of concentration of CO and SO2 follow almost the same pattern. So that, the highest concentration of CO and SO2 were observed between 13:00–15:00 and 12:00–16:00, respectively (Fig. 3b and c).

The mean hourly variations of PM2.5, CO, SO2, and O3 concentration

The daily variations of all hourly concentrations of PM2.5, CO, SO2, and O3
The reason for the increasing trend of pollutants in the morning to evening has directly correlated to the road traffic caused by the opening (morning) and closure (afternoon) of offices and schools, construction and demolition activities and families shopping, and so on. Also, the increasing trend of pollutants such as PM2.5 in the nighttime from 2.00 a.m. can be due to declining the temperature and low mixing height and weak wind and the occurrence of the inversion. Al-Hemoud et al. (2019) and Faridi et al. (2019) showed that mean hourly variations of air pollutants concentration exactly was related to road traffic [34, 42]. The daily peaks of PM2.5, NO2, SO2, and CO in the morning and the evening was mostly attributed to traffic emissions [44].
The trend of O3 concentration was increased since 7:00 a.m., so that the maximum concentrations was observed in midday between 13:00 and 16:00 and minimum concentrations in the late night (23:00–2:00 a.m.) that are related to solar radiation intensity (Fig. 3b). According to Fig. 3b, a small peak of O3 was seen between 3:00–4:00 a.m. Given that there was no photochemical reaction as well as ozone generation during the night, the reason can only because of horizontal and vertical transportation of ozone from other regions [42, 45]. In Iran, Saturday to Thursday are weekdays, and weekend is Friday. With this explanation, daily variations of PM2.5, CO, SO2, and O3 in Fig. 4a, b, c, and d indicated that the trend of these pollutant changes follows a similar pattern. So that the concentration of pollutants decreases from Saturday to Friday and the lowest concentration of pollutants was seen on weekends, ie Friday. The increase in these pollutants on weekdays can be attributed to the start of schools and office activities, which leads to increased concentrations of air pollutants due to congestions and road traffic. But, the reduction in the concentration of these pollutants at the weekend (Friday) is due to the “holiday effect” which leads to reduced vehicle traffic and other emission sources [42]. The Kuerban et al. (2020) indicated that, in North China, the PM2.5, PM10, SO2, NO2, and CO concentrations on the weekend were lower than weekdays [44]. Based on Fig. 4, almost a small decrease was found in pollutant levels on Tuesday which may be due to the car-free Tuesday’s plan that is running in Isfahan in recent years.
The monthly and seasonal variations of air pollutants
The monthly and seasonal box plot graph of the hourly average level of PM2.5, CO, SO2, and O3 thorough the research period 2018–2019 is indicated in Figs. 5 and 6, respectively. According to Fig. 5a the PM2.5 concentrations trend in cold months (October, December, November, and January) were more compared with others. Also, the lowest and highest PM2.5 concentration was related to October (40.26 μg/m3) and February (20 μg/m3). The highest and lowest CO level were found in March (2.74 mg/m3) and October (1.28 mg/m3), respectively (Fig. 5 b). SO2 concentrations in November (34.98 μg/m3) and February (37.83 μg/m3) was greater than the other months (Fig. 5c). Based on Fig.5d, O3 concentration enhanced by an increase in air temperature, so that O3 concentrations had the highest and lowest concentrations in June (83.87 μg/m3) and March (10.25 μg/m3), respectively.

The monthly box plot graph of the hourly mean concentration of PM2.5, CO, SO2, and O3

The seasonal box plot graph of the hourly mean concentration of PM2.5, CO, SO2, and O3
Based on the seasonal variations of the hourly PM2.5 levels (Fig. 6a), the PM2.5 level in cold seasons was more than the warm ones. With the start of autumn, temperatures begin to decrease, so the atmosphere starts to reverse the process. This trend of PM2.5 variation and its increase in the cold seasons have been announced earlier [17, 46, 47]. The seasonal variations of CO in Fig. 6b showed that the concentration of CO is as follows: spring > winter ˃ summer ˃ autumn. Based on Fig. 6c, the mean SO2 levels in the winter was more compared with the other seasons.
According to Fig. 6a, most fluctuations in PM2.5 and SO2 concentrations are related to seasonal changes. So that, the pattern of increasing the concentration of these pollutants in cold seasons are mostly ascribed to: i) The temperature inversion as well as stability of weather during cold seasons because of climate conditions, like low winds and mixing height, and temperatures [42, 48, 49]; ii) the decline of temperature and an increase in to use fossil fuels in Residential, commercial, and industrial regions that can be considered as an important emission sources of air pollutants during the cold seasons [48, 50] iii) A drop in O3 concentration, the subsequent, decline of hydroxyl radical, and resulting, the decrease in the oxidation potential in winter.
According to a similar study in Tehran, the average concentration of PM2.5 in winter and fall was more than summers and springs [51]. In contrast to our research, studies in Hamadan, Ilam, Ahvaz (Iran) and India found that PM2.5 level in warm seasons because of high temperatures, low wind as well as speed severity of sand storms are higher compared with other seasons [13, 37, 52, 53]. Also, Yousefian et al. in Tehran (2020) and Geo et al. in Beijing (2017) Showed that the concentration of PM2.5, NO2, SO2, and CO in the cold seasons because of decrease sunshine time, temperature inversion, and air stability was higher than the warm seasons [35, 51].
The O3 level demonstrates an inverse seasonal trend Compared to PM2.5, SO2, and CO, so that, the highest mean concentrations of O3 with a value of 76.34 μg/m3 related to the summer season, which was higher than in other seasons’ values (Fig. 6d). The results of similar studies showed that the O3 concentrations within summers and springs were significantly more than that of other seasons [53, 54].
The high O3 concentration in the warm seasons, especially in summer, is mainly attributed to sun radiation due to the rising daylight and sunshine hours and increasing the surface temperatures, which all increasing ozone-producing photochemical reactions [35, 55]. Solar radiation and high temperature with O3 production are positively correlated [56, 57].
Health risk assessment of exposure to PM2.5 and O3
Table 2 presents the health impacts of short and long-term exposure to ambient PM2.5 level more than 10 μg/m3 achieved from the AirQ+ software. The AP of 11.43% (95% CI: 7.62–14.86) was calculated for the natural mortality for PM2.5 levels and the excess death cases of 683 (454–887) cases was approximated. Comparing the rate of natural mortality due to PM2.5 in similar investigations indicated that the related cases in the current research was lower compared with other investigations. For instance, in Tehran, the rate of those attributable to long-term exposure to PM2.5 from 2015 to 2016 and 2017 to 2018 was 5073 and 6710 cases, respectively [33, 58]. Karimi et al. (2019) in Ahvaz reported 4061 deaths because of long-term exposure to PM2.5 from 2006 to 2015 [25]. Also, Manojkumar et al. (2019) reported 90,807, 57,812 and 26,635 deaths because of long-term exposure to PM2.5 in Delhi, Chennai, and Lucknow, respectively [59]. The high number of deaths because of long term exposure to PM2.5 in India, Tehran, and Ahvaz in comparison with our research may be the high at-risk population as well as high PM2.5 concentration in such research. We estimated that on average 11.43% (7.59% -14.84%) of deaths in Isfahan in 2018–2019 was due to long term exposure to PM2.5 that it was 15% reported by a relevant research in Tehran [20]. The number of deaths because of respiratory diseases due to long-term exposure to O3 with AP 0.07% (95% CI: 0.03–0.12) was 0 (0–1) cases which is negligible. This value in the study conducted in Ahvaz during 2016–2017 was reported 1 (0–2) case [25]. In our research, the natural death rate because of short-term exposure to PM2.5 with AP 0.63% (95% CI: 0.23–1.02) during 2018–2019 was 38 (14–61) cases. The death rate of 131 cases was reported from Hamadan towing to short-term exposure to PM2.5 [13]. According to Table 2 the total natural death rate because of short-term exposure to O3 was 1 negligible case.
Also, based on Table 2, the total death rate from Lang cancer due to long term exposure to PM2.5 with AP 15.96% (95% Cl: 7.61–23.22%) in 2018–2019 was estimated 2 (6–17) cases. In similar studies were obtained the death rate because of long-term exposure to PM2.5 owing to LC in Islamabad and Tabriz were 24 and 7 cases [46, 48]. Yarahmadi et al. (2018) in Tehran reported 427 deaths from LC were because of long-term exposure to PM2.5 [58]. The difference between death rates due to LC reported in our research and Yarahmadi et al. study may be the differences in the baseline death rates since the at-risk population in Tehran was more than the Isfahan. LC is the fourth reason for mortality because of outdoor air pollution, so that, PM2.5 can penetrate the lungs and secrete cytokines and oxidative stress resulting in LC [33, 60]. According to Boldo et al., 15 and 20 μg/m3 decrease in ambient PM2.5 level can reduce nearly 1296 and 1901 causes of mortality in 23 European cities [61]. In the current research, on average 2.66% (8–22.66%) of deaths from LC was because of exposure to PM2.5 for a long time. Ansari et al. (2019) reported that 17.36% of deaths because of LC in Tehran from 2017 to 2018 resulted from exposure to PM2.5 for a long time [33].
The total mortality of COPD attributable to PM2.5 during 2018–2019 with AP 13.41% (95% Cl: 8.08–19.84%) was estimated 19 (12–29) cases (Table 3). The mean rate of COPD mortality due to exposure of PM2.5 for a long time in Rome, Ahvaz and Tehran was 279, 75 and 158 cases [17, 25, 58]. In the present study, on average 13.1% (8.27–20%) of deaths because of COPD was due to long-term exposure to PM2.5 thorough the research. This value in in Mashhad was 4.5% [62]. In our study, the contradiction between the numbers of deaths from COPD with other studies may be due to the difference in the value of baseline mortalities.
Based on the WHO, IHD, stroke, and COPD are respectively the first, second and third reasons for mortality because of exposure to air pollution (WHO, 2014). There was an association between 10 μg/m3 increase in the atmospheric PM2.5 levels and 25% increase in mortality due to IHD and 0.51% increase from cardiovascular admissions [17, 63]. The overall death rates of IHD due to PM2.5 in 2018–2019 with AP 15.15% (95% Cl: 9.61–30.2%) was estimated 202 (128–403) cases, respectively (Table 2). The studies conducted in Taiwan and Iran (Tehran) 1477 to 3797 people died of IHD because of PM2.5, respectively [64, 65]. The comparison of our findings with the mentioned investigations indicated that the death rate of IHD in Tehran was more compared with the Isfahan since those at risk and PM2.5 levels are higher in Tehran. The annual average PM2.5 level in Tehran was 49 μg/m3 [66], which was 30.17 μg/m3 in our research. The present study estimated that on average 15.15% (9.6–30.23%) of mortality due to IHD thorough the research was because of exposure to PM2.5 for a long time, which was 17.4% in a relevant research in Tehran from 2006 to 2015 [42].
Many epidemiological studies indicated a positive correlation between stroke and exposure to ambient PM2.5 level for a long time [67,68,69]. Increasing every 5 μg/m3 in the PM2.5 level increased hazard ratio nearly 1.11 (95% CI: 1.05, 1.17) for the occurrence and mortality of stroke [69]. The mortality rate because of stroke has an association with exposure to PM2.5 for a long time between 2018 and 2019 with AP 13.1% (95% Cl: 6.99–20.44%) was estimated to be 55 (30–86) cases (Table 2). According to the similar studies, the death rates because of Stroke in Tehran from 2015 to 2017 due to ambient PM2.5 were 1500 and 1145 cases, respectively [33, 64]. The difference between the death rates owing to Stroke in our research with similar investigations can be the differences in the baseline death rates. In our research, 13% (7.09–20.33%) of mortality because of stroke was associated with exposure to PM2.5 for a long time thorough the research.
Conclusion
This study was done for investigating daily, weekly, monthly and seasonal differences of PM2.5, CO, SO2, and O3 and assessing the health risk of short- and long-term exposure to ambient air pollutants in Isfahan during 2018–2019. We used the AirQ+ software for estimating natural mortality as well as other mortalities because of COPD, LC, IHD, and stroke resulting from long-term exposure to PM2.5. Based on our results, the annual average concentrations of PM2.5, O3, SO2, and CO from 2018 to 2019 were between 30.17, 42.2, 24.46 μg/m3 and 2.54 mg/m3, respectively. The annual mean PM2.5 levels were approximately 3 times more compared with the WHO recommendation. Also, our results showed that those living in Isfahan during 2018–2019 in almost 240, 167, and 134 of the days during 1 year has exposure to PM2.5, SO2, and O3 over than the WHO daily recommendation (25, 20 and 50 μg/m3), respectively. Daily variations of PM2.5, CO, and SO2 concentration showed the increasing trend of pollutants in the morning to evening which has directly correlated to the road traffic. The maximum concentration of O3 was observed in midday 13:00 and 16:00 that are related to solar radiation intensity. The concentration of PM2.5, CO, SO2, and O3 on weekends (Friday) due to the “holiday effect” (low traffic and other sources of emission) was lower than the weekdays. The monthly and seasonal differences in PM2.5, CO, and SO2 showed that approximately, the concentrations of these pollutants in the cold months and cold seasons were more compared with the hot months and hot seasons. But, the concentration of O3 due to solar radiation and increasing ozone-producing photochemical reactions in warm months and seasons was higher than in other months and seasons. The mortality rate resulting from natural death, COPD, LC, IHD, and stroke showed an association with ambient PM2.5 were 683, 19, 2, 202, and 55, respectively. Based on our study estimation, 11.43% of the natural mortality, 2.66% of LC, 13.1% of COPD, 15.15% of IHD, and 13% of stroke mortalities in Isfahan was associated with long-term exposure to ambient PM2.5. We indicated that the high mortality rate due to air pollution in Isfahan can cause several economic burden. Thus, according to the daily, monthly and seasonal variations of critical air pollutants in Isfahan, provincial managers as well as politicians should use proper models and techniques to control air pollution in order to decrease the mortalities due to air pollutants.
References
Mohammadi A, Ghassoun Y, Löwner MO, Behmanesh M, Faraji M, Nemati S, et al. Spatial analysis and risk assessment of urban BTEX compounds in Urmia, Iran. Chemosphere. 2020;246:125769.
Hanedar A, Alp K, Kaynak B, Baek J, Avsar E, Odman MT. Concentrations and sources of PAHs at three stations in Istanbul, Turkey. Atmos Res. 2011;99:391–9.
Hanedar A, Alp K, Kaynak B, Avşar E. Toxicity evaluation and source apportionment of polycyclic aromatic hydrocarbons (PAHs) at three stations in Istanbul, Turkey. Sci Total Environ. 2014;488:437–46.
Ozturk H, Alp K, Hanedar A, Avsar E, Malak U. Partitioning of heavy metals in the Istac medical waste incinerator. Glob Nest J. 2013;25:37–48.
Saatcioglu T, Alp K, Hanedar A, Avsar E. Effect of the Marmaray project on air pollution in Istanbul: an IVE model application. Fresenius Environ Bull. 2011;20(9A):2340–9.
Jafari AJ, Kermani M, Arfaeinia KRR. The Effect Of Traffic On Levels, Distribution And Chemical Partitioning Of Harmful Metals In The Street Dust And Surface Soil From Urban Areas Of Tehran, Iran. Environ Earth Sci. 2018;38:77.
Lin CW, Yeh JF, Kao TC. Source Characterization Of Total Suspended Particulate Matter Near A Riverbed In Central Taiwan. J Hazard Mater. 2008;157:418–22.
IARC. Outdoor air pollution a leading environmental cause of Cancer deaths, International Agency For Research On Cancer; 2011.
Miri M, Ghassoun Y, Dovlatabadi A, Ebrahimnejad A, Löwner M. Estimate annual and seasonal Pm1, PM2.5 and PM10 concentrations using land use regression model. Ecotox Environ Safe. 2019;174:137–45.
Chen Y, Ebenstein A, Greenstone M, Li H. Evidence on the impact of sustained exposure to air pollution on life expectancy from China’s Huai River policy. P Natl Acad Sci. 2013;110:12936–41.
Conti GO, Heibati B, Kloog I, Fiore M, Ferrante M. A review of Airq models and their applications for forecasting the air pollution health outcomes. Environ Sci Pollut Res. 2017;24:6426–45.
Tavakoly M. Estimation of acute air pollution conditions in tehran due to the concentration of ozone and particulate matter using artificial neural network. masters thesis, masters thesis, ministry of science, research, technology tarbiat modares; 2013 .
Asl FB, Leili M, Vaziri Y, Arian SS, Cristaldi A, Conti GO, et al. Health impacts quantification of ambient air pollutants using Airq model approach in Hamadan, Iran. Environ Res. 2018;161:114–21.
Avsar E, Hanedar A, Toroz I, Alp K, Kaynak B. Investigation of PM10 concentrations and noise levels of the road sweepers operating in Istanbul-Turkey: a case study. Fresenius Environ Bull. 2010;19:2033–9.
Farrokhzadeh H, Jafari N, Sadeghi M, Talesh Alipour M, Amin MM, Abdolahnejad A. Estimation of spatial distribution of PM10, lead, and radon concentrations in Sepahanshahr, Iran using geographic information system (GIS). J Mazandaran Univ Med Sci. 2018;27(159):84–96.
Abdolahnejad A, Jafari N, Mohammadi A, Miri M, Hajizadeh Y, Nikoonahad A. Cardiovascular, Respiratory, And Total Mortality Ascribed To PM10 And PM2.5 Exposure In Isfahan, Iran. J Educ Health Promot. 2017;6:109.
De Marco A, Amoatey P, Khaniabadi YO, Sicard P, Hopke PK. Mortality and morbidity for cardiopulmonary diseases attributed to PM2.5 exposure in the Metropolis of Rome, Italy. Eur J Intern Med. 2018;57:49–57.
Naddafi K, Hassanvand MS, Yunesian M, Momeniha F, Nabizadeh R, Faridi S, et al. Health impact assessment of air pollution in megacity of Tehran, Iran. Iranian J Environ Health Sci Eng. 2012;9:28.
Duan C, Talbott E, Brooks M, Park SK, Broadwin R, Matthews K, et al. Five-year exposure to PM2.5 and ozone and subclinical atherosclerosis in late midlife women: the study of Women's health across the. Nation. 2019;222:168–76.
Bayat R, Ashrafi K, Shafiepour Motlagh M, Hassanvand MS, Daroudi R, Fink G, et al. Health impact and related cost of ambient air pollution in Tehran. Environ Res. 2019;176:108547.
Krewski D, Jerrett M, Burnett RT, Ma R, Hughes E, Shi Y, et al. Extended follow-up and spatial analysis of the American Cancer Society study linking particulate air pollution and mortality. Boston: Health Effects Institute; 2009.
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, et al. Estimates And 25-Year Trends Of The Global Burden Of Disease Attributable To Ambient Air Pollution: An Analysis Of Data From The Global Burden Of Diseases Study 2015. Lancet. 2017;389:1907–18.
Dastoorpoor M, Riahi A, Yazdaninejhad H, Borsi SH, Khanjani N, Khodadadi N, et al. Exposure to particulate matter and carbon monoxide and cause-specific cardiovascular-respiratory disease mortality in Ahvaz. Toxin Rev. 2020:1–11.
Pascal M, Corso M, Ung A. Guidelines for assessing the health impacts of air pollution in European cities. Work Package: Aphekom Project; 2011.
Karimi A, Shirmardi M, Hadei M, Birgani YT, Neisi A, Takdastan A, et al. Concentrations and health effects of short-and long-term exposure to PM2.5, NO2, and O3 in ambient air of Ahvaz City, Iran (2014–2017). Ecotox Environ Safe. 2019;180:542–8.
WHO. Airq+ Glossary: World Health Organization; 2016a.
Hosseiniebalam F, Ghaffarpasand O. The effects of emission sources and meteorological factors on Sulphur dioxide concentration of great Isfahan, Iran. Atmos Environ. 2015;100:94–101.
Kelishadi R, Moeini R, Poursafa P, Farajian S, Yousefy H, Okhovat-Souraki AA. Independent association between air pollutants and vitamin D deficiency in young children in Isfahan, Iran. Paediatr Int Child H. 2014;34:50–5.
Abdolahnejad A, Jafari N, Mohammadi A, Miri M, Hajizadeh Y. Mortality and morbidity due to exposure to ambient NO2, SO2, and O3 in Isfahan in 2013–2014. Int J Prev Med. 2018;9:11.
Union. Directive 2008/50/Ec of the European Parliament and of the council of 2008 On Ambient Air Quality And Cleaner Air For Europe; 2008.
WHO. Ambient Air Pollution: A Global Assessment Of Exposure And Burden Of Disease; 2016b.
WHO. Evolution Of WHO Air Quality Guidelines: Past, Present And Future. Copenhagen: WHO Regional Offce For Europe; 2017.
Ansari M, Ehrampoush MH. Meteorological correlates and Airq(+) health risk assessment of ambient fine particulate matter in Tehran. Iran. Environ Res. 2019;170:141–50.
Al-Hemoud A, Gasana J, Al-Dabbous A, Alajeel A, Al-Shatti A, Behbehani W, et al. Exposure levels of air pollution (pm2.5) and associated health risk in kuwait. Environ Res. 2019;179:108730.
Guo H, Wang Y, Zhang H. Characterization of criteria air pollutants in Beijing during 2014–2015. Environ Res. 2017;154:334–44.
Fan H, Zhao C, Yang Y. A comprehensive analysis of the Spatio-temporal variation of urban air pollution in China during 2014–2018. Atmos Environ. 2020;220:117066.
Shahsavani A, Naddafi K, Haghighifard NJ, Mesdaghinia A, Yunesian M, Nabizadeh R, et al. The evaluation of PM10, PM2.5, and Pm1 concentrations during the middle eastern dust (med) events in Ahvaz, Iran, from April through Septembe 2010. J. Arid Environ. 2012;77:72–83.
Hu X, Waller L, Lyapustin A, Wang Y, Liu Y. 10-Year Spatial And Temporal Trends Of PM2.5 Concentrations In The Southeastern Us Estimated Using High-Resolution Satellite Data. Atmos Chem Phys. 2014;14:6301.
Jadidi H, Shahsavani A, Mahaki B. Spatial and temporal variations of PM2.5 concentration and air quality in Isfahan City in 2016. J Environ Health Sustainable Dev. 2019;4(1):557–66.
Safavy S, Mousavi M, Dehghanzadeh Reihani R, Shakeri MH. Seasonal and spatial zoning of air quality index and ambient air pollutants by arc-Gis for Tabriz City and assessment of the current executive problem. J Health. 2016;7:158–77.
Soleimani M, Amini N, Sadeghian B, Wang D, Fang L. Heavy metals and their source identification in particulate matter (PM2.5) in Isfahan City, Iran. J Environ Sci. 2018;72:166–75.
Faridi S, Shamsipour M, Krzyzanowski M, Kunzli N, Amini H, Azimi F, et al. Long-term trends and health impact of PM2.5 and O3 in Tehran, Iran, 2006–2015. Environ. Int. 2018;114:37–49.
Jang E, Do W, Park G, Kim M, Yoo E. Spatial and temporal variation of urban air pollutants and their concentrations in relation to meteorological conditions at four sites in Busan. South Korea Atmos Pollut Res. 2017;8:89–100.
Kuerban M, Waili Y, Fan F, Liu Y, Qin W, Dore AJ, et al. Spatio-temporal patterns of air pollution in China from 2015 to 2018 and implications for health risks. Environ Pollut. 2020;258:113659.
Hu XM, Klein PM, Xue M, Zhang F, Doughty DC, Forkel R, et al. Impact of the vertical mixing induced by low-level jets on boundary layer ozone concentration. Atmos Environ. 2013;70:123–30.
Mehmood T, Tianle Z, Ahmad I, Li X. Integration of airq+ and particulate matter mass concentration to calculate health and ecological constraints in islamabad, pakistan. 2019 16th international bhurban conference on applied sciences and technology (ibcast), vol. Ieee; 2019. p. 248–54.
Shah MH, Shaheen N, Nazir R. Assessment of the trace elements level in urban atmospheric particulate matter and source apportionment in Islamabad, Pakistan. Atmos Pollut Res. 2012;3:39–45.
Barzeghar V, Sarbakhsh P, Hassanvand MS, Faridi S, Gholampour A. Long-Term Trend Of Ambient Air Pm10, PM2.5, And O3 And Their Health Effects In Tabriz City, Iran, During 2006–2017. Sustain Cities Soc. 2020;54:101988.
Li R, Cui L, Li J, Zhao A, Fu H, Wu Y, et al. Spatial and temporal variation of particulate matter and gaseous pollutants in China during 2014–2016. Atmo Environ. 2017;161:235–46.
Ye WF, Ma ZY, Ha XZ. Spatial-temporal patterns of PM2.5 concentrations for 338 Chinese cities. Sci Total Environ. 2018;631:524–33.
Yousefian F, Faridi S, Azimi F, Aghaei M, Shamsipour M, Yaghmaeian K, et al. Temporal variations of ambient air pollutants and meteorological influences on their concentrations in Tehran during 2012–2017. Sci Rep. 2020;10(1):1–11.
Kermani M, Arfaeinia H, Masroor K, Abdolahnejad A, Fanaei F, Shahsavani A, et al. Health impacts and burden of disease attributed to long-term exposure to atmospheric PM10/PM2.5 in Karaj, Iran: effect of meteorological factors. Int J Environ Anal Chem. 2020;28:1–7.
Azmi SZ, Latif MT, Ismail AS, Juneng L, Jemain AA. Trend and status of air quality at three different monitoring stations in the Klang Valley, Malaysia. Air Qual Atmos Hlth. 2010;3:53–64.
Masiol M, Agostinelli C, Formenton G, Tarabotti E, Pavoni B. Thirteen years of air pollution hourly monitoring in a large City: potential sources, trends, cycles and effects of car-free days. Sci Total Environ. 2014;494:84–96.
Zhao S, Yu Y, Yin D, He J, Liu N, Qu J, et al. Annual and diurnal variations of gaseous and particulate pollutants in 31 provincial capital cities based on in situ air quality monitoring data from China National Environmental Monitoring Center. Environ Int. 2016;86:92–106.
Mirzaei N, Arfaeinia H, Moradi M, Mohammadi Moghadam F, Velayati A, Sharafi K. The statistical analysis of seasonal and time variations on trend of important air pollutants (SO2, O3, NOx, CO, PM10)-in Western Iran: a case study. Int J Pharm. 2015;7:9610–22.
Silva Júnior RSD, Oliveira M, MDF A. Weekend/weekday differences in concentrations of ozone, Nox, and non-methane hydrocarbon in the metropolitan area of São Paulo. Rev Bras de Meteorol. 2009;24:100–10.
Yarahmadi M, Hadei M, Nazari SSH, Conti GO, Alipour MR, Ferrante M, et al. Mortality assessment attributed to long-term exposure to fine particles in ambient air of the megacity of Tehran, Iran. Environ Sci Pollut Res Int. 2018;25:14254–62.
Manojkumar N, Srimuruganandam B. Health effects of particulate matter in major Indian cities. Int J Environ Health Res. 2021;31(3):258–70.
Wei H, Liang F, Cheng W, Zhou R, Wu X, Feng Y, et al. The mechanisms for lung Cancer risk of PM2.5: induction of epithelial-Mesenchymal transition and Cancer stem cell properties in human non-small cell lung Cancer cells. Environ Toxicol. 2017;32:2341–51.
Boldo E, Medina S, Letertre A, Hurley F, Mucke HG, Ballester F, et al. Apheis: health impact assessment of long-term exposure to pm(2.5) in 23 European cities. Eur J Epidemiol. 2006;21:449–58.
Miri M, Derakhshan Z, Allahabadi A, Ahmadi E, Conti GO, Ferrante M, et al. Mortality and morbidity due to exposure to outdoor air pollution in Mashhad Metropolis, Iran. Airq Model Approach Environ Res. 2016;151:451–7.
Xie W, Li G, Zhao D, Xie X, Wei Z, Wang W, et al. Relationship between fine particulate air pollution and Ischaemic heart disease morbidity and mortality. Cardiac Risk Factors Prev. 2015;101:257–63.
Hadei M, Hopke PK, Nazari SSH, Yarahmadi M, Shahsavani A, Alipour MR. Estimation of mortality and hospital admissions attributed to criteria air pollutants in Tehran Metropolis, Iran (2013–2016). Aerosol Air Qual Res. 2017a;17:2474–81.
Hwang SL, Lin YC, Hsiao KY, Lin CM, Chi MC. Spatiotemporal assessment of mortality attributable to ambient PM2.5 exposure in Taiwan during 2008–2015. Air Qual Atmos Hlth. 2020;13:233–45.
Hadei M, Nazari SSH, Eslami A, Khosravi A, Yarahmadi M, Naghdali Z, et al. Distribution and number of ischemic heart disease (Ihd) and stroke deaths due to chronic exposure to PM2.5 in 10 cities of Iran (2013-2015); an Airq+ Modelling. J Air Pollut Health. 2017b;2:129–36.
Cai Y, Hodgson S, Blangiardo M, Gulliver J, Morley D, Fecht D, et al. L. Road traffic noise, air pollution and incident cardiovascular disease: a joint analysis of the hunt, epic-Oxford and Uk biobank cohorts. Environ Int. 2018;114:191–201.
Gandini M, Scarinzi C, Bande S, Berti G, Carna P, Ciancarella L, et al. Long term effect of air pollution on incident hospital admissions: results from the Italian longitudinal study within life med hiss project. Environ Int. 2018;121:1087–97.
Yuan S, Wang J, Jiang Q, He Z, Huang Y, Li Z, et al. Long-term exposure to PM2.5 and stroke: a systematic review and meta-analysis of cohort studies. Environ Res. 2019;177:108587.
Acknowledgements
This paper was inspired by the results of a research project no.198202 approved by Isfahan University of Medical Sciences, Iran. The authors would like to thank the Isfahan Department of Environment and Isfahan Air Quality Monitoring Center for providing the required data of studied pollutants.
Funding
Financial support of this research project (no.198202) was by Isfahan University of Medical Sciences, Iran.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical considerations
The authors declare that this manuscript is original, has not been published before, and is not currently being considered for publication elsewhere.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hajizadeh, Y., Jafari, N., Fanaei, F. et al. Spatial patterns and temporal variations of traffic-related air pollutants and estimating its health effects in Isfahan city, Iran. J Environ Health Sci Engineer 19, 781–791 (2021). https://doi.org/10.1007/s40201-021-00645-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40201-021-00645-6