
Abstract
Few studies regarding the health effects of long-term exposure to particulate matter with an aerodynamic diameter of 2.5 μm or less (PM2.5) have been carried out in Asia or the Middle East. The objective of our study was to assess total, lung cancer and chronic obstructive pulmonary disease (COPD) mortality attributed to long-term exposure to PM2.5 among adults aged over 30 years in Tehran from March 2013 to March 2016 using AirQ+ software. AirQ+ modeling software was used to estimate the number of deaths attributed to PM2.5 concentrations higher than 10 μg m−3. Air quality data were obtained from the Department of Environment (DOE) and Tehran Air Quality Control Company (TAQCC). Only valid stations with data completeness of 75% in all 3 years were selected for entry into the model. The 3-year average of the 24-h concentrations was 39.17 μg m−3. The results showed that the annual average concentration of PM2.5 in 2015–2016 was reduced by 13% compared to that in 2013–2014. The annual average number of all natural, COPD, and lung cancer deaths attributable to long-term exposure to PM2.5 in adults aged more than 30 years was 5073, 158, and 142 cases, respectively. The results of all three health endpoints indicate that the mortality attributable to PM2.5 decreased yearly from 2013 to 2016 and that the reduced mortality was related to a corresponding reduction in the PM2.5 concentration. Considering these first positive results, the steps that have been currently taken for reducing air pollution in Tehran should be continued to further improve the already positive effects of these measures on reducing health outcomes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Air pollution is described as the most important environmental health risk worldwide (Krzyzanowski et al. 2014). Adverse effects of air pollution on health in terms of premature deaths and disability-adjusted life years (DALYs) can reduce economic development and quality of life as well as eventually cause a reduction in income and productivity (World Bank 2016). In fact, according to the World Bank, exposure to air pollution is the fourth leading cause of death in the world after metabolic risks, dietary risks, and tobacco smoke (World Bank 2016). It is well recognized that short- and long-term exposure to ambient particulate matter with an aerodynamic diameter of 2.5 μm or less (PM2.5) is associated with increased mortality and morbidity due to various adverse health effects (Dianat et al. 2016, Halonen et al. 2016, Khamutian et al. 2015, Mohseni Bandpi et al. 2016, Soleimani et al. 2016, Zanobetti et al. 2014).
PM2.5 is more harmful to health than particulate matter with an aerodynamic diameter of 10 μm or less (PM10) because PM2.5 can be inhaled more deeply into the lungs due to its small size with respect to PM10 and because it has a greater surface area; hence, PM2.5 could provide potentially larger concentrations of adsorbed or condensed air toxicants per unit mass (Tsai et al. 2014). The number of deaths attributable to air pollution worldwide is estimated by the World Bank to be 5,500,000 deaths annually (World Bank 2016), and a World Health Organization (WHO) report showed that more than 7,000,000 premature deaths occur per year due to air pollution, 3,000,000 of which are due to outdoor air quality (WHO 2014c). Air pollution-related diseases include lung cancer, heart disease, stroke, acute respiratory infections (Carey et al. 2013, Mohseni Bandpi et al. 2017) and chronic obstructive pulmonary diseases (COPD) (World Bank 2016). It is estimated that more than 87% of the world’s population is living in areas in which the PM2.5 concentration is higher than the World Health Organization’s guidelines (Brauer et al. 2016).
A health impact assessment of air pollution can be an effective tool for policy-makers and authorities to assess the effects of their actions (Likhvar et al. 2015). Additionally, the World Bank has reported that the total welfare losses and contribution of attributable deaths to air pollution to gross domestic product (GDP) were estimated to be 31 billion USD and 2.48% in 2013, respectively. Furthermore, the total labor output loss and its contribution to Iran’s GDP were 1471 billion USD and 0.12%, respectively (World Bank 2016). As a result, it is critical to quantify the health impacts of air pollution and to observe the trends over the time.
Tehran is the capital city and economic center of Iran and has more than 8,000,000 residents. In 2014, the PM10 and PM2.5 annual average concentrations in Tehran were 77 and 32 μg m−3, respectively, which are higher than the WHO guidelines for PM10 (20 μg m−3) and PM2.5 (10 μg m−3) (WHO 2014a). Several studies have been conducted to estimate the health impacts of air pollution in Iran (Hadei et al. 2017a, b, Hopke et al. 2018, Maleki et al. 2016, Mohammadi et al. 2016, Oliveri Conti et al. 2017), but there are no studies that quantify the health impact of long-term exposure to atmospheric PM2.5 and COPD mortality. In addition, the use of AirQ+ software in this field has not been documented. This software was released by the WHO in 2016 and is based on new epidemiological findings. The procedure used in this study to validate monitoring stations was performed according to the European Commission guideline, which has some innovative criteria (EC Directive 2008). Despite previous studies, the baseline incidence of mortality used in this study is based on trustworthy information acquired from Ministry of Health and Medical Education (Khosravi et al. 2016).
The objective of this study was to estimate total, lung cancer and COPD mortality attributed to long-term exposure to ambient PM2.5 among adults aged over 30 years in the megacity of Tehran from March 2013 to March 2016 using WHO AirQ+ software.
Materials and methods
Data collection
According to the Persian calendar, three 1-year periods were considered in this study. The first period was from 21 March 2013 to 20 March 2014. The second period was from 21 March 2014 to 20 March 2015. The third period was between 21 March 2015 and 19 March 2016.
The hourly concentrations of ambient PM2.5 measured by 15 fixed monitoring stations associated with the Department of Environment (DOE) and 22 fixed monitoring stations of the Tehran Air Quality Control Company (TAQCC) from 21 March 2013 to 19 March 2016 were used in this study (Fig. 1).

Air quality monitoring stations in Tehran (red and yellow signs represent invalid and valid monitoring stations, respectively)
Demographic information, including the yearly population and different age groups of Tehran, was obtained from the Statistical Center of Iran. The number of deaths classified by age groups was obtained from the center of Health Networks associated with the Public Health Deputy, Ministry of Health and Medical Education (Khosravi et al. 2016).
AirQ+ estimates the health impacts attributed to air pollution in predefined age groups. This is due to the fact that prior works (Burnett et al. 2014, Hoek et al. 2013, WHO-Europe 2013) has suggested that depending on health outcome, the risk estimates for people older than a certain age are more robust than those including younger individuals. Based on this information, the baseline incidence rate of natural mortality in adults aged over 30 years in Tehran was calculated to be 943 deaths per 100,000 people. In addition, the baseline incidences of lung cancer and COPD mortality have been reported to be 15.50 and 21.73 deaths per 100,000 people. The Ministry of Health and Medical Education statistics were from 2012. Due to the lack of any recent formal and approved reports, the same value was used for the whole study period.
Data validation
The initial determination of the hourly PM2.5 concentrations involved the deletion of negative and false zero values. At first, the 24-h averages were calculated for days that had more than 75% of hourly data. Then, an annual average for each station was calculated only for the stations that had more than 90% of valid hourly values or (if not available) 24-h values over 1 year (EC Directive 2008). Stations that could not meet this criterion were excluded from the study. Then, only valid stations for all 3 years were selected to enter the model, and the others were excluded. This was done to develop a constant assumption for population exposure to PM2.5. Additionally, the spatial distribution of the selected stations was determined. Out of the 37 fixed monitoring stations over these 3 years, 7 stations (19% of the total) were valid to enter the model, and these stations are illustrated in Fig. 1. The overall 24-h averages of the city were calculated from the 24-h averages of all of the selected stations on each day.
AirQ+
The World Health Organization, Regional Office for Europe, developed AirQ+ 1.0 to estimate the magnitude of the short- and long-term health impacts of air pollution in a specific population. AirQ+ calculates the attributable proportion of cases, number of attributable cases, number of attributable cases per 100,000 people of the at-risk population, and proportion of cases per category of the air pollutant concentration. Epidemiological studies are the source of the methodology and concentration-response functions used in AirQ+ (WHO Regional Office for Europe 2016).
To quantify the long-term effects of PM2.5, the following data should be provided as the input: 24-h averages of PM2.5 concentrations; at-risk population; health data, such as the baseline rates of health outcomes; a cutoff value for consideration; and relative risk (RRs) values (Pierpaolo Mudu and Dunbar 2016).
The attributable proportion (AP) is the attributed fraction of the health outcome due to the exposure in a given population for a certain period of time, and it can be calculated using Eq. 1:
where
RR(c) is the relative risk for the health outcome in the category of exposure (c), and p(c) is the proportion of the population in the category of exposure (c).
With a certain baseline incidence (B) of the selected health endpoint in the population, the rate or the number of cases per unit population (BE) can be calculated as:
For a population of a given size N, the number of attributable cases (NE) can be estimated (Krzyzanowski 1997):
The daily average concentrations of the 3-year period, demographic data, and baseline incidence rate were prepared for entry into the model. AirQ+ software provides default RR values. To avoid overestimation, the linear-log method was selected over log-linear calculations. These two methods are two types of modeling approaches to deal with different types of dose-response curves and estimating relative risks for different concentrations.
Statistics
All of the calculations were performed using SPSS 14. One-way ANOVA was used to analyze whether the reduction of the Annual PM2.5 concentration over the whole period was significant.
Results and discussion
We used AirQ+ to estimate the total mortality attributed to long-term exposure to PM2.5 in ambient air in the megacity of Tehran from March 2013 until March 2016. In addition, the number of lung cancer and COPD deaths attributable to long-term exposure to PM2.5 was estimated.
PM2.5 concentration
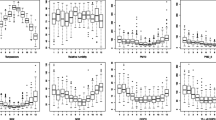
Descriptive statistics of ambient fine particulate matter, including the median, quartiles, minimum, maximum, and outlier values, in Tehran from 2013 to 2016 are reported in Fig. 2. These values are published elsewhere (Hadei et al. 2017b). The annual averages were 41.90, 31.17, and 36.43 μg m−3, respectively. The 3-year average of the 24-h averages was 39.17 μg m−3.

Descriptive statistics of the PM2.5 concentrations of ambient air, Tehran (March 2013–March 2016), including the median, quartiles, minimum and maximum (whiskers), outliers (circles), and extreme values (asterisks)
The results of one-way ANOVA showed that the reduction in PM2.5 concentrations over the 2013–2016 period was statistically significant (p value < 0.05). This is an important finding because, in recent years, many efforts have been made to reduce the concentration of particulate matter in Tehran. These efforts have included fuel substitution in mobile sources and the industrial sector as well as replacing older vehicles with new ones, among others, and these efforts may be the reason for this reduction (Department of Environment (DOE) 2017). However, the average annual concentration was still far from the guidelines set by the WHO. The annual concentrations of PM2.5 in March 2013–March 2014, March 2014–March 2015, and March 2015–March 2016 were, respectively, 4.2, 3.9, and 3.6 times higher than the guideline value of 10 μg m−3, which is the annual average recommended by the WHO (WHO 2006). The annual average PM2.5 concentration in 2015–2016 was reduced by 13% compared to that in 2013–2014 (from 41.90 to 36.43 μg m−3). According to the latest WHO report, the annual average PM2.5 concentration in Tehran (2014) was 32.00 μg m−3 (WHO 2014a). This difference might be due to the different criteria used to quantify valid stations to calculate the average concentration.
The reason for the high PM2.5 concentrations in Tehran can be found in a report published by TAQCC (Shahbazi et al. 2015). The authors, in fact, declare that there are more than 3,000,000 personal cars in Tehran, 25% of which are older than 10 years and 75% of which have emissions that meet the Euro-2 standard and less. In addition, there are approximately 750,000 motorcycles, 40% of which are older than 10 years, and more than 95% of their emissions meet the Euro-2 standard and less. The Tehran Air Quality Control Company’s calculations show that each year more than 8600 tons of particulate matter from vehicles is released in Tehran. In total, the major sources of particulate matter in Tehran include: mobile sources (70.2%), the energy conversion sector (19.6%), industries (7.1%), households and commercial emissions (2.1%), and public terminals (0.9%) (Asl et al. 2015, Shahbazi et al. 2015). It is necessary to conduct studies to more precisely apportion the sources of particulate matter in Tehran, as it is carried out in Ahvaz, which has an average PM10 concentration of 319.60 μg m−3 and is one of the most polluted cities in Iran and the world, due to the Middle Eastern dust storms and improper management of water resources (Ashrafi et al. 2018, Moghaddam et al. 2017, Shahsavani et al. 2017, Sowlat et al. 2013).
Figure 3 illustrates the number of days during which people were exposed to daily PM2.5 concentrations from March 2013 to March 2016. The number of days with a lower concentration than the WHO’s 24-h guideline value of 25 μg m−3 increased by 57% in the period from March 2015–March 2016 in comparison to the period from March 2013–March 2014 (from 40 to 94 days in a year). The number of days with concentrations of less than 30 μg m−3 has increased from the first period to the third period. This may be due to the decrease in the number of days with concentrations higher than 30 μg m−3, and also the decrease in the number of days with dust storms (average PM2.5 concentrations higher than 35 μg m−3) in the third year (Arhami et al. 2017, Shahbazi et al. 2015). This improve in air quality might be due to several actions performed during the past few years, such as improving the quality of fuel, upgrading the standards of vehicles, phasing-out of old cars and increasing the size of the public transport fleet (Shahbazi et al. 2015, Sharafi et al. 2015).

The number of days with concentrations in each PM2.5 concentration interval
Total mortality estimation
Table 1 shows the long-term health impacts of exposure to PM2.5 concentrations above 10 μg m−3 including the attributable proportion (AP) and attributable cases of natural mortality in adults aged more than 30 years from March 2013 to March 2016. In total, 15,219 deaths can be attributed to long-term exposure to fine particulate matter from 2013 to 2016. On average, the number of deaths was 5073 cases over the 3 years.
In 2015–2016, natural mortality was reduced by 2.4 and 8.4% compared to 2014–2015 and 2013–2014, respectively. Despite the increase in population from 2013 to 2016, the attributable proportion and cases of deaths were decreased due to the reduction of the PM2.5 concentration. As mentioned before, the baseline incidence rate was kept constant during the 3 years. The results showed that 58 deaths per 100,000 people in the whole population were attributable to long-term exposure to PM2.5 in Tehran during 2013–2016, while the world average number of deaths was 53 per 100,000 people (WHO 2014b).
The results of Fisher’s study indicated that long-term exposure to PM10 was directly related to mortality in adults older than 30 years old. They reported that for each 10 μg m−3 increase in PM10, the associated hazard ratio was 1.08 (95% CI 1.07–1.09) (Fischer et al. 2015). Carugno’s investigation on air pollution exposure and cause-specific deaths confirmed the strong relationship between the concentration of PM10 and natural mortality (Carugno et al. 2016). There is no study on the long-term effects of PM2.5 on mortality in Tehran. However, quantification of the short-term effects of other air pollutants has been performed in some studies. Naddafi et al. (2012) estimated all natural deaths due to short-term exposure to PM10 in the whole population of Tehran. The results showed that there were annually 2194 attributable deaths to PM10 exposure (Naddafi et al. 2012). This value is less than the number of attributable deaths estimated in this study. This difference is because despite Naddafi et al., we considered long-term health impacts, not short-term impacts.
COPD mortality estimation
Another objective of the study was to estimate the attributable proportion (AP) and cases of mortality of COPD caused by long-term exposure to a concentration of PM2.5 above the reference concentration of 10 μg m−3 in adults aged over 30 years between 2013 and 2016. Table 2 shows that 474 people died due to COPD due to long-term exposure to fine particulate matter in Tehran from 2013 to 2016. The annual average of attributable COPD deaths was 158 cases. Our findings demonstrated that the number of deaths attributable to COPD was also reduced by 9% over the research period. This decrease was attributable to the reduction in the fine particulate matter concentration over the last 3 years. As mentioned before, the baseline incidence rate was kept constant during the 3 years.
The results of the Neuberger et al. (2013) study also indicated that short-term exposure to a 10 μg m−3 increase in PM2.5 caused a 14% (95% CI 4.9–24) increase in mortality, and this increase in mortality was marked by a 0- to 7-day lag from exposure to death (Neuberger et al. 2013). According to the WHO in 2014, each year, approximately 389,000 people in the world died due to COPD caused by exposure to ambient air pollution. The result of this report showed that COPD, after ischemic heart disease (IHD) and stroke, was the third leading cause of death from exposure to ambient air pollution (WHO 2014b). According to the report of the global burden of disease in 2013, COPD was the ninth cause of years of life lost in Iran (Global Burden of Disease (GBD) 2015). There is no health impact assessment study on estimating COPD mortality attributed to air pollution in Iran. However, the number of COPD hospital admissions due to gaseous pollutants has been well documented (Naddafi et al. 2012).
Lung cancer mortality estimation
Table 3 shows the attributable cases of lung cancer mortality due to long-term exposure to PM2.5 in adults aged over 30 years in Tehran from 2013 to 2016. The results provided in Table 3 show that 427 cases of lung cancer deaths were attributable to long-term exposure to fine particulate matter in Tehran during the whole period. On average, the annual number of lung cancer deaths was 142. Our study demonstrated that the number of lung cancer deaths was reduced by approximately 9% in 2016 compared to 2013. As mentioned before, the baseline incidence rate was kept constant during the 3 years.
The WHO reported that, each year, approximately 227,000 people in the world died due to lung cancer caused by exposure to ambient air pollution. Furthermore, the report indicated that lung cancer is the fourth leading cause of death because of exposure to ambient air pollution (WHO 2014c). In addition, the WHO has reported the number of deaths, years of life lost (YLL) and disability-adjusted life years (DALY) due to lung cancer caused by air pollution in each country. The number of deaths, YLLs, and DALYs of lung cancer caused by particulate air pollution in Iran during 2012 were 1460, 37,894, and 38,258, respectively (WHO 2016). It can be concluded that our results are consistent with the WHO’s report because Tehran’s population is approximately one tenth of the total country, as well as one tenth of the estimated number of lung cancer deaths. In an industrial area in Italy, approximately 433 and 1204 YLLs were attributed to a PM2.5 concentration higher than 10 μg m−3 during the first year and next 10 years, respectively. The yearly average concentration of PM2.5 in that region was 42 μg m−3 (Fattore et al. 2011).
Tomczak et al.’s (2016) study on long-term exposure to fine particulate matter air pollution and the risk of lung cancer among participants of the Canadian National Breast Screening Study showed that a 10 μg m−3 increase in PM2.5 was associated with an elevated lung cancer risk (HRs 1.34; 95% CI = 1.10, 1.65) (Tomczak et al. 2016). The finding of Villeneuve et al. (2015) from a cohort study showed that a 10 μg m−3 increase in PM2.5 exposure was associated with elevated risks of lung cancer (HRs 1.12; 95% CI = 0.94, 1.34) (Villeneuve et al. 2015). In another cohort study by Cesaroni et al. (2013), it was found that long-term exposure to PM2.5 was associated with increased mortality due to lung cancer in this large population-based cohort (Cesaroni et al. 2013).
Conclusion
AirQ+ modeling software was used to estimate the number of total, lung cancer and COPD mortality cases attributed to long-term exposure to ambient PM2.5 among adults aged over 30 years in the megacity of Tehran from March 2013 until March 2016. The results showed that the annual averages of PM2.5 from March 2013–March 2014, March 2014–March 2015, and March 2015–March 2016 years were higher than the guideline value recommended by the WHO. However, the annual concentration from March 2015–March 2016 decreased compared to that from March 2013–March 2014. The 3-year averages of all natural, COPD, and lung cancer deaths attributable to long-term exposure to ambient PM2.5 were 5073, 158, and 142 deaths, respectively. The mortality attributable to PM2.5 decreased from 2013 to 2016, which is a consequence of the reduction in the PM2.5 concentration. This might be due to several factors, such as improving the quality of fuel, upgrading of standards of vehicles, phasing-out of old cars and an increasing the size of the public transport fleet. Considering these results, the trend of reducing particulate air pollution in Tehran should be continued to reduce its health impacts.
References
Arhami M, Hosseini V, Shahne MZ, Bigdeli M, Lai A, Schauer JJ (2017) Seasonal trends, chemical speciation and source apportionment of fine PM in Tehran. Atmos Environ 153:70–82
Ashrafi K, Fallah R, Hadei M, Yarahmadi M, Shahsavani A (2018) Source apportionment of total suspended particles (TSP) by positive matrix factorization (PMF) and chemical mass balance (CMB) modeling in Ahvaz. Iran, Arch Environ Contam Toxicol
Asl FB, Kermani M, Aghaei M, Karimzadeh S, Arian SS, Shahsavani A, Goudarzi G (2015): Estimation of diseases and mortality attributed to NO2 pollutant in five metropolises of Iran using AirQ model in 2011-2012. J Mazandaran Univ Med Sci 25, 239–249
Brauer M, Freedman G, Frostad J, van Donkelaar A, Martin RV, Dentener F, Dingenen R, Estep K, Amini H, Apte JS, Balakrishnan K, Barregard L, Broday D, Feigin V, Ghosh S, Hopke PK, Knibbs LD, Kokubo Y, Liu Y, Ma S, Morawska L, Sangrador JLT, Shaddick G, Anderson HR, Vos T, Forouzanfar MH, Burnett RT, Cohen A (2016) Ambient air pollution exposure estimation for the global burden of disease 2013. Environ Sci Technol 50:79–88
Burnett RT, Pope CA 3rd, Ezzati M, Olives C, Lim SS, Mehta S, Shin HH, Singh G, Hubbell B, Brauer M, Anderson HR, Smith KR, Balmes JR, Bruce NG, Kan H, Laden F, Prüss-Ustün A, Turner MC, Gapstur SM, Diver WR, Cohen A (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect 122:397–403
Carey IM, Atkinson RW, Kent AJ, van Staa T, Cook DG, Anderson HR (2013) Mortality associations with long-term exposure to outdoor air pollution in a national English cohort. Am J Respir Crit Care Med 187:1226–1233
Carugno M, Consonni D, Randi G, Catelan D, Grisotto L, Bertazzi PA, Biggeri A, Baccini M (2016) Air pollution exposure, cause-specific deaths and hospitalizations in a highly polluted Italian region. Environ Res 147:415–424
Cesaroni G, Badaloni C, Gariazzo C, Stafoggia M, Sozzi R, Davoli M, Forastiere F (2013) Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ Health Perspect 121:324–331
Department of Environment (DOE) (2017) Actions and programs of the National Center for Air and Climate Change [in Persian], Deopartment of Environment (DOE)
Dianat M, Radmanesh E, Badavi M, Mard SA, Goudarzi G (2016) Disturbance effects of PM(1)(0) on iNOS and eNOS mRNA expression levels and antioxidant activity induced by ischemia-reperfusion injury in isolated rat heart: protective role of vanillic acid. Environ Sci Pollut Res Int 23:5154–5165
EC Directive (2008) Council directive 2008/50/EC on ambient air quality and cleaner air for Europe. Off J Eur Communities, L 151:1–44
Fattore E, Paiano V, Borgini A, Tittarelli A, Bertoldi M, Crosignani P, Fanelli R (2011) Human health risk in relation to air quality in two municipalities in an industrialized area of northern Italy. Environ Res 111:1321–1327
Fischer PH, Marra M, Ameling CB, Hoek G, Beelen R, de Hoogh K, Breugelmans O, Kruize H, Janssen NA, Houthuijs D (2015) Air pollution and mortality in seven million adults: the Dutch Environmental Longitudinal Study (DUELS). Environ Health Perspect 123:697–704
Global Burden of Disease (GBD) (2015) Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385:117–171
Hadei M, Hashemi Nazari SS, Yarahmadi M, Kermani M, Farhadi M, Shahsavani A (2017a): Estimation of Gender-Specific Lung Cancer Deaths due to Exposure to PM2.5 in 10 Cities of Iran During 2013–2016: A Modeling Approach. Int J Cancer Manag In Press, e10235
Hadei M, Hopke PK, Hashemi Nazari SS, Yarahmadi M, Shahsavani A, Alipour MR (2017b) Estimation of mortality and hospital admissions attributed to criteria air pollutants in Tehran metropolis, Iran (2013-2016). Aerosol Air Qual Res 17:2474–2481
Halonen JI, Blangiardo M, Toledano MB, Fecht D, Gulliver J, Ghosh R, Anderson HR, Beevers SD, Dajnak D, Kelly FJ, Wilkinson P, Tonne C (2016) Is long-term exposure to traffic pollution associated with mortality? A small-area study in London. Environ Pollut 208:25–32
Hoek G, Krishnan RM, Beelen R, Peters A, Ostro B, Brunekreef B, Kaufman JD (2013) Long-term air pollution exposure and cardio-respiratory mortality: a review. Environ Health 12:1
Hopke PK, Hashemi Nazari SS, Hadei M, Yarahmadi M, Kermani M, Yarahmadi E, Shahsavani A (2018) Spatial and temporal trends of short-term health impacts of PM2.5 in Iranian cities: a modelling approach (2013-2016). Aerosol Air Qual Res 18:497–504
Khamutian R, Najafi F, Soltanian M, Shokoohizadeh MJ, Poorhaghighat S, Dargahi A, Sharafi K, Afshari A (2015) The association between air pollution and weather conditions with increase in the number of admissions of asthmatic patients in emergency wards: a case study in Kermanshah. Med J Islam Repub Iran 29:229
Khosravi AA, Saeedeh; Kazemi, Elaheh; Kalantari, Naser; (2016): The outlook of mortality in 30 provinces of Iran during 2011–2012, Ministry of Health and Medical Education, Tehran, Iran
Krzyzanowski M (1997) Methods for assessing the extent of exposure and effects of air pollution. Occup Environ Med 54:145–151
Krzyzanowski M, Apte JS, Bonjour SP, Brauer M, Cohen AJ, Prüss-Ustun AM (2014) Air pollution in the mega-cities. Curr Environ Health Rep 1:185–191
Likhvar VN, Pascal M, Markakis K, Colette A, Hauglustaine D, Valari M, Klimont Z, Medina S, Kinney P (2015) A multi-scale health impact assessment of air pollution over the 21st century. Sci Total Environ 514:439–449
Maleki H, Sorooshian A, Goudarzi G, Nikfal A, Baneshi MM (2016) Temporal profile of PM10 and associated health effects in one of the most polluted cities of the world (Ahvaz, Iran) between 2009 and 2014. Aeolian Res 22:135–140
Moghaddam VK, Changani F, Mohammadi A, Hadei M, Ashabi R, Majd LE, Mahvi AH (2017) Sustainable development of water resources based on wastewater reuse and upgrading of treatment plants: a review in the Middle East. Desalin Water Treat 65:463–473
Mohammadi A, Azhdarpoor A, Shahsavani A, Tabatabaee H (2016) Investigating the health effects of exposure to criteria pollutants using airq2.2.3 in Shiraz, Iran. Aerosol Air Qual Res 16:1035–1043
Mohseni Bandpi A, Eslami A, Shahsavani A, Khodagholi F, Aliaghaei A, Alinejad A (2016) Water-soluble and organic extracts of ambient PM2.5 in Tehran air: assessment of genotoxic effects on human lung epithelial cells (A549) by the comet assay. Toxin Rev:1–9
Mohseni Bandpi A, Eslami A, Shahsavani A, Khodagholi F, Alinejad A (2017) Physicochemical characterization of ambient PM2.5 in Tehran air and its potential cytotoxicity in human lung epithelial cells (A549). Sci Total Environ 593–594:182–190
Naddafi K, Hassanvand MS, Yunesian M, Momeniha F, Nabizadeh R, Faridi S, Gholampour A (2012) Health impact assessment of air pollution in megacity of Tehran, Iran. Iran J Environ Health Sci Eng 9:28
Neuberger M, Moshammer H, Rabczenko D (2013) Acute and subacute effects of urban air pollution on cardiopulmonary emergencies and mortality: time series studies in Austrian cities. Int J Environ Res Public Health 10:4728–4751
Oliveri Conti G, Heibati B, Kloog I, Fiore M, Ferrante M (2017) A review of AirQ models and their applications for forecasting the air pollution health outcomes. Environ. Sci. Pollut. Res, Int
Pierpaolo Mudu CG, Dunbar M (2016) airQ+ 1.0 example of calculations, World Health Organization
Shahbazi HB, Mahdi, Afshin H, Hosseini V (2015) Tehran’s air pollution emission inventory for the year 2013- Volume II: mobile sources [In Persian]. QM/94/04/03/(U)/02. Tehran Air Quality Control Company, Tehran
Shahsavani A, Yarahmadi M, Hadei M, Sowlat MH, Naddafi K (2017) Elemental and carbonaceous characterization of TSP and PM10 during middle eastern dust (MED) storms in Ahvaz, southwestern Iran. Environ Monit Assess 189:462
Sharafi K, Khosravi T, Moradi M, Pirsaheb M (2015): Air quality and variations in PM10 pollutant concentration in western Iran during a four-year period (2008–2011), Kermanshah–a case study. J Eng Sci Technol 10, 47–56
Soleimani Z, Goudarzi G, Sorooshian A, Marzouni MB, Maleki H (2016) Impact of middle eastern dust storms on indoor and outdoor composition of bioaerosol. Atmos Environ 138:135–143
Sowlat MH, Naddafi K, Yunesian M, Jackson PL, Lotfi S, Shahsavani A (2013) PM10 source apportionment in Ahvaz, Iran, using positive matrix factorization. Clean–Soil, Air, Water 41:1143–1151
Tomczak A, Miller AB, Weichenthal SA, To T, Wall C, van Donkelaar A, Martin RV, Crouse DL, Villeneuve PJ (2016) Long-term exposure to fine particulate matter air pollution and the risk of lung cancer among participants of the Canadian National Breast Screening Study. Int J Cancer 139:1958–1966
Tsai SS, Chang CC, Liou SH, Yang CY (2014) The effects of fine particulate air pollution on daily mortality: a case-crossover study in a subtropical city, Taipei, Taiwan. Int J Environ Res Public Health 11:5081–5093
Villeneuve PJ, Weichenthal SA, Crouse D, Miller AB, To T, Martin RV, Van Donkelaar A, Wall C, Burnett RT (2015) Long-term exposure to fine particulate matter air pollution and mortality among Canadian women. Epidemiology 26:536–545
WHO-Europe (2013) Health risks of air pollution in Europe—HRAPIE project recommendations for concentration–response functions for cost–benefit analysis of particulate matter, ozone and nitrogen dioxide. World Health Organization regional Office for Europe. Geneva, Switzerland: World Health Organization
WHO (2006) Air quality guidelines: global update 2005: particulate matter, ozone, nitrogen dioxide, and sulfur dioxide. World Health Organization
WHO (2014a) Ambient (outdoor) air pollution in cities database. World Health Organization, Geneva
WHO (2014b) Burden of disease from household air pollution for 2012. World Health Organization
WHO (2014c) 7 million premature deaths annually linked to air pollution
WHO (2016) Ambient air pollution: a global assessment of exposure and burden of disease. Switzerland, Geneva
WHO Regional Office for Europe (2016) AirQ+: key features. In: WHO regional Office for Europe
World Bank (2016) The cost of air pollution: strengthening the economic case for action. World Bank Group, Washington, D.C.
Zanobetti A, Dominici F, Wang Y, Schwartz JD (2014) A national case-crossover analysis of the short-term effect of PM2.5 on hospitalizations and mortality in subjects with diabetes and neurological disorders. Environ Health 13:38
Acknowledgements
The authors wish to thank the Shahid Beheshti University of Medical Sciences (grant number #13846)). We thank the Environmental and Occupational Health Center of Ministry of Health and Medical Education and Environmental and Occupational Hazards Control Research Center for providing data.
Funding
This study was funded by the Shahid Beheshti University of Medical Sciences (grant number #13846) and by the Environmental and Occupational Health Center of the Ministry of Health and Medical Education.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Rights and permissions
About this article

Cite this article
Yarahmadi, M., Hadei, M., Nazari, S.S.H. et al. Mortality assessment attributed to long-term exposure to fine particles in ambient air of the megacity of Tehran, Iran. Environ Sci Pollut Res 25, 14254–14262 (2018). https://doi.org/10.1007/s11356-018-1680-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-018-1680-4