
Abstract
Purpose of Review
To discuss emerging understandings of adolescent long COVID or post-COVID-19 conditions, including proposed clinical definitions, common symptoms, epidemiology, overlaps with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and orthostatic intolerance, and preliminary guidance on management.
Recent Findings
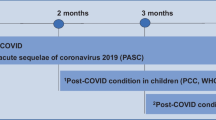
The recent World Health Organization clinical case definition of post-COVID-19 condition requires a history of probable or confirmed SARS-CoV-2 infection, with symptoms starting within 3 months of the onset of COVID-19. Symptoms must last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms of the post-COVID-19 condition include, but are not limited to, fatigue, shortness of breath, and cognitive dysfunction. These symptoms generally have an impact on everyday functioning. The incidence of prolonged symptoms following SARS-CoV-2 infection has proven challenging to define, but it is now clear that those with relatively mild initial infections, without severe initial respiratory disease or end-organ injury, can still develop chronic impairments, with symptoms that overlap with conditions like ME/CFS (profound fatigue, unrefreshing sleep, post-exertional malaise, cognitive dysfunction, and orthostatic intolerance).
Summary
We do not yet have a clear understanding of the mechanisms by which individuals develop post-COVID-19 conditions. There may be several distinct types of long COVID that require different treatments. At this point, there is no single pharmacologic agent to effectively treat all symptoms. Because some presentations of post-COVID-19 conditions mimic disorders such as ME/CFS, treatment guidelines for this and related conditions can be helpful for managing post-COVID-19 symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As of January 2022, there had been over 300 million confirmed cases of SARS-CoV-2 globally and over 5.4 million deaths [1]. While the vast majority of surviving patients return to their baseline health [2••], it has been evident from early in the pandemic that a proportion of patients experience chronic health impairments. Some of these conditions are sequelae of more severe acute COVID-19 such as acute respiratory distress syndrome, post-ICU syndrome, myocarditis, thrombosis, renal injury, stroke, and multisystem inflammatory syndrome in children (MIS-C). Sequelae of MIS-C and the more organ-specific complications have been discussed elsewhere [3,4,5, 6•]. The focus of this review is on adolescents who have developed long-term symptoms, including those with mild respiratory or systemic illnesses in the acute phase. These individuals have been described as having post-COVID-19 conditions, also referred to as long COVID [7•]. In this paper, we review proposed definitions of post-COVID-19 chronic conditions, discuss the epidemiology of pediatric long COVID, and the overlaps with orthostatic intolerance and other post-infectious illnesses like myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Based largely on our experience treating these overlapping conditions, we offer preliminary recommendations on management.
Search Strategy
In addition to papers and materials known to the authors, we conducted a search of PubMed, Embase, Scopus, World Health Organization (WHO) COVID database (which contains preprints from bioRxiv and medRxiv), and I Love Evidence. The search was conducted in mid-November 2021 and used multiple methods of identifying pediatric and adolescent articles, along with various synonyms for long COVID or post-COVID conditions (described in detail in Supplemental File 1).
Definitions
Definitions for post-COVID conditions and other disorders discussed in this review can be found in Table 1. We will use the terms post-COVID-19 condition, post-COVID conditions, and long COVID interchangeably throughout.
Long COVID Symptoms
Long COVID is a spectrum of disease, likely with multifactorial etiologies. Children and adolescents with long COVID are presenting with a variety of complaints, although some patterns are beginning to emerge. Long COVID symptoms can occur in hospitalized [8, 9] or non-hospitalized children [10, 11•, 12]. As in adults, many pediatric patients present with symptoms of long COVID after experiencing only mild or asymptomatic acute infections [11•, 12].
The time course and constellation of symptoms may vary in adults and children with long COVID. As acknowledged in the WHO definition, some have persistent symptoms that linger after an acute infection, while others develop new or a relapse of symptoms after complete recovery from the initial infection [13•, 14]. Some of the fluctuation in symptom frequency and intensity may relate to post-exertional exacerbation in symptoms (discussed below). The literature describing pediatric long COVID remains sparse [15, 16], and there is a lack of consistency in how symptoms are elicited. Additional studies are needed to clarify the nature and duration of long COVID symptoms in pediatric populations.
-
Fatigue or low energy is one of the most common symptoms reported in children with long COVID, with recent studies suggesting that up to 87% of affected children report fatigue [10, 11•, 14, 17•, 18,19,20,21,22, 23••]. Fatigue in this population often leads to difficulty with physical and cognitive activity, which can limit participation in school, extracurricular activities, and sports. Excessive sleep, problems initiating or maintaining sleep, or non-refreshing sleep often accompany fatigue in pediatric long COVID. Fatigue may persist even with an improvement in sleep patterns.
-
Post-exertional malaise (PEM) is also common in long COVID. PEM refers to an exacerbation not just of fatigue, but of many symptoms, including lightheadedness, cognitive fogginess, sensory sensitivity, headaches, and pain, occurring after relative increases in physical activity or cognitive demands. Orthostatic stress and neuromuscular strain are additional triggers of PEM in ME/CFS and may also be capable of causing symptom exacerbations in long COVID [24, 25]. Sometimes typical activities of daily life like participation in a full day of school can lead to substantial PEM, thereby contributing to functional impairment and distress in these patients.
-
Cognitive difficulties or “brain fog” are also commonly reported by children with long COVID [10, 11•, 18, 19, 21, 23••]. Cognitive difficulties, while inconsistently ascertained in the literature, tend to include problems with concentration, short-term memory, and school performance [10, 11•, 17•, 18, 23••]. Similar to physical fatigue and PEM, cognitive difficulties or “brain fog” can also be exacerbated by mental exertion, such as schoolwork or studying for examinations.
-
Headaches are also commonly reported both in the acute and post-acute phase of COVID in children [10, 11•, 17•, 19,20,21,22, 23••, 26]. Additional studies are needed to characterize the nature and specific types of headaches experienced, as well as the best treatment options. Patients with a history of headaches prior to COVID infection may develop more severe or more frequent headaches, but these can arise as a new symptom. Headaches usually are not attributable to any secondary cause (brain lesion, brain injury, etc.).
-
Orthostatic symptoms: Many patients also report orthostatic symptoms, including lightheadedness or dizziness, syncope, blurred vision, exercise intolerance, dyspnea, chest discomfort, palpitations, tremulousness, anxiety, diaphoresis, and nausea [10, 17•, 22]. In some cases, patients meet criteria for postural tachycardia syndrome (POTS) or other forms of orthostatic intolerance (OI) [27]. Many patients with POTS also have overlapping symptoms with long COVID, including fatigue, cognitive difficulties, headaches, gastrointestinal symptoms, anxiety, and mood concerns. Other patients have heart rate changes that do not meet the threshold for POTS, but still experience significant orthostatic symptoms that may represent a spectrum of dysautonomia [17•].
-
Cardiopulmonary symptoms: Many adolescents have reported a variety of cardiopulmonary symptoms including dyspnea, chest pain or tightness, and cough [10, 11•, 17•, 21, 22, 23••, 28, 29]. In the absence of severe acute pulmonary disease, cardiopulmonary work-up in these patients tends to be negative [28, 29]. The underlying pathology for these symptoms is unclear at this point.
-
Mental health and behavioral symptoms also are prominent in this population, with anxiety and depression being the most prevalent [17•, 21, 30]. Whether this is directly related to the effects of the virus, effects of physical symptoms of long COVID or effects of the pandemic in general is not completely clear. However, recent studies in both adults and children suggest that mood and cognitive functioning after SARS-CoV-2 infection are impaired when compared to controls with similar pandemic-related experiences [31, 32].
-
Changes in taste and smell including anosmia, ageusia, parosmia, and dysgeusia are reported with acute SARS-CoV-2 infection in children [20] and adults [33]. Some children with long COVID also experience persistent alterations to taste and smell, impacting appetite and potentially leading to weight loss [10, 21, 23••, 26, 34]. These sensory alterations tend to cluster closer to the earlier phase of the illness.
Long COVID is a broad umbrella term that encompasses many symptoms. The symptoms described here are a subset of the ones that have been reported. Evidence is beginning to emerge that different phenotypes may exist within long COVID. We have found that adolescents experiencing prolonged symptoms after mild, acute COVID infection often report a phenotype that overlaps with OI or ME/CFS.
Epidemiology
The reported rates of prolonged symptoms following COVID-19 vary based on the age of the participants, the duration of follow-up (4 weeks vs 3 months vs 6–12 months), and the design of the study. Differences in design include whether the study population was clinic based or population based, whether there was a clinical evaluation to exclude other causes of symptoms, whether ascertainment of symptoms and function relied on validated questionnaires or on self- or parent-report, and on the precision with which specific symptoms were investigated. Few studies differentiate the rates of prolonged symptoms after SARS-CoV-2 infection from more general symptoms caused by the pandemic itself [32].
Currently, published studies on long COVID have used various designs to answer different epidemiologic questions. For instance, some ask: in patients who have had COVID-19 infection, what is the risk of developing long COVID? In hospital and clinic-based studies, 45–70% of patients with SARS-CoV-2 infection report prolonged symptoms for a variable duration after infection, but many of these studies do not have a comparison group, are subject to referral biases, and have relatively small sample sizes (reviewed by Zimmermann et al. [23••]). Larger studies and those with comparison groups have the potential to more accurately estimate symptom prevalence in patients with confirmed versus suspected SARS-CoV-2 infection. For example, the CLoCK study in the United Kingdom (UK) surveyed individuals aged 11–17-year-old 3 months after a positive PCR test and also enrolled controls who had a negative PCR test (performed due to symptoms, anxiety, contact, or other reasons) [22]. The prevalence of at least one symptom at 3 months of follow-up was 66.5% in test-positives versus 53.4% in test-negatives and 30.3% versus 16.2% respectively for three or more symptoms. These results must be interpreted with appropriate caution, as only 13% of the eligible test-positive and test-negative population responded to the survey, a limitation that also complicates interpretation of the incidence data from a nationwide study in Denmark [35].
Other studies have asked: what proportion of the population is experiencing symptoms suggestive of long COVID at this time? For example, a study by the National Office for Statistics in the UK reports a much lower prevalence of post-COVID conditions [36••]. The study randomly surveyed over 350,000 UK residents living in private households, defining long COVID as still experiencing symptoms 4 or more weeks after infection, including pre-existing symptoms that worsened after COVID. As illustrated in Fig. 1, post-COVID symptoms at 12 weeks and 12 months were least common in those ages 2–11 (0.21% vs 0.12%), increasing in 12–16-year-old (0.82% vs 0.26%) and approximating adult rates in the 17–24-year-old group (1.31% vs 0.48%).

Estimated percentage of UK respondents at different ages reporting persistent COVID-19 symptoms at 12 weeks and 12 months after suspected or confirmed infection (from reference 37, United Kingdom Office of National Statistics data collected in the 4 weeks preceding December 6, 2021, published January 6, 2022)
Several additional caveats are germane. Ascertainment of the full range of post-COVID symptoms was incomplete in early studies; many early post-COVID studies focused primarily on respiratory or infectious symptoms (e.g., shortness of breath, fever, congestion). Notably, symptoms associated with OI were not initially recognized, described, or assessed as being common [37•]. Moreover, attribution of individual symptoms to specific causes has been problematic in some studies. Labeling problems with attention, processing, and short-term memory as psychiatric symptoms could be misleading given that orthostatic stress can provoke cognitive problems in the absence of classical psychiatric conditions [38]. Similarly, in OI, orthostatic dyspnea can occur [39, 40], and the hyperadrenergic response to reductions in cerebral blood flow can be misinterpreted as anxiety [41].
Future large scale longitudinal studies with comparison groups are needed in order to understand the full constellation of symptoms, risk factors, and prevalence of long COVID in children and adolescents.
Orthostatic Intolerance After COVID-19 Infection
The common forms of OI are listed in Table 1. Beginning with the report of Miglis [42•], and followed by reports from a variety of centers (reviewed by Bisaccia et al.), it became clear that syndromes of OI were common in association with COVID-19 [43•]. Information on pediatric post-COVID OI is more limited. One case report describes a previously healthy 12-year-old girl who contracted COVID-19 in March 2020; orthostatic symptoms progressed until she became bedbound by July 2020 [44]. Testing revealed severely symptomatic OI associated with a drop in blood pressure and resting tachycardia. Another case series describes a 19-year-old male with confirmed COVID-19 who developed orthostatic symptoms within the first 2 weeks of infection [45]. Orthostatic testing 3 months into the illness revealed a striking 70-bpm increase in heart rate (HR) from supine to standing, consistent with POTS. In our pediatric post-COVID clinic, we perform a 10-min passive standing test (Table 2) in all patients. In a case series describing the initial cohort of patients seen at the Kennedy Krieger Institute Pediatric Post-COVID-19 Rehabilitation Clinic, two of eight patients met criteria for POTS, and all but one experienced increased symptoms during the 10 min upright, even though they did not meet formal HR criteria for POTS [17•]. In a case series of 20 adults who developed circulatory dysfunction after COVID-19 infection, many experienced improvement in symptoms with treatment targeted to OI [46], emphasizing the importance of recognizing OI as a treatable complication of COVID-19 infection.
Similar to the observed patterns of long COVID in children of different ages, OI affects adolescents more than pre-pubertal children, and females are more likely to be affected than males. OI can also be triggered by immunizations, pregnancy, surgery, or trauma [47••]. Symptom burden can be significant, resulting in limited ability to participate in school or work. POTS itself is heterogeneous, with several proposed mechanisms including autoimmunity [48], increased sympathetic activity [49], hypovolemia, and peripheral sympathetic noradrenergic denervation [50].
The development of OI following COVID-19 infection is not surprising. Prior to the pandemic, those with POTS specifically or OI in general often reported a history of infection closely preceding the onset of their orthostatic symptoms [51]. Among patients who develop lightheadedness and other orthostatic symptoms in the first 2 weeks of COVID-19 infection, it would be reasonable to postulate a direct effect of the virus on central autonomic networks [52]. The short time frame also argues against deconditioning or inactivity as an etiology of symptoms [45, 53]. For those developing symptoms beyond 2 weeks, after the emergence of antibodies directed at SARS-CoV-2, an autoimmune pathogenesis has been proposed, consistent with pre-pandemic observations that POTS may have an autoimmune etiology [54, 55].
It remains unclear whether OI is more prevalent or different in some manner after COVID-19 compared to other infections, and how long orthostatic symptoms after COVID-19 will persist [53]. As the number of patients affected by post-COVID OI increases, one challenge will be to meet the clinical demand, as the number of physicians treating OI was insufficient for the existing patient volume prior to the pandemic [46].
Is Long COVID a Unique Illness or Is SARS-CoV-2 Another Trigger for ME/CFS?
The illness formerly termed chronic fatigue syndrome is now referred to by the US National Institutes of Health and the Centers for Disease Control and Prevention as ME/CFS (Table 1) [56••]. While evidence of classical encephalomyelitis is not present, evidence of disturbed cognitive function and autonomic nervous system control are prominent. Early in the COVID-19 pandemic, it became clear that a subset of patients with prolonged symptoms had features consistent with ME/CFS. It remains to be determined whether these patients with long COVID persisting more than 6 months meet the criteria for ME/CFS or if long COVID is in some way distinctive. Our preliminary observations suggest that SARS-CoV-2 is emerging as a common trigger for ME/CFS.
As is true for the pathogenesis of ME/CFS, the cause or causes of long COVID remain uncertain. There may be different phenotypes of long COVID, and causes of long COVID are likely to be multifactorial in some patients. For certain patients, acute COVID-19 might exacerbate pre-existing ME/CFS. Prominent hypotheses for ME/CFS pathophysiology include autoimmunity [57,58,59], a physiologic stress response that does not attenuate once the acute infection or stressor has resolved [60], a chronic inflammatory response to an initial infection [61, 62] (including glial cell activation [63,64,65]), viral reactivation, or a hypo-metabolic cellular response. Any postulated mechanism must also explain the presence of circulatory dysfunction and reduced cerebral blood flow [66••] as a prominent component of the persistence of ME/CFS symptoms. OI has a prevalence of over 95% in pediatric patients with ME/CFS [56••, 67]. Recent evidence using extracranial Doppler echography of the vertebral and internal carotid arteries demonstrates that 90% of adults with ME/CFS experience significant reductions in cerebral blood flow during head-up tilt, confirming OI even when heart rate and blood pressure responses might be normal [66••].
Some of the current hypotheses for the development of long COVID include SARS-CoV-2 tropism for the brainstem [68•, 69], renin-angiotensin system dysfunction leading to central and peripheral circulatory abnormalities [70], chronic immune activation [71, 72], mast cell activation [70, 73•], persistence of whole virus or remnants of SARS-CoV-2 [74], the ability of the virus to lead to hemostatic imbalance, reactivation of Epstein-Barr virus (EBV) [75, 76] and other viruses, interference with fibrinolysis and promotion of micro-thrombi [77, 78], and the development of auto-antibodies [79,80,81].
Our experience in a single center suggests that a subset of adolescents with a moderate or severe burden of long COVID symptoms and impaired health-related quality of life have features consistent with ME/CFS [45]. One recent case–control study in adults shows that cerebral blood flow reductions during upright posture in long COVID patients are at least as severe as the reductions in comparison groups with ME/CFS and POTS and ME/CFS with a normal heart rate and blood pressure response to upright posture [82•]. In the 10 long COVID patients, all of whom had POTS, cerebral blood flow fell 33% over the 30 min upright, comparable to the 20 with ME/CFS and POTS (29%) and the 20 with ME/CFS and a normal heart rate and blood pressure response (25%), all significantly different than the 4% reduction in cerebral blood flow for the 20 healthy controls.
Whether the risk factors and co-morbid clinical conditions in long COVID are similar to those in pediatric ME/CFS remains to be determined. Prominent biological risk factors previously identified for pediatric ME/CFS include age [83•] (adolescents more affected than pre-pubertal children), sex (females are affected 3–4 times more commonly [84]), and joint hypermobility [85] (seen in 60% with ME/CFS versus 20–24% of age and sex-matched controls). One trial of IVIG for pediatric ME/CFS identified cutaneous anergy in 21% [86]. Conditions found more commonly in ME/CFS (possibly a consequence of the initial infectious or inflammatory trigger but also possibly preceding the illness and creating a risk of prolonged impairment) include OI in > 95% [67, 87], allergic inflammation [88], mast cell activation syndrome (MCAS) in a subset [89], and restrictions in symptom-free range of motion in > 80% [24, 90]. Further research is needed to determine whether treatment for co-morbid conditions in pediatric ME/CFS is relevant to and improves function in pediatric long COVID.
Management
There may be several distinct types of post-COVID conditions that require different treatments. At this time, there is no single pharmacologic agent for all variations of post-COVID symptoms nor is there a uniform treatment approach. Several groups have authored recommendations for investigation and management [91•, 92, 93, 94•]. The provisional CDC guidance states that some presentations of post-COVID conditions mimic disorders such as ME/CFS, MCAS, and OI [93]. Treatment guidelines for these conditions can be helpful for managing post-COVID symptoms. At present, the management of post-COVID conditions focuses primarily on addressing symptoms. Based on our clinical experience evaluating pediatric OI and ME/CFS, our approach includes the diagnostic testing in Table 2. Below we offer evaluation and management suggestions for specific symptoms:
Orthostatic Intolerance
Although lightheadedness/dizziness has been ascertained in some long COVID studies [10, 26], OI is not ascertained in a consistent manner in the majority of the pediatric long COVID literature. It is important to ask about specific conditions that can provoke orthostatic symptoms, and not simply to ask about lightheadedness, as adolescent patients may not be aware that what they experience is abnormal. Typical situations that provoke symptoms in those with OI include standing in line, standing at a reception or religious service, shopping, showering, and being in hot environments. To elicit symptoms of OI, practitioners might ask questions such as “How long can you stand still before having to sit down?” and “Do you fidget and move around when standing, study in a reclining position, or sit with your knees to your chest or with your feet under you?”.
The CDC guidance recommends testing post-COVID patients with a 3-min standing test [93]. However, a 3-min standing test will miss 43% of adolescent and young adult patients with POTS [95]. While 10 min is insufficient to document NMH, most patients with NMH or low orthostatic tolerance will be quite symptomatic during the first ten minutes upright. An at-home 10-min standing test using a heart rate monitor might be a helpful screening measure, but needs to be supervised because of the potential for developing syncope. Formal tilt-table testing is expensive and not always available, but might be warranted in specific situations or research studies [96].
If the patient presents with OI, non-pharmacological management can be initiated with simple treatments like avoiding aggravating conditions, increasing dietary salt and fluid intake, using cooling garments, and employing postural counter-maneuvers and wearing compression garments to reduce gravitational pooling of blood and improve the blood return to the heart [97, 98]. Gradual increases in activity, designed to avoid provoking PEM, are part of the overall approach [99, 100]. If non-pharmacologic management alone is insufficient, a variety of medications can be used, such as vasoconstrictors (e.g., midodrine, stimulants), agents that improve blood volume (e.g., hormonal birth control therapy, fludrocortisone, desmopressin acetate), and medicines that control sympathetic tone, heart rate, or the effect and release of catecholamines (e.g., beta-blockers, clonidine, SSRIs/SNRIs, pyridostigmine bromide, ivabradine). Doses are published elsewhere [83•]. Medications can be selected based on a variety of clinical factors, including the resting heart rate and blood pressure, and whether two problems can be treated with a single medication. For example, a beta-blocker might be appropriate in the presence of a relatively high resting heart rate or in someone with headaches. Fludrocortisone might be a better first choice in somebody with a low resting blood pressure or a very high salt appetite. Stimulants or clonidine can treat both OI and cognitive dysfunction. OI is one of the more treatable components of ME/CFS and may prove to have similar benefits in long COVID.
PEM and Managing Activity
Exercise intolerance was identified as a common symptom in some pediatric long COVID studies [8, 101•], but few have ascertained for PEM. We recommend utilizing pacing techniques for many post-COVID symptoms. Pacing as a management technique can be helpful to avoid exacerbating symptoms. Gradual return to activities should be approached with caution and modified to accommodate the severity of each patient’s condition. For patients who are moderately to severely impaired and cannot tolerate exercise while seated or standing, exercise should occur while lying down. Start with stretching for 1–2 min and increase the duration of activity gradually as long as PEM is not provoked. For the mildly impaired, start with 5–15 min of walking. Manual forms of physical therapy can be a bridge to tolerating exercise. Sometimes exercise will not be tolerated until OI is adequately treated [83•].
Cognitive Dysfunction
Cognitive impairments can be demonstrated on baseline neuropsychiatric testing, but may also emerge with more complex tasks and in response to upright tilt-table testing [38]. Aside from treating OI as mentioned above, helpful strategies include dividing work into smaller and more manageable sections, performing mental work lying down, snacks and regular fluid intake, and reducing stressors [83•]. In some instances, stimulants may be helpful. A gradual transition back to learning is recommended, with educational and environmental accommodations as needed.
Behavioral Symptoms
Referral to a psychologist can be helpful for those who are struggling to cope with the effects of the illness or who have true depression or anxiety disorders. A behavioral psychologist can also work with patients to incorporate the lifestyle modifications that are recommended for management of long COVID, OI, or ME/CFS. It remains to be seen whether behavioral symptoms in long COVID will be similar to ME/CFS. While adolescents with ME/CFS might be frustrated and demoralized by their illness, they are less likely to endorse the primary features of depression such as feelings of worthlessness, guilt, and low self-esteem, or a lack of interest in friendships, relationships, or activities they previously enjoyed [83•]. ME/CFS differs from depression in that individuals with depression often feel better after exercise, while untreated ME/CFS patients can have a prolonged post-exertional increase in symptoms. Patients with ME/CFS have plans for the future and would like to participate in school and other activities but are often physically limited by their symptoms [83•].
Headaches
For those experiencing headaches, lifestyle modifications can be effective for many. These include stress management, adequate hydration, identifying and avoiding headache triggers, and satisfactory sleep patterns [102,103,104]. Neuroimaging may be warranted if abnormalities are present on a neurological examination or if there are red flags on history that are concerning for increase intracranial pressure or secondary causes of headache [103, 104]. Medications for preventing headaches can include magnesium, riboflavin, cyproheptadine, beta-adrenergic antagonists, tricyclic antidepressant medications, anti-convulsants, and, for those with migraines, calcitonin gene receptor antagonists [102, 104].
Sleep Disturbances
Patients experiencing sleep disturbances can benefit from a specified, regular bedtime, avoiding daytime naps where possible, and avoiding caffeine late in the day. Using phones, computers, or other electronics after “lights out” can aggravate fatigue and should be avoided after bedtime. White noise or meditative phone apps can be helpful. Parents may need to awaken those with hypersomnolence after 12 h of sleep to ensure better hydration. Individuals can go back to sleep if needed, but long periods of uninterrupted sleep promote low blood volume and can aggravate OI. If insomnia is impressive and unresponsive to relaxation techniques and standard sleep hygiene measures, pharmacologic treatment may be needed.
MCAS and Allergic Phenomenon
MCAS has emerged as a co-morbid and potentially causal factor in patients with OI and ME/CFS and has been hypothesized as a pathophysiologic influence on the severity of COVID-19 [105•]. Infections of all types as well as physical and chemical stimuli can activate mast cells, leading to degranulation and release of multiple mediators, including histamine and cytokines [106]. Clinical suspicion for MCAS increases in those with recurring rashes, pruritus, urticaria, facial flushing, and an intolerance of multiple foods and medications. Treatment consists of avoidance of triggers, as well as the addition of antihistamines and medications to stabilize mast cell membranes such as cromolyn, leukotriene inhibitors, and others.
Some allergic phenomena may be addressed with dietary changes. For example, up to 31% of ME/CFS adolescents in one study met the criteria for a delayed cow’s milk protein hypersensitivity, which can be recognized by a triad of upper gastrointestinal symptoms that include epigastric pain, gastroesophageal reflux, and early satiety, sometimes associated with recurrent aphthous ulcers [88]. A diet free of cow’s milk protein in those with milk protein intolerance usually improves the local upper gastrointestinal symptoms, and in some can improve overall well-being, fatigue, and orthostatic symptoms.
Individualized Approach
Mononucleosis can cause persistent fatigue in 13% of adolescents at 6 months post-infection [107]. As with mononucleosis, there is likely to be some spontaneous improvement over time in those with milder post-COVID symptoms. Consequently, some patients may not need intensive intervention and can expand activities as tolerated. Similarly, recommendations cover a broad range of symptoms and may not apply to each patient. Although a patient may meet long COVID diagnostic criteria, we recommend that patients be evaluated on a case-by-case basis. A standing test or pharmacological intervention will not be necessary for every presenting patient. In a setting of limited resources, practitioner discretion will help to avoid inundating long COVID clinics with those who do not require extensive care and will leave resources for individuals with increasingly severe impairments. We recommend that follow-up time and treatment be decided according to the impact long COVID has on the patient’s quality of life.
Conclusion
Emerging data confirm that prolonged symptoms can develop following even mild or asymptomatic initial SARS-CoV-2 infection. The most common symptoms are fatigue, cognitive dysfunction, and headaches. As ascertainment for orthostatic intolerance in these patients improves, lightheadedness is becoming more commonly recognized. A proportion of long COVID patients meet the criteria for ME/CFS at 6 months. At present, management of post-COVID conditions focuses primarily on addressing symptoms, borrowing management strategies from conditions like OI and ME/CFS.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
The Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU): COVID-19 Dashboard. https://coronavirus.jhu.edu/map.html (2022). Accessed January 14, 2022.
•• Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2021. https://doi.org/10.1016/S1473-3099(21)00703-9. (WHO case definition; a pediatric version is expected soon.)
Centers for Disease Control and Prevention: Information for Healthcare Providers about Multisystem Inflammatory Syndrome in Children (MIS-C). https://www.cdc.gov/mis/mis-c/hcp/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fmis%2Fhcp%2Findex.html (2021). Accessed December 30, 2021.
Farooqi KM, Chan A, Weller RJ, Mi J, Jiang P, Abrahams E, et al. Longitudinal outcomes for multisystem inflammatory syndrome in children. Pediatrics. 2021;148(2). https://doi.org/10.1542/peds.2021-051155.
Davies P, du Pré P, Lillie J, Kanthimathinathan HK. One-year outcomes of critical care patients post–COVID-19 multisystem inflammatory syndrome in children. JAMA Pediatr. 2021;175(12):1281–3. https://doi.org/10.1001/jamapediatrics.2021.2993.
• Crook H, Raza S, Nowell J, Young M, Edison P. Long covid-mechanisms, risk factors, and management. BMJ. 2021;374: n1648. https://doi.org/10.1136/bmj.n1648. (Comprehensive review.)
• Centers for Disease Control and Prevention: Post-COVID conditions: information for healthcare providers. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html (2021). Accessed December 30, 2021. (Helpful clinical guidance.)
Asadi-Pooya AA, Nemati H, Shahisavandi M, Akbari A, Emami A, Lotfi M, et al. Long COVID in children and adolescents. World J Pediatr. 2021;17(5):495–9. https://doi.org/10.1007/s12519-021-00457-6.
Osmanov IM, Spiridonova E, Bobkova P, Gamirova A, Shikhaleva A, Andreeva M, et al. Risk factors for long covid in previously hospitalised children using the ISARIC Global follow-up protocol: a prospective cohort study. Eur Respir J. 2021. https://doi.org/10.1183/13993003.01341-2021.
Ashkenazi-Hoffnung L, Shmueli E, Ehrlich S, Ziv A, Bar-On O, Birk E, et al. Long COVID in children: observations from a designated pediatric clinic. Pediatr Infect Dis J. 2021;40(12):e509–11. https://doi.org/10.1097/inf.0000000000003285.
• Buonsenso D, Munblit D, De Rose C, Sinatti D, Ricchiuto A, Carfi A, et al. Preliminary evidence on long COVID in children. Acta Paediatr. 2021;110(7):2208–11. https://doi.org/10.1111/apa.15870. (Single center experience with pediatric long-COVID, with ranking of symptom frequency.)
Say D, Crawford N, McNab S, Wurzel D, Steer A, Tosif S. Post-acute COVID-19 outcomes in children with mild and asymptomatic disease. Lancet Child Adolesc Health. 2021;5(6):e22–3. https://doi.org/10.1016/s2352-4642(21)00124-3.
• Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Re’em Y, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. medRxiv. 2020:2020.12.24.20248802. https://doi.org/10.1101/2020.12.24.20248802. (Important early on-line survey of long COVID symptoms in adults.)
Buonsenso D, Espuny Pujol F, Munblit D, McFarland S, Simpson F. Clinical characteristics, activity levels and mental health problems in children with long COVID: a survey of 510 Children. Preprints.org; 2021.
Michelen M, Manoharan L, Elkheir N, Cheng V, Dagens A, Hastie C, et al. Characterising long COVID: a living systematic review. BMJ Glob Health. 2021;6(9). https://doi.org/10.1136/bmjgh-2021-005427.
Munblit D, Sigfrid L, Warner JO. Setting priorities to address research gaps in long-term COVID-19 outcomes in children. JAMA Pediatr. 2021;175(11):1095–6. https://doi.org/10.1001/jamapediatrics.2021.2281.
• Morrow AK, Ng R, Vargas G, Jashar DT, Henning E, Stinson N, et al. Postacute/long COVID in pediatrics: development of a multidisciplinary rehabilitation clinic and preliminary case series. Am J Phys Med Rehabil. 2021;100(12):1140–7. https://doi.org/10.1097/phm.0000000000001896. (Describes features of a multidisciplinary pediatric long COVID clinic.)
Brackel CLH, Lap CR, Buddingh EP, van Houten MA, van der Sande L, Langereis EJ, et al. Pediatric long-COVID: an overlooked phenomenon? Pediatr Pulmonol. 2021;56(8):2495–502. https://doi.org/10.1002/ppul.25521.
Matteudi T, Luciani L, Fabre A, Minodier P, Boucekine M, Bosdure E, et al. Clinical characteristics of paediatric COVID-19 patients followed for up to 13 months. Acta Paediatr. 2021;110(12):3331–3. https://doi.org/10.1111/apa.16071.
Molteni E, Sudre CH, Canas LS, Bhopal SS, Hughes RC, Antonelli M, et al. Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2. Lancet Child Adolesc Health. 2021;5(10):708–18. https://doi.org/10.1016/s2352-4642(21)00198-x.
Roge I, Smane L, Kivite-Urtane A, Pucuka Z, Racko I, Klavina L, et al. Comparison of persistent symptoms after COVID-19 and other non-SARS-CoV-2 infections in children. Frontiers in Pediatrics. 2021;9(1177). https://doi.org/10.3389/fped.2021.752385.
Stephenson T, Pereira S, Shafran R, De Stavola B, Rojas N, McOwat K, et al. Long COVID - the physical and mental health of children and non-hospitalised young people 3 months after SARS-CoV-2 infection; a national matched cohort study (The CLoCk) Study. ResearchSquare. 2021. https://doi.org/10.21203/rs.3.rs-798316/v1.
•• Zimmermann P, Pittet LF, Curtis N. How common is long COVID in children and adolescents? Pediatr Infect Dis J. 2021;40(12):e482–7. https://doi.org/10.1097/inf.0000000000003328. (Elegant review of the methodological challenges in pediatric long-COVID studies.)
Rowe PC, Fontaine KR, Lauver M, Jasion SE, Marden CL, Moni M, et al. Neuromuscular strain increases symptom intensity in chronic fatigue syndrome. PLoS ONE. 2016;11(7): e0159386. https://doi.org/10.1371/journal.pone.0159386.
van Campen CMC, Rowe PC, Verheugt FWA, Visser FC. Numeric rating scales show prolonged post-exertional symptoms after orthostatic testing of adults with myalgic encephalomyelitis/chronic fatigue syndrome. Frontiers in Medicine. 2021;7(1083). https://doi.org/10.3389/fmed.2020.602894.
Smane L, Roge I, Pucuka Z, Pavare J. Clinical features of pediatric post-acute COVID-19: a descriptive retrospective follow-up study. Ital J Pediatr. 2021;47(1):177. https://doi.org/10.1186/s13052-021-01127-z.
Raj SR, Arnold AC, Barboi A, Claydon VE, Limberg JK, Lucci VM, et al. Long-COVID postural tachycardia syndrome: an American Autonomic Society statement. Clin Auton Res. 2021;31(3):365–8. https://doi.org/10.1007/s10286-021-00798-2.
Leftin Dobkin SC. Respiratory findings in children post-COVID-19 infection. American Journal of Respiratory and Critical Care Medicine. 2021;203(9). https://doi.org/10.1164/ajrccm-conference.2021.203.1_MeetingAbstracts.A3404.
Knoke L, Schlegtendal A, Maier C, Eitner L, Luecke T, Brinkmann F. More complaints than findings - Long-term pulmonary function in children and adolescents after COVID-19. 2021.
Victor MC, Faith MG, Roy HP. Persistence of neuropsychiatric symptoms associated with SARS-CoV-2 positivity among a cohort of children and adolescents. medRxiv. 2021. https://doi.org/10.1101/2021.09.28.21264259.
Lamontagne SJ, Winters MF, Pizzagalli DA, Olmstead MC. Post-acute sequelae of COVID-19: Evidence of mood & cognitive impairment. Brain Behav Immun Health. 2021;17: 100347. https://doi.org/10.1016/j.bbih.2021.100347.
Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA Pediatr. 2021;175(11):1142–50. https://doi.org/10.1001/jamapediatrics.2021.2482.
Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A, et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol. 2020;277(8):2251–61. https://doi.org/10.1007/s00405-020-05965-1.
Blomberg B, Mohn KG, Brokstad KA, Zhou F, Linchausen DW, Hansen BA, et al. Long COVID in a prospective cohort of home-isolated patients. Nat Med. 2021;27(9):1607–13. https://doi.org/10.1038/s41591-021-01433-3.
Borch L, Holm M, Knudsen M, Ellermann-Eriksen S, Hagstroem S. Long COVID symptoms and duration in SARS-CoV-2 positive children — a nationwide cohort study. Eur J Pediatr. 2022. https://doi.org/10.1007/s00431-021-04345-z.
•• Office for National Statistics. Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK. 2022. (Rich database on persistent symptoms post-COVID by age and impact.)
• Carfì A, Bernabei R, Landi F, Group ftGAC-P-ACS. Persistent symptoms in patients after acute COVID-19. JAMA. 2020;324(6):603–5. https://doi.org/10.1001/jama.2020.12603. (Early report drawing attention to persistent fatigue post-COVID in adults.)
Ocon AJ, Messer ZR, Medow MS, Stewart JM. Increasing orthostatic stress impairs neurocognitive functioning in chronic fatigue syndrome with postural tachycardia syndrome. Clin Sci. 2011;122(5):227–38. https://doi.org/10.1042/cs20110241.
Del Pozzi AT, Schwartz CE, Tewari D, Medow MS, Stewart JM. Reduced cerebral lood flow with orthostasis precedes hypocapnic hyperpnea, sympathetic activation, and postural tachycardia syndrome. Hypertension. 2014;63(6):1302–8. https://doi.org/10.1161/HYPERTENSIONAHA.113.02824.
Gibbons CH, Freeman R. Orthostatic dyspnea: a neglected symptom of orthostatic hypotension. Clin Auton Res. 2005;15(1):40–4. https://doi.org/10.1007/s10286-005-0227-1.
Owens AP, Low DA, Iodice V, Critchley HD, Mathias CJ. The genesis and presentation of anxiety in disorders of autonomic overexcitation. Autonomic Neuroscience: Basic and Clinical. 2017;203:81–7. https://doi.org/10.1016/j.autneu.2016.10.004.
Miglis MG, Prieto T, Shaik R, Muppidi S, Sinn D-I, Jaradeh S. A case report of postural tachycardia syndrome after COVID-19. Clin Auton Res. 2020;30(5):449–51. https://doi.org/10.1007/s10286-020-00727-9.Earlydescriptionofpost-COVIDPOTS.
• Bisaccia G, Ricci F, Recce V, Serio A, Iannetti G, Chahal AA, et al. Post-acute sequelae of COVID-19 and cardiovascular autonomic dysfunction: what do we know? J Cardiovasc Dev Dis. 2021;8(11). https://doi.org/10.3390/jcdd8110156. (Review of post-COVID circulatory dysfunction.)
Younger DS. Post-acute sequelae of SARS-CoV-2 infection (PASC): peripheral, autonomic, and central nervous system features in a child. Neurol Sci. 2021;42(10):3959–63. https://doi.org/10.1007/s10072-021-05345-5.
Petracek LS, Suskauer SJ, Vickers RF, Patel NR, Violand RL, Swope RL, et al. Adolescent and young adult ME/CFS after confirmed or probable COVID-19. Frontiers in Medicine. 2021;8(525). https://doi.org/10.3389/fmed.2021.668944.
Blitshteyn S, Whitelaw S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: a case series of 20 patients. Immunol Res. 2021;69(2):205–11. https://doi.org/10.1007/s12026-021-09185-5.
•• Vernino S, Bourne KM, Stiles LE, Grubb BP, Fedorowski A, Stewart JM, et al. Postural orthostatic tachycardia syndrome (POTS): state of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting - Part 1. Autonomic Neuroscience. 2021:102828. https://doi.org/10.1016/j.autneu.2021.102828. (Excellent recent review on POTS.)
Low PA, Opfer-Gehrking TL, Textor SC, Benarroch EE, Shen WK, Schondorf R, et al. Postural tachycardia syndrome (POTS). Neurology. 1995;45(4 Suppl 5):S19-25.
Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia? Neurology. 1993;43(1):132–7. https://doi.org/10.1212/wnl.43.1_part_1.132.
Bonyhay I, Freeman R. Sympathetic nerve activity in response to hypotensive stress in the postural tachycardia syndrome. Circulation. 2004;110(20):3193–8. https://doi.org/10.1161/01.Cir.0000147280.90339.E9.
Sandroni P, Opfer-Gehrking TL, McPhee BR, Low PA. Postural tachycardia syndrome: clinical features and follow-up study. Mayo Clin Proc. 1999;74(11):1106–10. https://doi.org/10.4065/74.11.1106.
Goldstein DS. The extended autonomic system, dyshomeostasis, and COVID-19. Clin Auton Res. 2020;30(4):299–315. https://doi.org/10.1007/s10286-020-00714-0.
Goodman BP, Khoury JA, Blair JE, Grill MF. COVID-19 dysautonomia. Front Neurol. 2021;12: 624968. https://doi.org/10.3389/fneur.2021.624968.
Gunning WT 3rd, Kvale H, Kramer PM, Karabin BL, Grubb BP. Postural orthostatic tachycardia syndrome is associated with elevated G-protein coupled receptor autoantibodies. J Am Heart Assoc. 2019;8(18): e013602. https://doi.org/10.1161/jaha.119.013602.
Li H, Yu X, Liles C, Khan M, Vanderlinde-Wood M, Galloway A, et al. Autoimmune basis for postural tachycardia syndrome. J Am Heart Assoc. 2014;3(1): e000755. https://doi.org/10.1161/jaha.113.000755.
•• Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome, Board on the Health of Select Populations, Institute of Medicine. The National Academies Collection: Reports funded by National Institutes of Health. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Washington (DC): National Academies Press (US) Copyright 2015 by the National Academy of Sciences. All rights reserved.; 2015. (Comprehensive review of the core symptoms and diagnosis of ME/CFS.)
Sotzny F, Blanco J, Capelli E, Castro-Marrero J, Steiner S, Murovska M, et al. Myalgic encephalomyelitis/chronic fatigue syndrome - evidence for an autoimmune disease. Autoimmun Rev. 2018;17(6):601–9. https://doi.org/10.1016/j.autrev.2018.01.009.
Bynke A, Julin P, Gottfries CG, Heidecke H, Scheibenbogen C, Bergquist J. Autoantibodies to beta-adrenergic and muscarinic cholinergic receptors in Myalgic Encephalomyelitis (ME) patients - A validation study in plasma and cerebrospinal fluid from two Swedish cohorts. Brain Behav Immun Health. 2020;7: 100107. https://doi.org/10.1016/j.bbih.2020.100107.
Loebel M, Grabowski P, Heidecke H, Bauer S, Hanitsch LG, Wittke K, et al. Antibodies to β adrenergic and muscarinic cholinergic receptors in patients with chronic fatigue syndrome. Brain Behav Immun. 2016;52:32–9. https://doi.org/10.1016/j.bbi.2015.09.013.
Mackay A. A paradigm for post-Covid-19 fatigue syndrome analogous to ME/CFS. Front Neurol. 2021;12: 701419. https://doi.org/10.3389/fneur.2021.701419.
Bansal AS, Bradley AS, Bishop KN, Kiani-Alikhan S, Ford B. Chronic fatigue syndrome, the immune system and viral infection. Brain Behav Immun. 2012;26(1):24–31. https://doi.org/10.1016/j.bbi.2011.06.016.
Stewart CC, Cookfair DL, Hovey KM, Wende KE, Bell DS, Warner CL. Predictive immunophenotypes: disease-related profile in chronic fatigue syndrome. Cytometry B Clin Cytom. 2003;53(1):26–33. https://doi.org/10.1002/cyto.b.10034.
Nakatomi Y, Kuratsune H, Watanabe Y. Neuroinflammation in the brain of patients with myalgic encephalomyelitis/chronic fatigue syndrome. Brain Nerve. 2018;70(1):19–25. https://doi.org/10.11477/mf.1416200945.
Noda M, Ifuku M, Hossain MS, Katafuchi T. Glial activation and expression of the serotonin transporter in chronic fatigue syndrome. Front Psychiatry. 2018;9:589. https://doi.org/10.3389/fpsyt.2018.00589.
Glassford JA. The neuroinflammatory etiopathology of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Front Physiol. 2017;8:88. https://doi.org/10.3389/fphys.2017.00088.
•• van Campen CMC, Verheugt FWA, Rowe PC, Visser FC. Cerebral blood flow is reduced in ME/CFS during head-up tilt testing even in the absence of hypotension or tachycardia: a quantitative, controlled study using Doppler echography. Clin Neurophysiol Pract. 2020;5:50–8. https://doi.org/10.1016/j.cnp.2020.01.003. (Novel, large study confirming the reductions in cerebral blood flow during upright tilt in adults with ME/CFS.)
Stewart JM, Gewitz MH, Weldon A, Arlievsky N, Li K, Munoz J. Orthostatic intolerance in adolescent chronic fatigue syndrome. Pediatrics. 1999;103(1):116–21. https://doi.org/10.1542/peds.103.1.116.
• Yong SJ. Persistent brainstem dysfunction in long-COVID: a hypothesis. ACS Chem Neurosci. 2021;12(4):573–80. https://doi.org/10.1021/acschemneuro.0c00793. (Intriguing hypothesis on pathogenesis.)
Meinhardt J, Radke J, Dittmayer C, Franz J, Thomas C, Mothes R, et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat Neurosci. 2021;24(2):168–75. https://doi.org/10.1038/s41593-020-00758-5.
Hassani M, Fathi Jouzdani A, Motarjem S, Ranjbar A, Khansari N. How COVID-19 can cause autonomic dysfunctions and postural orthostatic syndrome? A review of mechanisms and evidence. Neurol Clin Neurosci. 2021;9(6):434–42. https://doi.org/10.1111/ncn3.12548.
Hu F, Chen F, Ou Z, Fan Q, Tan X, Wang Y, et al. A compromised specific humoral immune response against the SARS-CoV-2 receptor-binding domain is related to viral persistence and periodic shedding in the gastrointestinal tract. Cell Mol Immunol. 2020;17(11):1119–25. https://doi.org/10.1038/s41423-020-00550-2.
Liu B, Han J, Cheng X, Yu L, Zhang L, Wang W, et al. Reduced numbers of T cells and B cells correlates with persistent SARS-CoV-2 presence in non-severe COVID-19 patients. Sci Rep. 2020;10(1):17718. https://doi.org/10.1038/s41598-020-73955-8.
• Weinstock LB, Brook JB, Walters AS, Goris A, Afrin LB, Molderings GJ. Mast cell activation symptoms are prevalent in Long-COVID. Int J Infect Dis. 2021;112:217–26. https://doi.org/10.1016/j.ijid.2021.09.043. (Novel examination of mast cell symptoms in long COVID.)
Vibholm LK, Nielsen SSF, Pahus MH, Frattari GS, Olesen R, Andersen R, et al. SARS-CoV-2 persistence is associated with antigen-specific CD8 T-cell responses. EBioMedicine. 2021;64: 103230. https://doi.org/10.1016/j.ebiom.2021.103230.
Chen T, Song J, Liu H, Zheng H, Chen C. Positive Epstein-Barr virus detection in coronavirus disease 2019 (COVID-19) patients. Sci Rep. 2021;11(1):10902. https://doi.org/10.1038/s41598-021-90351-y.
Gold JE, Okyay RA, Licht WE, Hurley DJ. Investigation of long COVID prevalence and its relationship to Epstein-Barr virus reactivation. Pathogens. 2021;10(6). https://doi.org/10.3390/pathogens10060763.
Grobbelaar LM, Venter C, Vlok M, Ngoepe M, Laubscher GJ, Lourens PJ, et al. SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19. Biosci Rep. 2021;41(8):BSR20210611. https://doi.org/10.1042/bsr20210611.
Pretorius E, Vlok M, Venter C, Bezuidenhout JA, Laubscher GJ, Steenkamp J, et al. Persistent clotting protein pathology in long COVID/post-acute sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol. 2021;20(1):172. https://doi.org/10.1186/s12933-021-01359-7.
Bertin D, Kaphan E, Weber S, Babacci B, Arcani R, Faucher B, et al. Persistent IgG anticardiolipin autoantibodies are associated with post-COVID syndrome. Int J Infect Dis. 2021;113:23–5. https://doi.org/10.1016/j.ijid.2021.09.079.
Hohberger B, Harrer T, Mardin C, Kruse F, Hoffmanns J, Rogge L, et al. Case report: neutralization of autoantibodies targeting G-protein-coupled receptors improves capillary impairment and fatigue symptoms after COVID-19 infection. Front Med (Lausanne). 2021;8: 754667. https://doi.org/10.3389/fmed.2021.754667.
Khamsi R. Rogue antibodies could be driving severe COVID-19. Nature. 2021;590(7844):29–31. https://doi.org/10.1038/d41586-021-00149-1.
• van Campen CMC, Rowe PC, Visser FC. Orthostatic symptoms and reductions in cerebral blood low in long-haul COVID-19 patients: similarities with myalgic encephalomyelitis/chronic fatigue syndrome. Medicina. 2022;58(1):28. https://doi.org/10.3390/medicina58010028. (First demonstration that cerebral blood flow is reduced during tilt in long COVID.)
• Rowe PC, Underhill RA, Friedman KJ, Gurwitt A, Medow MS, Schwartz MS, et al. Myalgic encephalomyelitis/chronic fatigue syndrome diagnosis and management in young people: a primer. Frontiers in Pediatrics. 2017;5(121). https://doi.org/10.3389/fped.2017.00121. (Practical Open-Access monograph on the diagnosis and management of pediatric ME/CFS.)
Nijhof SL, Maijer K, Bleijenberg G, Uiterwaal CS, Kimpen JL, van de Putte EM. Adolescent chronic fatigue syndrome: prevalence, incidence, and morbidity. Pediatrics. 2011;127(5):e1169–75. https://doi.org/10.1542/peds.2010-1147.
Hakim A, De Wandele I, O’Callaghan C, Pocinki A, Rowe P. Chronic fatigue in Ehlers-Danlos syndrome-hypermobile type. Am J Med Genet C Semin Med Genet. 2017;175(1):175–80. https://doi.org/10.1002/ajmg.c.31542.
Rowe KS. Double-blind randomized controlled trial to assess the efficacy of intravenous gammaglobulin for the management of chronic fatigue syndrome in adolescents. J Psychiatr Res. 1997;31(1):133–47. https://doi.org/10.1016/s0022-3956(96)00047-7.
Stewart JM. Autonomic nervous system dysfunction in adolescents with postural orthostatic tachycardia syndrome and chronic fatigue syndrome is characterized by attenuated vagal baroreflex and potentiated sympathetic vasomotion. Pediatr Res. 2000;48(2):218–26. https://doi.org/10.1203/00006450-200008000-00016.
Rowe PC, Marden CL, Jasion SE, Cranston EM, Flaherty MA, Kelly KJ. Cow’s milk protein intolerance in adolescents and young adults with chronic fatigue syndrome. Acta Paediatr. 2016;105(9):e412–8. https://doi.org/10.1111/apa.13476.
Shibao C, Arzubiaga C, Roberts LJ, Raj S, Black B, Harris P, et al. Hyperadrenergic postural tachycardia syndrome in mast cell activation disorders. Hypertension. 2005;45(3):385–90. https://doi.org/10.1161/01.HYP.0000158259.68614.40.
Rowe PC, Marden CL, Flaherty MAK, Jasion SE, Cranston EM, Fontaine KR, et al. Two-year follow-up of impaired range of motion in chronic fatigue syndrome. J Pediatrics. 2018;200:249-53.e1. https://doi.org/10.1016/j.jpeds.2018.05.012.
• Vance H, Maslach A, Stoneman E, Harmes K, Ransom A, Seagly K, et al. Addressing post-COVID symptoms: a guide for primary care physicians. J Am Board Fam Med. 2021;34(6):1229–42. https://doi.org/10.3122/jabfm.2021.06.210254. (Helpful summary of long COVID management suggestions.)
Chaplin S. Summary of joint guideline on the management of long COVID. Prescriber. 2021;32(8–9):33–5. https://doi.org/10.1002/psb.1941.
Centers for Disease Control and Prevention: evaluating and caring for patients with post-COVID conditions: interim guidance. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-index.html (2021). Accessed December 22, 2021 2021.
• Herrera JE, Niehaus WN, Whiteson J, Azola A, Baratta JM, Fleming TK, et al. Multidisciplinary collaborative consensus guidance statement on the assessment and treatment of fatigue in postacute sequelae of SARS-CoV-2 infection (PASC) patients. PMR. 2021;13(9):1027–43. https://doi.org/10.1002/pmrj.12684. (Helpful summary of long COVID management suggestions.)
Roma M, Marden CL, Rowe PC. Passive standing tests for the office diagnosis of postural tachycardia syndrome: new methodological considerations. Fatigue: Biomedicine, Health & Behavior. 2018;6(4):179–92. https://doi.org/10.1080/21641846.2018.1512836.
Shen WK, Sheldon RS, Benditt DG, Cohen MI, Forman DE, Goldberger ZD, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2017;136(5):e25–59. https://doi.org/10.1161/cir.0000000000000498.
van Campen CMC, Rowe PC, Visser FC. Compression stockings improve cardiac output and cerebral blood flow during tilt testing in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) patients: a randomized crossover trial. Medicina. 2022;58(1):51. https://doi.org/10.3390/medicina58010051.
Bourne KM, Sheldon RS, Hall J, Lloyd M, Kogut K, Sheikh N, et al. Compression garment reduces orthostatic tachycardia and symptoms in patients with postural orthostatic tachycardia syndrome. J Am Coll Cardiol. 2021;77(3):285–96. https://doi.org/10.1016/j.jacc.2020.11.040.
Fu Q, Levine BD. Exercise and non-pharmacological treatment of POTS. Auton Neurosci. 2018;215:20–7. https://doi.org/10.1016/j.autneu.2018.07.001.
Sheldon RS, Grubb BP 2nd, Olshansky B, Shen WK, Calkins H, Brignole M, et al. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015;12(6):e41-63. https://doi.org/10.1016/j.hrthm.2015.03.029.
• Walsh-Messinger J, Manis H, Vrabec A, Sizemore BSJ, Bishof K, Debidda M, et al. The kids are not alright: a preliminary report of Post-COVID syndrome in university students. Journal of American College Health. 2021:1–7. https://doi.org/10.1080/07448481.2021.1927053. (Early report on the impact of long COVID in university students.)
Oskoui M, Pringsheim T, Billinghurst L, Potrebic S, Gersz EM, Gloss D, et al. Practice guideline update summary: pharmacologic treatment for pediatric migraine prevention: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology. 2019;93(11):500–9. https://doi.org/10.1212/wnl.0000000000008105.
Lewis DW, Ashwal S, Dahl G, Dorbad D, Hirtz D, Prensky A, et al. Practice parameter: evaluation of children and adolescents with recurrent headaches: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2002;59(4):490–8. https://doi.org/10.1212/wnl.59.4.490.
Langdon R, DiSabella MT. Pediatric headache: an overview. Curr Probl Pediatr Adolesc Health Care. 2017;47(3):44–65. https://doi.org/10.1016/j.cppeds.2017.01.002.
• Afrin LB, Weinstock LB, Molderings GJ. Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome. Int J Infect Dis. 2020;100:327–32. https://doi.org/10.1016/j.ijid.2020.09.016. (Intriguing hypothesis on the role of mast cell activation in the acute and chronic state post-COVID.)
Afrin LB, Molderings GJ. A concise, practical guide to diagnostic assessment for mast cell activation disease. World Journal of Hematology. 2014;3(1):1–17. https://doi.org/10.5315/wjh.v3.i1.1.
Katz BZ, Shiraishi Y, Mears CJ, Binns HJ, Taylor R. Chronic fatigue syndrome after infectious mononucleosis in adolescents. Pediatrics. 2009;124(1):189–93. https://doi.org/10.1542/peds.2008-1879.
Low PA, Sandroni P, Joyner M, Shen WK. Postural tachycardia syndrome (POTS). J Cardiovasc Electrophysiol. 2009;20(3):352–8. https://doi.org/10.1111/j.1540-8167.2008.01407.x.
Stewart JM, Javaid S, Fialkoff T, Tuma-Marcella B, Visintainer P, Terilli C, et al. Initial orthostatic hypotension causes (transient) postural tachycardia. J Am Coll Cardiol. 2019;74(9):1271–3. https://doi.org/10.1016/j.jacc.2019.06.054.
Freeman R, Wieling W, Axelrod FB, Benditt DG, Benarroch E, Biaggioni I, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69–72. https://doi.org/10.1007/s10286-011-0119-5.
Bou-Holaigah I, Rowe PC, Kan J, Calkins H. The relationship between neurally mediated hypotension and the chronic fatigue syndrome. JAMA. 1995;274(12):961–7. https://doi.org/10.1001/jama.1995.03530120053041.
Adkisson WO, Benditt DG. Pathophysiology of reflex syncope: a review. J Cardiovasc Electrophysiol. 2017;28(9):1088–97. https://doi.org/10.1111/jce.13266.
Benditt DG, Adkisson WO. Approach to the patient with syncope: venues, presentations, diagnoses. Cardiol Clin. 2013;31(1):9–25. https://doi.org/10.1016/j.ccl.2012.09.002.
Grubb BP. Neurocardiogenic syncope. N Engl J Med. 2005;352(10):1004–10. https://doi.org/10.1056/NEJMcp042601.
Roma M, Marden CL, De Wandele I, Francomano CA, Rowe PC. Postural tachycardia syndrome and other forms of orthostatic intolerance in Ehlers-Danlos syndrome. Autonomic Neuroscience: Basic and Clinical. 2018;215:89–96. https://doi.org/10.1016/j.autneu.2018.02.006.
Rowe PC, Marden CL, Flaherty MAK, Jasion SE, Cranston EM, Johns AS, et al. Impaired range of motion of limbs and spine in chronic fatigue syndrome. J Pediatrics. 2014;165(2):360–6. https://doi.org/10.1016/j.jpeds.2014.04.051.
Afrin LB, Ackerley MB, Bluestein LS, Brewer JH, Brook JB, Buchanan AD, et al. Diagnosis of mast cell activation syndrome: a global “consensus-2.” Diagnosis. 2020. https://doi.org/10.1515/dx-2020-0005.
Walker LS, Greene JW. The functional disability inventory: measuring a neglected dimension of child health status. J Pediatr Psychol. 1991;16(1):39–58. https://doi.org/10.1093/jpepsy/16.1.39.
Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800–12. https://doi.org/10.1097/00005650-200108000-00006.
Varni JW, Burwinkle TM, Szer IS. The PedsQL Multidimensional Fatigue Scale in pediatric rheumatology: reliability and validity. J Rheumatol. 2004;31(12):2494–500.
Bentall RP, Wood GC, Marrinan T, Deans C, Edwards RH. A brief mental fatigue questionnaire. Br J Clin Psychol. 1993;32(3):375–9. https://doi.org/10.1111/j.2044-8260.1993.tb01070.x.
White D, Leach C, Sims R, Atkinson M, Cottrell D. Validation of the Hospital Anxiety and Depression Scale for use with adolescents. Br J Psychiatry. 1999;175:452–4. https://doi.org/10.1192/bjp.175.5.452.
Beck AT, Steer RA, Brown GK. Beck depression inventory (BDI-II). Pearson; 1996.
Winker R, Prager W, Haider A, Salameh B, Rüdiger HW. Schellong test in orthostatic dysregulation: a comparison with tilt-table testing. Wien Klin Wochenschr. 2005;117(1–2):36–41. https://doi.org/10.1007/s00508-004-0288-5.
Thijs RD, Brignole M, Falup-Pecurariu C, Fanciulli A, Freeman R, Guaraldi P, et al. Recommendations for tilt table testing and other provocative cardiovascular autonomic tests in conditions that may cause transient loss of consciousness. Clin Auton Res. 2021;31(3):369–84. https://doi.org/10.1007/s10286-020-00738-6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Adolescent Medicine
Supplementary Information
ESM 1
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Morrow, A.K., Malone, L.A., Kokorelis, C. et al. Long-Term COVID 19 Sequelae in Adolescents: the Overlap with Orthostatic Intolerance and ME/CFS. Curr Pediatr Rep 10, 31–44 (2022). https://doi.org/10.1007/s40124-022-00261-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40124-022-00261-4