
Abstract
SCN1A mutations are found in up to 80 % of patients with Dravet syndrome (DS), and the sudden unexpected death in epilepsy (SUDEP) rate is higher in DS than in most forms of severe epilepsy. The aim of this study is to examine the autonomic cardiac function and the risk of arrhythmia in DS patients by evaluating QT and P wave dispersion and heart rate variability (HRV) using standard electrocardiography (ECG) and 24-h ECG. The study group consisted of 15 patients (9 boys and 6 girls aged 3.5–17 years) who were genetically diagnosed with DS. The control group comprised 20 healthy subjects, 13 boys and 7 girls aged 4–17 years. P wave dispersion (44.6 ± 3.5 ms), QT dispersion (58.8 ± 7.5 ms) and QTc dispersion (70.8 ± 7.4 ms) were significantly higher in DS patients as compared to the control group (p < 0.001 for all values). However, there was no significant difference in PR, QT or QTc length between the groups. 24-h Holter ECG showed that all HRV parameters were significantly lower in patients with DS. The decreased HRV and increased P wave and QT dispersion seen in DS patients are important signs of autonomic dysfunction with increased adrenergic tone. To determine whether autonomic dysfunction is correlated with SUDEP in DS, long-term electrocardiographic monitoring and wider prospective studies are necessary.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dravet syndrome (DS) is a severe epileptic encephalopathy that occurs in the first year of life in previously normal infants [1]. SCN1A mutations are found in up to 80 % of patients with DS, and the sudden unexpected death in epilepsy (SUDEP) rate is higher in DS than in most other forms of severe epilepsy [1–3]. The underlying mechanisms of SUDEP are still being debated [4, 5], and possible pathomechanisms that have been suggested are cardiac arrhythmia due to myocardial ischemia, arrhythmogenic drugs, electrolyte disturbances, transmission of epileptic activity to the heart via the autonomic nervous system, and central or obstructive apnea [6].
Because an increasing number of epileptic syndromes are being attributed to ion channel mutations, recent reports have speculated on a pathogenic link between neuronal and cardiac channelopathies that could also explain the high incidence of SUDEP [5, 7, 8]. This theory is further supported by the fact that particularly in animal model studies, products of SCN1A, the neuronal gene responsible for DS in the majority of patients, are also found in the heart and play an important role in sinoatrial node activity [9]. In a study by Delogu et al. [7], DS patients were found to have HRV abnormalities, pointing to a link between cardiac autonomic dysfunction and SUDEP.
Cardiac autonomic dysfunction has been shown to be associated with life-threatening ventricular arrhythmias and is a known risk factor for sudden cardiac death in several cardiac diseases. HRV is an indicator of sympathetic/parasympathetic cardiac autonomic balance, and measuring HRV using Holter ECG is an effective way to evaluate the autonomic nervous system [7, 10]. Decreased HRV values indicate an increased adrenergic tone. In addition to HRV, evaluating QT and P wave dispersion using 12-lead ECG can also be useful in establishing autonomic dysfunction and the risk of arrhythmia. Increased QT dispersion has also been linked to ventricular dysrhythmias that can lead to sudden death [10–13]. However, to the best of our knowledge, P wave and QT dispersion has not been studied in the context of Dravet syndrome.
In this study, we set out to determine whether patients with DS show abnormalities in electrical characteristics of cardiac function (by measuring QT length and dispersion), as well as to study the effect of autonomic nervous activity on sinus node function (by measuring HRV and P wave dispersion).
Patients and methods
Study population
The study group consisted of 15 patients (9 boys and 6 girls aged 3.5–17 years; mean age 8.2 ± 4 years) who were diagnosed with DS (SCN1A gene mutation demonstrated in all patients) at the Pediatric Neurology Department of the Istanbul Medical Faculty. The control group consisted of 20 healthy subjects (13 boys and 7 girls aged 4–17 years; mean age 8.1 ± 3 years). Written consent was obtained from all participant families and the study was carried out in compliance with the Helsinki Declaration standards.
The majority of patients receiving antiepileptic drugs (AED) were taking valproic acid, clobazam and/or topiramate. Most patients were on multiple AED therapy, and one patient was also taking levetiracetam. None of the patients were taking drugs like lamotrigine or carbamazepine that could affect the ECG results.
Cardiac evaluation
All patients and control subjects underwent a standard 12-lead ECG and a 24-h ambulatory Holter ECG, as well as M-mode, 2D and color Dopper echocardiography to eliminate any structural heart disease that could affect the ECG. Ventricular systolic and diastolic function was shown to be normal in all patients and control subjects.
All electrocardiograms were evaluated for rhythm, rate, QRS axis, PR, QRS, and QT and RR intervals, as well as ventricular hypertrophy and repolarization abnormality. The obtained values were compared with normal values according to age [14]. The QT interval was measured on the standard 12-lead ECG, and the corrected QT interval (QTc) was calculated using the Bazzett formula [QTc = QT √(R–R)]. QT dispersion was calculated as the difference between the longest and the shortest QT interval; QTc dispersion was calculated in the same manner. P wave duration was measured over three consecutive cardiac cycles for each lead, and the average of these values was used for analysis. The P maximum was defined as the longest duration among the 12 leads, and the P minimum was defined as the shortest duration. P wave dispersion was calculated as the difference between the maximum and the minimum P wave durations [11].
Heart rate variability was assessed based on Holter ECG recordings. Both time-domain parameters (RR interval, SDNN, SDANN and SDNN index) and frequency-domain parameters (HF and LF amplitude) were obtained. All measurements were performed in accordance with standards established by the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology [15].
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS, Chicago, IL, USA), version 13.0 for Windows. Descriptive statistics was used and all data were expressed as mean ± SD and percentage ratio. Quantitative values were compared using the Mann–Whitney U test and qualitative values were compared using the Chi-square test. The difference was considered to be significant if the p value was below 0.05.
Results
The demographic and clinical characteristics of the patients and control subjects are presented in Table 1. No significant difference was found between the groups in terms of age, sex, height, weight, body mass index, systolic and diastolic blood pressures, or heart rate parameters.
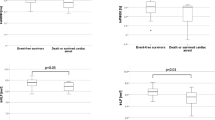
Upon evaluation of the electrocardiograms of patients and control subjects, no abnormality was detected in terms of rhythm, rate, QRS axis, PR and QRS intervals, q, R and S voltage in the precordial leads, and ST and T waves. The PR interval, P wave parameters, QTc length, QT dispersion and QTc dispersion in both groups are shown in Table 2. The maximum duration of P wave, RR interval, and QT and QTc values were similar in the two groups (p > 0.05). In contrast, patients with DS had significantly higher P wave, QT and QTc dispersion than the control group (p < 0.001 for all parameters). Additionally, the minimum P wave duration was significantly shorter in DS patients (p < 0.001). 24-hour Holter electrocardiograms showed that all HRV parameters were significantly lower in DS patients than in control subjects (Table 3).
Discussion
Electrocardiographic features and cardiac autonomic functions in patients with Dravet syndrome are evaluated in this study and the most important results obtained are as follows: all HRV parameters were significantly lower in DS patients and these patients had significantly higher P wave, QT and QTc dispersions.
Compared to the general population, epilepsy patients are more prone to premature death, with sudden unexpected death in epilepsy being the most common cause of seizure-related mortality in refractory epilepsy [4]. SUDEP is known to be an issue in Dravet syndrome patients as well, and the incidence of SUDEP in the pediatric population is probably higher in DS than in other epilepsies [1, 3, 7].
Several high risk factors for SUDEP have recently been proposed after a critical review of medical literature [16]: young age, the male sex, early onset of seizures, generalized tonic–clonic seizures and being bedridden. However, these risk factors are debatable in the context of pediatric studies, where the epilepsy syndrome seems to be the most reliable factor. The highest risk of SUDEP in the pediatric population is associated with infants who have DS-related generalized tonic–clonic seizures and adolescents with idiopathic generalized epilepsy [17]. Sakauchi et al. [3] analyzed 59 death cases out of 623 Dravet syndrome cases (disease-related mortality was 10.1 %), finding that the cause of death in 53 % of cases was SUDEP and that there were no other prognostic factors related to SUDEP besides age (1–3 years, especially).
The underlying mechanisms of SUDEP are still unclear, although both respiratory and cardiac systems are thought to be involved [4, 7]. In a recent review, Nashef et al. [5] suggested that some of the deaths may be due to cardiac arrhythmias. Especially in the recent years, the discovery that some epileptic syndromes previously diagnosed as idiopathic or cryptogenic are linked to sodium and potassium ion channel mutations brings to mind the possible association between sudden death syndromes related to cardiac ion channel disease and epilepsy-related deaths. The so far known SCN5 mutations that can lead to sudden cardiac death (long QT-3 and Brugada syndrome) and other arrhythmogenic diseases have not been shown to have a pathogenic connection with epileptic seizures [5, 7]. However, a study published in 2009 in which approximately half of the patients clinically and genetically diagnosed with long QT2 syndrome had seizures brought the discussion of this connectoin back to agenda [18].
While SCN1A is primarily a neuronal gene, several animal studies have found that Nav1.1, a product of SCN1A, is present in various regions of the heart in rats, mice, rabbit neonates and dogs [19]. For instance, Maier et al. [9] showed that the correct functioning of these channels is necessary for normal sinoatrial node activity and consequently for normal heart rate and HRV control in the mouse heart.
The study by Delogu et al. [7] is the only study that clinically evaluates autonomic dysfunction and sinoatrial node activity in DS patients. In this study, 20 DS patients are compared with other epilepsy patients and healthy control subjects and are shown to have lower HRV, which can reportedly create risk of tachyarrhythmia. No difference in QT and QTc length between groups was found in this study, and QT dispersion was not analyzed [7].
It is well known that increased QT and P wave dispersion can be a sign of autonomic dysfunction and that these two conditions can create risk of atrial and ventricular dysrhythmias [12, 20, 21]. QT dispersion is the difference between the longest and the shortest QT intervals within a 12-lead ECG, and it is helpful for the non-invasive assessment of the heterogeneity of repolarization within the ventricular myocardium [25, 26]. The larger the QTd, the higher is the risk of reentry arrhythmias, and it is not age or gender dependent [26, 27]. In apparently healthy populations, QTd > 50 ms is considered abnormal [27], indicating an increased risk of arrhythmia and sudden death in various disease states including cardiomyopathies, mitral valve prolapse, ischemic heart disease, long QT syndromes and renal failure [12, 13]. Pathologic QT dispersion also seems to predict arrhythmias (mainly premature atrial and ventricular contractions) with electroconvulsive therapy [28]. Therefore, seizure activity in the presence of pathologic QT dispersion could favor the onset of cardiac arrhythmia. P wave dispersion is a measure of heterogeneity in atrial refractoriness and its prolongation shows intraatrial and interatrial non-uniform conduction [11, 20, 22]. In diabetic patients with autonomic neuropathy and in patients with increased sympathetic tone, prolongation of P wave dispersion is considered an indicator of autonomic dysfunction [11, 22, 29]. To summarize, autonomic dysfunction-related increased sympathetic activity can lead to an increase in QT and P wave dispersion, as it leads to decreased HRV on Holter ECG [11, 23, 24].
As is well known, SCN1A mutations are found in up to 80 % of patients with DS, and the SUDEP risk is higher in DS than in most other forms of severe epilepsy [1–3]. In our study, 15 DS patients who all had SCN1A mutation were found to have lower HRV parameters as compared to the control group. We considered this anomaly, which can develop due to excessive sympathetic activity, to be a possible sign of autonomic dysfunction. Further, we found no difference in QT and QTc length between the study group and the control group, while QT and QTc dispersion was increased in the study group. Therefore, it would be reasonable to speculate that SCN1A mutation in DS patients may be linked to subclinical autonomic dysfunction, which can be explained by disruption of cardiac sinoatrial activity or the regulatory center in the brain stem. However, some anti-epileptic drugs can lead to electrocardiographic abnormalities and arrhythmias [5, 13]. Among the antiepileptics, carbamazepine is the drug that is most frequently accused of heart blocks at high doses, but direct relation between carbamazepine and SUDEP was not demonstrated in large studies [3–5]. None of the patients in our study was using carbamazepine. Considering the small number of patients in the study, determining the rare effects of the other antiepileptic drugs on rhythm abnormalities has not been possible.
Characteristics of the seizures and the age of the patients are among the most important parameters in SUDEP related to epileptic conditions. In patients with refractory generalized tonic–clonic seizures and in younger patients with status epilepticus associated with acute encephalopathy, high mortality rate has been demonstrated [3, 30]. On the other hand, sudden death in the majority of DS patients has been reported in febrile children in the early morning [3]. Similar deaths in Brugada syndrome, a cardiac sodium channelopathy, points to SCN1A mutation-associated pathogenesis [31].
One of the most important limitations of our study is the small number of patients. On the other hand, ventricular repolarization abnormalities and increased QT dispersion in refractory epileptic patients had been reported in adult-based studies conducted in recent years [26, 32]. The results of these studies suggest that our findings may not be specific. For this reason, follow-up studies are necessary to assess whether the cardiac autonomic imbalance found in DS patients is connected with the increased rate of SUDEP in DS, which may confirm the possible arrhythmogenic cause of death in a portion of DS patients.
Conclusion
The decreased HRV and increased P wave and QT dispersion in DS patients are important signs of autonomic dysfunction with increased adrenergic tone. In order to determine whether autonomic dysfunction is correlated with SUDEP in DS, long-term electrocardiographic monitoring and wider prospective studies are necessary.
References
Dravet C, Bureau M, Oguni H, Fukuyama Y, Cokar O (2005) Severe myoclonic epilepsy in infancy (Dravet syndrome). In: Roger J, Bureau M, Dravet C, Genton P, Tassinari CA, Wolf P (eds) Epileptic syndromes in infancy, childhood and adolescence, 4th edn. John Libbey, London, pp 77–89
Marini C, Mei D, Temudo T et al (2007) Idiopathic epilepsies with seizures precipitated by fever and SCN1A abnormalities. Epilepsia 48:1678–1685
Sakauchi M, Oguni H, Kato I et al (2011) Mortality in Dravet syndrome: search for risk factors in Japanese patients. Epilepsia 52:50–54
Hitiris N, Suratman S, Kelly K, Stephen LJ, Sills GJ, Brodie MJ (2007) Sudden unexpected death in epilepsy: a search for risk factors. Epilepsy Behav 10:138–141
Nashef L, Hindocha N, Makoff A (2007) Risk factors in sudden death in epilepsy (SUDEP): the quest for mechanisms. Epilepsia 48:859–871
Stöllberger C, Finsterer J (2004) Cardiorespiratory findings in sudden unexplained/unexpected death in epilepsy (SUDEP). Epilepsy Res 59:51–60
Delogu AB, Spinelli A, Battaglia D et al (2011) Electrical and autonomic cardiac function in patients with Dravet syndrome. Epilepsia 52:55–58
Hindocha N, Nashef L, Elmslie F et al (2008) Two cases of sudden unexpected death in epilepsy in a GEFS+ family with an SCN1A mutation. Epilepsia 49:360–365
Maier SK, Westenbroek RE, Yamanushi TT et al (2003) An unexpected requirement for brain-type sodium channels for control of heart rate in the mouse sinoatrial node. Proc Natl Acad Sci USA 100:3507–3512
Kanter RJ (1998) Syncope and sudden death. In: Garson A Jr, Bricker JT, Fisher DJ et al (eds) The science and practice of pediatric cardiology. Williams & Wilkins, Baltimore, pp 2169–2199
Babaoglu K, Altun G, Binnetoğlu K (2011) P-wave dispersion and heart rate variability in children with mitral valve prolapse. Pediatr Cardiol 32:449–454
Higham PD, Campbell RWF (1994) QT dispersion. Br Heart J 71:508–510
Akalin F, Tirtir A, Yilmaz Y (2003) Increased QT dispersion in epileptic children. Acta Paediatr 92:916–920
Davignon A, Rautaharju P, Boiselle E et al (1979) Normal ECG standards for infants and children. Pediatr Cardiol 1:123–131
American College of Cardiology/American Heart Association (1998) ACC/AHA guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients with Valvular Heart Disease). J Am Coll Cardiol 32:1486–1588
Monté CP, Arends JB, Tan IY, Aldenkamp AP, Limburg M, de Krom MC (2007) Sudden unexpected death in epilepsy patients: risk factors. A systematic review. Seizure 16:1–7
Nabbout R (2008) Can SCN1A mutations account for SUDEP? Commentary on Hindocha et al. Epilepsia 49:367–368
Johnson JN, Hofman N, Haglund CM, Cascino GD, Wilde AAM, Ackerman MJ (2009) Identification of a possible pathogenic link between congenital long QT syndrome and epilepsy. Neurology 72:224–231
Lei M, Jones SA, Liu J et al (2004) Requirement of neuronal- and cardiac-type sodium channels for murine sinoatrial node pacemaking. J Physiol 559:835–848
Li Z, Hertervig E, Carlson J, Johansson C, Olsson SB, Yuan S (2002) Dispersion of refractoriness in patients with paroxysmal atrial fibrillation. Evaluation with simultaneous endocardial recordings from both atria. J Electrocardiol 35:227–234
Day CP, McComp LM, Campbell RWF (1990) QT dispersion: an indication of arrhythmia risk in patients with long QT intervals. Br Heart J 63:342–344
Cheema AN, Ahmed MW, Kadish AH, Goldberger JJ (1995) Effects of autonomic stimulation and blockade on signal-averaged P wave duration. J Am Coll Cardiol 26:497–502
Guven B, Eroglu AG, Babaoglu K et al (2008) QT dispersion and diastolic functions in differential diagnosis of primary mitral valve prolapse and rheumatic mitral valve prolapse. Pediatr Cardiol 29:352–358
Malik M, Batchvarov VN (2000) Measurement, interpretation and clinical potential of QT dispersion. J Am Coll Cardiol 36:1749–1766
Engel G, Beckerman JG, Froelicher VF, Yamazaki T, Chen HA, Richardson K, McAuley RJ, Ashley EA, Chun S, Wang PJ (2004) Electrocardiographic arrhythmia risk testing. Curr Probl Cardiol 29:365–432
Surges R, Taggart P, Sander JW, Walker MC (2010) Too long or too short? New insights into abnormal cardiac repolarization in people with chronic epilepsy and its potential role in sudden unexpected death. Epilepsia 51:738–744
Macfarlane PW, McLaughlin SC, Rodger JC (1998) Influence of lead selection and population on automated measurement of QT dispersion. Circulation 98:2160–2167
Rasmussen KG, Hooten WM, Dodd ML, Ryan DA (2007) QTc dispersion on the baseline ECG predicts arrhythmias during electroconvulsive therapy. Acta Cardiol 62:345–347
Köken R, Demir T, Sen TA, Kundak AA, Oztekin O, Alpay F (2010) The relationship between P-wave dispersion and diastolic functions in diabetic children. Cardiol Young 20:133–137
Nashef L, Ryvlin P (2009) Sudden unexpected death in epilepsy (SUDEP): update and reflections. Neurol Clin 27:1063–1074
Junttila MJ, Gonzalez M, Lizotte E, Benito B, Vernooy K, Sarkozy A, Huikuri HV, Brugada P, Brugada J, Brugada R (2008) Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Circulation 117:1890–1893
Surges R, Adjei P, Kallis C, Erhuero J, Scott CA, Bell GS, Sander JW, Walker MC (2010) Pathologic cardiac repolarization in pharmacoresistant epilepsy and its potential role in sudden unexpected death in epilepsy: a case–control study. Epilepsia 51:233–242
Conflicts of interest
The authors report no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ergul, Y., Ekici, B., Tatli, B. et al. QT and P wave dispersion and heart rate variability in patients with Dravet syndrome. Acta Neurol Belg 113, 161–166 (2013). https://doi.org/10.1007/s13760-012-0140-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13760-012-0140-z