
Abstract
Diabetes and its complications have been linked to increased levels of free radicals and systemic pro-inflammatory cytokines and to an altered lipid profile. Coenzyme Q10 and curcumin are potent antioxidants and anti-inflammatory agents but are underutilized clinically because of their poor bioavailability when administered orally. We have recently developed poly(d,l-lactic-co-glycolic acid)-based nanoparticles in which we have encapsulated coenzyme Q10 and curcumin to increase the oral bioavailability and therapeutic efficacy of the antioxidant molecules. These formulations when tested in streptozotocin-induced diabetic rats demonstrated protective effects on inflammatory markers as well as lipid metabolism. Coenzyme Q10 nanoparticulates reduced only C-reactive protein levels, whereas curcumin nanoparticles reduced levels of C-reactive protein, interleukin-6 and tumor necrosis factor-α. Administration of both nanoparticulates resulted in significant reductions of plasma triglycerides and total cholesterol and an increase in high-density lipoprotein cholesterol. Together, these data indicate the promise of coenzyme Q10 and curcumin in diabetes when delivered through nanoparticulate formulations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vascular inflammation and cardiovascular disease are the leading causes of morbidity and mortality in the diabetic population [1]. Oxidative stress has been correlated to inflammatory markers [2] and hyperlipidemia [3], promoting atherosclerosis and subsequent cardiovascular disease. Reactive oxygen species can activate nuclear factor-κB and mediate nuclear factor-κB-dependent mitogenic and cytotoxic signals of cytokines [4]. Levels of the widely recognized inflammatory mediators, tumor necrosis factor α (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP) are known to be elevated in experimental diabetes [5] and in diabetic populations [6]. Antioxidants and antioxidant defense mechanisms, which are inherent in cells and tissues, can inhibit inflammation by intervening in the pathways mediated by reactive oxygen species. However, in diabetic patients the antioxidant defense system weakens due to reduced levels of antioxidants such as glutathione [7]. Glycation of antioxidative enzymes during hyperglycemia impairs cellular antioxidant defense mechanisms, leading to the development of oxidative stress and progression of complications [8]. Antioxidant status has a major role on the rate of low-density lipoprotein (LDL) oxidation and on atherogenicity in humans [9]. Apart from oxidation of LDL, activity of lipoprotein lipase, an enzyme involved in lipid metabolism has been positively correlated with total antioxidant capacity and the atherogenic index has been negatively correlated with this capacity in rats [10].
Coenzyme Q10 (CoQ10) is a strong antioxidant that is an important component in the mitochondrial electron transport chain. CoQ10 is gaining importance in the treatment of cardiovascular diseases, neurodegenerative disorders and diabetes [11]. Although CoQ10 has many applications poor bioavailability as a consequence of poor aqueous solubility and high molecular weight remains a limitation [12]. To improve the oral bioavailability of CoQ10, several new approaches have been considered and tested in animals or humans [13]. Micro- and nanoparticle preparations are the most important approaches being investigated these days to improve bioavailability and many types of micro- and nanoparticles of CoQ10 have been formulated for this purpose [14–16]. The poly(d,l-lactic-co-glycolic acid) (PLGA) nanoparticles, encapsulated with CoQ10, prepared for the present study are biocompatible and biodegradable using the stabilizer didodecyl dimethyl ammonium bromide (DMAB) which gives smaller particles (around 100 nm in diameter).
Curcumin (the active ingredient of the spice turmeric), on the other hand, is a natural plant-derived antioxidant mainly found in the rhizomes of Curcuma longa. Curcumin is also known to possess various pharmacological applications in cardiovascular diseases, neurodegenerative disorders and diabetes. After oral administration, only very low amounts of curcumin reach the systemic circulation; thus curcumin shows poor activity in clinical trials. Clinical development of oral forms of curcumin has been hampered because of its very low bioavailability, which is attributed to its poor solubility, instability and tendency to undergo first-pass metabolism [17]. Curcumin decomposes when exposed to sunlight, in ethanolic and methanolic extracts, in neutral-basic pH conditions, and as a solid [18]. The present study employs curcumin-encapsulated PLGA nanoparticles using poly(vinyl alcohol) (PVA) as the stabilizer, which were previously been reported to improve the oral bioavailability of curcumin [19].
Nanoparticles are being investigated for oral delivery of many challenging molecules that are limited in their use because of their poor biopharmaceutical and pharmacokinetic properties. Entrapment of active ingredients in polymeric nanoparticles results in improved stability [20], uptake [21], and distribution profiles [22]. Nanoparticles, upon oral administration, are believed to be absorbed intact [23] and to circulate for extended periods in the blood releasing the entrapped agent in a sustained fashion, resulting in dose reduction [19]. In our previous studies, CoQ10 nanoparticles showed improved antioxidant and antihyperlipidemic activities over a suspension formulation in experimental diabetes [24], and curcumin nanoparticles showed improved oral bioavailability in normal rats [19]. Based on the advantages of the polymeric nanoparticles, the current research program aims to evaluate the nanoparticulate forms of CoQ10 and curcumin in a rat model of diabetes by measuring the inflammatory markers and lipid levels in the blood.
Materials and methods
Materials
PLGA (Resomer R503H; MW 35–40 kDa) was purchased from Boehringer Ingelheim, (Ingelheim, Germany). PVA (MW 30–70 kDa), DMAB, and ethyl acetate were purchased from Sigma-Aldrich (Poole, UK). High-performance liquid chromatography-grade methanol, ethanol, and acetonitrile were procured from J.T. Baker (now Avantor Performance materials, Phillipsburg, NJ). Curcumin and CoQ10 were gift samples from Indsaff, Punjab, India, and Tishcon Corp., Westbury, NY, respectively.
Preparation of CoQ10 and curcumin nanoparticles
Nanoparticles loaded with CoQ10 or curcumin were prepared by a modified emulsion–diffusion–evaporation method, previously reported [25]. Briefly, CoQ10 (10 mg) or curcumin (7.5 mg) and PLGA (50 mg) were dissolved in 2.5 ml of ethyl acetate and stirred at 1,000 rpm for 30 min under room temperature to obtain a homogeneous solution. Either PVA (50 mg) or DMAB (50 mg), used as a stabilizer, was dissolved in 5 ml distilled water. The organic phase containing the active ingredient and PLGA was then added in a drop-wise manner to the stabilizer solution during homogenization. Homogenization was continued for 5 min at 15,000 rpm. After this step, the emulsion was transferred to 20 ml water to facilitate diffusion and was stirred overnight to ensure the complete evaporation of the organic solvent. After the evaporation step was complete, the nanoparticle solution was centrifuged at 15,000×g for 15 min to separate free active ingredient and any unbound stabilizer in the solution. The supernatant was separated and the pellet was redispersed in 20 ml water. The CoQ10 nanoparticles were stabilized with DMAB and curcumin nanoparticles with PVA.
Size and zeta potential
All nanoparticles were characterized using a Zetasizer Nano ZS (Malvern Instruments, Ltd., Malvern, UK) for size (average of five measurements for one batch) and zeta potential (average of 20 measurements for one batch). The size given by the Zetasizer is the measure of hydrodynamic diameter based on the Brownian motion of the nanoparticles. The average of three batch measurements was expressed as mean ± standard deviation.
Transmission electron microscopy
The morphology of the prepared CoQ10 and curcumin was analyzed using transmission electron microscopy (LEO 912 Omega, Zeiss, Cambridge, UK). Carbon-coated 200-mesh copper grids (Polysciences, Inc., Eppelheim, Germany) were glow discharged, and specimens in distilled water were dried down to a thin layer onto the hydrophilic support film. Next, 20 μl of 1% aqueous methylamine vanadate (NanoVan, Nanoprobes, Yaphank, NY) stain was applied and the mixture dried down immediately with filter paper to remove excess liquid. The dried specimens were imaged with a LEO 912 energy filtering transmission electron microscope at 120 kV. Contrast-enhanced, zero-loss energy-filtered digital images were recorded with a 14-bit/2K charge-coupled device camera (Proscan Electronische Systeme, Germany).
Entrapment efficiency
Entrapment efficiency (EE) of both CoQ10 and curcumin nanoparticles was calculated by measuring the amount of free active agent in the supernatant and subtracting it from the initial amount loaded. EE was determined by centrifuging the nanoparticles loaded with the active ingredient at 15,000×g for 15 min and separating the supernatant. The supernatant was analyzed for free CoQ10 and curcumin. CoQ10 was analyzed using high-performance liquid chromatography. Separation was achieved using a reversed phase C18 column (Hypersil GOLD 15 × 4.6 mm, 5 μm, Thermo Scientific, Loughborough, UK) fitted with a guard column (Hypersil 10 × 4 mm Thermo Scientific, Loughborough, UK). A ratio of 9:1 parts of ethanol and methanol was used as the mobile phase at a flow rate of 1 ml/min with ultraviolet detection at 275 nm. Curcumin was detected using a fluorescence spectrophotometer (Cary Eclipse, Varian Ltd, UK) at an excitation wavelength of 420 nm and emission wavelength of 530 nm. The EE was calculated using the following formula.
Effect of CoQ10 and curcumin nanoparticles in experimental diabetes
Diabetes was induced in male Sprague Dawley rats (250–300 g; n = 6 per group). All animal experiments were performed according to a project license under the Animals (Scientific Procedures) Act 1986 (UK). Upon receiving, all rats were allowed to stabilize for 15 days and were housed under 12-h dark–light cycles with access to food and water ad libitum. Animals were divided into six groups; group I comprised normal animals (NC); animals in groups II–VI were made diabetic by a single intraperitoneal injection of 55 mg/kg streptozotocin (STZ) in 10 mM ice-cold citrate buffer adjusted to pH 4.5. Only the rats with plasma glucose levels >250 mg/dl after 48 h of diabetes induction were considered diabetic and were used in the study. Blood samples were collected by the tail prick method, and glucose levels were estimated using the Accu-Check Aviva Nano® Glucometer (Roche Diagnostics, Mannheim, Germany). From the 16th day of diabetes induction, group II (STZ) diabetic animals received vehicle, group III (STZ+CoN) received 100 mg/kg/day CoQ10 nanoparticles, group IV (STZ+CuN) received 100 mg/kg/day curcumin nanoparticles, group V (STZ+BD) received blank PLGA nanoparticles stabilized with DMAB, and group VI (STZ+BP) received blank PLGA nanoparticles stabilized with PVA. All formulations were given orally using an oral gavage needle. After 31 days from the diabetes induction, animals were sacrificed and blood was collected. Blood samples were centrifuged at 10,000 rpm for 5 min, and plasma was separated and stored at −20°C until further analysis. Evaluation of treatment efficacy was carried out by assaying the plasma levels of inflammatory and lipid markers in the blood samples comprised of IL-6, CRP, TNF-α, triglycerides (TG), total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C). These parameters were estimated using their respective assay kits. Rat TNF-α kits were purchased from Assay Designs (now part of Enzo Life Sciences, Inc., Farmingdale, NY), rat IL-6 assay kits from R&D Systems (Abingdon, UK) and rat CRP assay kits from BD Biosciences Pharmingen (San Diego, CA). TG, TC, and HDL-C quantitation kits were purchased from Source BioScience Autogen (Nottingham, UK). The results were expressed as graphs. Statistical analysis was carried out using one-way analysis of variance followed by comparison of the STZ group to other groups using Holm-Sidak method and Sigma Stat (Systat Software, Inc., San Jose, CA).
Results
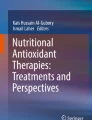
Nanoparticles with encapsulated CoQ10 and curcumin have been prepared successfully using the emulsion diffusion evaporation method. The particle Z-average sizes of CoQ10- and curcumin-encapsulated nanoparticles were 115 ± 12 and 237 ± 6 nm, respectively (Fig. 1). The electron micrographs indicated the spherical shape of all nanoparticles (Fig. 1). The zeta potential values (at pH ∼6) were 75.4 ± 9.5 mV for CoQ10-loaded nanoparticles and −10.8 ± 1.9 mV for curcumin-loaded nanoparticles. The EEs of CoQ10 and curcumin nanoparticles were determined to be 70 ± 3% and 66 ± 3%, respectively, with 20% w/w and 15% w/w initial loading of the polymer PLGA. Both CoQ10 and curcumin nanoparticles were studied using a 100 mg/kg dose of the active ingredient. Based on the initial loading and the EE, the polymer content associated with curcumin was higher than that of CoQ10.

Size distribution (left panel) and transmission electron microscopy images (right panel) of a CoQ10 nanoparticles and b curcumin nanoparticles
At the end of the experimental period, IL-6 and CRP levels in the STZ group were not significantly different from those of the normal group (Figs. 2 and 3). After 1 month, STZ rats were found to have elevated levels of TNF-α (Fig. 4), plasma TG (Fig. 5), and TC (Fig.6) in comparison with the NC rats. HDL-C levels were significantly decreased in the STZ group in comparison to the NC group (Fig. 7).

Plasma interleukin-6 levels. NC non-diabetic negative control, STZ diabetic positive control developed by injecting STZ, STZ+CoN CoQ10 nanoparticle-treated diabetic rats, STZ+CuN curcumin nanoparticle-treated diabetic rats, STZ+BD DMAB stabilized blank nanoparticle-treated diabetic rats, STZ+BP PVA stabilized blank nanoparticle-treated diabetic rats. Values are depicted as mean ± S.E.M. *p < 0.05 vs. STZ group

Plasma C-reactive protein levels. NC non-diabetic negative control, STZ diabetic positive control developed by injecting STZ, STZ+CoN CoQ10 nanoparticle-treated diabetic rats, STZ+CuN curcumin nanoparticle-treated diabetic rats, STZ+BD DMAB stabilized blank nanoparticle-treated diabetic rats, STZ+BP PVA stabilized blank nanoparticle-treated diabetic rats. Values are depicted as mean ± S.E.M. *p < 0.05 vs. STZ group

Plasma TNF-α levels. NC non-diabetic negative control, STZ diabetic positive control developed by injecting STZ, STZ+CoN CoQ10 nanoparticle-treated diabetic rats, STZ+CuN curcumin nanoparticle-treated diabetic rats, STZ+BD DMAB stabilized blank nanoparticle-treated diabetic rats, STZ+BP PVA stabilized blank nanoparticle-treated diabetic rats. Values are depicted as mean ± S.E.M. *p < 0.05 vs. STZ group

Plasma triglyceride levels. NC non-diabetic negative control, STZ diabetic positive control developed by injecting STZ, STZ+CoN CoQ10 nanoparticle-treated diabetic rats, STZ+CuN curcumin nanoparticle-treated diabetic rats, STZ+BD DMAB stabilized blank nanoparticle-treated diabetic rats, STZ+BP PVA stabilized blank nanoparticle-treated diabetic rats. Values are depicted as mean ± S.E.M. *p < 0.05 vs. STZ group

Plasma cholesterol levels. NC non-diabetic negative control, STZ diabetic positive control developed by injecting STZ, STZ+CoN CoQ10 nanoparticle-treated diabetic rats, STZ+CuN curcumin nanoparticle-treated diabetic rats, STZ+BD DMAB stabilized blank nanoparticle-treated diabetic rats, STZ+BP PVA stabilized blank nanoparticle-treated diabetic rats. Values are depicted as mean ± S.E.M. *p < 0.05 vs. STZ group

Plasma HDL levels. NC non-diabetic negative control, STZ diabetic positive control developed by injecting STZ, STZ+CoN CoQ10 nanoparticle-treated diabetic rats, STZ+CuN curcumin nanoparticle-treated diabetic rats, STZ+BD DMAB stabilized blank nanoparticle-treated diabetic rats, STZ+BP PVA stabilized blank nanoparticle-treated diabetic rats. Values are depicted as mean ± S.E.M. *p < 0.05 vs. STZ group
Although IL-6 and CRP levels were not significantly raised in the STZ group in comparison with the normal group, CRP levels were significantly lower in the STZ+CoN group, and both IL-6 and CRP levels were lower in STZ+CuN group compared with the STZ group (Figs. 2 and 3). TNF-α levels were significantly lower in the STZ+CuN group (but not the STZ+CoN group) in comparison with the STZ rats at the end of the study (Fig. 4). After 15 days of treatment with CoQ10 and curcumin nanoparticles, plasma TG and TC levels were reduced significantly in the STZ+CoN and STZ+CuN groups, in comparison with the STZ group (Figs. 5 and 6). Plasma HDL-C levels were significantly higher in the STZ+CoN and STZ+CuN groups in comparison with the STZ group (Fig. 7). Diabetic rats treated with blank nanoparticles, stabilized with either DMAB (STZ+BD group) or PVA (STZ+BP group), showed similar levels as the diabetic control (STZ) showing no effect of the blank nanoparticles on all the measured parameters (Figs. 2, 3, 4, 5, 6, and 7).
Discussion
Coenzyme Q10- and curcumin-loaded nanoparticles
The present study illustrates the use of a novel delivery strategy using polymer nanoparticles for peroral administration of CoQ10 and curcumin, which otherwise are poorly bioavailable [26, 27]. Owing to this shortcoming, these compounds were tested by a non-oral route of administration [26, 28]; however, the oral route is preferred for such compounds until therapeutic efficacy and doses are established. The simplest approach is to use oil-based formulations of CoQ10 and curcumin [13, 27]; these result in only slight increases in bioavailability [12], but show better efficacy than suspension formulations. Although the nanoparticle approach is not new for delivering drugs, it is new for antioxidants and is slowly gaining importance. Polymer nanoparticles offered enhanced uptake of CoQ10 in comparison to the solubilized form of a commercial CoQ10 formulation in studies of in situ uptake in rodents [14]. Curcumin nanoparticles showed a ninefold increase in bioavailability compared with curcumin plus the absorption enhancer piperine [19]. Together, these results paved the way for evaluating these formulations in a disease model.
The smaller size of the CoQ10 nanoparticles in comparison to curcumin nanoparticles can be attributed to the characteristics of the stabilizers used (Fig. 1). DMAB was found to be superior to PVA in minimizing interfacial tension [29]. However, not all compounds are compatible with DMAB; in the case of curcumin, it was not possible to formulate the particles with DMAB because of the precipitation of curcumin during the nanoparticle preparation process in the presence of DMAB. Nanoparticles with curcumin loading more than 15% w/w resulted in larger size distributions of the nanoparticles because of the limited solubility of curcumin in ethyl acetate, which is used as the organic phase in the nanoparticle preparation process. Other researchers have also encountered similar problem when initial loading of curcumin more than 17% w/w was attempted while preparing curcumin-loaded poly (ε-caprolactone) nanofibers [30]. The differences in EEs of CoQ10 and curcumin nanoparticles can be attributed to the properties of the stabilizers used and the antioxidant physicochemical properties per se. CoQ10 is highly soluble, but curcumin has limited solubility in ethyl acetate.
The stabilizer is believed to form a coat around the particle [31] and thus to exert a major effect on the surface charge. The zeta potential of CoQ10 nanoparticles was positive and that of curcumin nanoparticles was negative, depending on the stabilizer’s characteristics. Owing to its cationic nature, DMAB gives a high positive charge to the nanoparticles [32]. PVA, on the other hand, is a polymer without any charge and gives the nanoparticles a slight negative charge.
Protective effects of CoQ10 and curcumin nanoparticles in experimental diabetes
Oxidative stress is correlated to the increase in inflammation and dyslipidemia in humans [2, 3]. Increased oxidative stress is also associated with the increased oxidation of LDL in humans [9]. Together, oxidative stress, inflammation and dyslipidemia work in a complex way to foster the rapid development of atherosclerosis leading to cardiovascular disease in diabetes. The variable increase in inflammatory markers in diabetic rats is perhaps due to the short duration of the present study (i.e., 4 weeks); however, with longer durations (7 weeks or more) after diabetes induction, IL-6 and CRP levels also increase significantly in experimental diabetes [5, 27]. The development of diabetes in humans is more closely mimicked by rodent models using feeding of high-fat diet and injection of a low dose STZ. The use of a rodent model developed this way can be an effective tool in pharmacological screening of therapeutic agents [33, 34].
CoQ10 showed anti-inflammatory activity only in terms of CRP, although these levels were not elevated significantly in diabetic rats (Fig. 3). CoQ10 has been shown to possess anti-inflammatory activity in other disease models with systemic inflammation, for example it lowered elevated CRP levels in a model of hypertensive rats developing metabolic syndrome [35] and in a mouse model of diet-induced obesity [36]. IL-6 and TNF-α levels were slightly reduced with CoQ10 nanoparticle treatment; however, these levels were not significantly different from those of untreated diabetic rats (Fig. 4), which was also the case with the supplementation of CoQ10 in humans [37]. The anti-inflammatory effect of CoQ10 was shown to be independent of its activity on lipid peroxidation in obese mice [36].
Our results are in agreement with reports in the literature in which curcumin has shown its strong anti-inflammatory effects against TNF-α and IL-6 release in a diabetic rat model as well as in cultured monocytes subjected to high levels of glucose [27]. The inhibitory effect of curcumin on TNF-α and IL-6 release was found to be dose dependent in cell cultures. The studies conducted in diabetic animals employed a similar dose of curcumin as in our study (100 mg/kg). It was proposed that the anti-inflammatory effects of curcumin can be mediated through both oxidative stress-dependent (through generation of reactive oxygen species) and independent pathways (through induction of GSH) [38, 39].
In the present study, CoQ10- or curcumin-encapsulated nanoparticles showed statistically significant reductions in plasma TG and TC levels and increased the HDL-C levels in diabetic rats (Figs. 5, 6, and 7). We recently developed co-encapsulated antioxidant nanoparticles that use CoQ10 and ellagic acid together for synergistic effects and the evaluation involved the measurement of lipid peroxidation, plasma insulin, glucose, and TG levels in diabetic rats [24]. CoQ10 alone nanoparticle-treated group in that study, which was used as control, showed decreases in TG and TC [24]. In humans 150 mg/kg CoQ10 in combination with fenofibrate increased the effect of fenofibrate in lowering the massive hypertriglyceridemia [40]. The lipid-lowering effects of CoQ10 can be attributed to its direct effect on mitochondria to increase fatty acid oxidation, an antioxidant effect that could decrease oxidative stress, and/or a direct vascular effect that might have led to increased lipolysis of TG-rich lipoproteins [26, 40]. The literature supports the notion that curcumin is effective against hyperlipidemia developed in the STZ-induced diabetic rats [41] and in hamsters fed a high-fat diet [42]. The hypolipidemic action of dietary curcumin is believed to be mediated by the increase in activity of hepatic cholesterol-7a-hydroxylase suggesting a higher rate of cholesterol catabolism [41]. Blank nanoparticles were used as controls in the present study and showed similar results to that of the STZ group in all the parameters studied, suggesting that the polymer PLGA and stabilizers DMAB and PVA had no significant effect on any of the parameters studied.
Conclusion
This study describes the protective effects of nanoparticulate coenzyme Q10 and curcumin on inflammatory markers and lipid metabolism, which can be beneficial in diabetic conditions. Curcumin nanoparticles were effective on all the inflammatory markers studied, such as CRP, IL-6, and TNF-α, whereas CoQ10 nanoparticles reduced only CRP levels. Plasma TG, TC, and HDL-C were normalized by both CoQ10 and curcumin nanoparticles.
References
Frankel DS, Wilson PWF, Meigs JB. Diabetes mellitus and cardiovascular disease. In: Grundy SM, editor. Atlas of atherosclerosis and metabolic syndrome. New York: Springer; 2011. p. 227–52.
Dohi Y, Takase H, Sato K, Ueda R. Association among C-reactive protein, oxidative stress, and traditional risk factors in healthy Japanese subjects. Int J Cardiol. 2007;115:63–6.
Kostapanos MS, Spyrou AT, Tellis CC, Gazi IF, Tselepis AD, Elisaf M, et al. Ezetimibe treatment lowers indicators of oxidative stress in hypercholesterolemic subjects with high oxidative stress. Lipids. 2011;46:341–8.
Gloire G, Legrand-Poels S, Piette J. NF-kB activation by reactive oxygen species: fifteen years later. Biochem Pharmacol. 2006;72:1493–505.
Lu L, Zhang Q, Pu LJ, Xu XW, Zhang RY, Zhang JS, et al. Elevation of tumor necrosis factor-α, interleukin-1β and interleukin-6 levels in aortic intima of Chinese Guizhou minipigs with streptozotocin-induced diabetes. Chin Med J (Engl). 2007;120:479–84.
King DE, Mainous III AG, Buchanan TA, Pearson WS. C-reactive protein and glycemic control in adults with diabetes. Diabetes Care. 2003;26:1535–9.
Sekhar RV, McKay SV, Patel SG, Guthikonda AP, Reddy VT, Balasubramanyam A, et al. Glutathione synthesis is diminished in patients with uncontrolled diabetes and restored by dietary supplementation with cysteine and glycine. Diabetes Care. 2011;34:162–7.
Kang JH. Modification and inactivation of human Cu, Zn-superoxide dismutase by methylglyoxal. Mol Cells. 2003;15:194–9.
Yang RL, Shi YH, Hao G, Li W, Le GW. Increasing oxidative stress with progressive hyperlipidemia in human: relation between malondialdehyde and atherogenic index. J Clin Biochem Nutr. 2008;43:154–8.
Yang R, Le G, Li A, Zheng J, Shi Y. Effect of antioxidant capacity on blood lipid metabolism and lipoprotein lipase activity of rats fed a high-fat diet. Nutrition. 2006;22:1185–91.
Bank G, Kagan D, Madhavi D. Coenzyme Q10: clinical update and bioavailability. J Evid Based Complement Altern Med. 2011;16:129–37.
Bhagavan HN, Chopra RK. Plasma coenzyme Q10 response to oral ingestion of coenzyme Q10 formulations. Mitochondrion. 2007;7(Suppl):S78–88.
Žmitek J, Žmitek K, Pravst I. Improving the bioavailability of CoQ10, from theory to practice. Agro Food Ind Hi Tech. 2008;19:4–9.
Ankola DD, Viswanad B, Bhardwaj V, Ramarao P, Kumar MN. Development of potent oral nanoparticulate formulation of coenzyme Q10 for treatment of hypertension, can the simple nutritional supplements be used as first line therapeutic agents for prophylaxis/therapy? Eur J Pharm Biopharm. 2007;67:361–9.
Hsu CH, Cui Z, Mumper RJ, Jay M. Preparation and characterization of novel coenzyme Q10 nanoparticles engineered from microemulsion precursors. AAPS Pharm Sci Tech. 2003;4:E32.
Hu X, Guo Y, Wang L, Hua D, Hong Y, Li J. Coenzyme Q10 nanoparticles prepared by a supercritical fluid-based method. J Supercrit Fluids. 2011;57:66–72.
Garcea G, Jones DJ, Singh R, Dennison AR, Farmer PB, Sharma RA, et al. Detection of curcumin and its metabolites in hepatic tissue and portal blood of patients following oral administration. Br J Cancer. 2004;90:1011–5.
Wang YJ, Pan MH, Cheng AL, Lin LI, Ho YS, Hsieh CY, et al. Stability of curcumin in buffer solutions and characterization of its degradation products. J Pharm Biomed Anal. 1997;15:1867–76.
Shaikh J, Ankola DD, Beniwal V, Singh D, Kumar MN. Nanoparticle encapsulation improves oral bioavailability of curcumin by at least 9 fold when compared to curcumin administered with piperine as absorption enhancer. Eur J Pharm Sci. 2009;37:223–30.
Kwon SS, Nam YS, Lee JS, Ku BS, Han SH, Lee JY, et al. Preparation and characterization of coenzyme Q10-loaded PMMA nanoparticles by a new emulsification process based on microfluidization. Colloids Surf A Physicochem Eng Asp. 2002;210:95–104.
Bala I, Bhardwaj V, Hariharan S, Kharade SV, Roy N, Kumar MN. Sustained release nanoparticulate formulation containing antioxidant-ellagic acid as potential prophylaxis system for oral administration. J Drug Target. 2006;14:27–34.
Mittal G, Sahana DK, Bhardwaj V, Kumar MN. Estradiol loaded PLGA nanoparticles for oral administration: effect of polymer molecular weight and copolymer composition on release behavior in vitro and in vivo. J Control Release. 2007;119:77–85.
Hussain N, Jaitley V, Florence AT. Recent advances in the understanding of uptake of microparticulates across the gastrointestinal lymphatics. Adv Drug Deliv Rev. 2001;50:107–42.
Ratnam DV, Chandraiah G, Sonaje K, Viswanad B, Bhardwaj V, Ramarao P, et al. A potential therapeutic strategy for diabetes and its complications in the form of co-encapsulated antioxidant nanoparticles (NanoCAPs) of ellagic acid and coenzyme Q10: preparation and evaluation in streptozotocin induced diabetic rats. J Biomed Nanotechnol. 2008;4:33–43.
Hariharan S, Bhardwaj V, Bala I, Sitterberg J, Bakowsky U, Kumar MN. Design of estradiol loaded PLGA nanoparticulate formulations: a potential oral delivery system for hormone therapy. Pharm Res. 2006;23:184–95.
Modi KP, Vishwakarma SL, Goyal RK, Bhatt PA. Effects of coenzyme Q10 on lipid levels and antioxidant defenses in rats with fructose induced hyperlipidemia and hyperinsulinaemia. Internet J Pharmacol. 2007;5:1 [Accessed online September 16, 2011: http://www.ispub.com/journal/the_internet_journal_of_pharmacology/volume_5_number_1_30/article/effects_of_coenzyme_q10_on_lipid_levels_and_antioxidant_defenses_in_rats_with_fructose_induced_hyperlipidemia_and_hyperinsulinaemia.html].
Jain SK, Rains J, Croad J, Larson B, Jones K. Curcumin supplementation lowers TNF-alpha, IL-6, IL-8, and MCP-1 secretion in high glucose-treated cultured monocytes and blood levels of TNF-alpha, IL-6, MCP-1, glucose, and glycosylated hemoglobin in diabetic rats. Antioxid Redox Signal. 2009;11:241–9.
Kanitkar M, Gokhale K, Galande S, Bhonde RR. Novel role of curcumin in the prevention of cytokine-induced islet death in vitro and diabetogenesis in vivo. Br J Pharmacol. 2008;155:702–13.
Sonaje K, Italia JL, Sharma G, Bhardwaj V, Tikoo K, Kumar MN. Development of biodegradable nanoparticles for oral delivery of ellagic acid and evaluation of their antioxidant efficacy against cyclosporine A-induced nephrotoxicity in rats. Pharm Res. 2007;24:899–908.
Merrell JG, McLaughlin SW, Tie L, Laurencin CT, Chen AF, Nair LS. Curcumin-loaded poly(epsilon-caprolactone) nanofibres: diabetic wound dressing with anti-oxidant and anti-inflammatory properties. Clin Exp Pharmacol Physiol. 2009;36:1149–56.
Sahoo SK, Panyam J, Prabha S, Labhasetwar V. Residual polyvinyl alcohol associated with poly (DL-lactide-co-glycolide) nanoparticles affects their physical properties and cellular uptake. J Control Release. 2002;82:105–14.
Bhardwaj V, Ankola DD, Gupta SC, Schneider M, Lehr CM, Kumar MN. PLGA nanoparticles stabilized with cationic surfactant: safety studies and application in oral delivery of paclitaxel to treat chemical-induced breast cancer in rat. Pharm Res. 2009;26:2495–503.
Srinivasan K, Viswanad B, Asrat L, Kaul CL, Ramarao P. Combination of high-fat diet-fed and low-dose streptozotocin-treated rat: a model for type 2 diabetes and pharmacological screening. Pharmacol Res. 2005;52:313–20.
Zhang M, Lv XY, Li J, Xu ZG, Chen L. The characterization of high-fat diet and multiple low-dose streptozotocin induced type 2 diabetes rat model. Exp Diabetes Res. 2008;2008:704045.
Kunitomo M, Yamaguchi Y, Kagota S, Otsubo K. Beneficial effect of coenzyme Q10 on increased oxidative and nitrative stress and inflammation and individual metabolic components developing in a rat model of metabolic syndrome. J Pharmacol Sci. 2008;107:128–37.
Sohet FM, Neyrinck AM, Pachikian BD, de Backer FC, Bindels LB, Niklowitz P, et al. Coenzyme Q10 supplementation lowers hepatic oxidative stress and inflammation associated with diet-induced obesity in mice. Biochem Pharmacol. 2009;78:1391–400.
Gökbel H, Gergerlioğlu HS, Okudan N, Gül I, Büyükbaş S, Belviranli M. Effects of coenzyme Q10 supplementation on plasma adiponectin, interleukin-6, and tumor necrosis factor-alpha levels in men. J Med Food. 2010;13:216–8.
Kowluru RA, Kanwar M. Effects of curcumin on retinal oxidative stress and inflammation in diabetes. Nutr Metab (Lond). 2007;4:8.
Sandur SK, Pandey MK, Sung B, Ahn KS, Murakami A, Sethi G, et al. Curcumin, demethoxycurcumin, bisdemethoxycurcumin, tetrahydrocurcumin and turmerones differentially regulate anti-inflammatory and antiproliferative responses through a ROS-independent mechanism. Carcinogenesis. 2007;28:1765–73.
Cicero AF, Derosa G, Miconi A, Laghi L, Nascetti S, Gaddi A. Possible role of ubiquinone in the treatment of massive hypertriglyceridemia resistant to PUFA and fibrates. Biomed Pharmacother. 2005;59:312–7.
Babu PS, Srinivasan K. Hypolipidemic action of curcumin, the active principle of turmeric (Curcuma longa) in streptozotocin induced diabetic rats. Mol Cell Biochem. 1997;166:169–75.
Jang E-M, Choi M-S, Jung UJ, Kim M-J, Kim H-J, Jeon S-M, et al. Beneficial effects of curcumin on hyperlipidemia and insulin resistance in high-fat-fed hamsters. Metabolism. 2008;57:1576–83.
Acknowledgments
Venkat Ratnam Devadasu acknowledges PhD fellowship from the Faculty of Science, University of Strathclyde. The authors are thankful to Tishcon Corporation, Westbury, NY, and Indsaff, Ltd., Punjab, India, for providing gratis samples of CoQ10 and curcumin, respectively.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Devadasu, V.R., Wadsworth, R.M. & Kumar, M.N.V.R. Protective effects of nanoparticulate coenzyme Q10 and curcumin on inflammatory markers and lipid metabolism in streptozotocin-induced diabetic rats: a possible remedy to diabetic complications. Drug Deliv. and Transl. Res. 1, 448–455 (2011). https://doi.org/10.1007/s13346-011-0041-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13346-011-0041-3