
Abstract
Our recent work demonstrated that circulating levels of IgG antibody to linear peptide antigens derived from annexin A1 (ANXA1) were significantly increased in lung cancer. The present study was then undertaken to test whether circulating anti-ANXA1 antibodies were also altered in breast cancer. An enzyme-linked immunosorbent assay was developed in-house to determine circulating IgG against ANXA1-derived peptide antigens in 152 female patients with breast cancer and 160 female control subjects. Student’s t test revealed that patients with breast cancer had significantly higher levels of anti-ANXA1 IgG than control subjects (t = 4.75, P < 0.0001). Receiver operating characteristic (ROC) analysis showed that the area under the ROC curve was 0.73 with 95 % confidence interval (CI) 0.67–0.78, and the sensitivity of anti-ANXA1 IgG assay was 23.2 % against the specificity of 90 %. The levels of anti-ANXA1 IgG did not appear to be stage-dependent, and Pearson correlation analysis showed no correlation between the anti-ANXA1 IgG levels and the stages of breast cancer (r = −0.02, df = 149, P = 0.796). This work suggests that circulating IgG for ANXA1-derived peptide antigens may have both diagnostic and prognostic values for breast cancer although further screening is needed to identify more such peptide antigens derived from tumor-associated antigens.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common malignancy in female people and often develops through sequential stages from normal ductal epithelium to ductal carcinoma in situ (DCIS), invasive cancer, and metastatic carcinoma. It is the second leading cause of cancer mortality among women [1]. With the advent of modern technologies such as mammography for screening early-stage breast cancer, the death rates of breast cancer have been declining in most Western countries over the past few decades [2]. However, not all cancers can be visualized on mammographic screening, and the sensitivity of mammography has been very low (<50 %) in women with extremely dense breasts [3]. It is thus particularly important to develop a more powerful diagnostic tool for early diagnosis of breast cancer.
The secretion of circulating antibodies to tumor-associated antigens (TAAs) has been reported in a large body of publications [4–10]. While a range of anti-TAA antibodies have been identified in breast cancer [9, 10], the sensitivity of serological antibody test with a single antigen is too low for clinical application so that a panel of antigens are needed to develop a powerful test like the EarlyCDT®-Lung test that was the first autoantibody-based diagnostic tool in lung cancer [7, 8, 11]. Annexin-1 (ANXA1) is known to be involved in the initiation of breast cancer [12, 13]. In a recent study, we found that circulating levels of IgG antibodies to ANXA1 were significantly increased in lung cancer [14]. The present work was therefore undertaken to investigate whether circulating IgG antibodies to ANXA1 was also altered in breast cancer.
Materials and methods
Subjects
A total of 152 patients aged 50.1 ± 9.1 years, who were newly diagnosed as having breast cancer, were recruited for this study by the Third Affiliated Hospital of Harbin Medical University, Harbin, China. Of these 152 patients, 126 suffered from ductal carcinoma (DC) and 26 from lobular carcinoma (LC). Their diagnoses were made based on mammographic examination and histological confirmation with staging information. Blood samples were taken prior to any anticancer treatment. One hundred sixty healthy subjects aged 50.9 ± 5.5 years were also recruited as controls. Clinical interview and radiographic examination were applied to rule out the control subjects who had history of breast cancer or any other malignant tumors. All the subjects were of Chinese Han origin, and all gave written informed consent to participate in this study. This work was approved by the Ethics Committee of Jilin University and conformed to the requirements of the Declaration of Helsinki.
Autoantibody testing
Enzyme-linked immunosorbent assay (ELISA) was developed in-house using a linear peptide antigen derived from human ANXA1 protein (NCBI accession NP_000691), H-FNTILTTRSYPQLRRVFQKYTLIRIMVSRSEID-OH, to detect circulating IgG to ANXA1; a peptide fragment derived from recombinant goat alpha-lactalbumin T29i (NCBI accession 1FKV_A), H-VFQKLKDLKDYGGVSLPEWVKIAFHTSG-OH, was used as the control antigen. Briefly, synthetic peptides were dissolved in 67 % acetic acid to obtain a concentration of 5 mg/ml as stock solution. The antigens were diluted into a working solution just before use with phosphate-buffered saline (PBS), pH 7.4, containing 0.1 % sodium azide. Coaster 96-well microtiter EIA plates (ImmunoChemistry Technologies, USA) were half-coated in 0.1 ml/well of the ANXA1-derived peptide antigen (1 μg/well) and half-coated in 0.1 ml/well of the control antigen (2 μg/well) as described in our previous study [14]. After overnight incubation at 4 °C, the antigen-coated microplate was washed three times with PBS containing 0.05 % Tween-20 (PBS-T), 100 μl plasma sample diluted 1:200 in Assay Buffer (DS98200, Life Technologies) was then added to the sample wells, and 100 μl Assay Buffer was added to the negative control (NC) wells. Following 3 h incubation at room temperature, the plate was washed three times with PBS-T and 100 μl peroxidase-conjugated goat anti-human IgG antibodies (A8667, Sigma-Aldrich) diluted 1:30000 in Assay Buffer was added to each well. After incubation at room temperature for 2 h, color development was initiated by adding 100 μl Stabilized Chromogen (SB02, Life Technologies) and terminated 25 min later by adding 50 μl Stop Solution (SS04, Life Technologies). The measurement of optical density (OD) was completed on a microplate reader (BioTeck, USA) within 10 min at 450 nm with a reference wavelength of 620 nm.
Each sample was tested in duplicate. To reduce the interference from a nonspecific signal produced by passive absorption of various antibodies in plasma to the surface of 96-well microplate, a specific binding index (SBI) was used to express the levels of circulating antibodies to ANXA1. SBI was calculated as follows:
To minimize the intra-assay deviation, the ratio of the difference between duplicated OD values to their sum was used to assess the precision for assay of each sample. If the ratio was >10 % then the test of this sample was treated as being invalid and would not be used for data analysis.
Data analysis
The mean ± SD in SBI was used to present data. Student’s t test was performed to examine the difference in SBI between the patient group and the control group; Pearson correlation analysis was performed to examine the correlation between circulating IgG levels and the stages of breast cancer. Receiver operating characteristic (ROC) analysis was applied to work out the area under the ROC curve (AUC) with calculation of 95 % confidence interval (CI) and ELISA sensitivity against a specificity of 90 %.
Results
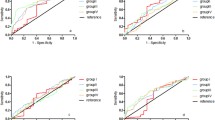
As shown in Table 1, patients with breast cancer had significant higher levels of circulating IgG to ANXA1 than control subjects (t = 4.75, P < 0.0001), and both DC and LC appeared to contribute to the increased levels of anti-ANXA1 IgG antibodies in the circulation (Table 1). The levels of anti-ANXA1 IgG did not show stage-dependence (Table 2); as shown in Fig. 1, Pearson correlation analysis demonstrated no significant correlation between the anti-ANXA1 IgG levels and the stages of breast cancer (r = −0.02, df = 149, P = 0.796).

Correlation between the stages of breast cancer and the anti-ANXA1 IgG levels. r = −0.02, df = 149, P = 0.796
As shown in Table 3, ROC analysis showed an AUC of 0.73 with 95 % CI 0.67–0.78 for anti-ANXA1 IgG, and the sensitivity of ELISA antibody test was 23.2 % against the specificity of 90 %.
Discussion
The present work confirmed that circulating levels of IgG antibodies for ANXA1-derived peptide antigens were significantly increased in breast cancer although the sensitivity of antibody test was rather low (Table 3). Apparently, a panel of antigens is needed to develop a highly sensitive test for clinical diagnosis. A number of studies have identified a range of anti-TAA antibodies in breast cancer, including those for p53, MUC1, HSP27, HSP60, HSP90, HER2, MYC, MYB, NY-ESO-1, BRCA1, BRCA2, GIPC1, endostain, lipophilin B, cyclin D1, fibulin, IGFBP2, TOPO2α, cathepsin D, and CD25 [5, 6, 9, 10, 15]. These autoantibodies have promised the diagnostic potential for the malignant disease.
ANXA1 is a member of the calcium-dependent phospholipid-binding protein family and has a critical role in cellular and immunological responses [12, 13, 16]. It is a candidate regulator of oncogene-induced cell morphology switch, such as the epithelial-mesenchymal transition (EMT) phenotypic switch [17]. Such a switch enables tumor cells to increase their mobility and invasiveness, leading to metastasis and progression [18]. What mechanism underlies the elevation of IgG antibodies for ANXA1 remains unknown, but the change of ANXA1 expression varies in different subtypes of breast cancer. For example, high ANXA1 expression is associated with the basal-like breast cancer (BLBC) subtype in a panel of breast cancer cell lines, while the loss of ANXA1 expression is associated with invasive carcinoma [19]. It is possible that increased anti-ANXA1 antibodies could inhibit the activity of ANXA1 and facilitate invasiveness of breast cancer. This may be the reason why increased anti-ANXA1 IgG levels were observed in all four stages of breast cancer in this study (Tables 2 and 3). If this was a case, circulating anti-ANXA1 IgG could have both diagnostic and prognostic values for breast cancer.
References
DeSantis C, Siegel R, Bandi P, Jemal A. Breast cancer statistics, 2011. CA Cancer J Clin. 2011;61:409–18.
Autier P, Boniol M, La Vecchia C, Vatten L, Gavin A, Hery C, et al. Disparities in breast cancer mortality trends between 30 European countries: retrospective trend analysis of WHO mortality database. BMJ. 2010;341:c3620. doi:10.1136/bmj.c3620.
Mandelson MT, Oestreicher N, Porter PL, White D, Finder CA, Taplin SH, et al. Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancer. J Natl Cancer Inst. 2000;92:1081–7.
Tan HT, Low J, Lim SG, Chung MC. Serum autoantibodies as biomarkers for early cancer detection. FEBS J. 2009;276:6880–904.
Piura E, Piura B. Autoantibodies to tumor-associated antigens in breast carcinoma. J Oncol. 2010;2010:264926. doi:10.1155/2010/264926.
Piura E, Piura B. Autoantibodies to tailor-made panels of tumor-associated antigens in breast carcinoma. J Oncol. 2011;2011:982425. doi:10.1155.2011/982425.
Lam S, Boyle P, Healey GF, Maddison P, Peek L, Murray A, et al. EarlyCDT-Lung: an immunobiomarker test as an aid to early detection of lung cancer. Cancer Prev Res (Phila). 2011;4:1126–34.
Chapman CJ, Healey GF, Murray A, Boyle P, Robertson C, Peek LJ, et al. EarlyCDT®-Lung test: improved clinical utility through additional autoantibody assays. Tumour Biol. 2012;33:1319–26.
Ye H, Sun C, Ren P, Dai L, Peng B, Wang K, et al. Mini-array of multiple tumor-associated antigens (TAAs) in the immunodiagnosis of breast cancer. Oncol Lett. 2013;5:663–8.
Lacombe J, Mangé A, Solassol J. Use of autoantibodies to detect the onset of breast cancer. J Immunol Res. 2014;2014:574981. doi:10.1155/2014/574981.
Jett JR, Peek LJ, Fredericks L, Jewell W, Pingleton WW, Robertson JF. Audit of the autoantibody test, EarlyCDT®-lung, in 1600 patients: an evaluation of its performance in routine clinical practice. Lung Cancer. 2014;83:51–5.
Swa HL, Blackstock WP, Lim LH, Gunaratne J. Quantitative proteomics profiling of murine mammary gland cells unravels impact of annexin-1 on DNA damage response, cell adhesion, and migration. Mol Cell Proteomics. 2012;11:381–93.
Swa HL, Shaik AA, Lim LH, Gunaratne J. Mass spectrometry based quantitative proteomics and integrative network analysis accentuates modulating roles of annexin-1 in mammary tumorigenesis. Proteomics. 2014; [Epub ahead of print].
Wang W, Guan S, Sun S, Jin Y, Lee K-H, Chen Y, et al. Detection of circulating antibodies to linear peptide antigens derived from ANXA1 and DDX53 in lung cancer. Tumour Biol. 2014;35:4901–5.
Liu T, Song YN, Shi QY, Liu Y, Bai XN, Pang D. Study of circulating antibodies against CD25 and FOXP3 in breast cancer. Tumour Biol. 2014;35:3779–83.
Araujo TG, Marangoni K, Rocha RM, Maia YC, Araujo GR, Alcântar TM, et al. Dynamic dialog between cytokeratin 18 and annexin A1 in breast cancer: a transcriptional disequilibrium. Acta Histochem. 2014;116:1178–84.
de Graauw M, van Miltenburg MH, Schmidt MK, Pont C, Lalai R, Kartopawiro J, et al. Annexin A1 regulates TGF-beta signaling and promotes metastasis formation of basal-like breast cancer cells. Proc Natl Acad Sci U S A. 2010;107:6340–5.
Fidler IJ. The pathogenesis of cancer metastasis: the ‘seed and soil’ hypothesis revisited. Nat Rev Cancer. 2003;3:453–8.
Yom CK, Han W, Kim SW, Kim HS, Shin HC, Chang JN, et al. Clinical significance of annexin A1 expression in breast cancer. J Breast Cancer. 2011;14:262–8.
Acknowledgments
We thank all the patients and control subjects for their participation in this study. We also thank the Third Affiliated Hospital of Harbin Medical University, Harbin, China, for the recruitment of patients with breast cancer. This work was supported by YingJi Biotechnology Exploitation Co. Ltd., Shenzhen, China, and by Glory Biomedical Co. Ltd., Taipei, Taiwan.
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding authors
Additional information
Yile Huang and Cong Zhang contributed equally to this work.
Rights and permissions
About this article

Cite this article
Huang, Y., Zhang, C., Chen, C. et al. Investigation of circulating antibodies to ANXA1 in breast cancer. Tumor Biol. 36, 1233–1236 (2015). https://doi.org/10.1007/s13277-014-2751-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-014-2751-x