
Abstract
Human epididymis protein 4 (HE4) is a novel tumour marker in epithelial ovarian cancer (EOC). Data on its profile and predictive potential for subsequent outcome after neoadjuvant chemotherapy (NACT) are still under investigation. The aim of this study was to compare CA125 and HE4 profiles with radiologic response after NACT and to evaluate their potential as predictors of clinical outcome in a primarily inoperable EOC patient cohort. Twenty-five EOC patients of high-grade subtype (HGSC) treated with NACT were enrolled in the study. Serum HE4 and CA125 samples were taken at the time of diagnosis and before interval debulking surgery (IDS). Pre-NACT and pre-IDS HE4 and CA125 and their percentage changes were compared with NACT response seen on CT and surgical outcome in IDS. We also evaluated the biomarkers’ abilities to predict platinum-free interval (PFI), progression-free survival (PFS) and overall survival (OS). All 25 patients were considered inoperable in laparoscopy at the time of diagnosis. HE4 and CA125 changes during NACT did not correlate with the changes seen on CT. Surgical outcome in IDS was associated with pre-IDS biomarker values but not with those taken before diagnosis. In IDS, 87 % had <1-cm residual tumour. In patients with HE4 change >80 and <80 % during NACT, the median OS was 3.38 and 1.60 years (p = 0.01), respectively. Serum HE4 is a promising additional tool when evaluating advanced HGSC patient’s response to NACT. It may be helpful when deciding whether to proceed to IDS or to second-line chemotherapy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
More than two-thirds of high-grade serous ovarian cancers (HGSC), the most important EOC subtype, are diagnosed at an advanced stage. Macroradical cytoreductive surgery followed by chemotherapy is the primary standard treatment for epithelial ovarian cancer (EOC). Neoadjuvant chemotherapy (NACT) followed by interval debulking surgery (IDS) is an alternative treatment strategy [1–3]. Optimal cytoreduction, FIGO stage and platinum sensitivity are some of the most important prognostic factors for survival [4, 5]. In advanced EOC patients, an attempt to achieve optimal cytoreduction means extensive surgery. If it is not successful, the patient undergoes an unnecessary surgical procedure and is exposed to a risk for complications and a delay of chemotherapy. Therefore, it is important to have tools to predict which patients can be optimally debulked.
Among NACT patients, serum tumour marker CA125 and imaging with computed tomography (CT) are generally used to evaluate the treatment response [6, 7]. There are several studies on CA125 accuracy in predicting surgical outcome and survival. In NACT patients, preoperative serum CA125 values and regression rate of CA125 prior to IDS have been associated with favourable surgical outcome [8–10]. In EOC patients treated with primary surgery followed by chemotherapy, CA125 half-life and nadir serum level have been reported to be independent prognosticators of overall survival (OS) and progression-free survival (PFS) [11, 12].
Human epididymis protein 4 (HE4) is a promising novel tumour marker in EOC patients. It has been reported to give additive information when combined with CA125 in detecting ovarian cancer in patients with an adnexal mass [13–15]. There are also data suggesting that HE4 might be an early indicator of both chemosensitivity and recurrent ovarian cancer [16, 17]. Recent studies indicate that preoperative HE4 may predict optimal cytoreduction [18] and residual tumour mass in surgery [19]. Data on pre-IDS HE4 as a predictor of surgical outcome or survival in NACT patients do not exist.
The aim of this study was to evaluate the profile of HE4 during NACT in a primarily inoperable HGSC patient cohort. The biomarkers HE4 and CA125 were compared with radiologic response after three cycles of chemotherapy as predictors of OS, PFS and platinum sensitivity. In addition, we evaluated their potential as predictors of IDS outcome.
Materials and methods
Patients
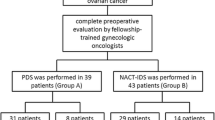
The study population consisted of 25 primarily inoperable HGSC patients treated with NACT at Turku University Hospital in Finland. Patient characteristics are presented in Table 1. The subtype of each tumour was reconfirmed by an expert in gynaecological pathology. The patients participated in a prospective clinical trial designed to study the role of positron emission tomography/computed tomography (PET/CT) and novel serum biomarkers in EOC preoperative diagnostics and treatment response evaluation. The study protocol was approved by the local ethics committee (ClinicalTrials.gov Identifier: NCT01276574, Epithelial Ovarian Cancer —Staging and response to chemotherapy evaluated by PET/CT (MUPET)). The decision to start the treatment either with debulking surgery or NACT was made based on the results of preoperative whole-body contrast-enhanced FDG-PET/CT and a diagnostic laparoscopy or laparotomy. In the case of laparoscopy, a scoring system presented by Fagotti et al. [20] was used to predict the possibility of optimal cytoreduction. The patients who were estimated to be primarily inoperable were scheduled for three cycles of paclitaxel/carboplatin chemotherapy before IDS. In cases where patients’ general condition was poor, carboplatin was used as a single agent. Two patients received four cycles of chemotherapy due to medical reasons delaying IDS. Experienced gynaecologic oncologists and a digestive surgical consultant performed all the operations. The recruitment of the patients for this analysis was started on October 2009 and continued until September 2012. The patients were followed until January 2014 or death.
Analysis of serum HE4 and CA125
Blood samples were collected before diagnostic laparoscopy, before interval debulking surgery and before each chemotherapy cycle. After primary chemotherapy, the samples were collected every 3 months until disease progression. Blood was drawn into non-heparinised tubes and centrifuged for 15 min at 3,000 rpm (800 g) after a 30-min incubation at room temperature. CA125 concentrations (U/mL) were analysed using the ECLIA method (Modular E170 automatic analyser, Roche Diagnostic GmbH, Mannheim, Germany). Serum was dispensed into 2-ml cryotubes and stored at −20 or −80 °C. HE4 concentrations (pmol/L) were manually analysed by ELISA (Fujirebio Diagnostics Inc., Malvern, PA, USA) according to the manufacturer's instructions.
Treatment response evaluation
Patients’ radiological responses to NACT were estimated with contrast-enhanced CT prior to IDS. The patients were classified according to RECIST 1.1 criteria [6] as complete responders (CR) or partial responders (PR) and as having stable disease (SD) or progressive disease (PD). Since the majority of HGSC patients responded to NACT to some extent, the partial responders were further divided into two groups. The patients with marked target lesion reduction of more than 50 % were separated from poor responders with less than 50 % reduction. Similar division based on response was presented by Menczer and co-workers [21]. RECIST 1.1 response and CA125 response were incorporated as suggested by the Gynaecological Cancer Intergroup [7]. These combined criteria was also used when determining the response at the end of first line therapy as well as the time of progression. HE4 values were not available at the time of response evaluation and did not affect clinical decision-making.
Data analysis
Serum HE4 and CA125 percentage changes were calculated using the values at the time of diagnosis and after NACT, but before IDS. Three patients had only baseline biomarker values available, and biomarker changes were calculated from only 22 patients. The biomarker changes were compared with CT response, surgical outcome, platinum-free interval (PFI), progression-free survival (PFS) and overall survival (OS). The strength of the association between biomarkers and CT response, cytoreduction and patient outcome was calculated with the Somer’s D. Kaplan-Meier curves were drawn to assess overall survival and progression-free survival. P values from the log rank test were calculated to compare the curves between >80 and <80 % biomarker changes. The area under the curve (AUC) was calculated with receiver operating characteristic (ROC) analysis and was used to evaluate the biomarkers’ ability to predict surgical outcome. ROC curves were used to select optimal cut-off values to find the best possible combination of sensitivity and specificity of biomarker values. Statistical analysis was performed using SAS for Windows version 9.3 and R [22] softwares.
Results
Changes in biomarkers compared to changes in CT
The changes in HE4 and CA125 during NACT and their pre-IDS values are presented in Table 2. A clear reduction in HE4 and CA125 levels was seen in all the groups regardless of radiologic response to NACT. Even though the CA125 change was found to correlate with CT response in statistical analysis, it did not reflect the clinical situation. Even the patients with progressive disease had a median CA125 decrease of 83 %. In all five patients with PD, the original target lesions showed some decrease in tumour size, but the radiologic response was classified as PD due to new lesions.
HE4 and CA125 in predicting surgical outcome
HE4 values at the time of diagnosis and HE4 changes during NACT did not correlate with surgical outcome, but pre-IDS values predicted it with AUC 0.877. Pre-NACT CA125 values were not associated with surgical outcome. However, it was predicted by CA125 change and pre-IDS CA125 values with AUC 0.895 and 0.947, respectively.
As pre-IDS HE4 and CA125 did predict surgical outcome, we used ROC curves to find cut-off values in order to identify patients likely to have suboptimal (>1 cm) surgical outcome. A pre-IDS HE4 value of 645 pmol/L was considered to be an optimal cut-off value, with a sensitivity of 67 %, a specificity of 95 % and an AUC of 0.877, in identifying patients who would not benefit from IDS. For pre-IDS CA125, the cut-off value of 389 U/mL was considered optimal with a sensitivity of 67 %, a specificity of 100 %, and an AUC of 0.947.
Changes in biomarkers during NACT and patient outcome
Change in CA125 during NACT predicted patients’ PFS and change in HE4 were associated with OS. Biomarker changes during NACT and patient outcomes are presented in Fig. 1. For the overall study population, median OS was 2.81 years. In patients with HE4 changes of >80 and <80 %, the median OS was 3.38 and 1.60 years (p = 0.01), respectively. In patients with CA125 changes of >80 and <80 %, the median OS was 3.38 and 1.13 years (p = 0.35), respectively. Analysing the data using continuous variables also supported these findings.

Patient characteristics
PFS in the whole study population was 1.02 years. In patients with HE4 changes of >80 and <80 %, the median PFS was 1.32 and 0.81 years (p = 0.06), respectively. The median PFS in the patients with CA125 changes of >80 and <80 % was 1.30 and 0.41 years (p = 0.0002), respectively.
PFI was evaluated in patients with complete response (CR, n = 16) after primary treatment. In all the patients with CR, the median time from the end of chemotherapy to disease progression was 0.75 years. In the CR patients with HE4 changes of >80 and <80 %, the median PFI period was 0.99 and 0.43 years (p = 0.15), respectively. CA125 decreased >80 % during NACT in all patients who achieved CR after primary treatment.
Discussion
This study is the first to focus on HE4 profile during NACT in a primarily inoperable HGSC patient cohort. We were able to demonstrate that pre-IDS HE4 values are predictive of surgical outcome and that HE4 change during NACT predicts OS. Our other key findings were that biomarker changes did not correlate with the changes seen on CT and that biomarker levels at the time of diagnosis did not correlate with surgical outcome in IDS.
We have previously studied HE4 profile during EOC primary treatment with 11 patients. The data of our pilot study suggested that HE4 changes may predict radiologic response better than CA125 [23]. In the current study, neither CA125 nor HE4 change correlated with the changes seen in CT. Yildirim et al. [24] and Bellati et al. [25] have debated that guidelines to evaluate NACT response with radiologic imaging may be misleading. It is uncertain whether CT is sensitive enough to measure NACT response. In a study of Menzer et al. [21], CT results prior to IDS did not predict PFS. It is obvious that new methods are needed to evaluate response to NACT to help in clinical decision-making. In the future, both functional imaging like FDG-PET/CT and diffusion MRI and biomarkers like HE4 may be important tools in NACT response evaluation. Our current finding suggesting that HE4 change during NACT correlates with OS supports this assumption, but needs to be confirmed in larger studies.
The results of the current study suggest that pre-IDS HE4 and CA125 values predict IDS outcome in primarily inoperable patients. The finding on CA125 is in line with earlier studies [8–10]. Pre-IDS values of CA125 ranging from <100 [8] to <20 U/mL [9] have been reported to be predictive of no residual tumour. Complete debulking rates in these studies were 47.5 and 61.3 %, respectively. Instead of complete debulking, we chose to search cut-off values finding patients who had a residual tumour of >1 cm in IDS and are unlikely to benefit from surgery. We acknowledge that surgical skills and aggressiveness of surgical approach vary between operating centres. Yet, we are certain that the patients with over 1-cm residual tumour in this study would have been inoperable in any surgical centre. These patients should instead be treated with second-line chemotherapy to avoid unnecessary IDS, with its potential for lowering the quality of life. In our patient population, pre-IDS CA125 >389 U/mL and HE4 >645 pmol/L were cut-off values for inoperability.
Preoperative HE4 values in predicting surgical outcome in primary debulking surgery have been evaluated in recent studies. Angioli et al. [18] demonstrated that cut-off values of HE4 <262 pmol/L combined with ascites of <500 ml were able to target candidates with the potential for optimal cytoreduction. They referred suboptimally debulked patients to NACT. Braicu et al. [19] evaluated 275 primary EOC patients in a multicentre study. CA125 and HE4 values used together correlated with surgical outcome and achieved higher sensitivity and specificity in predicting optimal cytoreduction than either of them alone. Our study is the first to demonstrate the value of pre-IDS HE4 in predicting IDS outcome and suggests that HE4 may be a useful additional tool to predict surgical outcome.
In the present study, the change of biomarkers during NACT was associated with patient’s prognosis. Earlier data of HE4 change on NACT patients do not exist, whereas the behaviour of CA125 during NACT and its association with OS and PFS have been studied earlier. Tate et al. [26] and Vasudev et al. [10] have reported that CA125 regression rate during NACT predicts OS. Furukawa et al. [9] found low pre-IDS CA125 of <20 kU/L to predict both complete IDS and longer OS. On the other hand, there are also data suggesting that CA125 response to NACT is not an independent prognostic factor for PFS [27].
In the current study, the change of HE4 less than 80 % during NACT was associated with poor prognosis in our patient material. This is in line with a recent study by Angioli indicating that HE4 level >70 pmol/L after primary surgery and three cycles of chemotherapy predicted platinum resistance [16]. The cut-off values used in our study were chosen based on previous studies on CA125. Le et al. [27] reported that a 50 % reduction in CA125 during NACT was not predictive of PFS. Instead, Rodriquez et al. [8] chose </>80 % reduction in CA125 as the cut-off value and found it to predict PFI. However, in our material, only three patients presented CA125 change of less than 80 %. This unbalanced division of patients may have influenced the CA125 results. The HE4 values were more equally distributed.
The small number of patients is a limitation and might bias the results. On the other hand, the strength of our study is the carefully selected study population. This study is part of a larger prospective clinical trial conducted with a strict protocol. Our study population represents clinically homogenous highly challenging group of primarily inoperable HGSC patients. Operability is a complex issue to study because it depends highly on patient cohort and the quality and extent of surgery. Our complete resection rate of 23 % in IDS was rather low. However, residual tumour of <1 cm (87 %) in this primarily inoperable patient cohort was comparable with randomised EORTC trial on NACT (81 %) [1], even though the patients in our study were not randomised to NACT but selected due to very extensive disease dissemination. Nevertheless, the decision to pursue surgical treatment cannot be based solely on laboratory results, but all the available clinical data, including physical examination, imaging, and the patient’s general condition, must be considered.
The findings of pre-IDS HE4 being a predictor of surgical outcome and HE4 change during NACT being associated with OS give additional support of the value of HE4 as a clinically useful biomarker of EOC. Larger trials on HE4’s potential to find inoperable patients are warranted.
References
Vergote I, Tropé CG, Amant F, Kristensen GB, Ehlen T, Johnson N, et al. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med. 2010;363(10):943–53.
Vergote I, Amant F, Kristensen G, Ehlen T, Reed NS, Casado A. Primary surgery or neoadjuvant chemotherapy followed by interval debulking surgery in advanced ovarian cancer. Eur J Cancer. 2011;47 Suppl 3:S88–92.
Kang S, Nam BH. Does neoadjuvant chemotherapy increase optimal cytoreduction rate in advanced ovarian cancer? Meta-analysis of 21 studies. Ann Surg Oncol. 2009;16(8):2315–20.
Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002;20(5):1248–59.
du Bois A, Reuss A, Pujade-Lauraine E, Harter P, Ray-Coquard I, Pfisterer J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: by the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d'Investigateurs Nationaux Pour les Etudes des Cancers de l'Ovaire (GINECO). Cancer. 2009;115(6):1234–44.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47.
Rustin GJ, Vergote I, Eisenhauer E, Pujade-Lauraine E, Quinn M, Thigpen T, et al. Definitions for response and progression in Ovarian Cancer Clinical Trials Incorporating RECIST 1.1 and CA 125 agreed by the Gynecological Cancer Intergroup (GCIG). Int J Gynecol Cancer. 2011;21(2):419–23.
Rodriguez N, Rauh-Hain JA, Shoni M, Berkowitz RS, Muto MG, Feltmate C, et al. Changes in serum CA-125 can predict optimal cytoreduction to no gross residual disease in patients with advanced stage ovarian cancer treated with neoadjuvant chemotherapy. Gynecol Oncol. 2012;125(2):362–6.
Furukawa N, Sasaki Y, Shigemitsu A, Akasaka J, Kanayama S, Kawaguchi R, et al. CA-125 cut-off value as a predictor for complete interval debulking surgery after neoadjuvant chemotherapy in patients with advanced ovarian cancer. J Gynecol Oncol. 2013;24(2):141–5.
Vasudev NS, Trigonis I, Cairns DA, Hall GD, Jackson DP, Broadhead T, et al. The prognostic and predictive value of CA-125 regression during neoadjuvant chemotherapy for advanced ovarian or primary peritoneal carcinoma. Arch Gynecol Obstet. 2011;284(1):221–7.
Riedinger JM, Wafflart J, Ricolleau G, Eche N, Larbre H, Basuyau JP, et al. CA 125 half-life and CA 125 nadir during induction chemotherapy are independent predictors of epithelial ovarian cancer outcome: results of a French multicentric study. Ann Oncol. 2006;17(8):1234–8.
van Altena AM, Kolwijck E, Spanjer MJ, Hendriks JC, Massuger LF, de Hullu JA. CA125 nadir concentration is an independent predictor of tumor recurrence in patients with ovarian cancer: a population based study. Gynecol Oncol. 2010;119(2):265–9.
Moore RG, Brown AK, Miller MC, Skates S, Allard WJ, Verch T, et al. The use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol Oncol. 2008;108(2):402–8.
Huhtinen K, Suvitie P, Hiissa J, Junnila J, Huvila J, Kujari H, et al. Serum HE4 concentration differentiates malignant ovarian tumours from ovarian endometriotic cysts. Br J Cancer. 2009;100(8):1315–9.
Park Y, Lee JH, Hong DJ, Lee EY, Kim HS. Diagnostic performances of HE4 and CA125 for the detection of ovarian cancer from patients with various gynecologic and non-gynecologic diseases. Clin Biochem. 2011;44(10–11):884–8.
Angioli R, Capriglione S, Aloisi A, Guzzo F, Luvero D, Miranda A, et al. Can HE4 predict platinum response during first-line chemotherapy in ovarian cancer? Tumour Biol. 2014 Apr 21.
Anastasi E, Marchei GG, Viggiani V, Gennarini G, Frati L, Reale MG. HE4: a new potential early biomarker for the recurrence of ovarian cancer. Tumour Biol. 2010;31(2):113–9.
Angioli R, Plotti F, Capriglione S, Aloisi A, Montera R, Luvero D, et al. Can the preoperative HE4 level predict optimal cytoreduction in patients with advanced ovarian carcinoma? Gynecol Oncol. 2013;128(3):579–83.
Braicu EI, Fotopoulou C, Van Gorp T, Richter R, Chekerov R, Hall C, et al. Preoperative HE4 expression in plasma predicts surgical outcome in primary ovarian cancer patients: results from the OVCAD study. Gynecol Oncol. 2013;128(2):245–51.
Fagotti A, Ferrandina G, Fanfani F, Garganese G, Vizzielli G, Carone V, et al. Prospective validation of a laparoscopic predictive model for optimal cytoreduction in advanced ovarian carcinoma. Am J Obstet Gynecol. 2008;199:642e1–6.
Menczer J, Usviatzov I, Ben-Shem E, Golan A, Levy T. Neoadjuvant chemotherapy in ovarian, primary peritoneal and tubal carcinoma: can imaging results prior to interval debulking predict survival? J Gynecol Oncol. 2011;22(3):183–7.
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. 2012. ISBN 3-900051-07-0, URL http://www.R-project.org/.
Hynninen J, Auranen A, Dean K, Lavonius M, Carpen O, Perheentupa A, et al. Serum HE4 profile during primary chemotherapy of epithelial ovarian cancer. Int J Gynecol Cancer. 2011;21(9):1573–8.
Yildirim Y, Ertas IE, Dogan A, Gultekin OE, Gultekin E. The predictors of response to neoadjuvant chemotherapy in advanced epithelial ovarian cancer. J Surg Oncol. 2012;105(2):200–5.
Bellati F, Gasparri ML, Caccetta J, Palaia I, Benedetti Panici P. Response criteria can be misleading when drawing conclusion regarding neoadjuvant chemotherapy in advanced ovarian cancer. J Surg Oncol. 2012;106(4):529. author reply 527-8.
Tate S, Hirai Y, Takeshima N, Hasumi K. CA125 regression during neoadjuvant chemotherapy as an independent prognostic factor for survival in patients with advanced ovarian serous adenocarcinoma. J Gynecol Oncol. 2005;96(1):143–9.
Le T, Hopkins L, Faught W, Fung-Kee-Fung M. The lack of significance of Ca125 response in epithelial ovarian cancer patients treated with neoadjuvant chemotherapy and delayed primary surgical debulking. Gynecol Oncol. 2007;105(3):712–5.
Acknowledgments
This study was financially supported by the Clinical Research (EVO) funding of Turku University Hospital. We are thankful to Pia Roering for the technical assistance with HE4 analyses.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Vallius, T., Hynninen, J., Auranen, A. et al. Serum HE4 and CA125 as predictors of response and outcome during neoadjuvant chemotherapy of advanced high-grade serous ovarian cancer. Tumor Biol. 35, 12389–12395 (2014). https://doi.org/10.1007/s13277-014-2553-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-014-2553-1