
Abstract
Vascular endothelial growth factor (VEGF) is considered as a prime mediator of angiogenesis and has been implicated in carcinogenesis and metastasis. Various studies examined the relationship between VEGF overexpression with the clinical outcome in patients with osteosarcoma but yielded conflicting results. Electronic databases updated to April 2013 were searched to find relevant studies. A meta-analysis was conducted with eligible studies which quantitatively evaluated the relationship between VEGF overexpression and survival of patients with osteosarcoma. Survival data were aggregated and quantitatively analyzed. We performed a meta-analysis of eight studies that evaluated the correlation between VEGF overexpression and survival in patients with osteosarcoma. Combined hazard ratios suggested that VEGF overexpression had an unfavorable impact on overall survival (hazard ratio (HR) = 1.75, 95 % confidence interval (CI): 1.21–2.28) in patients with osteosarcoma for overall populations, 2.37 (1.35–3.39) in Asian studies but not in non-Asian studies (HR = 1.51, 95 % CI: 0.89–2.14). No significant heterogeneity was observed among all studies. VEGF overexpression indicates a poor prognosis for patients with osteosarcoma. However, the prognostic value of VEGF on survival in osteosarcoma patients still needs further large-scale prospective trials to be clarified.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteosarcoma is the most common malignant bone tumor in adolescents and young adults [1]. The oncological treatment of osteosarcoma consisting of chemotherapy and a surgical excision of the tumor leads to a 5-year overall survival (OS) rate at 60–70 % of patients with the disease localized at presentation. The OS rate decreases to 30 % when metastases are detected at the time of diagnosis [2]. Despite recent advances in surgical, radiotherapy, and chemotherapy treatment protocols, the long-term survival of patients with osteosarcoma still lacks significant improvement for the past decades. The factors that additionally influence the prognosis are the axial localization of the primary tumor, the tumor diameter of more than 8 cm, and the unfavorable histological response to pre-operative chemotherapy [3, 4]. However, the prognostic factors do not fully predict individual clinical outcome. There is the need for better markers to identify patients with poor prognosis at the time of diagnosis. Researchers have focused on the potential role of new biological factors involved in the carcinogenic process as prognostic markers in patients with osteosarcoma.
Angiogenesis, the formation of new blood vessels from existing vasculature, is an important process in many malignancies including osteosarcoma. It is the result of an intricate balance between pro-angiogenic and anti-angiogenic factors. VEGF (also referred to as VEGF-A, vascular permeability factor) is a critical pro-angiogenic factor in cancer. The role of VEGF in the regulation of angiogenesis is the object of intense investigation for more than a decade. The VEGF family is composed of several subtypes, including VEGF-A, VEGF-B, VEGF-C, and VEGF-D, which exist as numerous splice variant isoforms [5, 6]. Many anti-angiogenic compounds are being developed, most of which target VEGF and/or its receptors. It is necessary to establish whether VEGF expression is a prognostic marker in osteosarcoma patients.
Many retrospective studies have evaluated whether overexpression of VEGF may be a prognostic factor for survival in patients with osteosarcoma. However, the results of the studies are inconclusive, and no consensus has been reached. It is unknown whether differences in these investigations have been mostly due to their limited sample size or genuine heterogeneity. Thus, we conducted a meta-analysis of all available studies relating VEGF with the clinical outcome in patients with osteosarcoma.
Materials and methods
Search strategy and study selection
The electronic databases PubMed, Embase, and CNKI (China National Knowledge Infrastructure) were searched for studies to include in the present meta-analysis. An upper date limit of April 1, 2013 was applied; we used no lower date limit. Searches included the terms “osteosarcoma,” “osteogenic sarcoma,” “VEGF,” “vascular endothelial growth factor,” and “prognosis”. We also reviewed the Cochrane Library for relevant articles. The references reported in the identified studies were also used to complete the search.
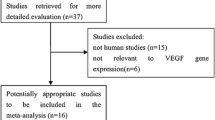
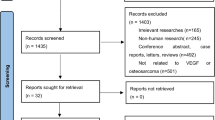
Studies eligible for inclusion in this meta-analysis met the following criteria: (1) measure VEGF expression in the osteosarcoma tissue with immunohistochemistry (IHC) or reverse transcription-polymerase chain reaction (RT-PCR), (2) provide information on survival, including OS, (3) have a follow-up time exceeding 5 years, and (4) when the same author reported results obtained from the same patient population in more than one publication, only the most recent report or the most complete one, which was included in the analysis. Two reviewers (X.Y. and T.W.) independently determined study eligibility. Disagreements were resolved by consensus.
Data extraction and quality assessment
The final articles included were assessed independently by two reviewers (X.Y. and T.W.). Data retrieved from the reports included author, publication year, patient source, histo-subtype, disease stage, test method, definition of positivity (cutoff value), VEGF positive, and survival data (Table 1). If data from any of the above categories were not reported in the primary study, items were treated as “not applicable”. We did not contact the author of the primary study to request the information. We did not use pre-specified quality-related inclusion or exclusion criteria and did not weigh each study by a quality score because the quality score has not received general agreement for use in a meta-analysis, especially observational studies [7]. The data extraction and quality assessment were reported in previous meta-analysis [8–12].
Statistical methods
For the quantitative aggregation of the survival results, we measured the impact of VEGF overexpression on survival by HR between the two survival distributions. HRs and 95 % CIs were used to combine as the effective value. If the HRs and their 95 % CIs were given explicitly in the articles, we used crude ones. When these variables were not given explicitly, they were calculated from the available numerical data using methods reported by Parmar et al. [13].
Heterogeneity of the individual HRs was calculated with χ2 tests according to Peto's method [14]. Heterogeneity test with inconsistency index (Ι2) statistic and Q statistic was performed. If HRs were found to have fine homogeneity, a fixed effect model was used for secondary analysis; if not, a random-effect model was used. DerSimonian–Laird random effects analysis [15] was used to estimate the effect of VEGF overexpression on survival. By convention, an observed HR >1 implies worse survival for the group with VEGF overexpression. The impact of VEGF on survival was considered to be statistically significant if the 95 % CI did not overlap with 1. Horizontal lines represent 95 % CIs. Each box represents the HR point estimate, and its area is proportional to the weight of the study. The diamond (and broken line) represents the overall summary estimate, with CI represented by its width. The unbroken vertical line is set at the null value (HR = 1.0).
Evidence of publication bias was sought using the methods of Egger et al. [16] and Begg and Mazumdar [17]. Intercept significance was determined by the t test suggested by Egger (P < 0.05 was considered representative of statistically significant publication bias). All of the calculations were performed by STATA version 11.0 (Stata Corporation, College Station, TX).
Results
Study selection and characteristics
A total of 13 studies [18–30] published between 1999 and 2012 were included in the analysis. However, the five studies [14, 18, 20, 22, 23] did not provide the data on overall survival of patients in VEGF overexpression. Eight studies reported the prognostic value of VEGF status for overall survival. The major characteristics of the 13 eligible publications are reported in Table 1. The total number of patients included meta-analysis was 323, ranging from 15 to 91 patients per study (median 32). The studies were conducted in three countries (China, Japan, and Korea) and published between 1999 and 2012. Among the eight studies, six studies (176 patients, 54.5 %) were performed in Asian populations, and the remaining two studies (147 patients) followed non-Asian patients. All patients in the eligible studies were determined by pathological stage.
All of the studies reported the prognostic value of VEGF status for survival in patients with osteosarcoma. Of the eight studies, four directly reported HRs (multivariate analysis), while the other four studies provided survival curves. Among them, the proportion of patients exhibiting VEGF overexpression in individual studies ranged from 20 % to 96 %. Six of the eight studies identified VEGF overexpression as an indicator of poor prognosis, and the other two studies showed no statistically significant impact of VEGF overexpression on survival.
Meta-analysis
The results of the meta-analysis were shown in Table 2 and Fig. 1. Overall, the combined HR for all eight eligible studies evaluating VEGF overexpression on OS was 1.75 (95 % CI: 1.21–2.28), suggesting that VEGF overexpression was an indicator of poor prognosis for osteosarcoma patients. No significant heterogeneity was observed among the studies (Q = 4.39, I 2 = 15.3 %, P = 0.310). When grouped according to geographic settings of individual studies, the combined HRs of Asian studies and non-Asian studies were 2.37 (95 % CI: 1.35–3.39) and 1.51 (95 % CI: 0.89–2.14), respectively, indicating that VEGF is an indicator of poor prognosis of OS in Asian patients but not in non-Asian patients. No significant heterogeneity was observed among the studies on VEGF overexpression on Asian studies (Q = 3.48, I 2 = 0.0 %, P = 0.360) and non-Asian studies (Q = 4.53, I 2 = 0.0 %, P = 0.370)

Meta-analysis (forest plot) of the eight evaluable studies assessing VEGF in osteosarcoma stratified by patient source for overall survival
Publication bias
Begg's funnel plot and Egger's test were performed to assess the publication bias in the literature. All eight eligible studies investigating VEGF overexpression on OS yielded a Begg's test score of P = 0.019 and an Egger's test score of P = 0.001; meanwhile, according to the funnel plot (Fig. 2), the publication bias was found. These results suggested that there were publication biases in these subgroup analyses.

Funnel plot of the eight evaluable studies assessing VEGF in osteosarcoma for overall survival
Discussion
Members of the VEGF family promote two very important processes in vivo, angiogenesis, and lymphangiogenesis, which involve growth of new blood and lymphatic vessels from pre-existing vasculature, respectively. VEGF-A exists as a homodimer or can heterodimerize with either VEGF-B or non-VEGF factors such as placenta growth factor [31–33]. VEGF-A and VEGF-B promote vascular angiogenesis primarily through activation of vascular endothelial cell associated VEGFR-1 (Flt1) and VEGFR-2 (Flk1/KDR).
The present meta-analysis has combined eight publications including 323 patients to yield statistics, indicating a statistically significant role of VEGF on overall survival in osteosarcoma patients. In subgroup analysis according to the geographic settings of individual studies, statistically significant detrimental effect of VEGF was found in Asian patients but not in non-Asian patients. In our meta-analysis, patient cohorts were mainly from Eastern Asian countries (176 patients, 54.5 %), only two study patient sources were non-Asian. In our meta-analysis, the combined hazard ratios mainly represented the Eastern Asian; however, the results of western countries remained unclear.
There were several meta-analyses studying the prognostic value of VEGF in other cancer types, such as head and neck squamous cancer [34], lung cancer [35], colon cancer [36], gastric cancer [37], and hepatocellular carcinoma [38]. Association of VEGF overexpression with poor outcomes provides a rationale for anti-angiogenic use in the treatment of cancer. VEGF has become a leading therapeutic target for the treatment of cancer. Potentially, therapeutic strategies to inhibit VEGF pathway include monoclonal antibodies directed against VEGF, tyrosine kinase inhibitors (TKIs), and antisense strategies [39]. Bevacizumab (a humanized monoclonal antibody) is an effective anti-angiogenic agent that is the first to be approved by the American Food and Drug Administration as the first-line treatment for metastatic colorectal cancer [40], and it blocks secreted VEGF and prolongs overall survival of patients with advanced NSCLC in combination with standard chemotherapy in a randomized phase 3 trial [41] and patients who respond well to Bevacizumab with recurrent malignant gliomas [42].
The heterogeneity issue was complicated in the systematic review and meta-analysis. We found no significant heterogeneity among all studies and subgroup analysis included. Another potential source of bias is related to the method of HR and 95 % CI extrapolation. If these statistics were not reported by the authors, we calculated them from the data available in the article. If this was not possible, we extrapolated them from the survival curves, necessarily making assumptions about the censoring process. Data for multivariate survival analysis reported in the article were included in the present systematic review with meta-analysis; if these data were not available, data calculated from survival curves by univariate analysis were included. These results should be confirmed by an adequately designed prospective study. Furthermore, the exact value of VEGF overexpression status needs to be determined by appropriate multivariate analysis. Unfortunately, few prospectively designed prognostic studies concerning biomarkers have been reported; thus, our collection of many retrospective studies revealed more significance.
Publication bias [43] is a major concern for all forms of meta-analysis; positive results tend to be accepted by journals, while negative results are often rejected or not even submitted. The present analysis does support publication bias; the obtained summary statistics likely approximate the actual average. It should be noted that our meta-analysis could not completely exclude biases. For example, the study was restricted to papers published in English and Chinese, which probably introduced bias.
In conclusion, our meta-analysis is the first study to systematically estimate the association between VEGF expression and survival of patients with osteosarcoma. As determined in our meta-analysis, we concluded that VEGF expression was associated with poor overall survival in osteosarcoma, and there is no significant heterogeneity among all studies. To strengthen our findings, well-designed prospective studies with better standardized assessment of prognostic markers should help to explore the relation between VEGF overexpression and survival of osteosarcoma.
References
Mirra JM, Gold RH, Picci P. Osseous tumors of intramedullary origin. In: Mirra JM, editor. Bone tumors: clinical radiologic, and pathologic correlations. Philadelphia: Lea and Febiger; 1989. p. 143–438.
Bielack S, Jürgens H, Jundt G, et al. Osteosarcoma: the COSS experience. Cancer Treat Res. 2010;152:289–308.
Davis AM, Bell RS, Goodwin PJ. Prognostic factors in osteo-sarcoma: a critical review. J Clin Oncol. 1994;12:423–31.
Bacci G, Longhi A, Versari M, et al. Prognostic factors for osteosarcoma of the extremity treated with neoadjuvant chemo-therapy: 15-year experience in 789 patients treated at a single institution. Cancer. 2006;1:1154–61.
Ferrara N. VEGF and the quest for tumour angiogenesis factors. Nat Rev Cancer. 2002;2:795–803.
Hicklin DJ, Ellis LM. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J Clin Oncol. 2005;23:1011–27.
Altman DG. Systematic reviews of evaluations of prognostic variables. BMJ. 2001;323(7306):224–8.
Zhan P, Qian Q, Yu LK. Prognostic value of COX-2 expression in patients with non-small cell lung cancer: a systematic review and meta-analysis. J Thorac Dis. 2013;5(1):40–7. doi:10.3978/j.issn.2072-1439.2013.01.02.
Zhan P, Qian Q, Wan B, Yan TD, Yu LK. Prognostic value of TTF-1 expression in patients with non-small cell lung cancer: a meta-analysis. Transl Cancer Res. 2013;2(1):25–32. doi:10.3978/j.issn.2218-676X.2013.02.08.
Zhan P, Wang Q, Qian Q, Yu LK. Megestrol acetate in cancer patients with anorexia-cachexia syndrome: a meta-analysis. Transl Cancer Res. 2013;2(2):74–9. doi:10.3978/j.issn.2218-676X.2013.04.13.
Zhan P, Wang Q, Qian Q, Yu LK. Risk of venous thromboembolism with the erythropoiesis-stimulating agents (ESAs) for the treatment of cancer-associated anemia: a meta-analysis of randomized control trials. Clin Oncol: Chin; 2013 Jan 03.
Zhan P, Qian Q, Yu LK. Prognostic significance of vascular endothelial growth factor expression in hepatocellular carcinoma tissue: a meta-analysis. Hepatobiliary Surg Nutr 2013 Jun 21. doi: 10.3978/j.issn.2304-3881.2013.06.06
Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform metaanalyses of the published literature for survival endpoints. Stat Med. 1998;17:2815–34.
Yusuf S, Peto R, Lewis J, et al. Blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis. 1985;27:335–71.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Egger M, Smith GD, Schneider M. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–101.
Lee YH, Tokunaga T, Oshika Y, et al. Cell-retained isoforms of vascular endothelial growth factor (VEGF) are correlated with poor prognosis in osteosarcoma. Eur J Cancer. 1999;35(7):1089–93.
Handa A, Tokunaga T, Tsuchida T, et al. Neuropilin-2 expression affects the increased vascularization and is a prognostic factor in osteosarcoma. Int J Oncol. 2000;17(2):291–5.
Kaya M, Wada T, Akatsuka T, et al. Vascular endothelial growth factor expression in untreated osteosarcoma is predictive of pulmonary metastasis and poor prognosis. Clin Cancer Res. 2000;6(2):572–7.
Jung ST, Moon ES, Seo HY, Kim JS, Kim GJ, Kim YK. Expression and significance of TGF-beta isoform and VEGF in osteosar-coma. Orthopedics. 2005;28(8):755–60.
Charity RM, Foukas AF, Deshmukh NS, Grimer RJ. Vascular endothelial growth factor expression in osteosarcoma. Clin Orthop Relat Res. 2006;448:193–8.
Ek ET, Ojaimi J, Kitagawa Y, Choong PF. Does the degree of intratumoural microvessel density and VEGF expression have prognostic significance in osteosarcoma. Oncol Rep. 2006;16(1):17–23.
Oda Y, Yamamoto H, Tamiya S, et al. CXCR4 and VEGF expression in the primary site and the metastatic site of human osteosarcoma: analysis within a group of patients, all of whom developed lung metastasis. Mod Pathol. 2006;19(5):738–45.
Abdeen A, Chou AJ, Healey JH, et al. Correlation between clinical outcome and growth factor pathway expression in osteogenic sarcoma. Cancer. 2009;115(22):5243–50.
Kaya M, Wada T, Nagoya S, Sasaki M, Matsumura T, Yamashita T. The level of vascular endothelial growth factor as a predictor of a poor prognosis in osteosarcoma. J Bone Joint Surg Br. 2009;91(6):784–8.
Boulytcheva IV, Soloviev YN, Kushlinskii NE, Mahson AN. Expression of molecular markers in the tumor and survival prognosis in osteosarcoma. Bull Exp Biol Med. 2010;150(2):237–42.
Zhou Q, Zhu Y, Deng Z, Long H, Zhang S, Chen X. VEGF and EMMPRIN expression correlates with survival of patients with osteosarcoma. Surg Oncol. 2011;20(1):13–9.
Ługowska I, Woźniak W, Klepacka T, Michalak E, Szamotulska K. A prognostic evaluation of vascular endothelial growth factor in children and young adults with osteosarcoma. Pediatr Blood Cancer. 2011;15;57(1):63–8.
Chen Y, Wang CM, Shi YQ, Yang Y. Expression of hypoxia-inducible factor 1α in osteosarcoma and its value in predicting chemosensitivity [in Chinese]. Chien J Oncol. 2012;34(12):899–904.
Parikh AA, Ellis LM. The vascular endothelial growth factor family and its receptors. Hematol Oncol Clin North Am. 2004;18(5):951–71. vii.
Xie K, Wei D, Shi Q, Huang S. Constitutive and inducible expression and regulation of vascular endothelial growth factor. Cytokine Growth Factor Rev. 2004;15(5):297–324.
Hicklin DJ, Ellis LM. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J Clin Oncol. 2005;23(5):1011–27.
Kyzas PA, Cunha IW, Ioannidis JP. Prognostic significance of vascular endothelial growth factor immunohistochemical expression in head and neck squamous cell carcinoma: a meta-analysis. Clin Cancer Res. 2005;11(4):1434–40.
Zhan P, Wang J, Lv XJ, Wang Q, Qiu LX, Lin XQ, et al. Prognostic value of vascular endothelial growth factor expression in patients with lung cancer: a systematic review with meta-analysis. J Thorac Oncol. 2009;4(9):1094–103.
Des Guetz G, Uzzan B, Nicolas P, Cucherat M, Morere JF, Benamouzig R, et al. Microvessel density and VEGF expression are prognostic factors in colorectal cancer. Meta-analysis of the literature Br J Cancer. 2006;94(12):1823–32.
Peng L, Zhan P, Zhou Y, Fang W, Zhao P, Zheng Y, et al. Prognostic significance of vascular endothelial growth factor immunohistochemical expression in gastric cancer: a meta-analysis. Mol Biol Rep. 2012 Oct;39(10):9473–84.
Schoenleber SJ, Kurtz DM, Talwalkar JA, Roberts LR, Gores GJ. Prognostic role of vascular endothelial growth factor in hepatocellular carcinoma: systematic review and meta-analysis. Br J Cancer. 2009;100(9):1385–92.
Kowanetz M, Ferrara N. Vascular endothelial growth factor signaling pathways: therapeutic perspective. Clin Cancer Res. 2006;12(17):5018–22.
Ranieri G, Patruno R, Ruggieri E, Montemurro S, Valerio P, Ribatti D. Vascular endothelial growth factor (VEGF) as a target of bevacizumab in cancer: from the biology to the clinic. Curr Med Chem. 2006;13(16):1845–57.
Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med. 2006;355(24):2542–50.
Xu T, Chen J, Lu Y, Wolff JE. Effects of bevacizumab plus irinotecan on response and survival in patients with recurrent malignant glioma: a systematic review and survival-gain analysis. BMC Cancer. 2010;10:252.
Begg CB, Berlin JA. Publication bias: a problem in interpreting medical data. J R Stat Soc A. 1988;151:419–63.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (no. 81071487), the Social Development Program of Jiangsu Province (no. BE2010744), Medical Scientific Research Foundation of Jiangsu Province (no. H201008), the Program for Medical Talents of Jiangsu Province (no. H201122), China Postdoctoral Science Foundation (no. 20100480598), and the Shanghai Postdoctoral Sustentation Fund (no. 11R21414400), the Natural Science Foundation of Shanghai Municipal Health Bureau (no. 20114y079); the Medicine and Engineering Foundation of Shanghai Jiaotong University (no. YG2011MS33).
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yu, XW., Wu, TY., Yi, X. et al. Prognostic significance of VEGF expression in osteosarcoma: a meta-analysis. Tumor Biol. 35, 155–160 (2014). https://doi.org/10.1007/s13277-013-1019-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-013-1019-1