
Abstract
Cancers found in colorectal region remain largely localized to the large intestine and rectum. They are derived from the epithelium and are considered to be among the most frequently detected cancers. They are known to occur in approximately 5 % population of the Western world. After metastasis, a patient’s 5-year postsurgical survival chances unfortunately fall from 90 to 10 % or even less. Adenocarcinoma, the most common cell type of colon cancer, alone constitutes 95 % of the cases. Lymphoma and squamous cell carcinoma can also be found in some cases. Because 5 % of persons are predisposed to development of colorectal cancer, this disease has often been addressed as an important public health issue. Factors that are known in particular to increase a person’s risk to develop this cancer are as follows: an individual’s age, dietary habits, any complaint of obesity, diabetes, previous history of cancer or intestinal polyps, personal habit of alcohol consumption and smoking, family history of colon cancer, race, sex, and ethnicity. Since the risk of colorectal cancer is increasing steadily in Kashmir, India, like in some other corners of Asia, exhaustive efforts are being made to find the association of above given and other risk factors with the development of this gastrointestinal tract cancer. Adoption of Western life style, diet mimicry, together with a habit of having physically inactive life style and consumption of red meat in particular can be blamed as being active players to a considerable extent.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Incidence and epidemiology
Colorectal cancer patient number has been going up continuously since 1975 (above 500,000). Boyle and Langman have observed that like most other types of cancers, different populations in different parts of world experience colorectal cancer with varying severities and these keep changing with time. Astonishingly, the adoption of the risk associated with the new community in the very first generation of migrant groups reflects the fact that geographic variations in incidence are unrelated to genetic differences [1].
Almost 9.4 % of cancers occurring among men and 10.1 % among women of the world constitutes colorectal cancer (CRC) [1]. This incidence, however, is not equal throughout; if the westernized countries (comprising mainly of Europe; Australasia, New Zealand, and North America) are combined, colorectal cancer accounts for 12.6 % of all incident cancers among men and 14.1 % among women. In other parts of the world, it represents 7.7 and 7.9 % of all incident cases in men and women, respectively [1]. Impressive differences in cancer survival are seen to exist between Great Britain, whole of Europe, and USA. No easy explanation has been given so far for this variation in survival except for treatment delivery or the stage of CRC at presentation or both [1].
Worldwide trend
According to GLOBOCAN 2008, approximately 60 % of the colorectal cancer cases have been reported to occur in more developed parts of the world. Worldwide incidence rates are seen to vary tenfold in both the male and female sexes: the most have been estimated in Western Europe and Australia/New Zealand, the least in Africa (except for South Africa) and Southern part of Central Asia, and intermediate have been estimated in Latin America. Overall, sex ratio of the age-standardized rates between male and females is 1.4:1. Nearly 608,000 deaths from CRC have been estimated throughout the world, that alone account for 8 % of total cancer-related deaths, and thus it is the fourth most common cause of cancer deaths. Mortality rates like incidence are less in females than males, except in the Caribbean. The worldwide rate has been seen to vary sixfold among males and fivefold among females; the most mortality rates in both sexes have been estimated in Central and Eastern parts of Europe (20.3/100,000 for men 12.1/100,000 for women) and the least in Middle of Africa (3.5 and 2.7, respectively) [3].
Nearly 150,000 residents of USA are diagnosed with colorectal cancer each year, and approximately one third of these patients die from the disease [3]. The lifetime risk of CRC in the USA has been estimated to be 6 %, and the average age of diagnosis to be 66 years [4, 5]. There are approximately 64 % chances of 5-year survival for persons with CRC in USA. It may vary from 90 % to merely 39 % depending on the stage of its detection [6]. Ferlay et al. have estimated that colorectal cancer was the second most common form of cancer in Europe during 2006 with 412,900 cancer diagnoses (12.9 % of total cancers) and 207,400 deaths (ranking second) [6]. Studies show that every year some 2,000 persons are diagnosed with CRC in New Zealand and about 1,000 die of it [7].
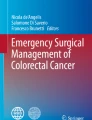
The disease is however uncommon in Africa, Asia, and South America, which might suggest a possible link with a diet rich in animal fat in developed nations [8]. This epidemiological trend is now changing in Asian countries, and the incidence of colorectal carcinomas is rising steadily [9, 10] (Fig. 1).

Estimated age-standardized rates (world) as per 100,000 IARC, GLOBOCAN 2008
World Health Organization data report has shown that during past few decades countries like Japan, China, South Korea, and Singapore have roughly experienced some two to fourfold increase in CRC incidence rates [11–14].
Indian scenario
While the incidence of colon cancer varies widely from one country to another throughout the world, according to GLOBOCAN 2008, the age standardized incidence rate of colorectal cancer in India is 20/100,000 for men and 16/100,000 for women, with the mortality rates estimated due to colorectal cancer for both sexes being 25/100,000 (14/100,000 for men and 11/100,000 for women) [2]. Time trend surveys based on population, carried out over the years in India, indicate a rising trend in the incidence of CRC [15] (Fig. 2). The overall 5-year survival rate studies for CRC patients were found out to be 34.3 %, lower than in either other Asian or Western countries [16]. Data also show that the rates of incidence for rectal cancer are higher than colon cancer throughout India [14, 17], especially in the rural parts of India [14, 17, 18]. The variation of the incidence rates of CRC across India is limited, unlike the striking north–south differences in the incidence rates of stomach cancer and gall bladder cancer [17, 18]. So strong is the role of lifestyle and dietary habits in the development of CRC that relative incidence rates of colorectal cancer in Indian immigrants to the UK and USA are seen to be quite higher [19–21].

Trends in incidence of colorectal cancer in India: age-standardized rate (W) per 100,000 men and women, respectively, according to GLOBOCAN–IARC 2008
CRC in Kashmir
Kashmir Valley, in the northern most part of India, has its unique geography and climate. Muslims of Kashmir representing more than 90 % of the population are known for their distinct dietary habits, nonmigratory nature, and distinct social culture. The valley has often been reported as a high incidence area for cancers of GIT [22, 23]. CRC has been seen to be the fourth most common cancer among males; it holds a third rank amongst the female folks of Kashmir in occurrence [24] and has been observed to constitute 8.3 % of all GIT cancers. A hospital-based study from Kashmir conducted by Javid et al. shows that the age-standardized incidence rate of 4.52 per 100,000 of the population and the age-specific rate for colorectal carcinoma to be highest in the age group 55–59 years (17.21/100,000), followed by 65–69 years (14.86/100,000) [25]. The male to female ratio of occurrence of CRC in Kashmir has been proposed to be 1.2:1, and that the incidence rates for CRC among Muslims and Hindus of Kashmir have been reported to be different, that is 3.64/100,000 and 0.45/100,000, respectively. Their study also suggest that the crude incidence rate for colorectal carcinoma is highest for Srinagar District (6.19/100,000 (urban area)) and lowest for Kupwara District (1.59/100,000 (rural area)), which clearly suggests a possible role of urbanization in relatively high-risk population of Srinagar (Table 1).
Risk factors associated with colorectal cancer
According to Boyle and Langman, CRC is believed to be an environmental disease, as 70–80 % of such cases have been observed to result from an interplay of ill-defined cultural, social, and lifestyle-associated factors, clearly identifying CRC as one of the major neoplasms in which causes may be readily identified and a considerable portion of the disease can theoretically be avoided [1]. Non-modifiable risk factors so far revealed by epidemiological studies include age, personal or family history of colorectal cancer or adenomatous polyps, and a personal history of chronic inflammatory bowel disease [26, 27]. All other factors listed below fall under the category of modifiable risk factor.
Age
Age can undoubtedly be regarded as the strongest non-modifiable risk factor for the development of CRC, the likelihood for the occurrence of CRC increases after the age of 40. According to Surveillance Epidemiology and End Results Cancer Statistics Review, reported between 1998 and 2002, 15 % or even lesser cases of CRC were diagnosed among persons below 54 years of age, 17 % among those who were between 55 and 64 years, 26.3 % were between 65 and 74 years, 29.2 % in among those between 75 and 84 years in age, and 12.6 % of fresh cases were those who were above 85 in age (http://seer.cancer.gov/csr/1975_2002/results_merged/topic_age_dist.pdf). When colon and rectal cancers are considered separately, over 50 % of new cases in each group still occur among those 65 to 84 years old (http://seer.cancer.gov/csr/1975_2002/results_merged/topic_age_dist.pdf). Studies have clearly proven that the rate of incidence of CRC is more than 50 times higher in persons aged 60 to 79 years than in those younger than 40 years [28, 29]. However, CRC now continuously appears to be increasing among younger persons [30, 31].
Not much study has been carried out on this malignancy in India, but what little data is available it suggests that the vast majority of patients with CRC are above the age of 65 years [32, 33]. CRC occurring before age of 40 years accounts for less than 10 % of the total colorectal cancer cases in India [34]. Data from Srinagar suggest that 68.7 % of the CRC patients have an age falling between 41 and 60 years at the time of diagnosis [35] and ASR is highest in the age group 55–59 years at 17.21/100,000 followed by the age group 65–69 years at 14.86/100 [25].
Sex
CRC is nowadays thought to be the third most common cancer among men (663,000 cases, 10.0 % of the total cancers) and the second among women (570,000 cases, 9.4 % of the total cases) worldwide [2, 36, 37]. Although majority of studies suggest that the incidence rates for cancer of the colon in both the sexes are similar, with a slight male predominance for rectal cancer [38–41]; in general, the incidence and mortality rates of CRC in USA are about 35 to 40 % higher among males than among females. The incidence rate of CRC between 2000 and 2004 was 69.2/100,000 population among men and 45.8/100,000 population among women of USA [27, 42].
In India, the male to female ratio of the occurrence of malignancies of the colon and rectum has been seen to be almost around unity for cancers of the colon but about 1.5 or larger for cancers involving the rectum [43]. According to Javid et al., colorectal carcinoma incidence is 8.77/100,000 in males and 7.66/100,000 in females in Kashmir [25].
Personal history of IBD
Patients having a history of inflammatory bowel disease (IBD) are at 4 to 20-fold risk of developing colorectal cancer [44]. IBD is a collective term for two diseases: ulcerative colitis (UC) and Crohn disease (CD). Ulcerative colitis induces inflammation of the mucosa of the colonic and rectal walls. Crohn disease induces inflammation of the full thickness of the bowel wall and may involve any part of the GIT beginning from the mouth to anus [38]. Actually, persons having IBD for years often are seen to develop dysplasia, which can change to cancer gradually.
Data suggests that the last 20 years have seen an increase in the occurrences of both UC and CD throughout Asia [45]. UC was the first among the two seen to emerge in developing countries; however, in the past two decades, CD has largely overtaken UC in incidence. Indian reports show of a UC/CD ratio of 8:1 (previously 10:1) [46]. Although IBD-CRC accounts for only 1–2 % of total cases of CRC, IBD with the involvement of the colon comes among the top 3 high-risk conditions for CRC [47].
Personal history of adenomatous polyps
Studies based on epidemiological data have shown that persons with a history of colorectal adenomatous polyps have higher chances of developing CRC than individuals with no previous history of adenomas [48]. The malignancy rates have been found higher for those with adenomas larger than 1 cm, having villous architecture and severe dysplasia [49–51]. In fact, data show that more than 70 % of CRC develop from sporadic adenomatous polyps; this is especially true if the polyps were large or if there were more than one [52].
A study carried out by Tony et al. shows that more than 90 % of polyps are located in the left colon in South Indians and that larger polyps are associated with severe degree of dysplasia [53].
Family history of colorectal cancer adenomatous polyps
According to Center for Disease Control and Prevention, people with a history of CRC or adenomatous polyps in one or more relatives are at an increased risk [38]. The risk is higher in people with a strong history of family, like a history of colorectal cancer or adenomatous polyps in any first-degree relative younger than age 60, or a history of colorectal cancer or adenomatous polyps in two or more first-degree relatives at any age [54]. The reasons for this although are not yet clear, but it seems that either inherited genes or shared environmental factors, or may be some combination of these, have got a role to play [38]. If these are looked into, large number of CRC cases can be theoretically prevented [1, 55, 56]
Diet
Dietary factors account for some 30 % of cancers in developed countries and about 20 % in developing countries [57]. A number of dietary factors have been linked to a higher risk of CRC and changes in food habit might reduce this burden up to an extent of 70 % [58]. In fact, the World Cancer Research Fund/American Institute for Cancer Research has prepared dietary recommendation list for prevention of cancers based on epidemiological evidence [39].
A typical “Western” diet is energy dense and consists of high intakes of red and processed meat; refined grains, potatoes, and sugar-containing foods; and less fruits and vegetables. Some studies have shown this dietary pattern to be positively associated with colorectal cancer [59–61]. Other commonly observed patterns include a “vegetable,” “prudent,” and the “healthy” diet, all of which are inversely related to CRC risk [62–64] that includes high intake of fruits and vegetables, fish and poultry, whole-grain products, and lowfat dairy products. A positive association with meat consumption that is stronger for colon cancer than rectal cancer has been documented [38, 65]. Potential underlying mechanisms for a such an association includes the presence of heme iron in red meat [38, 66, 67] and cooking at high temperature, which results in the production of heterocyclic amines and polycyclic aromatic hydrocarbons [67, 68], both of which are carcinogenic. Diets high in fat, animal fat in particular, are a major threat in CRC development, which favors the bacterial flora development, often capable of degrading bile salts to potentially carcinogenic N-nitroso compounds [1, 38, 65, 69]. On the contrary, large intake of fruits and vegetables, possessing dietary fiber, dilute fecal content, increase fecal bulk, and reduce transit time ultimately decreasing the risk [39]. Consumption of milk and other diets rich in vitamin D and calcium also decreases the risk of developing CRC [39, 70–73].
Micronutrient deficiency
Cereals, pulses, vegetables, fruits, spice, and other plant food have been shown to contain many micronutrients such as vitamins and minerals including phytochemicals, which have chemoprevention properties [74–76]. One of the hazards of alcohol consumption is that consumers of alcohol usually have diets low in essential nutrients, making tissues susceptible to carcinogenesis. Fruits and vegetables may protect against risk of CRC through their anti-carcinogenic components such as antioxidants like vitamins C and E, selenium, carotenoids folate, flavonoids, organosulphides, and isothiocyanates; vitamins C and E also protect against lipid peroxidation. Micronutrients like folate, vitamin B6, vitamin B12, and methionine have been reported to protect against cancer by preventing against aberrant DNA methylation patterns that are commonly seen in colorectal tumors [77–80]. The associations of micronutrients with colon and CRC cancer risk have been extensively studied in large epidemiological studies such as the Nurses Health Study and Health Professionals Follow-Up Study [79, 81] and the Cancer Prevention Study II [82]. Most evidence has confirmed the hypotheses of risk reduction due to adequate micronutrient intake. Calcium may reduce the risk of CRC by inducing apoptosis and binding bile and free fatty acids [83, 84], whereas both calcium and vitamin D may reduce epithelial cell proliferation.
Physical activity and obesity
Epidemiologic studies suggest that high levels of physical activity decrease the risk of colon cancer among men and women by possibly as much as 50 % [72]. Majority of the studies point towards a dose–response effect, which suggest that the frequency and intensity of physical activity is inversely associated with the risk [15, 48, 85, 86]. According to Haggar et al., the potential biological mechanism underlying the relationship is that sustained physical activity raises the rate of metabolism in the body, increasing gut motility, and maximal oxygen uptake [38, 39, 48], which in the longer term, increase the body’s metabolic efficiency together with the capacity, as well as reducing blood pressure and insulin resistance [86].
Obesity, suggested to be another factor associated with the risk of colorectal cancer, notably increases circulating estrogens and decreases insulin sensitivity, which in turn is believed to influence cancer risk [38]. The risk of CRC has been suggested to increase by an estimated 25 % in overweight men and 50 % in obese men [87, 88]. WHO has set forth a standard definition of each weight class based on BMI. A case–control study conducted by Caan et al. revealed males who had a BMI in the highest quintile were almost two times as likely to develop colon cancer as males with a BMI in the lowest quintile (OR = 1.96; 95 % CI 1.50–2.57). Females with a BMI in the highest quintile were approximately 1.5 times as likely to develop colon cancer when compared to females with BMIs in the lowest quintile (OR = 1.45; 95 % CI 1.08–1.94) [89].
Smoking and alcohol consumption
The International Agency for Research on Cancer concluded in November 2009 that tobacco smoking is the cause of CRC and that the association appears to be stronger for rectal than for colon cancer [27, 90–92]. A meta-analysis conducted by Botteri et al. based on 42 observational studies found that current smokers were at a much higher risk of developing adenomatous polyps than those who had never smoked (OR = 2.14; 95 % CI 1.86–2.46) [93]. Additionally, studies have shown that smokers have a greater risk of recurrent adenomas than nonsmokers [56]. Evidences also demonstrate an earlier average age of onset incidence of colorectal cancer among males and women who smoke cigarettes [94, 95].
Individuals who have a lifetime average of two to four alcoholic drinks per day have a 23 % higher risk of colorectal cancer than those who consume less than one drink per day [27]. Alcohol consumption is one of the factors responsible for the onset of colorectal cancer at a younger age [94, 95] as well as a disproportionate increase of tumors in the distal colon [96]. Reactive metabolites of alcohol such as acetaldehyde have been labeled as being carcinogenic [38, 97]; it interacts with smoking pathway. Alcohol also functions as a solvent, resulting in the increased penetration of other carcinogenic molecules into mucosal cells, and the effects of alcohol may be mediated through the generation of free radical oxygen species, lipid peroxidation, and production of prostaglandins [38, 97].
Conclusion and future course
This thing has continuously been given stress that the incident cases of colorectal cancer keep increasing in developing countries although developed countries have been able to control it in part by making its detection at an early stage possible. In order to tackle further the global issue of colorectal cancer and to reduce (loosen) its grip on these developing parts of the world as well, we need to unravel the complex synergistic effect of various environmental and dietary factors that fall in the group of modifiable and manageable risk factors by recognizing them in various parts through their exhaustive and thorough screening, thereby reducing the incidence of this disease in every part of world including our Kashmir that is unfortunately being named as “a valley of GIT cancers” now.
References
Boyle P, Langman JS. ABC of colorectal cancer. London: BMJ; 2001.
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917.
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics. Cancer J Clin. 2009;58:225–49.
Hawk ET, Levin B. Cancer prevention. J Clin Oncol. 2005;23:378–91.
Moghimi-Dehkordi B, Safaee A. An overview of colorectal cancer survival rates and prognosis in Asia. World J Gastrointest Oncol. 2012;4:71–5.
Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2007;18:581–92.
New Zealand Health Information Service. Cancer: new registrations and deaths: 1993. Wellington: Ministry of Health; 1997.
Willet W et al. Relation of meat, fat and fiber intake to the risk of colon cancer in a prospective study among women. N Engl J Med. 1990;13(323):1664–72.
Sung JJ et al. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol. 2005;6:871–6.
Yee YK, Tan VP, Chan P, Hung IF, Pang R, Wong BC. Epidemiology of colorectal cancer in Asia. J Gastroenterol Hepatol. 2009;24:1810–6.
Cheung DY, Kim TH, Kim CW, Kim JI, Cho SH, Park SH, et al. The anatomical distribution of colorectal cancer in Korea: evaluation of the incidence of proximal and distal lesions and synchronous adenomas. Int Med. 2008;47:1649–54.
Ji BT, Devesa SS, Chow WH, Jin F, Gao YT. Colorectal cancer incidence trends by subsite in urban Shanghai, 1972–1994. Cancer Epidemiol Biomark Prev. 1998;7:661–6.
Yiu HY, Whittemore AS, Shibata A. Increasing colorectal cancer incidence rates in Japan. Int J Cancer. 2004;109:777–81.
Curado MP, Edwards B, Shin HR, et al. Cancer incidence in five continents, volume IX. IARC Scientific Publication, no 160 IARC, Lyon 2004. Int J Cancer. 2007;109:777–81.
Yeole BB, Sunny L, Swaminathan R, Sankaranarayanan R, Parkin DM. Population-based survival from colorectal cancer in Mumbai, (Bombay) India. Eur J Cancer. 2001;37:1402–8.
Ghazali AK, Musa KI, Naing NN, Mahmood Z. Prognostic factors in patients with colorectal cancer at Hospital University Sains Malaysia. Asian J Surg. 2010;33:127–33.
National Cancer Registry Programme. http://www.icmr.nic.in/ncrp/cancer_reg.htm. Accessed 4 Nov 2010.
Swaminathan R, Selvakumaran R, Esmy PO, et al. Cancer pattern and survival in a rural district in South India. Cancer Epidemiol. 2009;33:325–31.
Rastogi T, Devesa S, Mangtani P, et al. Cancer incidence rates among South Asians in four geographic regions: India, Singapore, UK and US. Int J Epidemiol. 2008;37:147–60.
Ali R, Barnes I, Kan SW, Beral V. Cancer incidence in British Indians and British whites in Leicester, 2001–2006. Br J Cancer. 2010;103:143–8.
Miller AB, Chu KC, Hankey BF, Ries LAG. Cancer incidence and mortality patterns among specific Asian and Pacific Islander populations in the U.S. Cancer Causes Control. 2008;19:227–56.
Cunningham D, Atkin W, Lenz HJ, et al. Colorectal cancer. Lancet. 2010;375:1030–47.
Murtaza I, Mushtaq D, Margoob MA, Dutt A, et al. A study on p53 gene alterations in esophageal squamous cell carcinoma and their correlation to common dietary risk factors among population of the Kashmir Valley. World J Gastroenterol. 2006;12:4033–7.
Rasool MT, Lone MM, Wani ML, Afroz F, Zaffar S, Mohib-ul Haq M. Cancer in Kashmir, India: burden and pattern of disease. J Can Res Ther. 2012;8:243–6.
Javid G, Zargar SA, Rather S, Khan AR, Khan BA, Yattoo GN, et al. Incidence of colorectal cancer in Kashmir Valley, India. Indian J Gastroenterol. 2011;30(1):7–11.
Popek S, Tsikitis VL. Colorectal cancer: a review. Onclive; 2011, pp. 1–6.
American Cancer Society. Colorectal Cancer Facts & Figures 2011–2013. Atlanta: American Cancer Society; 2011.
Ries LAG, Melbert D, Krapcho M, et al. SEER cancer statistics review, 1975–2005. Bethesda: National Cancer Institute; 2008.
American Cancer Society. Colorectal cancer facts & figures special edition 2005. Oklahoma City: American Cancer Society; 2005.
O’Connell JB, Maggard MA, Liu JH, et al. Rates of colon and rectal cancers are increasing in young adults. Am Surg. 2003;2003(69):866–72.
O’Connell JB, Maggard MA, Livingston EH, Yo CK. Colorectal cancer in the young. Am J Surg. 2004;187(3):343–8.
Curado MP, Edwards B, Shin HR, et al. (eds). Cancer incidence in five continents, volume 9. Lyon: IARC; 2007. IARC Scientific Publication, no 160
Mohandas KM, Desai DC. Epidemiology of digestive tract cancers in India. V. Large and small bowel. Indian J Gastroenterol. 1999;18:118–21.
Zafar SY, Abernethy AP, Abbott DH, et al. Comorbidity, age, race and stage at diagnosis in colorectal cancer: a retrospective, parallel analysis of two health systems. BMC Cancer. 2008;8:345.
Shah A, Wani NA. A study of colorectal adenocarcinoma. Indian J Gastroenterol. 1991;10:12–3.
Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108.
Parkin DM. International variation. Oncogene. 2004;23:6329–40.
Haggar FA, Boushey RP. Colorectal cancer epidemiology: incidence, mortality, survival, and risk factors. Clin Colon Rectal Surg. 2009;22:191–7.
World Cancer Research Fund/American Institute for Cancer Research. Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Washington, DC: World Cancer Research Fund/American Institute for Cancer Research; 2007.
Thygesen LC, Gronbaek M, Johansen C. Colorectal cancer in Denmark 1943–1997. Dis Colon Rectum. 2004;47:1232–41.
Trifan A, Cojocariu C, Sfarti C, et al. Colorectal cancer in Romania: epidemiological trends. Rev Med Chir Soc Med Nat Iasi. 2006;110:533–9.
Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96.
Yeole BB. Trends in cancer incidence in esophagus, stomach, colon, rectum and liver in males in India. Asian Pac J Cancer Prev. 2008;9:97–100.
Janout V, Kolla’rova H. Epidemiology of colorectal cancer. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2001;145:5–10.
Goh KL. Inflammatory bowel disease: incidence and prevalence across Asia. In: Emerging issues in inflammatory bowel diseases, Falk Symposium 151, 3–11, Springer, 2006.
World Gastroenterology Organisation Global Guidelines. Inflammatory bowel disease: a global perspective June 2009.
Mattar MC, Lough D, Pishvaian MJ, Charabaty A. Current management of inflammatory bowel disease and colorectal cancer. Gastrointest Cancer Res; 2011 4(2):53–61. my GCRonline.org.
de Jong AE, Morreau H, Nagengast FM, et al. Prevalence of adenomas among young individuals at average risk for colorectal cancer. Am J Gastroenterol. 2005;100(1):139–43.
O’ Brein MJ, Winawe SJ, Zauber AG, et al. The National Polyp Study. Patient and polyp characteristics associated with high grade dysplasia in colorectal adenomas. Gastroenterology. 1990;98:371–9.
Jass JR. Do all colorectal carcinomas arise in preexisting adenomas. World J Surg. 1989;13:45–51.
Schuman BM, Sinsek H, Lyons RC. The association of multiple colonic adenomatous polyps with cancer of colon. Am J Gastroenterol. 1990;85:846–9.
Schatzkin A, Freedman LS, Dawsey SM, Lanza E. Interpreting precursor studies: what polyp trials tell us about large-bowel cancer. J Natl Cancer Inst. 1994;86(14):1053–7.
Tony J, Harish K, Ramachandran TM, Sunilkumar K, Thomas V. Profile of colonic polyps in a southern Indian population. Indian J Gastroenterol. 2007;26:127–9.
Boardman LA, Morlan BW, Rabe KG, et al. Colorectal cancer risks in relatives of young-onset cases: is risk the same across all first-degree relatives? Clin Gastroenterol Hepatol. 2007;5(10):1195–8.
Johnson IT, Lund EK. Review article: nutrition, obesity and colorectal cancer. Aliment Pharmacol Ther. 2007;26(2):161–81.
Heavey PM, McKenna D, Rowland IR. Colorectal cancer and the relationship between genes and the environment. Nutr Cancer. 2004;2:124–41.
Rasool S, Ganai BA, Sameer AS, Masood A. Esophageal cancer: associated factors with special reference to the Kashmir Valley. Tumori. 2012;98:191–203.
Willett WC. Diet and cancer: an evolving picture. J A M A. 2005;293(2):233–4.
Williams CD, Satia JA, Adair LS, Stevens J, Galanko J, Keku TO, RS Sandler. Dietary patterns, food groups, and rectal cancer risk in whites and african-americans. Cancer Epidemiol Biomarkers Prev 2009;1552–61.
Kim MK, Sasaki S, Otani T, Tsugane S. Dietary patterns and subsequent colorectal cancer risk by subsite: a prospective cohort study. Int J Cancer. 2005;115(5):790–8.
Kesse E, Clavel-Chapelon F, Boutron-Ruault MC. Dietary patterns and risk of colorectal tumors: a cohort of French women of the National Education System(E3N). Am J Epidemiol. 2006;164(11):1085–93.
Slattery ML, Boucher KM, Caan BJ, Potter JD, Ma KN. Eating patterns and risk of colon cancer. Am J Epidemiol. 1998;148(1):4–16.
Dixon LB, Balder HF, Virtanen MJ, Rashidkhani B, Mannisto S, Krogh V, et al. Dietary patterns associated with colon and rectal cancer: results from the Dietary Patterns and Cancer (DIETSCAN) Project. Am J Clin Nutr. 2004;80:1003–11.
Terry P, Hu FB, Hansen H, Wolk A. Prospective study of major dietary patterns and colorectal cancer risk in women. Am J Epidemiol. 2001;154(12):1143–9.
Larsson SC, Wolk A. Meat consumption and risk of colorectal cancer: a meta-analysis of prospective studies. Int J Cancer. 2006;119(11):2657–64.
Santarelli RL, Pierre F, Corpet DE. Processed meat and colorectal cancer: a review of epidemiologic and experimental evidence. Nutr Cancer. 2008;60(2):131–44.
Kabat GC, Miller AB, Jain M, Rohan TE. A cohort study of dietary iron and heme iron intake and risk of colorectal cancer in women. Br J Cancer. 2007;97(1):118–22.
Sinha R. An epidemiologic approach to studying heterocyclic amines. Mutat Res. 2002;506–507:197–204.
Sinha R, Chow WH, Kulldorf M, et al. Well done, grilled red meat increase the risk of colorectal adenomas. Cancer Res. 1999;59:4320–4.
Cho E, Smith-Warner SA, Spiegelman D, et al. Dairy foods, calcium, and colorectal cancer: a pooled analysis of 10 cohort studies. J Natl Cancer Inst. 2004;96(13):1015–22.
Chan AT, Giovannucci EL. Primary prevention of colorectal cancer. Gastroenterology. 2010;138(6):2029–43. e2010.
IARC Working Group on Vitamin D. Vitamin D and cancer: a report of the IARC Working Group on Vitamin D. Lyon, IARC; 2008.
Jenab M, Bueno-de-Mesquita HB, Ferrari P, et al. Association between pre-diagnostic circulating vitamin D concentration and risk of colorectal cancer in European populations: a nested case–control study. BMJ. 2010;340:b5500.
Nooyi SC, Murthy NS, Shivananjaiah S, Sreekantaiah P, Mathew A. Trends in rectal cancer incidence—Indian scenario. Asian Pac J Cancer Prev. 2011;12:2001–6.
WCRF and AICR. Food, nutrition and the prevention of cancer: a global perspective. Washington, DC: World Cancer Research Fund and American Institute for Cancer Research; 1997.
Mathew A, Peters U, Chatterjee N, Kulldorff M, Sinha R. Fat, fibre, fruits, vegetables and risk of colorectal adenomas. Int J Cancer. 2004;108:287–92.
Borek C. Dietary antioxidants and human cancer. Integr Cancer Ther. 2004;3(4):333–41.
Kovacic P, Jacintho JD. Mechanisms of carcinogenesis: focus on oxidative stress and electron transfer. Curr Med Chem. 2001;8(7):773–96.
Feinberg AP, Vogelstein B. Alterations in DNA methylation in human colon neoplasia. Semin Surg Oncol. 1987;3(3):149–51.
Timbo BB, Ross MP, McCarthy PV, Lin CT. Dietary supplements in a national survey: prevalence of use and reports of adverse events. J Am Diet Assoc. 2006;106(12):1966–74.
Freudenheim JL, Graham S, Marshall JR, Haughey BP, Wilkinson G. A case–control study of diet and rectal cancer in western New York. Am J Epidemiol. 1990;131(4):612–24.
Murtaugh MA, Ma KN, Benson J, Curtin K, Caan B, Slattery ML. Antioxidants, carotenoids, and risk of rectal cancer. Am J Epidemiol. 2004;159(1):32–41.
Chang D, Wang F, Zhao YS, Pan HZ. Evaluation of oxidative stress in colorectal cancer patients. Biomed Environ Sci. 2008;21(4):286–9.
Machlin LJ, Bendich A. Free radical tissue damage: protective role of antioxidant nutrients. FASEB J. 1987;1(6):441–5.
Samad AK, Taylor RS, Marshall T, Chapman MA. A meta-analysis of the association of physical activity with reduced risk of colorectal cancer. Colorectal Dis. 2005;7(3):204–13.
Lee KJ, Inoue M, Otani T, Iwasaki M, Sasazuki S, Tsugane S, et al. Physical activity and risk of colorectal cancer in Japanese men and women: the Japan Public Health Center-based prospective study. Cancer Causes Control. 2007;18(2):199–209.
Renehan AA. Body mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Am J Epidemiol. 2000;152(9):847–54.
Moghaddam AA. Obesity and risk of colorectal cancer: a meta-analysis of 31studies with 70,000 events. Cancer Epidemiol Biomark Prev. 2007;16(12):2533–47.
Caan BJ, Coates AO, Slattery ML, et al. Body size and the risk of colon cancer in a large case–control study. Int J Obes. 1998;22:178–84.
Secretan B, Straif K, Baan R, et al. A review of human carcinogens—part E: tobacco, areca nut, alcohol, coal smoke, and salted fish. Lancet Oncol. 2009;10(11):1033–4.
Paskett ED, Reeves KW, Rohan TE, et al. Association between cigarette smoking and colorectal cancer in the Women’s Health Initiative. J Natl Cancer Inst. 2007;99(22):1729–35.
Liang PS, Chen TY, Giovannucci E. Cigarette smoking and colorectal cancer incidence and mortality: systematic review and meta-analysis. Int J Cancer. 2009;124(10):2406–15.
Botteri E, Iodice S, Raimondi S, et al. Cigarette smoking and adenomatous polyps: a meta-analysis. Gastroenterology. 2008;2:388–95.
Zisman AL, Nickolov A, Brand RE, Gorchow A, Roy HK. Associations between the age at diagnosis and location of colorectal cancer and the use of alcohol and tobacco: implications for screening. Arch Intern Med. 2006;166(6):629–34.
Tsong WH, Koh WP, Yuan JM, Wang R, Sun CL, Yu MC. Cigarettes and alcohol in relation to colorectal cancer: the Singapore Chinese Health Study. Br J Cancer; 2007;96(5):821–7.
Bazensky I, Shoobridge-Moran C, Yoder LH. Colorectal cancer: an overview of the epidemiology, risk factors, symptoms, and screening guidelines. Medsurg Nurs. 2007;16(1):46–51.
Pöauthornameschl G, Seitz HK. Alcohol and cancer. Alcohol Alcohol. 2004;39(3):155–65.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rasool, S., Kadla, S.A., Rasool, V. et al. A comparative overview of general risk factors associated with the incidence of colorectal cancer. Tumor Biol. 34, 2469–2476 (2013). https://doi.org/10.1007/s13277-013-0876-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-013-0876-y