
Abstract
Objective
To prospectively examine the association between physical activity and the risk of developing colorectal cancer in a large population-based cohort study of Japanese men and women, and to investigate whether the effects of physical activity on colorectal cancer risk differ by sex and subsite.
Methods
We analyzed data from a population-based cohort of 65,022 subjects. A total of 486 incident colorectal cancers (154 proximal colon, 166 distal colon and 149 rectal cancers) was identified during 6 years of follow-up.
Results
We observed a significant inverse association between physical activity and the risk of developing colorectal cancer, particularly colon cancer, among men. Relative to men in the lowest level of metabolic equivalent (MET) hours per day, those in the highest level had a RR of 0.69 (95% CI = 0.49–0.97). A significant decrease in risk of colorectal cancer was associated with increasing MET hours per day among men. This inverse association was essentially limited to colon cancer. A significant decrease in risk with increasing MET-hour score was observed predominantly for proximal colon cancer among men. In contrast, no significant decrease was seen among women.
Conclusion
These findings suggest that physical activity may prevent colon cancer among Japanese men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer is the second most frequent cancer and the second most common cause of cancer death in more developed countries, with nearly 945,000 new cases diagnosed worldwide each year and 492,000 deaths [1]. In Japan, the incidence and mortality of colorectal cancer has recently increased, and it is now a leading cause of morbidity and mortality, with about 36,000 deaths in 2000 [2].
Although the role of physical activity in the etiology of colorectal carcinogenesis has drawn interest, results from epidemiological studies have been inconsistent. No randomized controlled trials of physical activity as a means of primary prevention of colorectal cancer have been published, but prospective studies have noted a consistent association between increased physical activity and lower risk of colon cancer among men [3–17]. In contrast, results from studies in women have been less consistent. Further, results for subsite-specific associations between physical activity and colorectal cancer have also been inconsistent, although few prospective studies have reported on physical activity and colorectal cancer by anatomical subsite [9–11, 17]. To date, moreover, no prospective results have been obtained in Japan [18, 19].
Here, we prospectively examined the association between physical activity and risk of developing colorectal cancer in a large population-based prospective study of Japanese men and women. We further investigated whether the effects of physical activity on colorectal cancer risk differed by sex and subsite.
Material and methods
Study population
The basis for this investigation lies with the Japan Public Health Center-based Prospective Study (JPHC Study), which was established in 1990 for Cohort I and in 1993 for Cohort II, and included questions on physical activity. Cohort I included those residents aged 40–59 years who had registered their addresses in five public health center (PHC) areas (Ninohe (Iwate Prefecture), Yokote (Akita Prefecture), Saku (Nagano Prefecture), Chubu (Okinawa Prefecture), and Katsushika (metropolitan Tokyo)), and Cohort II included those aged 40–69 years who had registered in six PHC areas (Mito (Ibaraki Prefecture), Nagaoka (Nigata Prefecture), Chuohigashi (Kochi Prefecture), Kamigoto (Nagasaki Prefecture), Miyako (Okinawa Prefecture) and Suita (Osaka Prefecture, including two cohorts)). Details of the study design have been provided elsewhere [20]. The study protocol was approved by the institutional review board of the National Cancer Center, Japan. For the present analysis, the Katsushika PHC area (metropolitan Tokyo) cohort and one of the two cohorts in the Suita PHC area were defined differently, and were therefore excluded because the population was aged 40 or 50 years at baseline and selected based on having been invited to undergo a comprehensive health check-up program conducted by the city government.
The 5-year follow-up survey, which included more comprehensive information on physical activity than the baseline survey, was conducted in 1995 for Cohort I and in 1998 for Cohort II. For the present study, therefore, we regarded the 5-year follow-up survey as the baseline, and sourced information on exposures from this survey, while follow-up time was counted from this 5-year follow-up survey to the end of the follow-up period, namely 2002.
A total of 99,808 subjects were identified as the study population. Of these, 19 were found to be ineligible during the follow-up period and excluded owing to non-Japanese nationality (n = 11) and late report of emigration before the start of the follow-up period (n = 8). As a result, a population-based cohort of 99,789 subjects was established.
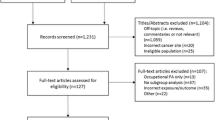
The self-administered follow-up questionnaire included items on socio-demographics, personal medical history, physical activity, smoking and alcohol drinking habits and diet by a food-frequency questionnaire of 138 items. A total of 83,487 subjects responded, giving a response rate of 84%. Excluded from the study were those who reported a history of cancer (e.g., colorectal, gastric, lung, liver, breast, uterine, and other cancer) (n = 1,205), were diagnosed with cancers (n = 959) or were censored (n = 1,274) before the start of the follow-up survey, or reported missing data for physical activity (n = 15,027). Finally, 65,022 eligible subjects (29,842 men and 35,180 women) were included in the analysis.
Follow-up
Subjects were followed from the 5-year follow-up survey until December 31, 2002. Residence status was confirmed annually through the residential registry maintained by the respective study area municipality; for those who moved out of the area, residence status was confirmed through the municipal office of the area to which they had moved. The occurrence of cancer was identified by active patient notification from major local hospitals in the study area and data linkage with population-based cancer registries, with permission from each of the local governments responsible for the cancer registries. Death certificate information was used as a supplementary information source. The site and histology of each case were coded using the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) [21].
As of December 2002, a total of 486 cases of newly diagnosed colorectal cancer were identified during the follow-up period based on ICD-O-3 (code: C18-C20). Subsite-specific analyses were conducted as follows: C180-C189 for colon cancer; C180-C185 for proximal colon cancer; C186 and C187 for distal colon cancer; and C199 and C209 for rectal cancer. Finally, 65,022 subjects (29,842 men and 35,180 women) were used for analysis, including 154 cases of proximal colon cancer, 166 of distal colon cancer and 149 of rectal cancer. In our cancer registry system, 5.5% of incident cases of colorectal cancer were notified by death certificate (Death Certificate Notification, DCN); 2.2% had no information other than death certificates (Death Certificate Only, DCO); and 94.7% were verified by histological examination (Histological Verification, HV).
Assessment of physical activity
The self-administered follow-up questionnaire included a section on physical activity. Subjects reported the average time per day spent for each of the following activities: heavy physical work or strenuous exercise (assigning the value of 0 for “none,” 0.5 for “less than 1 h,” and 3 for “1 h and more”), sedentary activity (1.5 for “less than 3 h,” 5.5 for “3–8 h,” and 7.5 for “more than 8 h”), and walking or standing (0.5 for “less than 1 h,” 2 for “1–3 h,” and 8.5 for “more than 3 h”) [unpublished data, Fujii H et al.].
Metabolic equivalent (MET) hours per day were estimated by multiplying the reported time spent at each activity per day by its assigned MET intensity [22]: heavy physical work or strenuous exercise (4.5), walking or standing (2.0), sedentary (1.5), and sleep or others (1.0). After summing across all activities, subjects were grouped into four exposure levels by quartiles of MET-hour score. The validity of MET-hour score was assessed using 110 volunteer samples (55 men and 55 women) from the cohort using a 4-day 24-h physical activity record (Sunday, or another day off if Sunday was a workday, plus three weekdays. The mean MET-score for physical activity obtained from the self-report was 35.5 in men and 34.4 in women and that from the 24-h physical activity record was 39.5 in men and 40.6 in women. Energy expenditure estimated in METs showed little difference by gender or area (p > 0.05). The rank correlation coefficient between MET-hour score and physical activity records was 0.64 (p < 0.0001) [unpublished data, Fujii H et al.]. We further examined gradients in hours per day (less than 3 h, or more) spent at walking or standing as well as gradients in hours (none, or yes) spent at heavy physical work or strenuous exercise.
Statistical analysis
Person-years were counted from the date of response to the follow-up survey until one of the following endpoints: the date of occurrence of colorectal cancer, the date of emigration from the study area, the date of death, or the end of the study period, whichever came first. Persons who were lost to follow-up were censored on the last confirmed date of their presence in the study area.
Incident cases of colorectal cancer were the main outcome measure. In addition, to estimate the incidence rate of invasive colorectal cancer, incident cases invading over the mucosal layer were considered as invasive cancer cases according to the depth of tumor invasion.
Relative risk (RR) and 95% confidence intervals (95% CI) were used to describe the RR of colorectal cancer incidence associated with physical activity. Subgroup analyses were done to investigate the relation of physical activity in men and women. Additional subsite-stratified analyses were done to examine associations with physical activity, and their respective RRs were estimated. Subgroup analyses stratified by body mass index (BMI) were also done and their respective RRs were estimated.
Cox proportional hazards modeling was used to examine the association between physical activity and the risk of developing colorectal cancer, with person-years of follow-up as time scale. The assumptions for the Cox proportional hazards model were checked and found to hold. We adjusted for age at the follow-up survey (continuous) and study area (10 PHC areas), and then additionally adjusted for a family history of colorectal cancer (yes or no), smoking status (never, former, or current), alcohol intake (none, occasional, or regular), and BMI (in quartiles). Further adjustment was made for intake of energy-adjusted dietary fiber (in quartiles), total folate (in quartiles) and red meat (in quartiles). These variables are either known or suspected risk or preventive factors for colorectal cancer [20, 23–30]. Additional adjustment for intake of energy-adjusted total calcium and vitamin D produced no appreciable change in the results and these variables were excluded from the final model. The significance of interactions between physical activity and these risk factors for colorectal cancer was determined by comparing the model of physical activity × the respective variable with the model that assessed the main effect only. The likelihood ratio test was used to assess statistical interaction. Statistical analyses were performed using SAS version 9.1 (SAS Institute, Inc., Cary, NC, USA). We used the median of each category as a continuous variable to calculate the tests for trend; P values for these tests were two-sided and considered significant at 0.05.
Results
During 6 years of follow-up (average follow-up period: 5.8 years) for 65,022 subjects (29,842 men and 35,180 women), a total of 486 cases of colorectal cancer (306 invasive and 180 in-situ) developed over 374,779 person-years. Mean age at the follow-up survey was 56.9 years among men and 57.2 years among women. Characteristics of study subjects according to level of physical activity are shown in Table 1. The MET-hour scores—the sum of the average time per day spent in each physical activity multiplied by the MET value for each study—for the 4 groups, the lowest, the second, the third and the highest were 28.25, 33.25, 35.25 and 43.75 in men and 28.50, 33.25, 35.25 and 43.75 in women, respectively. Men who were more physically active were more likely to report greater consumption of total folate, fiber, vitamin D, and calcium than men who were less physically active, but to have higher current smoking and regular drinking and greater consumption of daily mean energy, total fat, and red meat. No difference in mean age and BMI was observed between the groups by physical activity level. Similar trends were found for women (Table 1).
Associations between hours of physical activity and risk of incident colorectal cancer by type of activity in men and women are presented in Table 2. Those who reported vigorous physical activity had a 15% lower risk of colorectal cancer compared with those reporting none in men (RR = 0.85; 95% CI = 0.67–1.08), although this difference was not statistically significant. A statistically significant decrease was limited to colon cancer in men (RR = 0.73; 95% CI = 0.55–0.98). Moreover, a greater decrease was seen in risk for cancer of the proximal colon among men (RR = 0.43; 95% CI = 0.26–0.70). However, women who reported vigorous physical activity were not at lower risk of colorectal cancer. Analysis for men and women combined showed a significant decrease in risk of proximal colon cancer (RR = 0.57; 95% CI = 0.39–0.83).
Those who reported more than 3 h per day of walking or standing had a 18% lower risk of colorectal cancer than those reporting less than 3 h among men, although this difference was not statistically significant (RR = 0.82; 95% CI = 0.64–1.05). A significant decrease in risk of proximal colon cancer was observed in men (RR = 0.62; 95% CI = 0.40–0.98). However, no significant association was observed among women (Table 2).
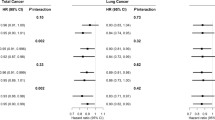
Table 3 shows the RR of colorectal cancer by physical activity level in men and women. Compared with men in the lowest level of MET hours per day, those in the highest level had a RR of 0.69 (95% CI = 0.49–0.97). A statistically significant decrease in risk of colorectal cancer was associated with increasing MET hours per day among men (P for trend = 0.022). This inverse association was essentially limited to colon cancer among men. A significant decrease in risk with increasing MET hours per day was observed predominantly in cancer of the proximal colon; men in the highest level were approximately 70% less likely to develop cancer at this site than those in the lowest level (RR = 0.29; 95% CI = 0.14–0.60; p for trend <0.001). No significant trend was found for rectal cancer. The same analyses in women showed a non-significant inverse association between physical activity and the risk of developing colon cancer (Table 3). There was no appreciable difference between the results in Tables 2 and 3 with and without adjustment for BMI.
Additional analysis stratified by BMI was investigated in relation to the risk of colorectal cancer among men and women (Table 4). Men categorized with both a BMI of less than 25 kg/m2 and a high level of physical activity had a significantly decreased risk for colorectal cancer relative to those with a low level of physical activity (RR = 0.54; 95% CI = 0.36–0.82). A statistically significant decrease in risk of colorectal cancer was associated with increasing MET hours per day in men with a BMI of less than 25 kg/m2 (P for trend = 0.004). This significant association was also noted for colon cancer. Moreover, the inverse association was seen predominantly in the risk of proximal colon cancer (RR = 0.23; 95% CI = 0.10–0.53; p for trend <0.001). Men categorized with a BMI of greater than 25 kg/m2 and a lower level of physical activity had a significantly increased risk of rectal cancer (RR = 3.37; 95% CI = 1.07–10.65), but no trend was seen. Further, no significant association was observed in any other site among men with a BMI of greater than 25 kg/m2. On the other hand, no significant associations were observed among women. We assessed the interaction of BMI and physical activity in men and women. No statistically significant interaction was observed (in men: p = 0.63 for colon, p = 0.23 for rectum; in women: p = 0.18 for colon, p = 0.58 for rectum). These stratified analyses were repeated after additional adjustment for BMI as a continuous variable, but the results were essentially unchanged (data not shown).
We also conducted additional analyses restricted to 306 cases of invasive colorectal cancer. Among men, the inverse association was slightly strengthened: those in the highest level of MET hours per day had a nearly 50% lower risk of colon cancer than those in the lowest (RR = 0.51; 95% CI = 0.30–0.85; p for trend = 0.005) (data not shown).
To avoid potential bias due to preclinical conditions, we performed further analyses after excluding colorectal cancer cases diagnosed during the first year of follow-up. The tendencies were essentially unchanged after this exclusion. However, the inverse association was slightly strengthened among women. We observed a significantly decreased risk of proximal colon cancer with increasing MET hours per day in women as well as in men, although the number of cases was small (for women, RR = 0.32; 95% CI = 0.11–0.95; p for trend = 0.037; for men, RR = 0.31; 95% CI = 0.14–0.66; p for trend = 0.001).
Discussion
In this large population-based prospective study of Japanese men and women, we found a significant inverse association between physical activity and the risk of developing colorectal cancer, particularly colon cancer, among men. Increasing levels of physical activity were associated with a significantly lower risk of colon cancer among men. In contrast, no significant associations were found among women. To our knowledge, the present results from the JPHC Study represent the first prospective study of the association between physical activity and colorectal cancer in Japan.
Previous studies [3–7, 13–15, 17] of men have found a statistically significant 40% lower risk of colorectal cancer among the most active compared with the least active subjects, whereas others have not [8, 10–12, 16]. Studies of women have shown a non-significant 10–20% lower risk with increased physical activity [3–5, 8, 10, 11, 13, 14, 17], although these results have also been inconsistent. However, the majority of these studies did not include a comprehensive evaluation of potential confounders such as lifestyle factors and dietary habits.
The present study showed a significant dose-response relationship between decreasing colorectal cancer risk and increasing MET hours per day of physical activity among men. This dose–response relationship has been reported by some but not all prospective studies. Whereas previous studies generally showed lower risk with increasing physical activity, three studies of men reported a significant dose–response relationship between increased physical activity and lower risk of colon cancer [5, 9, 14].
Few prospective studies have investigated physical activity and colon cancer by anatomical subsite [9–11, 17], and results have been inconsistent; two found a stronger inverse association between physical activity and distal colon cancer [9, 11], whereas others reported no difference by subsite in men and a stronger inverse association with proximal colon cancer in women [10], and an inverse association in men and women combined [17]. The lack of association between physical activity and rectal cancer in the present study is consistent with previous prospective studies, which have generally reported null results [6, 10].
Several potential biological mechanisms may contribute to the protective effect on physical activity and risk of colorectal cancer observed here, including hyperinsulinemia, obesity, change in prostaglandin ratio, lowered bile acid secretion and possibly enhanced immune function. Previous reports showed that subjects with colorectal cancer or polyps had higher levels of colonic mucosal prostaglandin (PG) E2 than control subjects, suggesting that prostaglandins are involved in proliferation and metastasis. Previous studies reported that increased physical activity had an inverse association, lowering PG E2, and also increasing PG F2α in relation to an increase in gut motility [19, 31, 32]. It is also possible that physical activity decreases stool transit time by stimulating colonic peristalsis, resulting in decreased exposure of the intestinal epithelium to potential carcinogens or mutagens. Physical activity may increase colon blood flow, causing the transporting away of potential carcinogens or mutagens from the mucous membrane [19, 31–34].
One finding of interest was the stronger decrease in risk of proximal colon cancer than of distal colon cancer among the most active compared with the least active subjects. These findings are consistent with some [10, 17] but not all previous prospective studies [9, 11]. One possible hypothesis might be that physical activity modifies metabolic hormone levels and growth factors and that the modification of these factors may influence developing cancer of the proximal rather than distal colon. It is also possible that physical activity affects gut motility more extensively in the proximal than the distal colon [10]. Further investigation of this question is required.
Another concern of this study was gender difference. We observed a non-significant decrease in the risk of colon cancer among women. Consistent with the findings in men, moreover, this decrease was seen predominantly in proximal colon cancer. Although we cannot rule out potentially true differences in the metabolic response to physical activity between men and women, it seems possible that misclassification of physical activity may have contributed to the non-significant findings in women, arising from a lack of detailed questions related to housework and a greater variability in physical activity at home than at work [8, 10, 11, 14]. On this basis, therefore, the present findings appear to show no marked gender difference in the influence of physical activity on colorectal cancer.
In addition, we found a statistically significant inverse association between physical activity and colorectal cancer risk among men with a BMI of less than 25 kg/m2, but not among those with a greater BMI. The reason for the null finding in this latter group is unclear, but may be attributable to the smaller number of subjects, at least in part. A second possibility is that a protective effect of physical activity on risk may have been weaker than the impact of BMI among those with a BMI greater than 25 kg/m2.
The main limitation of this study was its use of self-reports. However, because the data were collected before diagnosis, any imprecision was likely to have caused underestimation of associations rather than overestimation. More importantly, the accuracy of the self-reported physical activity questions used in the present study has been validated [unpublished data, Fujii H et al.]. The proportion of subjects excluded due to missing data for physical activity (18%) was relatively high. However, the characteristics of subjects with and without missing information did not differ. Although unmeasured confounders may not have been controlled in this study, lifestyle factors and dietary habits identified as potential confounding factors possibly associated with colorectal cancer in previous reports were accounted for [20, 23–30], with the expectation that statistical adjustment might be to some degree possible if information on associated variables were available.
Notwithstanding the known limitations of observational studies, the present study has the following strengths: it was a prospective population-based study with a 6-year follow-up period; information on physical activity was collected before the subsequent onset of cancer, eliminating the exposure recall bias inherent to case–control studies; study subjects were selected from the general population, and response rate to the questionnaire was high while the proportion of losses to follow-up was negligible; and finally, adjustment was made for lifestyle factors and dietary habits identified as possibly associated with colorectal cancer in previous reports [20, 23–30].
In conclusion, we observed a significant inverse association between physical activity and the risk of developing colorectal cancer, particularly colon cancer, among men. A stronger inverse association was noted for proximal than for distal colon cancer. These findings suggest that physical activity may prevent colon cancer among Japanese mssen.
References
Stewart BW, Kleihues P (eds) (2003) World cancer report. IARC Press, Lyon
Tajima K, Kuroishi T, Oshima A (eds) (2004) Cancer mortality and morbidity statistics: Japan and the World 2004. Japanese cancer association Gann Monograph on Cancer Research No. 51. Japan Scientific Societies Press, Tokyo
Wu AH, Paganini-Hill A, Ross RK, Henderson BE (1987) Alcohol, physical activity and other risk factors for colorectal cancer: a prospective study. Br J Cancer 55(6):687–694
Gerhardsson M, Floderus B, Norell SE (1988) Physical activity and colon cancer risk. Int J Epidemiol 17(4):743–746
Ballard-Barbash R, Schatzkin A, Albanes D et al (1990) Physical activity and risk of large bowel cancer in the Framingham Study. Cancer Res 50(12):3610–3613
Lee IM, Paffenbarger RS Jr, Hsieh C (1991) Physical activity and risk of developing colorectal cancer among college alumni. J Natl Cancer Inst 83(18):1324–1329
Thun MJ, Calle EE, Namboodiri MM et al (1992) Risk factors for fatal colon cancer in a large prospective study. J Natl Cancer Inst 84(19):1491–1500
Bostick RM, Potter JD, Kushi LH et al (1994) Sugar, meat, and fat intake, and non-dietary risk factors for colon cancer incidence in Iowa women (United States). Cancer Causes Control 5(1):38–52
Giovannucci E, Ascherio A, Rimm EB, Colditz GA, Stampfer MJ, Willett WC (1995) Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann Intern Med 122(5):327–334
Thune I, Lund E (1996) Physical activity and risk of colorectal cancer in men and women. Br J Cancer 73(9):1134–1140
Martinez ME, Giovannucci E, Spiegelman D, Hunter DJ, Willett WC, Colditz GA for the Nurses’ Health Study Research Group (1997) Leisure-time physical activity, body size, and colon cancer in women. J Natl Cancer Inst 89(13):948–955
Lee IM, Manson JE, Ajani U, Paffenbarger RS Jr, Hennekens CH, Buring JE (1997) Physical activity and risk of colon cancer: the Physicians’ Health Study (United States). Cancer Causes Control 8(4):568–574
Will JC, Galuska DA, Vinicor F, Calle EE (1998) Colorectal cancer: another complication of diabetes mellitus? Am J Epidemiol 147(9):816–825
Lund Nilsen TI, Vatten LJ (2001) Prospective study of colorectal cancer risk and physical activity, diabetes, blood glucose and BMI: exploring the hyperinsulinaemia hypothesis. Br J Cancer 84(3):417–422
Colbert LH, Hartman TJ, Malila N et al (2001) Physical activity in relation to cancer of the colon and rectum in a cohort of male smokers. Cancer Epidemiol Biomarkers Prev 10(3):265–268
Wannamethee SG, Shaper AG, Walker M (2001) Physical activity and risk of cancer in middle-aged men. Br J Cancer 85(9):1311–1316
Chao A, Connell CJ, Jacobs EJ et al (2004) Amount, type, and timing of recreational physical activity in relation to colon and rectal cancer in older adults: the Cancer Prevention Study II Nutrition Cohort. Cancer Epidemiol Biomarkers Prev 13(12):2187–2195
Kato I, Tominaga S, Ikari A (1990) A case–control study of male colorectal cancer in Aichi Prefecture, Japan: with special reference to occupational activity level, drinking habits and family history. Jpn J Cancer Res 81(2):115–121
Samad AK, Taylor RS, Marshall T, Chapman MA (2005) A meta-analysis of the association of physical activity with reduced risk of colorectal cancer. Colorectal Dis 7(3):204–213
Otani T, Iwasaki M, Inoue M, Tsugane S for the Japan Public Health Center-based Prospective Study Group (2005) Body mass index, body height, and subsequent risk of colorectal cancer in middle-aged and elderly Japanese men and women: Japan public health center-based prospective study. Cancer Causes Control 16(7):839–850
World Health Organization (2000) International classification of diseases for oncology, 3rd edn. World Health Organization, Geneva, Switzerland
Ainsworth BE, Haskell WL, Whitt MC et al (2000) Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 32(9 Suppl):S498–504
Otani T, Iwasaki M, Yamamoto S et al (2003) Alcohol consumption, smoking, and subsequent risk of colorectal cancer in middle-aged and elderly Japanese men and women: Japan Public Health Center-based prospective study. Cancer Epidemiol Biomarkers Prev 12(12):1492–1500
Tsubono Y, Otani T, Kobayashi M, Yamamoto S, Sobue T, Tsugane S for the JPHC Study Group (2005) No association between fruit or vegetable consumption and the risk of colorectal cancer in Japan. Br J Cancer 92(9):1782–1784
Otani T, Iwasaki M, Hanaoka T et al (2005) Folate, vitamin B6, vitamin B12, and vitamin B2 intake, genetic polymorphisms of related enzymes, and risk of colorectal cancer in a hospital-based case–control study in Japan. Nutr Cancer 53(1):42–50
Sanjoaquin MA, Allen N, Couto E, Roddam AW, Key TJ (2005) Folate intake and colorectal cancer risk: a meta-analytical approach. Int J Cancer 113(5):825–828
Slattery ML, Murtaugh M, Caan B, Ma KN, Neuhausen S, Samowitz W (2005) Energy balance, insulin-related genes and risk of colon and rectal cancer. Int J Cancer 115(1):148–154
Norat T, Bingham S, Ferrari P et al (2005) Meat, fish, and colorectal cancer risk: the European Prospective Investigation into cancer and nutrition. J Natl Cancer Inst 97(12):906–916
Larsson SC, Rafter J, Holmberg L, Bergkvist L, Wolk A (2005) Red meat consumption and risk of cancers of the proximal colon, distal colon and rectum: the Swedish Mammography Cohort. Int J Cancer 113(5):829–834
Park Y, Hunter DJ, Spiegelman D et al (2005) Dietary fiber intake and risk of colorectal cancer: a pooled analysis of prospective cohort studies. Jama 294(22):2849–2857
Pugh S, Thomas GA (1994) Patients with adenomatous polyps and carcinomas have increased colonic mucosal prostaglandin E2. Gut 35(2):675–678
Thun MJ, Namboodiri MM, Heath CW Jr (1991) Aspirin use and reduced risk of fatal colon cancer. N Engl J Med 325(2):1593–1596
McKeown-Eyssen G (1994) Epidemiology of colorectal cancer revisited: are serum triglycerides and/or plasma glucose associated with risk? Cancer Epidemiol Biomarkers Prev 3(8):687–695
Giovannucci E (1995) Insulin and colon cancer. Cancer Causes Control 6(2):164–179
Acknowledgments
K-J.L. was awarded a Visiting Scientist Fellowship from the Foundation for Promotion of Cancer Research in Japan. The authors thank all staff members in each study area for their unfailing efforts in conduction the baseline and follow-up surveys. We also express our gratitude to the Iwate, Aomori, and Okinawa Cancer Registries for providing the incidence data. This work was supported by a Grant-in-Aid for Cancer Research and by the Third-Term Comprehensive Control Research for Cancer from the Ministry of Health, Labour and Welfare, Japan.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Study group members are listed in the Appendix at the end of this article.
Appendix
Appendix
Members of the Japan Public Health Center-based Prospective Study (JPHC Study, principal investigator: S. Tsugane) Group are: S. Tsugane, M. Inoue, T. Sobue, and T. Hanaoka, Research Center for Cancer Prevention and Screening, National Cancer Center, Tokyo; J. Ogata, S. Baba, T. Mannami, and A. Okayama, National Cardiovascular Center, Suita; K. Miyakawa, F. Saito, A. Koizumi, Y. Sano, and I. Hashimoto, Iwate Prefectural Ninohe Public Health Center, Ninohe; Y. Miyajima, N. Suzuki, S. Nagasawa, and Y. Furusugi, Akita Prefectural Yokote Public Health Center, Yokote; H. Sanada, Y. Hatayama, F. Kobayashi, H. Uchino, Y. Shirai, T. Kondo, R. Sasaki, Y. Watanabe, and Y. Miyagawa, Nagano Prefectural Saku Public Health Center, Saku; Y. Kishimoto, E. Takara, T. Fukuyama, M. Kinjo, M. Irei, and H. Sakiyama, Okinawa Prefectural Chubu Public Health Center, Okinawa; K. Imoto, H. Yazawa, T. Seo, A. Seiko, F. Ito, and F. Shoji, Katsushika Public Health Center, Tokyo; A. Murata, K. Minato, K. Motegi, and T. Fujieda, Ibaraki Prefectural Mito Public Health Center, Mito; K. Matsui, T. Abe, M. Katagiri, and M. Suzuki, Niigata Prefectural Kashiwazaki and Nagaoka Public Health Center, Kashiwazaki and Nagaoka; M. Doi, A. Terao, and Y. Ishikawa, Kochi Prefectural Chuo-higashi Public Health Center, Tosayamada; H. Sueta, H. Doi, M. Urata, N. Okamoto, and F. Ide, Nagasaki Prefectural Kamigoto Public Health Center, Arikawa; H. Sakiyama, N. Onga, and H. Takaesu, Okinawa Prefectural Miyako Public Health Center, Hirara; F. Horii, I. Asano, H. Yamaguchi, K. Aoki, S. Maruyama, and M. Ichii, Osaka Prefectural Suita Public Health Center, Suita; S. Matsushima and S. Natsukawa, Saku General Hospital, Usuda; M. Akabane, Tokyo University of Agriculture, Tokyo; M. Konishi, and K. Okada, Ehime University, Ehime; H. Iso, Osaka University, Suita; Y. Honda and K. Yamagishi, Tsukuba University, Tsukuba; H. Sugimura, Hamamatsu University, Hamamatsu; Y. Tsubono, Tohoku University, Sendai; M. Kabuto, National Institute for Environmental Studies, Tsukuba; S. Tominaga, Aichi Cancer Center Research Institute, Nagoya; M. Iida and W. Ajiki, Osaka Medical Center for Cancer and Cardiovascular Disease, Osaka; S. Sato, Osaka Medical Center for Health Science and Promotion, Osaka; N. Yasuda, Kochi University, Nankoku; S. Kono, Kyushu University, Fukuoka; K. Suzuki, Research Institute for Brain and Blood Vessels Akita, Akita; Y. Takashima, Kyorin University, Mitaka; E. Maruyama, Kobe University, Kobe; M. Yamaguchi, Y. Matsumura, S. Sasaki, and S. Watanabe, National Institute of Health and Nutrition, Tokyo; T. Kadowaki, Tokyo University, Tokyo; Y. Kawaguchi, Tokyo Medical and Dental University, Tokyo; and H. Shimizu, Sakihae Institute, Gifu.
Rights and permissions
About this article
Cite this article
Lee, KJ., Inoue, M., Otani, T. et al. Physical activity and risk of colorectal cancer in Japanese men and women: the Japan Public Health Center-based prospective Study. Cancer Causes Control 18, 199–209 (2007). https://doi.org/10.1007/s10552-006-0098-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-006-0098-3