
Abstract
Diabetes mellitus significantly hampers the development of cardioprotective response to remote pre/post/perconditioning stimuli by impairing the activation of cardioprotective signaling pathways. Among the different pathways, the impairment in O-linked β-N-acetylglucosamine (O-GlcNAc) signaling and release of cardioprotective humoral factor may contribute in attenuating remote preconditioning-induced cardioprotection. Moreover, the failure to phosphorylate extracellular signal related kinase (ERK), phosphoinositide-3-kinase (PI3K), and AKT along with up-regulation of mechanistic target of rapamycin (mTOR) and decrease in autophagy may also attenuate remote preconditioning-induced cardioprotection. Remote perconditioning stimulus also fails to phosphorylate AKT kinase in diabetic heart. In addition, diabetes may increase the oxidative stress, reactive oxygen species (ROS) production, decrease the beclin expression, and inhibit autophagy to attenuate remote perconditioning-induced cardioprotection. Moreover, diabetes-induced increase in the Rho-associated kinase (ROCK) activity, decrease in the arginase activity, and reduction in nitric oxide (NO) bioavailability may also contribute in decreasing remote perconditioning-induced cardioprotection. Diabetes may reduce the phosphorylation of adenosine 5′-monophosphate activated protein kinase (AMPKα) and increase the phosphorylation of mTOR to attenuate cardioprotection of remote postconditioning. The present review describes the role of diabetes in attenuating remote ischemic conditioning-induced cardioprotection along with the possible mechanisms.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Remote ischemic conditioning (RIC) is the phenomenon in which short, repeated cycles of ischemia and reperfusion to a remote organ (other than heart) confer protection to heart against sustained ischemia–reperfusion injury [43, 54]. Indeed, in this treatment approach, there is activation of an endogenous protective adaptive response in the heart for counteracting ischemia–reperfusion injury [46, 50]. On the basis of time of delivery (before, during, or after sustained ischemia) and site of delivery (type of remote organ) of conditioning stimulus, remote ischemic conditioning is classified into different types. In remote ischemic preconditioning, short cycles of ischemia and reperfusion are delivered to the remote organ before index ischemia (sustained ischemia) [15]. In remote ischemic perconditioning, conditioning stimulus is delivered to the remote organ during the time of sustained cardiac ischemia. In remote ischemic post-conditioning, short cycles of ischemia and reperfusion are delivered to the remote organ during the initial minutes of heart reperfusion [10, 69]. Apart from the time of delivery, remote ischemic conditioning has also been classified into different types depending on the remote organ, which is subjected to short episodes of ischemia and reperfusion. In remote iliac artery ischemic conditioning, conditioning stimulus is delivered by clamping the iliac artery [41]. In remote renal conditioning, remote mesenteric conditioning, and remote hind limb conditioning, the conditioning stimulus is delivered by occluding renal arteries, mesenteric arteries, and femoral arteries, respectively [5, 6, 12, 15, 47,54,49, 55, 68]. Among these, remote hind limb conditioning has also been employed in the clinical studies because the hind limb may be occluded non-invasively by tying one of the limbs with the blood pressure cuff [7, 26, 32].
There have been a large number of studies documenting the clinical efficacy of remote ischemic conditioning in patients undergoing heart surgery [56, 60]. Moreover, this phenomenon is also shown to improve coronary artery function in patients with stable coronary artery disease [9]. On the other hand, some meta-analysis studies have documented that remote ischemic conditioning is unable to yield promising results in various cardiovascular disease conditions [19, 22, 40]. The lack of cardioprotective effects of remote conditioning in these clinical trials may be possibly attributed to certain factors that may limit its clinical application in patients [61]. Indeed, there have been studies showing that the beneficial effects of remote ischemic conditioning in humans is influenced by various factors including aging [33, 42, 51], comorbidities such as angina pectoris, hypertension, hyperlipidemia, heart failure, cardiac hypertrophy, changes in the coronary artery circulation, insulin resistance, and diabetes mellitus [13, 39, 63]. The pharmacotherapy used for treating these comorbidities or for other purposes such as statins, nitrates, oral hypoglycemic agents [8, 37], and anesthetics [30] may also affect the cardioprotective ability of remote ischemic conditioning [13]. Diabetes mellitus poses a significant challenge to the successful implementation of ischemic conditioning in protecting hearts in clinical setting [64]. On a similar lines, there have been a number of studies demonstrating a decrease in the cardioprotective effects of remote ischemic pre/per/postconditioning during diabetic state owing to interference with the cardioprotective mechanisms, defective post receptor signaling, or/and changes in the functioning of the mitochondria [4, 16, 21, 23, 24, 27, 28, 42]. The present review describes diabetes or an increase in glucose levels as one of the major risk factors in attenuating remote ischemic conditioning-induced cardioprotection along with the possible mechanisms.
The literature search for writing this present review was done using www.Pubmed.com as the search engine and different combinations of keywords were used to search the literature. These included “remote preconditioning, diabetes and heart,” “remote perconditioning, diabetes and heart,” and “remote postconditioning, diabetes and heart.” The cross-references from the papers collected from PubMed were also used to collect diabetes and remote conditioning-related literature.
Evidences that diabetes abolishes cardioprotective effect of remote ischemic conditioning
Remote ischemic preconditioning
There have been reports suggesting that diabetes mellitus or an increase in glucose levels may impair the cardioprotective effect of remote ischemic preconditioning. Hu et al. reported the impact of acute streptozotocin (STZ, 50 mg/kg, i.p.)-induced diabetes mellitus on left coronary artery ligation-induced ventricular arrhythmia in remote ischemic preconditioning subjected rats. Four cycles of 5 min of ischemia and 5 min of reperfusion served as remote ischemic preconditioning stimulus before myocardial ischemia reperfusion injury (5 min of ischemia followed by 20 min of reperfusion). The severity of arrhythmia was assessed by noting the development of ventricular tachycardia, fibrillation, and atrioventricular block. The authors reported that remote ischemic preconditioning significantly reduces all types of arrhythmias induced by ischemic reperfusion injury in non-diabetic rats, but it did not attenuate the incidence of all types of arrhythmias in diabetic rats. The atrioventricular block was significantly less (fourfold) in remote ischemic preconditioning-subjected rats as compared to control group of non-diabetic rats. However, remote ischemic preconditioning failed to attenuate atrioventricular block in diabetic rats [21].
A clinical study of Jensen et al. reported that remote preconditioning-induced release and effect of a circulating cardioprotective factor is reduced in type 2 diabetes mellitus patients suffering from peripheral neuropathy. Blood samples were withdrawn from nine non-diabetic patients, eight diabetic patients with no symptoms of peripheral neuropathy, and eight diabetic patients with symptoms of peripheral neuropathy before (control) and after remote ischemic preconditioning stimulus. In test persons, remote ischemic preconditioning stimulus of 4 cycles comprising 5 min of upper-arm ischemia and 5 min of reperfusion was given by inflation (up to 200 mmHg) and deflation of blood pressure cuff. After the initial 4 cycles of 5 min remote ischemic preconditioning stimulus, test persons with diabetic neuropathy immediately underwent additional 2 cycles of 10 min remote ischemic preconditioning stimulus (intensified remote ischemic preconditioning stimulus). The blood samples were withdrawn, dialyzed, and the cardioprotective effects of the dialysates were tested in rabbit hearts mounted on the Langendroff system [23]. It was reported that myocardial infarct size, the post-ischemic left ventricular developed pressure, dp/dtmin, dp/dtmax along with the rate pressure product were improved in rabbits’ hearts perfused with dialysate from both non-diabetic and diabetic subjects without peripheral neuropathy receiving remote ischemic preconditioning. However, dialysate obtained from diabetic neuropathy patients subjected to remote ischemic preconditioning episodes failed to reduce infarct size and improve contractility parameters. Furthermore, dialysate from the patients subjected to intensified remote ischemic preconditioning also failed to confer cardioprotection. Therefore, it was suggested that the presence of intact neurogenic pathway is essential for the release of the cardioprotective humoral factor during remote ischemic preconditioning. Accordingly, due to non-functional neurogenic pathway in diabetic neuropathy, the cardioprotective effect of dialysate from remote ischemic preconditioning subjected diabetic patients was not observed [23].
Another study from the same group of scientists also reported that diabetes influences the cardioprotective effects of remote preconditioning (Table 1). The effects of plasma dialysate obtained from healthy persons (n = 8) and type 2 diabetic patients (n = 8) before and after remote ischemic preconditioning stimulus were tested on human isolated atrial trabeculae against ischemia–reperfusion injury (ischemia of 30 min and reperfusion of 120 min). The dialysate obtained from normal persons after remote preconditioning produced cardioprotective effects on human atrial trabeculae. Similarly, dialysate isolated from diabetic persons produced cardioprotective effects; however, remote ischemic preconditioning stimulus in the diabetic patients failed to produce any additional beneficial effects [24].
Remote ischemic perconditioning
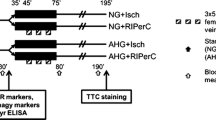
Apart from remote preconditioning, diabetes and acute hyperglycemia also abolish remote ischemic perconditioning-induced myocardial protection. A study of Baranyai et al. demonstrated that an acute rise in glucose levels attenuates remote ischemic perconditioning-induced cardioprotection in rats. Animals received 50% dextrose infusion to induce acute hyperglycemia and serum glucose levels were maintained at 15–20 mM concentration. In normal glycemic animals, 46% mannitol infusion was administered to maintain the similar osmolarity. Remote perconditioning stimulus was delivered by alternatively tying and untying the femoral vessels (arteries and veins) for short periods [4]. The study reported that remote ischemic perconditioning significantly reduces the extent of infarction in normoglycemic animals, while it does not decrease the infarct size in acute hyperglycemic animals. The authors also documented that the acute rise in glucose levels did not modulate ischemia-induced myocardial injury. This report is in contrast to studies showing that acute hyperglycemia per se increases the extent of infarction [25, 58]. These contradictory reports may be possibly due to the different glucose concentrations employed in these studies. The reports suggesting an enhancement in infarction in ischemia-subjected animals have employed relatively higher concentration of glucose (more than 30 mM concentration) [38]. On the contrary, Baranyai et al. maintained much lower concentration of glucose, i.e., 15–20 mM and documented no per se influence of acute hyperglycemia on ischemic injury. In contrast, the authors documented that the incidence and duration of arrhythmias was higher in acute hyperglycemic animals in comparison to normoglycemic animals during ischemic period. Moreover, remote ischemic perconditioning did not modulate arrhythmia in hyperglycemic and normoglycemic animals [4].
A study of Kiss et al. reported that remote ischemic perconditioning significantly reduces the myocardial infarct area in non-diabetic rats, but fails to modulate infarction in type 1 diabetic rats. However, the degree of myocardial infarction was comparable in non-diabetic and diabetic rats in response to ischemia–reperfusion injury. Remote ischemic perconditioning stimulus was delivered by occluding bilateral femoral arteries for 15 min during myocardial ischemia (30 min of coronary artery ligation followed by 2 h of reperfusion) [27, 28].
Remote ischemic postconditioning
A study of Han et al. demonstrated that autophagy plays a critical role in inducing cardioprotective effects of remote ischemic postconditioning in response to ischemia–reperfusion injury in normal mice, but not in diabetic mice. A single dose of STZ (150 mg/kg i.p.) was administered to induce diabetes in male mice. Remote ischemic postconditioning stimulus was delivered using three short cycles of ischemia and reperfusion (5 min of left femoral artery occlusion followed by 5 min of reperfusion) after 30 min of coronary artery occlusion and during initiation of reperfusion. Remote postconditioning attenuated myocardial infarction, improved left ventricular end diastolic and systolic diameter, improved cardiac ejection fraction, and preserved left ventricular systolic pressure in response to ischemia–reperfusion in non-diabetic mice. However, remote ischemic postconditioning did not modulate ischemic reperfusion injury in diabetic mice [16].
Possible mechanisms
The different mechanisms that may contribute in attenuating the cardioprotective effects of remote conditioning in diabetics are discussed below (Fig. 1).

Possible mechanisms that may be involved in abolishing conditioning-induced cardioprotection during diabetes
Remote ischemic preconditioning
Reperfusion injury salvage kinase (RISK) pathway
The RISK pathway refers to pro-survival kinases, which are activated during reperfusion phase of ischemia–reperfusion injury to confer cardioprotection. Indeed, this pathway includes a group of protein kinases including AKT, and ERK1/2, and their activation at the time of reperfusion decreases myocardial injury [18, 53]. Remote ischemia preconditioning produces cardioprotection against ischemia–reperfusion injury via activation of RISK pathway, and inhibition of GSK-3β (Ser 9) phosphorylation [18]. Hu et al. reported that remote preconditioning increases the levels of phosphorylated forms of ERK1/2, AKT, and GSK-3β during reperfusion phase. However, remote ischemic preconditioning increased the phosphorylation of these enzymes in the hearts of diabetic as well as in non-diabetic rats to a comparable degree. It suggests that diabetes does not impair the functioning or activation process of RISK pathway. Another study has shown that exogenous administration of H2S donor confers cardioprotection in diabetic rats by activation of endogenous protective RISK pathway [31] suggesting that RISK pathway remains intact and is not impaired in diabetic conditions. Therefore, it may be proposed that impairment of pro-survival kinases of RISK pathway may not be contributing in attenuating remote preconditioning-induced cardioprotection in diabetic state [21].
Neural pathway
There have been studies including from our laboratory showing the involvement of neural pathways in mediating the cardioprotective effects of remote ischemic preconditioning [2, 57]. It has been reported that resection of femoral or the sciatic nerves partially blocks remote ischemic preconditioning-induced cardioprotection, while resection of both the nerves completely abolishes the cardioprotective effect of remote ischemic preconditioning [35]. The study of Jensen et al. proposed that there is a release of a cardioprotective humoral factor during remote ischemic preconditioning, which may be dialyzed and administered to rabbits to confer them cardioprotection against ischemia–reperfusion injury. It was also proposed that release of the cardioprotective factor is dependent on the presence of intact neural pathway. However, it is well reported that there is significant impairment in neural functioning during long-standing diabetes, which is manifested in the form of diabetic neuropathy [20]. Therefore, it is possible to propose that during long-standing diabetes, nerve injury in the form of diabetic neuropathy may inhibit the release of cardioprotective factor during remote ischemic preconditioning, which is manifested in the form of attenuation of the cardioprotection [23].
O-Linked β-N-acetylglucosamine (O-GlcNAc) glycosylation
O-GlcNAc is an intercellular carbohydrate, which results in a post-translational modification of proteins (cytoplasmic, nuclear, and mitochondrial) in response to changes in extracellular concentration of glucose. O-GlcNAc glycosylation is the post-translational modification of proteins in response to high glucose levels in which N-acetylglucosamine is linked to serine or threonine residues of intracellular proteins via O-glycosidic linkage with the help of O-GlcNAc transferase (OGT). The levels of O-GlcNAc are increased during ischemic preconditioning to produce cardioprotection [24]. Remote ischemic preconditioning dialysate from non-diabetic volunteers augmented the levels of O-GlcNAc in isolated atrial trabeculae in comparison to control dialysate suggesting that an increase in O-GlcNAc may confer cardioprotection. However, remote ischemic preconditioning dialysate isolated from diabetic persons failed to augment the already raised O-GlcNAc levels due to diabetes [24]. Remote preconditioning-induced cardioprotection depends on O-GlcNAcylation and the levels of O-GlcNAc cannot increase beyond the limits in diabetic persons because these levels are already increased before remote preconditioning stimulus during diabetic conditions. Administration of azaserine (glutaminefructose-6-phosphate amidotransferase, GFAT, inhibitor) attenuated the increase in O-GlcNAc levels in the atrial tissue and also reduced the cardioprotective effects in response to remote ischemic preconditioning dialysate as well as diabetic control dialysate [24].
Remote ischemic perconditioning
Mechanistic target of rapamycin (mTOR) and AKT pathway
Baranyai et al. reported that remote perconditioning-induced cardioprotection was abolished during acute hyperglycemia due to activation of mTOR and AKT [4]. mTOR is serine/threonine kinase that crucially mediates energy metabolism and is present in two forms, mTOR complex 1 (mTORC1), which is inhibited by rapamycin, and mTOR complex 2 (mTORC2), which regulates cellular homeostasis, stress responses, energy metabolism, and autophagy [14, 62]. Baranyai et al. reported that mTOR (Ser2448) and S6 (Ser235/236) were phosphorylated during diabetes mellitus, indicating that the activity of mTOR complex 1 was increased in acute hyperglycemic animals. Furthermore, AKT phosphorylation at Ser473 was also increased in acute hyperglycemic animals. However, phosphorylation of AMPKα (Thr172) and ERK1/2 (Thr202/Tyr204) did not change in acute hyperglycemic animals in comparison to normal glycemic animals. It has been shown that remote perconditioning down-regulates mTOR [52]. There have been other studies showing an increase in mTOR and AKT activity during acute hyperglycemic condition [11]. It has also been reported that the elevation of mTOR and AKT signaling increases the extent of myocardial injury during ischemia [62]. Pre-treatment with rapamycin has been shown to attenuate the effect of increased levels of mTOR leading to improvement in the cardiac function resulting from cardiac ischemia–reperfusion injury in diabetic mice [67]. Therefore, it is possible to suggest that acute hyperglycemia may activate mTOR pathway and its upstream modulator AKT, which may abolish remote ischemic perconditioning-induced cardioprotection [4].
Oxidative stress
An increase in oxidative stress is a major pathogenic factor in ischemia–reperfusion injury [58]. Hyperglycemia promotes production of reactive oxygen species (ROS), which may be critically involved in the development of diabetic complications. The levels of functional glutathione peroxidase are reported to be significantly decreased in diabetic mice [34]. In type 2 diabetic patients, the levels of both enzymatic (glutathione peroxidase, superoxide dismutase, and catalase) and non-enzymatic (vitamin E and C, β-carotene, and retinol) antioxidants are relatively low in comparison to non-diabetic subjects [45]. Primarily, hyperglycemia leads to increased formation of oxygen free radicals in the cardiac tissue by causing interruption of electron transport chain, activation of NADPH oxidase, and uncoupling of nitric oxide synthase [1]. Accordingly, oxidative stress has been proposed as a link between hyperglycemia and increased tendency to ischemic heart injury [58]. Baranyai et al. reported that oxidative stress and nitrative stress were increased during acute hyperglycemia in rats, as indicated by the elevated levels of cardiac nitrative stress marker (3-nitrotyrosine) during hyperglycemia [4]. Thus, it is possible to suggest that an increase in oxidative stress and nitrative stress may possibly impair the cardioprotective effects of remote perconditioning.
Autophagy
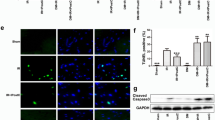
It is a process of auto-digestion in which the lysosomes degrade cellular organelles and other molecules. It helps in maintaining cellular homeostasis and it also provides cytoprotective actions [16]. It is proposed that the process of autophagy is activated during ischemia and reperfusion to protect the heart [16]. A study conducted by Qian et al. has suggested that inhibition of autophagy decreases the recovery of heart contractility against ischemia–reperfusion injury as observed in the transgenic mice with impaired autophagy in comparison to the non-transgenic animals [44]. However, Baranyai et al. reported that the quantitative index of autophagy, measured in terms of ratio of LC3II/LC3I, was decreased during remote ischemic perconditioning in acute hyperglycemia. However, the other autophagy proteins including Beclin-1, total and Triton X-100-insoluble SQSTMI/p62, phosphor-ULK1 (Ser555), ATG7, and BNIP3 did not change in acute hyperglycemic animals [4]. There have been earlier studies documenting that the presence of high glucose concentration (levels between 17 and 30 mM) leads to reduction in autophagy in comparison to normal glucose concentration (5.5 mM) [29]. Therefore, it may be proposed that an impairment in autophagy during diabetes may impair remote ischemic perconditioning-induced cardioprotection.
Rho A/Rho-associated kinase (ROCK) signaling pathway
ROCK is a serine/threonine protein kinase, which is an important component of intracellular signaling cascade [65]. RhoA is GTP binding protein and it activates ROCK, which exists in two isoforms (ROCK1 and ROCK2). During ischemia–reperfusion, there is up-regulation of RhoA in the heart, which activates Rho kinase and the latter plays a significant role in myocardial injury [3, 66]. It is also reported that diabetes may up-regulate the expression and actions of RhoA and ROCK [59]. It has been shown that remote perconditioning decreases the ROCK signaling and enhances the expression of endothelial nitric oxide synthase (eNOS) in normal rats. However, it failed to reduce ROCK activity and increase eNOS in diabetic rats. Furthermore, remote ischemic perconditioning failed to decrease arginase activity in diabetic rats in comparison to non-diabetic rats. Arginase degrades arginine and hence decreases the substrate for NO production. Remote perconditioning-induced cardioprotective effects were completely abolished in the presence of L-NMMA, an inhibitor of nitric oxide synthase, (10 mg/kg, i.v.) [27, 28]. Therefore, it may possible to suggest that a decrease in NO availability along with increase in ROCK activity during diabetes may abolish remote perconditioning-induced cardioprotection.
Remote ischemic postconditioning
Autophagy
Han and co-workers reported that remote ischemic postconditioning downregulates the levels of SQSTM1, increases the LC3-II/LC3-I ratio, and increases the number of autophagic vacuoles suggesting that activation of autophagy may be responsible for cardioprotection [16]. This contention was further supported by the finding that administration of 3-methyl adenine (3-MA), an autophagy inhibitor, attenuated remote postconditioning-induced cardioprotection in normal mice. However, remote postconditioning failed to activate autophagy in diabetic rats, and this effect was directly correlated to decrease in cardioprotection [16]. Therefore, it is possible to propose that diabetes may inhibit autophagy during remote postconditioning to abolish its cardioprotective effects.
Adenosine 5′-monophosphate-activated protein kinase (AMPK)
AMPK is an enzyme which senses ATP and it is activated during decrease in ATP levels such as in the case of hypoxia and decrease in glucose levels. In non-diabetic animals, remote ischemic postconditioning increased the phosphorylation of AMPK to increase the p-AMPKa (Thr172) levels suggesting that remote postconditioning-induced cardioprotection may be possibly due to an increase in AMPK activity [16]. However, the levels of phosphorylated AMPKα was not elevated in response to remote ischemic postconditioning in diabetic animals, suggesting that diabetes may inhibit AMPK activation and block cardioprotective effects of remote ischemic postconditioning [16]. Other studies have shown that ischemic postconditioning enhances AMPK phosphorylation to trigger cardioprotection [17]. Furthermore, the studies have also shown that diabetes decreases the AMPK activity and abolishes the cardioprotection [36].
Conclusion
Diabetes mellitus markedly abolishes the potential of remote pre/per/postconditioning stimuli to induce cardioprotection. The decrease in the release of humoral cardioprotective factors, O-GlcNAc signaling, and damage to the neural pathway due to diabetes may result in attenuating the cardioprotective effects of remote ischemic preconditioning. The protection conferred to the heart by remote ischemic perconditioning may be abolished in diabetic state owing to the activation of mTOR and AKT, increase in the oxidative stress, and upregulation of RhoA and ROCK. Diabetes may attenuate the cardioprotective activity of remote ischemic postconditioning as a consequence of decline in the activity of AMPK. The impairment of autophagy in diabetic state may be responsible for eliminating the cardioprotective effects of remote ischemic per and postconditioning.
References
Ansley DM, Wang B (2013 Jan) Oxidative stress and myocardial injury in the diabetic heart. J Pathol 229(2):232–241
Aulakh AS, Randhawa PK, Singh N, Jaggi AS (2017 Mar) Neurogenic pathways in remote ischemic preconditioning induced cardioprotection: evidences and possible mechanisms. Korean J Physiol Pharmacol 21(2):145–152
Bao W, Hu E, Tao L, Boyce R, Mirabile R, Thudium DT, Ma XL, Willette RN, Yue TL (2004) Inhibition of rho-kinase protects the heart against ischemia/reperfusion injury. Cardiovasc Res 61(3):548–558
Baranyai T, Nagy CT, Koncsos G, Onódi Z, Károlyi-Szabó M, Makkos A, Varga ZV, Ferdinandy P, Giricz Z (2015) Acute hyperglycemia abolishes cardioprotection by remote ischemic perconditioning. Cardiovasc Diabetol 14:151
Birnbaum Y, Hale SL, Kloner RA (1997) Ischemic preconditioning at a distance: reduction of myocardial infarct size by partial reduction of blood supply combined with rapid stimulation of the gastrocnemius muscle in the rabbit. Circulation 96(5):1641–1646
Bøtker HE, Kharbanda R, Schmidt MR, Bøttcher M, Kaltoft AK, Terkelsen CJ, Munk K, Andersen NH, Hansen TM, Trautner S, Lassen JF, Christiansen EH, Krusell LR, Kristensen SD, Thuesen L, Nielsen SS, Rehling M, Sørensen HT, Redington AN, Nielsen TT (2010) Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial. Lancet 375(9716):727–734
Cheung MM, Kharbanda RK, Konstantinov IE, Shimizu M, Frndova H, Li J, Holtby HM, Cox PN, Smallhorn JF, Van Arsdell GS, Redington AN (2006) Randomized controlled trial of the effects of remote ischemic preconditioning on children undergoing cardiac surgery: first clinical application in humans. J Am Coll Cardiol 47(11):2277–2282
Cleveland JC Jr, Meldrum DR, Cain BS, Banerjee A, Harken AH (1997) Oral sulfonylurea hypoglycemic agents prevent ischemic preconditioning in human myocardium. Two paradoxes revisited. Circulation 96(1):29–32
Corcoran D, Young R, Cialdella P, McCartney P, Bajrangee A, Hennigan B, Collison D, Carrick D, Shaukat A, Good R, Watkins S, McEntegart M, Watt J, Welsh P, Sattar N, McConnachie A, Oldroyd KG, Berry C (2018) The effects of remote ischaemic preconditioning on coronary artery function in patients with stable coronary artery disease. Int J Cardiol 252:24–30
Crimi G, Pica S, Raineri C, Bramucci E, De Ferrari GM, Klersy C, Ferlini M, Marinoni B, Repetto A, Romeo M, Rosti V, Massa M, Raisaro A, Leonardi S, Rubartelli P, Oltrona Visconti L, Ferrario M (2013) Remote ischemic post-conditioning of the lower limb during primary percutaneous coronary intervention safely reduces enzymatic infarct size in anterior myocardial infarction: a randomized controlled trial. JACC Cardiovasc Interv 6(10):1055–1063
Das A, Durrant D, Koka S, Salloum FN, Xi L, Kukreja RC (2014) Mammalian target of rapamycin (mTOR) inhibition with rapamycin improves cardiac function in type 2 diabetic mice: potential role of attenuated oxidative stress and altered contractile protein expression. J Biol Chem 289(7):4145–4160
Diwan V, Kant R, Jaggi AS, Singh N, Singh D (2008) Signal mechanism activated by erythropoietin preconditioning and remote renal preconditioning-induced cardioprotection. Mol Cell Biochem 315(1–2):195–201
Ferdinandy P, Hausenloy DJ, Heusch G, Baxter GF, Schulz R (2014) Interaction of risk factors, comorbidities, and comedications with ischemia/reperfusion injury and cardioprotection by preconditioning, postconditioning, and remote conditioning. Pharmacol Rev 66(4):1142–1174
Fraenkel M, Ketzinel-Gilad M, Ariav Y, Pappo O, Karaca M, Castel J, Berthault MF, Magnan C, Cerasi E, Kaiser N, Leibowitz G (2008) mTOR inhibition by rapamycin prevents beta-cell adaptation to hyperglycemia and exacerbates the metabolic state in type 2 diabetes. Diabetes 57(4):945–957
Gho BC, Schoemaker RG, van den Doel MA, Duncker DJ, Verdouw PD (1996) Myocardial protection by brief ischemia in noncardiac tissue. Circulation 94(9):2193–2200
Han Z, Cao J, Song D, Tian L, Chen K, Wang Y, Gao L, Yin Z, Fan Y, Wang C (2014) Autophagy is involved in the cardioprotection effect of remote limb ischemic postconditioning on myocardial ischemia/reperfusion injury in normal mice, but not diabetic mice. PLoS One 9(1):e86838
Hao M, Zhu S, Hu L, Zhu H, Wu X, Li Q (2017) Myocardial ischemic postconditioning promotes autophagy against ischemia reperfusion injury via the activation of the nNOS/AMPK/mTOR pathway. Int J Mol Sci 18(3):614
Hausenloy DJ, Yellon DM (2004) New directions for protecting the heart against ischaemia–reperfusion injury: targeting the reperfusion injury salvage kinase (RISK)-pathway. Cardiovasc Res 61(3):448–460
Hausenloy DJ, Candilio L, Evans R, Ariti C, Jenkins DP, Kolvekar S, Knight R, Kunst G, Laing C, Nicholas J, Pepper J, Robertson S, Xenou M, Clayton T, Yellon DM (2015) Remote ischemic preconditioning and outcomes of cardiac surgery. N Engl J Med 373:1408–1417
Heung Yong J, Baek HS, Park TS (2015) Morphologic changes in autonomic nerves in diabetic autonomic neuropathy. Diabetes Metab J 39(6):461–467
Hu Z, Chen M, Zhang P, Liu J, Abbott GW (2017) Remote ischemic preconditioning differentially attenuates post-ischemic cardiac arrhythmia in streptozotocin-induced diabetic versus nondiabetic rats. Cardiovasc Diabetol 16(1):57
Iliodromitis EK, Cohen MV, Dagres N, Andreadou I, Kremastinos DT, Downey JM (2015) What is wrong with cardiac conditioning? We may be shooting at moving targets. J Cardiovasc Pharmacol Ther 20(4):357–369
Jensen RV, Støttrup NB, Kristiansen SB, Bøtker HE (2012) Release of a humoral circulating cardioprotective factor by remote ischemic preconditioning is dependent on preserved neural pathways in diabetic patients. Basic Res Cardiol 107(5):285
Jensen RV, Zachara NE, Nielsen PH, Kimose HH, Kristiansen SB, Bøtker HE (2013) Impact of O-GlcNAc on cardioprotection by remote ischaemic preconditioning in non-diabetic and diabetic patients. Cardiovasc Res 97(2):369–378
Kannel WB, McGee DL (1979) Diabetes and cardiovascular disease. The Framingham study. JAMA 241(19):2035–2038
Kharbanda RK, Mortensen UM, White PA, Kristiansen SB, Schmidt MR, Hoschtitzky JA, Vogel M, Sorensen K, Redington AN, MacAllister R (2002) Transient limb ischemia induces remote ischemic preconditioning in vivo. Circulation 106(23):2881–2883
Kiss A, Tratsiakovich Y, Gonon AT, Fedotovskaya O, Lanner J, Andersson DC, Yang J, Pernow J (2014a) The role of arginase and rho kinase in cardioprotection from remote ischemic perconditioning in non-diabetic and diabetic rat in vivo. PLoS One 9(8):e104731
Kiss A, Tratsiakovich Y, Gonon AT, Fedotovskaya O, Lanner JT, Andersson DC, Yang J, Pernow J (2014b) The role of arginase and rho kinase in cardioprotection from remote ischemic perconditioning in non-diabetic and diabetic rat in vivo. PLoS One 9(8):e104731
Kobayashi S, Xu X, Chen K, Liang Q (2012) Suppression of autophagy is protective in high glucose-induced cardiomyocyte injury. Autophagy 8(4):577–592
Kottenberg E, Musiolik J, Thielmann M, Jakob H, Peters J, Heusch G (2014) Interference of propofol with signal transducer and activator of transcription 5 activation and cardioprotection by remote ischemic preconditioning during coronary artery bypass grafting. J Thorac Cardiovasc Surg 147(1):376–382
Lambert JP, Nicholson CK, Amin H, Amin S, Calvert JW (2014) Hydrogen sulfide provides cardioprotection against myocardial/ischemia reperfusion injury in the diabetic state through the activation of the RISK pathway. Med Gas Res 4(1):20
Lambert EA, Thomas CJ, Hemmes R, Eikelis N, Pathak A, Schlaich MP, Lambert GW (2016) Sympathetic nervous response to ischemia–reperfusion injury in humans is altered with remote ischemic preconditioning. Am J Physiol Heart Circ Physiol 311:H364–H370
Lee TM, Su SF, Chou TF, Lee YT, Tsai CH (2002) Loss of preconditioning by attenuated activation of myocardial ATP-sensitive potassium channels in elderly patients undergoing coronary angioplasty. Circulation 105(3):334–340
Lewis P, Stefanovic N, Pete J, Calkin AC, Giunti S, Thallas-Bonke V, Jandeleit-Dahm KA, Allen TJ, Kola I, Cooper ME, de Haan JB (2007) Lack of the antioxidant enzyme glutathione peroxidase-1 accelerates atherosclerosis in diabetic apolipoprotein E-deficient mice. Circulation 115(16):2178–2187
Lim SY, Yellon DM, Hausenloy DJ (2010) The neural and humoral pathways in remote limb ischemic preconditioning. Basic Res Cardiol 105(5):651–655
Lindholm CR, Ertel RL, Bauwens JD, Schmuck EG, Mulligan JD, Saupe KW (2013) A high-fat diet decreases AMPK activity in multiple tissues in the absence of hyperglycemia or systemic inflammation in rats. J Physiol Biochem 69(2):165–175
Loubani M, Fowler A, Standen NB, Galiñanes M (2005) The effect of gliclazide and glibenclamide on preconditioning of the human myocardium. Eur J Pharmacol 515(1–3):142–149
Mapanga RF, Joseph D, Symington B, Garson KL, Kimar C, Kelly-Laubscher R, Essop MF (2014) Detrimental effects of acute hyperglycaemia on the rat heart. Acta Physiol (Oxf) 210(3):546–564
McCafferty K, Forbes S, Thiemermann C, Yaqoob MM (2014) The challenge of translating ischemic conditioning from animal models to humans: the role of comorbidities. Dis Model Mech 7(12):1321–1333
Meybohm P, Bein B, Brosteanu O, Cremer J, Gruenewald M, Stoppe C, Coburn M, Schaelte G, Boning A, Niemann B, Roesner J, Kletzin F, Strouhal U, Reyher C, Laufenberg-Feldmann R, Ferner M, Brandes IF, Bauer M, Stehr SN, Kortgen A, Wittmann M, Baumgarten G, Meyer-Treschan T, Kienbaum P, Heringlake M, Schon J, Sander M, Treskatsch S, Smul T, Wolwender E, Schilling T, Fuernau G, Hasenclever D, Zacharowski K (2015) A multicenter trial of remote ischemic preconditioning for heart surgery. N Engl J Med 373:1397–1407
Motta GL, Souza PC, EBdos S, Bona SR, Schaefer PG, Lima CAT, Marroni NAP, Corso CO (2018) Effects of remote ischemic preconditioning and topical hypothermia in renal ischemia–reperfusion injury in rats. Acta Cir Bras 33(5):396–407
Przyklenk K (2011) Efficacy of cardioprotective ‘conditioning’ strategies in aging and diabetic cohorts the co-morbidity conundrum. Drugs Aging 28(5):331–343
Przyklenk K, Bauer B, Ovize M, Kloner RA, Whittaker P (1993) Regional ischemic ‘preconditioning’ protects remote virgin myocardium from subsequent sustained coronary occlusion. Circulation 87(3):893–899
Qian J, Ren X, Wang X, Zhang P, Jones WK, Molkentin JD, Fan G, Kranias EG (2009) Blockade of Hsp20 phosphorylation exacerbates cardiac ischemia/reperfusion injury by suppressed autophagy and increased cell death. Circ Res 105:1223–1231
Ramakrishna V, Jailkhani R (2008) Oxidative stress in non-insulin-dependent diabetes mellitus (NIDDM) patients. Acta Diabetol 45(1):41–46
Randhawa PK, Jaggi AS (2016) Gadolinium and ruthenium red attenuate remote hind limb preconditioning-induced cardioprotection: possible role of TRP and especially TRPV channels. Arch Pharmacol 389(8):887–896
Randhawa PK, Jaggi AS (2017a) Investigating the involvement of glycogen synthase kinase-3β and gap junction signaling in TRPV1 and remote hind preconditioning-induced cardioprotection. Eur J Pharmacol 814:9–17
Randhawa PK, Jaggi AS (2017b) Investigating the involvement of TRPV1 ion channels in remote hind limb preconditioning-induced cardioprotection in rats. Naunyn Schmiedeberg's Arch Pharmacol 390(2):117–126
Randhawa PK, Jaggi AS (2017c) Opioids in remote ischemic preconditioning-induced cardioprotection. J Cardiovasc Pharmacol Ther 22(2):112–121
Randhawa PK, Bali A, Jaggi AS (2015) RIPC for multiorgan salvage in clinical settings: evolution of concept, evidences and mechanisms. Eur J Pharmacol 746:317–332
Randhawa PK, Bali A, Virdi JK, Jaggi AS (2018) Conditioning-induced cardioprotection: aging as a confounding factor. Korean J Physiol Pharmacol. 22(5):467–479
Rohailla S, Clarizia N, Sourour M, Sourour W, Gelber N, Wei C, Li J, Redington AN (2014) Acute, delayed and chronic remote ischemic conditioning is associated with downregulation of mTOR and enhanced autophagy signaling. PLoS One 9(10):e111291
Rossello X, Yellon DM (2017) The RISK pathway and beyond. Basic Res Cardiol 113(1):2
Saxena P, Newman MA, Shehatha JS, Redington AN, Konstantinov IE (2010) Remote ischemic conditioning: evolution of the concept, mechanisms, and clinical application. J Card Surg 25(1):127–134
Schmidt MR, Smerup M, Konstantinov IE, Shimizu M, Li J, Cheung M, White PA, Kristiansen SB, Sorensen K, Dzavik V, Redington AN, Kharbanda RK (2007) Intermittent peripheral tissue ischemia during coronary ischemia reduces myocardial infarction through a KATP-dependent mechanism: first demonstration of remote ischemic perconditioning. Am J Physiol Heart Circ Physiol 292(4):H1883–H1890
Schmidt MR, Rasmussen ME, Bøtker HE (2017) Remote ischemic conditioning for patients with STEMI. J Cardiovasc Pharmacol Ther 22(4):302–309
Singh H, Kumar M, Singh N, Jaggi AS (2018) Late phases of cardioprotection during remote ischemic preconditioning and adenosine preconditioning involves activation of neurogenic pathway. J Cardiovasc Pharmacol. https://doi.org/10.1097/FJC.0000000000000634
Su H, Ji L, Xing W, Zhang W, Zhou H, Qian X, Wang X, Gao F, Sun X, Zhang H (2013) Acute hyperglycaemia enhances oxidative stress and aggravates myocardial ischaemia/reperfusion injury: role of thioredoxin-interacting protein. J Cell Mol Med 17(1):181–191
Sun Z, Wu X, Li W, Peng H, Shen X, Ma L, Liu H, Li H (2016) RhoA/rock signaling mediates peroxynitrite-induced functional impairment of rat coronary vessels. BMC Cardiovasc Disord 16(1):193
Tan W, Zhang C, Liu J, Li X, Chen Y, Miao Q (2018) Remote ischemic preconditioning has a cardioprotective effect in children in the early postoperative phase: a meta-analysis of randomized controlled trials. Pediatr Cardiol 39(3):617–626
Varga ZV, Giricz Z, Bencsik P, Madonna R, Gyongyosi M, Schulz R, Mayr M, Thum T, Puskas LG, Ferdinandy P (2015) Functional genomics of cardioprotection by ischemic conditioning and the influence of comorbid conditions: implications in target identification. Curr Drug Targets 16(8):904–911
Völkers M, Konstandin MH, Doroudgar S, Toko H, Quijada P, Din S, Joyo A, Ornelas L, Samse K, Thuerauf DJ, Gude N, Glembotski CC, Sussman MA (2013) Mechanistic target of rapamycin complex 2 protects the heart from ischemic damage. Circulation 128(19):2132–2144
Voucharas C, Lazou A, Triposkiadis F, Tsilimingas N (2011 Mar 23) Remote preconditioning in normal and hypertrophic rat hearts. J Cardiothorac Surg 6:34
Wider J, Przyklenk K (2014) Ischemic conditioning: the challenge of protecting the diabetic heart. Cardiovasc Diagn Ther 4(5):383–396
Yamamoto K, Maruyama K, Himori N, Omodaka K, Yokoyama Y, Shiga Y, Morin R, Nakazawa T (2014) The novel rho kinase (ROCK) inhibitor K-115: a new candidate drug for neuroprotective treatment in glaucoma. Invest Ophthalmol Vis Sci 55(11):7126–7136
Zhang J, Liu XB, Cheng C, Xu DL, Lu QH, Ji XP (2014) Rho-kinase inhibition is involved in the activation of PI3-kinase/Akt during ischemic-preconditioning-induced cardiomyocyte apoptosis. Int J Clin Exp Med 7(11):4107–4114 eCollection 2014
Zhang M, Sun D, Li S, Pan X, Zhang X, Zhu D, Li C, Zhang R, Gao E, Wang H (2015) Lin28a protects against cardiac ischaemia/reperfusion injury in diabetic mice through the insulin-PI3K-mTOR pathway. J Cell Mol Med 19(6):1174–1182
Zhou CC, Ge YZ, Yao WT, Wu R, Xin H, Lu TZ, Li MH, Song KW, Wang M, Zhu YP, Zhu M, Geng LG, Gao XF, Zhou LH, Zhang SL, Zhu JG, Jia RP (2017) Limited clinical utility of remote ischemic conditioning in renal transplantation: a meta-analysis of randomized controlled trials. PLoS One 12(1):e0170729
Zhu SB, Liu Y, Zhu Y, Yin GL, Wang RP, Zhang Y, Zhu J, Jiang W (2013) Remote preconditioning, perconditioning, and postconditioning: a comparative study of their cardio-protective properties in rat models. Clinics (Sao Paulo) 68(2):263–268
Acknowledgements
The authors are thankful to the Department of Pharmaceutical Sciences and Drug Research, Punjabi University, Patiala, India for supporting the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure of potential conflicts of interest
The authors declare no conflict of interests.
Research involving human participants and/or animals
The study did not involve usage of animals or employment of human participants.
Informed consent
The study did not involve participants of human volunteers.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
S.T. did the literature review and prepared the manuscript
J.K.V. helped in writing the manuscript and revised the manuscript
N.S. helped in literature review and completion of the article
A.S.J. conceived the idea and edited the manuscript
Rights and permissions
About this article

Cite this article
Tyagi, S., Singh, N., Virdi, J.k. et al. Diabetes abolish cardioprotective effects of remote ischemic conditioning: evidences and possible mechanisms. J Physiol Biochem 75, 19–28 (2019). https://doi.org/10.1007/s13105-019-00664-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13105-019-00664-w