
Abstract
Most early phase trials in stroke and brain trauma have failed in phase 3, including efforts to improve acute ischemic stroke outcomes beyond that achieved by intravenous recombinant tissue plasminogen activator (t-PA) (IVT). With the exception of more recent stent retriever trials, most subsequent phase 3 trials failed. We previously showed that baseline imbalances, non-linear relationships of these factors to outcome, and unrepresentative control populations invalidate traditional statistical analysis in early trials of heterogeneous diseases such as stroke. We developed an alternative approach using a pooled outcome model derived from control arms of randomized clinical trial (RCTs). This model then permits comparing treatment trials to an expected outcome of a pooled population. Here, we hypothesized we could develop such a model for IVT and tested it against outcomes without IVT. We surveyed literature for all trials involving one arm with IVT reporting baseline National Institute Stroke Scale (NIHSS), age, and outcome. A non-linear fit was performed including multi-dimensional statistical intervals (±95 %) permitting visual comparison of outcomes at their own baselines. We compared models derived from non-IVT control arms. Models from 24 IVT RCTs representing 3195 subjects were successfully generated for functional outcome, modified Rankin Scale (mRS) 0–2 (r 2 = 0. 83, p < 0.001), and mortality (r 2 = 0.54; p = 0.001). We confirmed better outcomes compared to no IVT and mixed use IVT models across the range of baseline factors. It was possible to generate an expected outcome model for IVT from existing literature. We confirmed benefit compared to placebo. This model should be useful to compare to new agents without the need for statistical manipulation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Other than more recent success with new generation stent retriever endovascular interventions [1–4], identifying neuro- or vasculo-protective strategies that improve upon thrombolysis with intravenous rt-PA (alteplase) have been mostly failures, with considerable resources expended on negative trials [5, 6]. Early phase trials of most of the ultimately unsuccessful agents or approaches appeared promising [7, 8]. Our prior work identified the contribution in smaller, early phase trials of baseline imbalances, unrepresentative control populations, and non-random noise distributions that invalidates the use of statistical correction to adjust for these factors [6]. The result is false-positive identification of treatments destined to fail. We also proposed the potential opposite scenario in which imbalances that favored better outcomes in the placebo arm may have generated false-negative results [9], missing an opportunity to identify a potential beneficial agent.
Baseline stroke severity and age have been associated with a large proportion of the variance related to group outcomes following stroke [9, 10]. We selected these factors to develop predictive outcome models from the pooled placebo arms of randomized stroke clinical trials [9] (RCTs). We compared treatments at their own baseline NIHSS and age to generate a pseudo-control model of patients treated without tPA (pPREDICTS; pooled Placebo REsponse Dictates TReatment Success). Using this method, early phase trials, where imbalances between treatment and control arm are common [6], and clinical case series without a control arm, can compare outcomes at the study’s own baseline conditions without statistical manipulation. In addition, we developed the novel feature of generating surfaces around the function that depict the probability that the result of any individual trial is different than the control function. Unlike other statistical methods that stratify or adjust for imbalances [11, 12], no such adjustment is needed here. Our methods have been successful in identifying those early phase trials and case series testing a new therapy compared to placebo that went on to be negative in phase 3 [13–15], including identifying the lack of net benefit of a heterogeneous group of endovascular interventions, a finding later confirmed in RCTs [16, 17].
In this paper, we present an analogous model from the rt-PA arms of RCTs (pPREDICTS-tPA). Successful generation of such a model would provide a means to compare treatments that intended to improve upon rt-PA, either as add-on or alternative therapies as well as non-randomized case series. The models were used to test outcomes against control arms that received no IVT or a mixed population that treated various percentages of subjects with IVT in order to determine whether we could confirm the known benefit of IVT.
Methods
Literature search to identify RCTs where all subjects in an arm received IVT
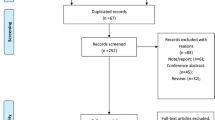
Medline database was searched (PM, AKS, SDS) for the words ‘acute’, ‘ischemic’, ‘stroke’, ‘alteplase’, ‘rt-PA’, ‘rtPA’, ‘t-PA’ and assessed to see if they fit the following selection criteria: (1) Randomized controlled trials. (2) Published in English. (3) Human Clinical Trials. (4) At least two arms in the trial and one of them requiring intravenous rt-PA. (5) At least ten subjects. (6) Treatment window up to 6 h. (7) Follow-up of 3 months. (8) Baseline NIHSS expressed as median (or subsequent contact with authors provided this information).
Development of the pPREDICTS-tPA and updated pPREDICTS models
Details of the methods to generate the pPREDICTS model have been previously published [9] and detailed in the Electronic supplementary material. Briefly, models were developed from 90-day outcomes of control arms of RCTS in a three-step procedure: (1) stabilizing the variance and linearizing a non-linear function by transforming the proportions by an arc-sine square root function (Supplement S1), (2) fitting a function to the transformed proportions (Supplement S2), and (3) eliminating outliers (Supplement S3). Multi-dimensional prediction interval surfaces were generated [18].
pPREDICTS-tPA Models for 90-day outcomes of mortality and mRS 0–2 were based on RCT arms where all subjects in the treated arm were randomized to receive IV rt-PA. We focused on mRS 0–2 and mortality since these were the most common outcomes employed and our prior work indicated mRS 0–2 as a reliable outcome for early phase stroke trials [19]. A second set of models were created using RCTs of control arms that permitted but did not require treatment of subjects with rt-PA simulating best medicine and a third set of models with RCTs of control arms that had no subjects treated with rt-PA. All three sets of models were based on RCTs with treatment windows up to 6 h.
Comparison of models with IVT
pPREDICTS-tPA models were tested against pPREDICTS models that contained no IV rt-PA arm or partially IV rt-PA treated arms to test if the model was able to demonstrate known benefit from IVT [20]. Different models were compared against each other using the F statistic [21].
Results
Generation of pPREDICTS-tPA models
pPREDICTS-tPA models were generated from 24 RCT rt-PA-alone treated arms with 3195 subjects. Of the 24 RCTs, there were 13 arms from RCTS that treated all subjects within 3 h [20, 22–33], five treated patients up to 4.5 h [2, 4, 34–36], one treated patients in the 3–4.5-h window [37], one in the 3–5-h window [38], one between 3 and 6 h [39], and three between 0 and 6 h [40–42]. Two trials (ATLANTIS-A [40] and CLASS-T [28]) did not provide mRS 0–2 data but did present mortality data. Four of these trials [2, 36, 39, 42] identified subjects using image guidance, but a separate analysis did not indicate any difference in outcomes and these trials were pooled with the others for subsequent analysis.
An overall functional outcome model for mRS 0–2 was developed from 22 RCTs. The model for mRS 0–2 along with ±95 % prediction interval surfaces is shown in Fig. 1a (R 2 = 0.83; p < 0.001). During the generation of the model, one study with 49 subjects (of 3096; 1.6%) was eliminated. A similar model for mRS 0–1 with ±95 % prediction interval surfaces was successfully generated (R 2 = 0.64; p < 0.001; figure not shown).

a pPREDICTS-tPA mRS 0–2 model (middle surface) developed from 22 control arms (R 2 = 0.83; p < 0.001). Surfaces on either side of the fit function represent ±95 % prediction intervals. b pPREDICTS-tPA mortality model (middle surface) developed from 21 control arms(R 2 = 0.54; p = 0.001). Surfaces on either side of the fit function represent ±95 % prediction intervals
During the generation of the mortality model, four studies with 166 subjects (5.2%) were eliminated in the outlier elimination step. The mortality model along with 95 % prediction intervals is shown Fig. 1b (R 2 = 0.54; p = 0.001).
Generation of updated pPREDICTS models
Models for mortality and mRS 0–2 were generated from control arms of 32 RCTs (7820 subjects) where some of the subjects were treated with IV rt-PA [13, 14, 20, 37–41, 43–65]. Seven of the 32 RCTs had treated subjects with rt-PA. Percentage of subjects treated with rt-PA ranged from a low of 9 % [51] to a high of 75 % [56]. Mortality and mRS 0–2 models were also generated from control arms of 25 RCTs (n = 4056) where none of the subjects were treated with IV rt-PA.
Comparison of pPREDICTS-tPA and pPREDICTS
The comparison of models of functional outcome of mRS 0–2 is shown in Fig. 2a (pPREDICTS-tPA, red mesh; pPREDICTS-No tPA, blue mesh; inset shows pPREDICTS, magenta mesh). Comparison of these models shows significant differences between models (pPREDICTS-tPA vs. pPREDICTS-No tPA, p = 0.01; pPREDICTS-tPA vs. pPREDICTS-partial tPA, p = 0.02). Comparison of mortality models between pPREDICTS-tPA (Fig. 2b, red mesh) and pPREDICTS (magenta mesh, with some subjects treated with IV rt-PA; blue mesh, no IV rt-PA) showed no significant differences (p >> 0.05). While not significantly different, visual inspection indicated some interesting trends. With respect to mRS 0–2 outcome, visual inspection of the surfaces suggests roughly parallel relationships between non-tPA and the tPA surfaces. The partial tPA surface is mostly between the others. With respect to mortality, the pPREDICTS-tPA surface appears to be lower throughout the range of NIHSS, but especially at higher NIHSS and lower age.

a Composite of pPREDICTS-tPA and pPREDICTS mRS 0–2 models. Significance values for the different comparisons: pPREDICTS-tPA vs. pPREDICTS-partial tPA: p = 0.02. pPREDICTS-tPA vs. pPREDICTS-No tPA: p = 0.01. b Composite of pPREDICTS-tPA and pPREDICTS mortality models. Significance for various comparisons: pPREDICTS-tPA vs. pPREDICTS-partial tPA: p = 0.51. pPREDICTS-tPA vs. pPREDICTS-No tPA: p = 0.37
Discussion
This report demonstrates the generation of IVT outcome models based on baseline NIHSS and age that were significantly associated with outcome. Based on goodness of fit, the relationship between these factors and functional outcome were more strongly associated than with mortality, a finding that is consistent with individual clinical trials that do not consistently demonstrate reduced mortality with IVT [20]. We confirmed that arms in which all patients were treated with IVT improved functional outcome compared to those with no or partial use of IVT. We did not have enough of the latter studies to test whether different percentages of subjects treated with IVT influenced outcomes except as a group. Similarly, few studies in the later time windows prevented a direct test of the influence of time to treatment on outcomes. We are working on alternative methods to address these issues.
We proposed this modeling approach to identify agents in which baseline imbalances may yield false-positive or false-negative results, particularly if the control arms are not representative of a broader population [6]. Statistical corrections are frequently applied to early trials since an imbalanced distribution of baseline factors and errors in assessment can affect outcomes separate from treatment effects [19], and non-random variation is more likely to occur in smaller trials [66]. However, we do not believe that application of statistical correction is justified in smaller trials with complex relationships between factors and outcome such as we have demonstrated in stroke [6]. Our prior work showed that issues such as improper use of statistical adjustments as well as a non-representative control arm (with worse outcomes than expected in a large population at multiple sites) were seen in 89 % of a sample of early phase stroke trials that led up to ultimately negative pivotal trials [6].
As imbalances diminish in larger trials, random effects would tend to even out and a more valid result would likely emerge. In applying pPREDICTS to early phase RCTs, we suggest the most valid early result would be those studies in which the control arm behaves similarly to the pPREDICTS pooled model. We also propose these models to test case series to a pooled model that can provide some early insight into whether improved outcomes might portend a positive RCT [67] or to look at balanced subgroups [68]. In versions without IVT, this model has successfully predicted retrospectively both the positive NINDS rt-PA trial and all negative phase 3 trials such as AbESTT and SAINT II [9]. Other updates have correctly identified among others, the negative citicoline trial [6], DP-b99, the zinc chelator [69], all of which had either non-representative control arms or major imbalances. Given this track record, perhaps this approach could aid in decision making related to which agents to pursue based on their early results [6].
References
Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372(1):11–20. Epub 2014/12/18.
Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372(11):1009–18. Epub 2015/02/12.
Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372(11):1019–30. Epub 2015/02/12.
Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015;372(24):2285–95. Epub 2015/04/18.
Fugate JE, Rabinstein AA. Update on intravenous recombinant tissue plasminogen activator for acute ischemic stroke. Mayo Clin Proc. 2014. Epub 2014/04/30.
Kent TA, Shah SD, Mandava P. Improving early clinical trial phase identification of promising therapeutics. Neurology. 2015;85(3):274–83.
Lapchak PA. Fast neuroprotection (fast-NPRX) for acute ischemic stroke victims: the time for treatment is now. Transl Stroke Res. 2013;4(6):704–9. Epub 2013/12/11.
Lapchak PA, Zhang JH. Resolving the negative data publication dilemma in translational stroke research. Transl Stroke Res. 2011;2(1):1–6. Epub 2011/06/15.
Mandava P, Kent TA. A method to determine stroke trial success using multidimensional pooled control functions. Stroke. 2009;40(5):1803–10. Epub 2009/03/17.
Uchino K, Billheimer D, Cramer SC. Entry criteria and baseline characteristics predict outcome in acute stroke trials. Stroke. 2001;32(4):909–16. Epub 2001/04/03.
Crager MR. Analysis of covariance in parallel-group clinical trials with pretreatment baselines. Biometrics. 1987;43(4):895–901. Epub 1987/12/01.
Koch GG, Tangen CM, Jung JW, Amara IA. Issues for covariance analysis of dichotomous and ordered categorical data from randomized clinical trials and non-parametric strategies for addressing them. Stat Med. 1998;17(15–16):1863–92. Epub 1998/09/28.
Lees KR, Zivin JA, Ashwood T, Davalos A, Davis SM, Diener HC, et al. NXY-059 for acute ischemic stroke. N Engl J Med. 2006;354(6):588–600. Epub 2006/02/10.
Shuaib A, Lees KR, Lyden P, Grotta J, Davalos A, Davis SM, et al. NXY-059 for the treatment of acute ischemic stroke. N Engl J Med. 2007;357(6):562–71. Epub 2007/08/10.
Davalos A, Alvarez-Sabin J, Castillo J, Diez-Tejedor E, Ferro J, Martinez-Vila E, et al. Citicoline in the treatment of acute ischaemic stroke: an international, randomised, multicentre, placebo-controlled study (ICTUS trial). Lancet. 2012;380(9839):349–57. Epub 2012/06/14.
Mandava P, Kent TA. Intra-arterial therapies for acute ischemic stroke. Neurology. 2007;68(24):2132–9. Epub 2007/06/15.
Mandava P, Suarez JI, Kent TA. Intravenous rt-PA versus endovascular therapy for acute ischemic stroke. Curr Atheroscler Rep. 2008;10(4):332–8. Epub 2008/07/09.
Dolan KD, Yang L, Trampel CP. Nonlinear regression technique to estimate kinetic parameters and confidence intervals in unsteady-state conduction-heated foods. J Food Eng. 2007;80:581–93.
Mandava P, Krumpelman CS, Shah JN, White DL, Kent TA. Quantification of errors in ordinal outcome scales using Shannon entropy: effect on sample size calculations. PLoS One. 2013;8(7):e67754. Epub 2013/07/19.
The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581–7. Epub 1995/12/14.
Using the F-test to compare two models. Non-linear regression. Stat Topic Files. 2013; Available from: https://sakai.duke.edu/access/content/group/25e08a3d-9fc4-41b0-a7e9-815732c1c4ba/New%20folder/Stat%20Topic%20Files/Non-Linear%20Regression/FTestTutorial.pdf.
Alexandrov AV, Molina CA, Grotta JC, Garami Z, Ford SR, Alvarez-Sabin J, et al. Ultrasound-enhanced systemic thrombolysis for acute ischemic stroke. N Engl J Med. 2004;351(21):2170–8. Epub 2004/11/19.
Broderick JP, Palesch YY, Demchuk AM, Yeatts SD, Khatri P, Hill MD, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 2013;368(10):893–903. Epub 2013/02/09.
Ciccone A, Valvassori L, Ponzio M, Ballabio E, Gasparotti R, Sessa M, et al. Intra-arterial or intravenous thrombolysis for acute ischemic stroke? The SYNTHESIS pilot trial. J Neurointervent Surg. 2010;2(1):74–9. Epub 2010/03/01.
Haley Jr EC, Thompson JL, Grotta JC, Lyden PD, Hemmen TG, Brown DL, et al. Phase IIB/III trial of tenecteplase in acute ischemic stroke: results of a prematurely terminated randomized clinical trial. Stroke. 2010;41(4):707–11. Epub 2010/02/27.
Hill MD, Martin RH, Palesch YY, Tamariz D, Waldman BD, Ryckborst KJ, et al. The Albumin in Acute Stroke Part 1 Trial: an exploratory efficacy analysis. Stroke. 2011;42(6):1621–5. Epub 2011/05/07.
Lang W, Stadler CH, Poljakovic Z, Fleet D. A prospective, randomized, placebo-controlled, double-blind trial about safety and efficacy of combined treatment with alteplase (rt-PA) and Cerebrolysin in acute ischaemic hemispheric stroke. Int J Stroke. 2013;8(2):95–104. Epub 2012/09/27.
Lyden P, Jacoby M, Schim J, Albers G, Mazzeo P, Ashwood T, et al. The Clomethiazole Acute Stroke Study in tissue-type plasminogen activator-treated stroke (CLASS-T): final results. Neurology. 2001;57(7):1199–205. Epub 2001/10/10.
Molina CA, Barreto AD, Tsivgoulis G, Sierzenski P, Malkoff MD, Rubiera M, et al. Transcranial ultrasound in clinical sonothrombolysis (TUCSON) trial. Ann Neurol. 2009;66(1):28–38. Epub 2009/08/12.
Pancioli AM, Adeoye O, Schmit PA, Khoury J, Levine SR, Tomsick TA, et al. Combined approach to lysis utilizing eptifibatide and recombinant tissue plasminogen activator in acute ischemic stroke-enhanced regimen stroke trial. Stroke. 2013;44(9):2381–7. Epub 2013/07/28.
Pancioli AM, Broderick J, Brott T, Tomsick T, Khoury J, Bean J, et al. The combined approach to lysis utilizing eptifibatide and rt-PA in acute ischemic stroke: the CLEAR stroke trial. Stroke. 2008;39(12):3268–76. Epub 2008/09/06.
Piironen K, Tiainen M, Mustanoja S, Kaukonen KM, Meretoja A, Tatlisumak T, et al. Mild hypothermia after intravenous thrombolysis in patients with acute stroke: a randomized controlled trial. Stroke. 2014;45(2):486–91. Epub 2014/01/18.
Zinkstok SM, Roos YB. Early administration of aspirin in patients treated with alteplase for acute ischaemic stroke: a randomised controlled trial. Lancet. 2012;380(9843):731–7. Epub 2012/07/04.
Chamorro A, Amaro S, Castellanos M, Segura T, Arenillas J, Marti-Fabregas J, et al. Safety and efficacy of uric acid in patients with acute stroke (URICO-ICTUS): a randomised, double-blind phase 2b/3 trial. Lancet Neurol. 2014;13(5):453–60. Epub 2014/04/08.
Ciccone A, Valvassori L, Nichelatti M, Sgoifo A, Ponzio M, Sterzi R, et al. Endovascular treatment for acute ischemic stroke. N Engl J Med. 2013;368(10):904–13. Epub 2013/02/08.
Huang X, Cheripelli BK, Lloyd SM, Kalladka D, Moreton FC, Siddiqui A, et al. Alteplase versus tenecteplase for thrombolysis after ischaemic stroke (ATTEST): a phase 2, randomised, open-label, blinded endpoint study. Lancet Neurol. 2015;14(4):368–76. Epub 2015/03/03.
Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–29. Epub 2008/09/26.
Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA. 1999;282(21):2019–26. Epub 1999/12/11.
Davis SM, Donnan GA, Parsons MW, Levi C, Butcher KS, Peeters A, et al. Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. Lancet Neurol. 2008;7(4):299–309. Epub 2008/02/26.
Clark WM, Albers GW, Madden KP, Hamilton S. The rtPA (alteplase) 0- to 6-hour acute stroke trial, part A (A0276g): results of a double-blind, placebo-controlled, multicenter study. Thrombolytic therapy in acute ischemic stroke study investigators. Stroke. 2000;31(4):811–6. Epub 2001/02/07.
Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet. 1998;352(9136):1245–51. Epub 1998/10/27.
Parsons M, Spratt N, Bivard A, Campbell B, Chung K, Miteff F, et al. A randomized trial of tenecteplase versus alteplase for acute ischemic stroke. N Engl J Med. 2012;366(12):1099–107. Epub 2012/03/23.
The RANTTAS Investigators. A randomized trial of tirilazad mesylate in patients with acute stroke (RANTTAS). Stroke. 1996;27(9):1453–8. Epub 1996/09/01.
Enlimomab Acute Stroke Trial Investigators. Use of anti-ICAM-1 therapy in ischemic stroke: results of the Enlimomab Acute Stroke Trial. Neurology. 2001;57(8):1428–34. Epub 2001/10/24.
Abciximab Emergent Stroke Treatment Trial (AbESTT) Investigators. Emergency administration of abciximab for treatment of patients with acute ischemic stroke: results of a randomized phase 2 trial. Stroke. 2005;36(4):880–90. Epub 2005/02/26.
Adams Jr HP, Effron MB, Torner J, Davalos A, Frayne J, Teal P, et al. Emergency administration of abciximab for treatment of patients with acute ischemic stroke: results of an international phase III trial: Abciximab in Emergency Treatment of Stroke Trial (AbESTT-II). Stroke. 2008;39(1):87–99. Epub 2007/11/23.
Bogousslavsky J, Victor SJ, Salinas EO, Pallay A, Donnan GA, Fieschi C, et al. Fiblast (trafermin) in acute stroke: results of the European-Australian phase II/III safety and efficacy trial. Cerebrovasc Dis. 2002;14(3–4):239–51. Epub 2002/10/31.
Camerlingo M, Salvi P, Belloni G, Gamba T, Cesana BM, Mamoli A. Intravenous heparin started within the first 3 hours after onset of symptoms as a treatment for acute nonlacunar hemispheric cerebral infarctions. Stroke. 2005;36(11):2415–20. Epub 2005/10/15.
Clark W, Ertag W, Orecchio E, Raps E. Cervene in acute ischemic stroke: results of a double-blind, placebo-controlled, dose-comparison study. J Stroke Cerebrovasc Dis. 1999;8(4):224–30. Epub 2007/09/27.
Clark WM, Coull BM, Karukin M, Hendin B, Kelley R, Rosing H, et al. Randomized trial of Cervene, a kappa receptor-selective opioid antagonist, in acute ischemic stroke. J Stroke Cerebrovasc Dis. 1996;6(1):35–40. Epub 1996/09/01.
Clark WM, Raps EC, Tong DC, Kelly RE. Cervene (Nalmefene) in acute ischemic stroke: final results of a phase III efficacy study. The Cervene Stroke Study Investigators. Stroke. 2000;31(6):1234–9. Epub 2000/06/03.
Davis SM, Lees KR, Albers GW, Diener HC, Markabi S, Karlsson G, et al. Selfotel in acute ischemic stroke: possible neurotoxic effects of an NMDA antagonist. Stroke. 2000;31(2):347–54. Epub 2000/02/05.
del Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA, Gent M. PROACT: a phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. PROACT Investigators. Prolyse in Acute Cerebral Thromboembolism. Stroke. 1998;29(1):4–11. Epub 1998/01/28.
Ehrenreich H, Weissenborn K, Prange H, Schneider D, Weimar C, Wartenberg K, et al. Recombinant human erythropoietin in the treatment of acute ischemic stroke. Stroke. 2009;40(12):e647–56. Epub 2009/10/17.
Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA. 1999;282(21):2003–11. Epub 1999/12/11.
Ginsberg MD, Palesch YY, Martin RH, Hill MD, Moy CS, Waldman BD, et al. The Albumin in Acute Stroke (ALIAS) Multicenter Clinical Trial Safety Analysis of Part 1 and Rationale and Design of Part 2. Stroke. 2011;42(1):119–27.
Grotta J. Lubeluzole treatment of acute ischemic stroke. The US and Canadian Lubeluzole Ischemic Stroke Study Group. Stroke. 1997;28(12):2338–46. Epub 1997/12/31.
Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kummer R, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA. 1995;274(13):1017–25. Epub 1995/10/04.
Levy DE, del Zoppo GJ, Demaerschalk BM, Demchuk AM, Diener H-C, Howard G, et al. Ancrod in acute ischemic stroke results of 500 subjects beginning treatment within 6 hours of stroke onset in the ancrod stroke program. Stroke. 2009;40(12):3796–803.
Ogawa A, Mori E, Minematsu K, Taki W, Takahashi A, Nemoto S, et al. Randomized trial of intraarterial infusion of urokinase within 6 hours of middle cerebral artery stroke: the middle cerebral artery embolism local fibrinolytic intervention trial (MELT) Japan. Stroke. 2007;38(10):2633–9. Epub 2007/08/19.
Rosso C, Corvol JC, Pires C, Crozier S, Attal Y, Jacqueminet S, et al. Intensive versus subcutaneous insulin in patients with hyperacute stroke: results from the randomized INSULINFARCT trial. Stroke. 2012;43(9):2343–9. Epub 2012/06/16.
Rudolf J. Hydroxyethyl starch for hypervolemic hemodilution in patients with acute ischemic stroke: a randomized, placebo-controlled phase II safety study. Cerebrovasc Dis. 2002;14(1):33–41. Epub 2002/07/05.
Sacco RL, DeRosa JT, Haley Jr EC, Levin B, Ordronneau P, Phillips SJ, et al. Glycine antagonist in neuroprotection for patients with acute stroke: GAIN Americas: a randomized controlled trial. JAMA. 2001;285(13):1719–28. Epub 2001/04/13.
Teal P, Davis S, Hacke W, Kaste M, Lyden PD, Fierus M, et al. A randomized, double-blind, placebo-controlled trial to evaluate the efficacy, safety, tolerability, and pharmacokinetic/pharmacodynamic effects of a targeted exposure of intravenous repinotan in patients with acute ischemic stroke modified randomized exposure controlled trial (mRECT). Stroke. 2009;40(11):3518–25.
Torgano G, Zecca B, Monzani V, Maestroni A, Rossi P, Cazzaniga M, et al. Effect of intravenous Tirofiban and aspirin in reducing short-term and long-term neurologic deficit in patients with ischemic stroke: a double-blind randomized trial. Cerebrovasc Dis. 2010;29(3):275–81.
Piggot TD. Missing data in meta-analysis: strategies and approaches. Advances in Meta-analysis. New York: Springer; 2012. p. 80–1.
Mandava P, Dalmeida W, Anderson JA, Thiagarajan P, Fabian RH, Weir RU, et al. A pilot trial of Low-dose intravenous Abciximab and unfractionated heparin for acute ischemic stroke: translating GP IIb/IIIa receptor inhibition to clinical practice. Transl Stroke Res. 2010;1(3):170–7. Epub 2010/09/01.
Mandava P, Martini SR, Munoz M, Dalmeida W, Sarma AK, Anderson JA, et al. Hyperglycemia worsens outcome after rt-PA primarily in the large-vessel occlusive stroke subtype. Transl Stroke Res. 2014;5(4):519–25. Epub 2014/04/05.
Mandava P, Shah SD, Sarma AK, Dalmeida D, Kent TA. A pooled analysis indicates the promise and pitfalls of improving upon intravenous rt-PA for ischemic stroke. International Stroke Conference; 2014. San Diego: American Heart Association; 2014.
Compliance with Ethical Standards:
Funding
Computing resources of the Computational and Integrative Biomedical Research Center at Baylor College of Medicine were utilized for this study (P.M.).
Conflict of Interest
Drs. Mandava P and Kent TA are copyright holders of pPREDICTS. Drs. Shah SD and Sarma AK have no conflicts of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 34 kb)
Rights and permissions
About this article

Cite this article
Mandava, P., Shah, S.D., Sarma, A.K. et al. An Outcome Model for Intravenous rt-PA in Acute Ischemic Stroke. Transl. Stroke Res. 6, 451–457 (2015). https://doi.org/10.1007/s12975-015-0427-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12975-015-0427-5