
Abstract
Purpose
To evaluate the impact of the COVID-19 pandemic on Canadian intensive care unit (ICU) workers.
Methods
Between June and August 2020, we distributed a cross-sectional online survey of ICU workers evaluating the impact of the pandemic, coping strategies, symptoms of post-traumatic stress disorder (PTSD; Impact of Events Scale-Revised), and psychological distress, anxiety, and depression (Kessler Psychological Distress Scale). We performed regression analyses to determine the predictors of psychological symptoms.
Results
We analyzed responses from 455 ICU workers (80% women; 67% from Ontario; 279 nurses, 69 physicians, and 107 other healthcare professionals). Respondents felt that their job put them at great risk of exposure (60%), were concerned about transmitting COVID-19 to family members (76%), felt more stressed at work (67%), and considered leaving their job (37%). Overall, 25% had probable PTSD and 18% had minimal or greater psychological distress. Nurses were more likely to report PTSD symptoms (33%) and psychological distress (23%) than physicians (5% for both) and other health disciplines professionals (19% and 14%). Variables associated with PTSD and psychological distress included female sex (beta-coefficient [B], 1.59; 95% confidence interval [CI], 1.20 to 2.10 and B, 3.79; 95% CI, 1.79 to 5.78, respectively; P < 0.001 for differences in scores across groups) and perceived increased risk due to PPE shortage or inadequate PPE training (B, 1.87; 95% CI, 1.51 to 2.31 and B, 4.88; 95% CI, 3.34 to 6.43, respectively). Coping strategies included talking to friends/family/colleagues (80%), learning about COVID-19 (78%), and physical exercise (68%). Over half endorsed the following workplace strategies as valuable: hospital-provided scrubs, clear communication and protocols by hospitals, knowing their voice is heard, subsidized parking, and gestures of appreciation from leadership.
Conclusions
This survey study shows that ICU workers have been impacted by the COVID-19 pandemic with high levels of stress and psychological burden. Respondents endorsed communication, protocols, and appreciation from leadership as helpful mitigating strategies.
Résumé
Objectif
Évaluer l’impact de la pandémie de COVID-19 sur les travailleurs canadiens des unités de soins intensifs (USI).
Méthode
Entre juin et août 2020, nous avons fait parvenir un sondage transversal en ligne aux travailleurs des soins intensifs pour évaluer l’impact de la pandémie, les stratégies d’adaptation et les symptômes de stress post-traumatique (SPT; Échelle révisée de l’impact de l’événement - IES-R), ainsi que la détresse psychologique, l’anxiété et la dépression (Échelle de détresse psychologique de Kessler). Nous avons réalisé des analyses de régression pour déterminer les prédicteurs de symptômes psychologiques.
Résultats
Nous avons analysé les réponses de 455 travailleurs des soins intensifs (80 % de femmes; 67 % de l’Ontario; 279 infirmières/infirmiers, 69 médecins et 107 autres professionnels de la santé). Les répondants ont estimé que leur emploi les plaçait face à un risque élevé d’exposition (60 %), craignaient de transmettre la COVID-19 aux membres de leur famille (76 %), se sentaient plus stressés au travail (67 %) et avaient envisagé de quitter leur emploi (37 %). Dans l’ensemble, 25 % souffraient probablement d’un SPT et 18 % présentaient une détresse psychologique minimale ou supérieure. Les infirmières et infirmiers étaient plus susceptibles de rapporter des symptômes de SPT (33 %) et de détresse psychologique (23 %) que les médecins (5 % pour les deux) et les professionnels de la santé des autres disciplines (19 % et 14 %). Les variables associées à un SPT et à la détresse psychologique comprenaient le sexe féminin (coefficient bêta [B], 1,59; intervalle de confiance [IC] à 95 %, 1,20 à 2,10 et B, 3,79; IC 95 %, 1,79 à 5,78, respectivement; P < 0,001 pour les différences de scores entre les groupes) et la perception d’un risque accru en raison des pénuries d’EPI ou d’une formation inadéquate en EPI (B, 1,87; IC 95 %, 1,51 à 2,31 et B, 4,88; IC 95 %, 3,34 à 6,43, respectivement). Les stratégies d’adaptation comprenaient le fait de parler aux amis, à la famille ou aux collègues (80 %), l’acquisition de connaissances concernant la COVID-19 (78 %) et l’exercice physique (68 %). Plus de la moitié ont estimé que les stratégies de travail suivantes étaient utiles : des uniformes fournis par les hôpitaux, une communication et des protocoles clairs de la part des hôpitaux, le fait de savoir que leur voix est entendue, un stationnement subventionné et des gestes d’appréciation de la part des dirigeants.
Conclusion
Cette étude montre que les travailleurs des soins intensifs ont été touchés par la pandémie de COVID-19 avec des niveaux élevés de stress et de fardeau psychologique. Les répondants ont déclaré que la communication, les protocoles et les gestes d’appréciation de la direction constituaient des stratégies d’atténuation utiles.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The COVID-19 pandemic has infected more than 250 million people and killed more than 5 million worldwide.Footnote 1 Intensive care unit (ICU) workers around the globe are stepping up to care for patients despite fatigue, personal and family risk, a shortage of personal protective equipment (PPE), and rapidly changing policies.1 Additional sources of stress may include uncertainty, misinformation, stigma, interpersonal isolation, and distrust of official communications.2 The need to wear PPE for prolonged periods is cumbersome and uncomfortable.3 Further, unprecedented restrictions, including social distancing, quarantine, and isolation, may affect an individual’s ability to cope.
Since March 2020, ICUs across Canada have been on high alert, either providing care for COVID-19 patients or engaging in pandemic preparedness. Rapid spread has exceeded the capacity of many ICUs and has led to ethical dilemmas related to triage and end-of-life care.4 Healthcare workers are faced with a rapidly changing situation and the barrage of emails, news items, and social media can be overwhelming. Intensive care unit workers are experiencing a range of emotions, including fears for themselves and their families.5
The COVID-19 pandemic has added additional stressors to the existing occupational stress faced by ICU workers. Intensive care unit workers anticipated they would be overwhelmed by the number of mechanically ventilated patients and are exposed to high-risk procedures such as endotracheal intubation and extubation. A Chinese study reported high rates of depression (50%), anxiety (45%), insomnia (34%), and distress (72%) in healthcare professionals (HCPs) who treated COVID-19 patients, particularly in women, nurses, and workers in Wuhan, where the pandemic is reported to have started.6
To effectively support frontline workers facing the highest risk during pandemics of emerging infections, we must understand their challenges and needs. Effective support will require an understanding of the psychological effects of the pandemic, their strategies to cope with fear and worry, and which strategies could help lessen their fear and anxiety. The purpose of this study was to evaluate work-related and personal concerns of workers in Canadian ICUs regarding the COVID-19 pandemic and the associated psychological impact of these concerns.
Methods
The study was approved by the Mount Sinai Hospital Research Ethics Board (#20-0089-E; April 2020). The need for informed consent was waived; completion of the questionnaire implied consent.
Survey development
We report survey methodology using the checklist for reporting results of internet e-surveys (CHERRIES) (Electronic Supplementary Material [ESM], eAppendix 1).7 The survey instrument (Study of Healthcare Workers’ Perception of Risk and Preventive Measures for SARS) was used by researchers in several countries during the 2003 SARS outbreak,8 including members of our team.9,10 Because the SARS outbreak was unprecedented and because the information required was specific to the outbreak, there was no opportunity to validate the survey against other measures of coping and perceived risk. The survey therefore has only face validity. For the current study, we modified the original version by deleting non-applicable questions and adding new questions based on review of published COVID-19 literature and concerns/issues identified by local and global ICU personnel.5,6,11,12,13,14,15 The adapted survey includes approximately 80 attitude statements regarding infection control procedures, perceived risk, and coping strategies, and opportunities to provide open-ended comments (ESM, eAppendix 2). Since the survey was adapted from an existing instrument that was used to evaluate the impact of the SARS outbreak on healthcare workers,8,9,10 we did not perform clinical sensibility testing.
We also administered two validated tools to assess post-traumatic stress disorder (PTSD) symptoms (Impact of Events Scale-Revised [IES-R]) and psychological distress (Kessler Psychological Distress Scale [K10]). The IES-R is a 22-question scale with a scoring range of 0–24. Impact of Events Scale-Revised cut-off scores of < 24 represent no clinical concern, 24–32 represent clinical concern, and ≥ 33 represent probable PTSD.16 The K10 is a 10-question screening scale of psychological distress, and includes subscales for depression and anxiety.17 For the K10, total scores of 10–19, 20–24, 25–29, and 30–50 were used to categorize no, mild, moderate, and severe psychological distress, respectively.18
All study investigators and a sample of ICU physicians, nurses, and other HCPs reviewed the survey for clarity, comprehensiveness, and redundancy. Then, the survey was pilot tested by frontline ICU workers (seven physicians, five nurses, three health disciplines professionals). The final survey was distributed by NoviSurvey® (Cambridge, MA, USA).
Survey distribution
An email invitation was sent to potential respondents in June 2020, with two monthly reminders in July and August 2020. The email invitation was sent to: 1) members of the Canadian Critical Care Trials Group (www.CCCTG.ca; > 350 members), 2) members of the Canadian Critical Care Society (www.canadiancriticalcare.org; 256 members), and 3) all ICU directors across Canada, who were requested to distribute the survey to the interprofessional members of their ICU.
Statistical analysis
Data are presented using descriptive statistics, including distributions, means, standard deviation (SD), and confidence intervals (CIs). We report the K10 total score as well as depression and anxiety subscores using descriptive statistics. We performed independent-samples Kruskal–Wallis tests to compare nursing professionals, physicians, and other health discipline professionals on the K10 total score, K10 subscore, and total IES-R score. Predictors of psychological symptoms were assessed using linear regression analyses. We selected predictors of interest according to their potential relevance to ICU workers and from recent publications pertaining to COVID-19 and healthcare workers (age, sex, years of practice, direct contact, children at home). All variables were entered in the initial regression model and those that yielded an association with the outcome variables with a P value < 0.1 were retained in the final model using a backward selection method. Data were analyzed using Statistical Package for Social Sciences Version 25.0 (IBM Corp, 2017; Armonk, NY, USA). Two investigators (K.H., D.L.) performed thematic content analysis of all open-ended responses to generate themes and subthemes.19
Results
Respondents
Of the 485 respondents who accessed the survey, 455 responded to at least one question beyond the background and demographic questions. We limited our analysis to those 455 respondents. Respondents were from nine provinces, 67% from Ontario, and were approximately equally distributed regarding the population of their city (Table 1). Both community (38% teaching and 21% non-teaching) and university-affiliated hospitals (41%) were represented. Most respondents worked in small–moderate sized hospitals, but 32% worked in hospitals that had more than 500 beds. Most respondents were working in mixed medical-surgical ICUs that provide care for adult patients; only six respondents worked in a dedicated COVID-19 ICU. Overall, 62% (281/472) of respondents stated that they expanded their ICU bed capacity during the first COVID-19 wave; most expanded by ≤ 50%.
Eighty percent of respondents were women, and there was a wide age distribution (51% respondents were 40 yr of age or younger; Table 2); 61% were nurses, 15% were physicians, and the remainder were respiratory therapists (7%), other health disciplines professionals, which included ICU pharmacists, occupational therapists, physiotherapists, and personal support workers (6%), or clerical, research, and administrative staff (10%). The number of years of healthcare experience was widely distributed. Eighty-six percent identified as White, 76% were married or in common-law relationships, and of 289 (64%) who had children, most of these (n = 204) had children residing with them. Three-quarters (76%) had an undergraduate or professional/graduate degree.
Personal and workplace experiences
Although none of the respondents were diagnosed with COVID-19 infection, 50% personally knew someone who had been diagnosed with COVID-19. These people were a colleague (n = 156; 35%), an acquaintance (n = 58; 13%), a community member (n = 55; 12%), a close friend (n = 38; 8%), or an immediate family member (n = 15; 3%). In their workplace, 76% respondents had direct contact with a suspected or confirmed COVID-19 patient; and 36% reported exposure daily or a few times weekly.
Sixty percent of respondents agreed or strongly agreed that their job had put them at great risk of exposure, and 58% were afraid of falling ill with COVID-19 (Fig. 1). Overall, 35% were preoccupied with their symptoms, and a similar percentage believed that they have little control over whether they become ill. More than half (56%) accepted the risk of getting COVID-19 as part of their job. Twenty-six percent and 18% believed they had greater chances of dying from COVID-19 over the subsequent year than from cancer or a traffic accident, respectively; however, few (9%) believed their chances of survival would be poor if they contracted COVID-19. Despite their fears, very few respondents (7%) agreed or strongly agreed they should not have been caring for patients with COVID-19.

Critical care workers’ perceptions of personal risk related to COVID-19 exposure in their workplace
Regarding their risk of transmitting COVID-19 to people close to them, 76%, 52%, 50%, and 35% expressed concern about risk to their family members, close friends, work colleagues, and patients, respectively. Approximately one in four respondents (28%) was afraid to tell their family about their exposure risk, and 67% expressed that people close to them were worried about the respondent’s health. Social stigma was a concern, because 54% of respondents agreed or strongly agreed that people had avoided them because of their job.
Perceptions about work environment, preparation, and appreciation
Although 44% felt that there was more conflict among colleagues, a similar percentage perceived good morale (Fig. 2). Two-thirds felt more stressed at work, and 37% had thought about leaving their job. Between 42% and 52% reported an increased workload, including working overtime and having to do work they do not normally do. Nevertheless, 55% felt there was adequate staffing. Most respondents reported they were adequately trained in PPE use (82%) and removal (81%), and 74% had access to a resource person for PPE assistance; 60% reported the availability of counselling if needed. Regarding recognition of their work, 62% and 45% felt appreciated by society and by their hospital, respectively, but only 36% were confident that their employer would look after their medical needs if they were to fall ill with COVID-19.

Critical care workers’ perceptions regarding work environment, workload, and personal protective equipment (PPE)
Coping strategies and suggested initiatives
The most commonly reported strategies for personal coping (strongly agree or agree) included talking to friends, family, and colleagues (81%), learning about COVID-19 (78%), exercising (68%), keeping a positive mindset (65%), accepting the inherent risk (55%), and trying not to think about the risk (49%) (Fig. 3). Almost half of respondents avoided social media (53%), and 39% avoided reading too much about COVID-19. Regarding potentially harmful strategies, 21% responded they used alcohol, marijuana, or other recreational drugs to help them cope.

Critical care workers’ coping strategies related to the COVID-19 pandemic
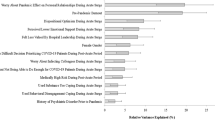
Preferred supportive strategies in the workplace reported by ≥ 50% respondents were scrubs provided by the hospital, clear communication, protocols, and procedures, knowing their voice is heard, free or subsidized parking, expressions of appreciation from leadership, and frequent team debriefs (Fig. 4).

Critical care workers perspectives on workplace strategies that would be helpful in coping during the COVID-19 pandemic
Post-traumatic stress and psychologic distress
The IES-R total score was higher in nurses and health disciplines professionals than in physicians (Table 3). Overall, 25% of respondents had an IES-R score ≥ 33, which indicates a probable diagnosis of PTSD; more nurses (33%) and other HCPs (19%) met this criterion than physicians (5%) did. Mean K10 total scores for all three groups (physicians, nurses, other HCPs) were within the range indicating no psychological distress (Table 3). Nevertheless, any degree of psychological distress (mild, moderate, or severe) was reported more frequently by nurses (23%) than by other HCPs (14%) and physicians (5%).
We conducted separate regression analyses to determine factors that were associated with psychological symptoms. Table 4 shows the final multivariate models. We identified four associations with PTSD: female sex, high-risk health status, living with a child or children, and feeling at increased risk because of PPE shortage or inadequate training. Regression analysis revealed five associations with psychological distress: younger age group, female sex, working in a community hospital, feeling at increased risk because of PPE shortage or inadequate training, and not living with a child or children.
Open-ended responses
Thematic content analysis of the open-ended questions identified three themes regarding the personal impact of the pandemic: personal coping and wellness, impact on family life, and relationship with the community. Four themes related to professional impact were: changes in the work environment, concerns about patient care and wellbeing, relationship with hospital leadership, and PPE (ESM, eAppendix 3).
Discussion
In this cross-sectional, web-based, self-administered survey of 455 personnel working in Canadian academic and non-academic ICUs, ICU personnel reported a significant burden of distress, including fear of contracting and transmitting COVID-19, and stigma associated with their professional roles. Overall, 37% respondents had PTSD symptoms, and 18% had psychological distress; women and nurses were at greatest risk. More than one-third of respondents had considered leaving their jobs.
Research by our team9,10 and others8 after the 2003 SARS outbreak reported that HCPs often experience effects of chronic stress, including burnout, absenteeism, and interpersonal problems, for months or years afterwards. The COVID-19 pandemic has been worse than the 2003 SARS outbreak because of a markedly higher number of cases, longer duration, longer duration of illness, and unprecedented population restrictions (social distancing, quarantine, isolation) that may have affected individuals’ coping. Another major difference from the SARS outbreak is the remarkable extent and speed of information distribution, enabled by social media.20 Although social media facilitates sharing of personal challenges faced by frontline workers and presents valuable opportunities for education, the sheer volume and rapid evolution as well as the ease of propagation of fake news and rumours may increase anxieties. Accordingly, approximately 50% of respondents stated that they avoided social media, and few reported posting on social media.
Most COVID-19 surveys have focused on physicians and nurses, with little exploration of the perspectives of other health professionals. Surveys of non-ICU HCPs from Canada,21 China,6,20,22 Italy,15 and the USA23 report high rates of psychological distress. Several surveys have explored the perspectives and mental health of ICU workers during the COVID-19 pandemic, with a few including validated mental health scales.5,24,25,26,27,28,29,30,31 In a cross-sectional survey of 1,058 HCPs (68% nurses, 29% physicians) who worked in 21 ICUs in France, Azoulay et al. administered three validated mental health tools.32 The rates of anxiety, depression, and peritraumatic dissociation were 50%, 30%, and 32%, respectively and were more prevalent in women than in men. The finding that women and nurses are at greater risk of psychological distress than men are is consistent across most studies.6,15,24,25,27,28,30,31,32,33 This may reflect greater and more prolonged direct exposure of nurses than other HCPs to COVID-19 patients, which may be intensified by the disproportionate burden of family and domestic responsibilities shouldered by women.34
Resource and personnel constraints have been associated with psychological distress.3 In surveys of ICU clinicians in the USA, the most important reported concerns were shortages of PPE and ICU staffing.5,26,35 In an international survey of 2,700 respondents, PPE and nurse shortages were associated with greater burnout.24 In a survey of approximately 600 Canadian HCPs, perceived inadequacy of PPE and infection control procedures was associated with higher anxiety scores.36 In our study, more than 80% responded that they had received adequate PPE training. Nevertheless, perceived PPE shortage or inadequate PPE training was significantly associated with psychological distress and PTSD.
Personal and institutional support strategies can improve resilience and mitigate the psychological effects of COVID-19 on healthcare workers.37,38,39 In our study, peer support (talking to family, friends, colleagues) and exercise were the two most commonly reported personal coping strategies. A single centre study from New York City also found that exercise was the most common stress-reducing behaviour reported by survey respondents.23 Pandemic stressors can also promote the rise in substance use disorders, drug overdoses, and suicides.40 In our study, indulging in potentially harmful (alcohol, marijuana, recreational drugs) coping strategies was reported by approximately 20% of respondents.
Institutional trust is foundational for the worker-employer relationship; workers are more motivated if they have confidence in the protection provided by their government and hospital.41 Fewer than half of respondents felt appreciated by their hospital, and only 35% were confident that their employer would look after their medical needs if they were to fall ill with COVID-19. When asked about institutional supportive strategies, respondents prioritized consistent unambiguous messaging, the presence of leaders at the frontline, having their voices valued, and expressions of appreciation for their work. Our findings underscore the need for healthcare organizations to build trust with workers. Underpinning principles of trust include effective and rapid communication, responsiveness to their needs, and reassurance of appropriate medical and financial support if they contract COVID-19. Other focuses should include destigmatizing mental health issues and equitable access to professional counsellors.
This study has captured data amid an unprecedented challenge for ICU workers. The strengths of this study include the large number of respondents from across Canada, and representation of community and academic ICUs. We sought interdisciplinary input from ICU HCPs (nurses, physicians, respiratory therapists, pharmacists) and other integral frontline staff (e.g., clerical and research) who have not yet been included in research on pandemic stress. We used a survey that was used during the previous SARS pandemic and revised it to reflect specific COVID-19 pandemic stressors. We also included validated scales for PTSD and psychological distress and asked respondents about personal and institutional supportive strategies. Our study has some limitations—the survey was available in English only, the response rate was not known, and more than two-thirds of respondents worked in Ontario ICUs. Most respondents were women, which may reflect the usual sex distribution of HCPs, but we cannot exclude responder bias. Because most respondents were White, we were unable to evaluate racial determinants of responses. Similarly, the relatively small number of physicians may preclude definitive conclusions about the impact of the pandemic in that profession. Furthermore, it is possible that non-respondents were considerably less distressed by the pandemic than respondents were, which may have led to an overestimation of the impact of the pandemic on ICU workers. Furthermore, the findings are based on self-reported symptomatology according to validated psychological instruments and are not considered diagnostic of depression, anxiety, or PTSD. Finally, this survey was distributed early in the pandemic, and the impact of COVID-19 may be even more pronounced now; conversely, increasing vaccination rates may have reduced HCP’s stress, although a survey of non-ICU HCWs did not find an effect.42 It will be important to explore these issues and the impact of the pandemic on long-term psychological morbidity.
Conclusions
Personnel working in the Canadian healthcare system deserve the right support at the right time. The findings of this study will enable a comprehensive and thoughtful response to the psychological needs of ICU workers, with consequent benefits to society in both the short- and long-term. Intensive care units and public health systems can respond to these findings with targeted interventions such as education, training, counselling, social support (such as childcare), or increased involvement of affected groups in pandemic planning. This study will help to build a foundation for the creation of effective strategies to protect the psychological safety of essential ICU workers during and after the COVID-19 pandemic, and in future pandemics.
Notes
Johns Hopkins Coronavirus Resource Center. November 2021. Available from URL: https://coronavirus.jhu.edu/map.html (accessed November 2021).
References
Mehta S, Machado F, Kwizera A, et al. COVID-19: a heavy toll on health-care workers. Lancet Respir Med 2021; 9: 226-8.
Cabrini L, Grasselli G, Cecconi M; COVID-19 Lombardy ICU Network. Yesterday heroes, today plague doctors: the dark side of celebration. Intensive Care Med 2020; 46: 1790-1.
Tabah A, Ramanan M, Laupland KB, et al. Personal protective equipment and intensive care unit healthcare worker safety in the COVID-19 era (PPE-SAFE): an international survey. J Crit Care 2020; 59: 70-5.
Robert R, Kentish-Barnes N, Boyer A, Laurent A, Azoulay E, Reignier J. Ethical dilemmas due to the Covid-19 pandemic. Ann Intensive Care 2020; DOI: https://doi.org/10.1186/s13613-020-00702-7.
Kleinpell R, Ferraro DM, Maves RC, et al. Coronavirus disease 2019 pandemic measures: reports from a national survey of 9,120 ICU clinicians. Crit Care Med 2020; 48: e846-55.
Lai J, Ma S, Wang Y, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open 2020; DOI: https://doi.org/10.1001/jamanetworkopen.2020.3976.
Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet e-surveys (CHERRIES). J Med Internet Res 2004; DOI: https://doi.org/10.2196/jmir.6.3.e34.
Koh D, Lim MK, Chia SE, et al. Risk perception and impact of severe acute respiratory syndrome (SARS) on work and personal lives of healthcare workers in Singapore: what can we learn? Med Care 2005; 43: 676-82.
Maunder R. The experience of the 2003 SARS outbreak as a traumatic stress among frontline healthcare workers in Toronto: lessons learned. Philos Trans R Soc Lond B Biol Sci 2004; 359: 1117-25.
Maunder RG, Lancee WJ, Balderson KE, et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg Infect Dis 2006; 12: 1924-32.
Azoulay E, De Waele J, Ferrer R, et al. Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak. Ann Intensive Care 2020; DOI: https://doi.org/10.1186/s13613-020-00722-3.
Carmassi C, Foghi C, Dell'Oste V, et al. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: what can we expect after the COVID-19 pandemic. Psychiatry Res 2020; DOI: https://doi.org/10.1016/j.psychres.2020.113312.
Chew NW, Lee GK, Tan BY, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun 2020; 88: 559-65.
De Sio S, Buomprisco G, La Torre G, et al. The impact of COVID-19 on doctors' well-being: results of a web survey during the lockdown in Italy. Eur Rev Med Pharmacol Sci 2020; 24: 7869-79.
Giusti EM, Pedroli E, D'Aniello GE, et al. The psychological impact of the COVID-19 outbreak on health professionals: a cross-sectional study. Front Psychol 2020; DOI: https://doi.org/10.3389/fpsyg.2020.01684.
Weiss DS, Marmar CR. The impact of even scale-revised. In: Wilson JP, Keane TM (Eds). Assessing Psychological Trauma and PTSD: A Practitioner’s Handbook. New York: Guilford Press; 1997: 399-411.
Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med 2002; 32: 959-76.
NovoPsych. The Kessler Psychological Distress Scale (K10); 2021. Available from URL: https://novopsych.com.au/assessments/outcome-monitoring/the-kessler-psychological-distress-scale-k10/ (accessed November 2021).
Braun V, Clarke V. What can "thematic analysis" offer health and wellbeing researchers? Int J Qual Stud Health Well-being 2014; DOI: https://doi.org/10.3402/qhw.v9.26152.
Merchant RM, South EC, Lurie N. Public health messaging in an era of social media. JAMA 2021; 325: 223-4.
Statistics Canada. Mental health among health care workers in Canada during the COVID-19 pandemic; 2021. Available from URL: https://www150.statcan.gc.ca/n1/en/daily-quotidien/210202/dq210202a-eng.pdf?st=F_m06Cxg (accessed November 2021).
Kang L, Ma S, Chen M, et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: a cross-sectional study. Brain Behav Immun 2020; 87: 11-7.
Shechter A, Diaz F, Moise N, et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen Hosp Psychiatry 2020; 66: 1-8.
Wahlster S, Sharma M, Lewis AK, et al. The coronavirus disease 2019 pandemic's effect on critical care resources and health-care providers: a global survey. Chest 2021; 159: 619-33.
Kok N, Hoedemaekers A, van der Hoeven H, Zegers M, van Gurp J. Recognizing and supporting morally injured ICU professionals during the COVID-19 pandemic. Intensive Care Med 2020; 46: 1653-4.
Kaplan LJ, Kleinpell R, Maves RC, Doersam JK, Raman R, Ferraro DM. Critical care clinician reports on coronavirus disease 2019: results from a national survey of 4,875 ICU providers. Crit Care Explor 2020; DOI: https://doi.org/10.1097/CCE.0000000000000125.
Acar Sevinc S, Metin S, Balta Basi N, Surhan Cinar A, Turkel Ozkan M, Oba S. Anxiety and burnout in anesthetists and intensive care unit nurses during the COVID-19 pandemic: a cross-sectional study. Braz J Anesthesiol 2021; DOI: https://doi.org/10.1016/j.bjane.2021.07.011.
Binnie A, Moura K, Moura C, D'Aragon F, Tsang JL. Psychosocial distress amongst Canadian intensive care unit healthcare workers during the acceleration phase of the COVID-19 pandemic. PLoS One 2021; DOI: https://doi.org/10.1371/journal.pone.0254708.
Garcia-Hedrera FJ, Gil-Almagro F, Carmona-Monge FJ, et al. Intensive care unit professionals during the COVID-19 pandemic in Spain: social and work-related variables, COVID-19 symptoms, worries, and generalized anxiety levels. Acute Crit Care 2021; 36: 232-41.
Penacoba C, Velasco L, Catala P, et al. Resilience and anxiety among intensive care unit professionals during the COVID-19 pandemic. Nurs Crit Care 2021; DOI: https://doi.org/10.1111/nicc.12694.
Wozniak H, Benzakour L, Moullec G, et al. Mental health outcomes of ICU and non-ICU healthcare workers during the COVID-19 outbreak: a cross-sectional study. Ann Intensive Care 2021; DOI: https://doi.org/10.1186/s13613-021-00900-x.
Azoulay E, Cariou A, Bruneel F, et al. Symptoms of anxiety, depression, and peritraumatic dissociation in critical care clinicians managing patients with COVID-19. A cross-sectional study. Am J Respir Crit Care Med 2020; 202: 1388-98.
Pappa S, Ntella V, Giannakas T, et al. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun 2020; 88: 901-7.
Shafer K, Scheibling C, Milkie MA. The division of domestic labor before and during the COVID-19 pandemic in Canada: stagnation versus shifts in fathers' contributions. Can Rev Sociol 2020; 57: 523-49.
Gray BM, Vandergrift JL, Barnhart BJ, et al. Changes in stress and workplace shortages reported by U.S. critical care physicians treating coronavirus disease 2019 patients. Crit Care Med 2021; DOI: https://doi.org/10.1097/CCM.0000000000004974.
Smith PM, Oudyk J, Potter G, Mustard C. The association between the perceived adequacy of workplace infection control procedures and personal protective equipment with mental health symptoms: a cross-sectional survey of Canadian health-care workers during the covid-19 pandemic. Can J Psychiatry 2021; 66: 17-24.
Wu PE, Styra R, Gold WL. Mitigating the psychological effects of COVID-19 on health care workers. CMAJ 2020; 192: E459-60.
Jun J, Tucker S, Melnyk BM. Clinician mental health and well-being during global healthcare crises: evidence learned from prior epidemics for COVID-19 Pandemic. Worldviews Evid Based Nurs 2020; 17: 182-4.
Albott CS, Wozniak JR, McGlinch BP, Wall MH, Gold BS, Vinogradov S. Battle buddies: rapid deployment of a psychological resilience intervention for health care workers during the COVID-19 pandemic. Anesth Analg 2020; 131: 43-54.
Czeisler ME, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep 2020; 69: 1049-57.
Imai H. Trust is a key factor in the willingness of health professionals to work during the COVID-19 outbreak: experience from the H1N1 pandemic in Japan 2009. Psychiatry Clin Neurosci 2020; 74: 329-30.
Jordan JA, Shannon C, Browne D, et al. COVID-19 Staff Wellbeing Survey: longitudinal survey of psychological well-being among health and social care staff in Northern Ireland during the COVID-19 pandemic. BJPsych Open 2021; DOI: https://doi.org/10.1192/bjo.2021.988.
Horowitz M, Wilner N, Alvarez W. Impact of event scale: a measure of subjective stress. Psychosom Med 1979; 41: 209-18.
Author contributions
Sangeeta Mehta conceived and designed the study. Sangeeta Mehta, Christopher Yarnell, Sumesh Shah, Peter Dodek, Jeanna Parsons-Leigh, Robert Maunder, Jessica Kayitesi, Catherine Eta-Ndu, and Kimia Honarmand participated in study design and reviewed and refined the survey. Robert Maunder provided expertise in psychological outcomes and impact of pandemics on healthcare workers. Sangeeta Mehta, Kimia Honarmand, Fran Priestap, Danielle LeBlanc, and Jennifer Chen performed quantitative data analysis. Danielle LeBlanc and Kimia Honarmand performed qualitative data analysis. All authors contributed to manuscript preparation/revision, approved the final version to be published, and agree to be accountable for all aspects of the work.
Acknowledgements
We thank our colleagues Dr. Marica Tucci and Ms. Nicole Zytaruk for their thoughtful review of the manuscript. We thank Mr. Kiyan Heybati for assistance with the figures.
Disclosures
None.
Funding statement
None.
Editorial responsibility
This submission was handled by Dr. Ronald B. George, Associate Editor, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mehta, S., Yarnell, C., Shah, S. et al. The impact of the COVID-19 pandemic on intensive care unit workers: a nationwide survey. Can J Anesth/J Can Anesth 69, 472–484 (2022). https://doi.org/10.1007/s12630-021-02175-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-021-02175-z