
Abstract
Purpose
The objective of this study was to assess if an increase in electrical impedance was associated with intraneural (sub-epineural) needle tip placement.
Methods
Two electrical impedance measurements were carried out in each of 140 peripheral nerve blocks. The first measurement was performed at a distance of 0.5-1 cm from the nerve trunk (reference value), and the second measurement was performed close to the nerve, either immediately before local anesthetic injection if no nerve puncture was suspected, or immediately before repositioning the needle if nerve puncture was suspected. Nerve puncture was suspected if any one of the following indications was present: pain or paresthesia; motor responses with a minimal stimulating current < 0.4 mA; needle tip observed inside the nerve using ultrasound; nerve swelling after injection of local anesthetic. Electrical impedance variations were compared between the no puncture and the suspected puncture groups.
Results
Nerve puncture was suspected in 21 cases. The median variation [quartiles] of electrical impedance was +6.6% [−20; 36%] in the suspected puncture group (n = 21) and −10.0% [−28; 0%] in the no puncture group (n = 119) (P = 0.02). Absolute values of electrical impedance close to the nerve were greater in the suspected puncture group (15.5 kΩ [12.0; 18.0 kΩ]) vs the no puncture group (12.0 kΩ [8.9; 15.1% kΩ]) (P = 0.013). A receiver operating characteristic (ROC) curve was constructed, and the optimal cut-off for impedance was +4.3%.
Conclusion
A > 4.3% increase in electrical impedance may indicate accidental nerve puncture during peripheral nerve block.
Résumé
Objectif
L’objectif de cette étude était de déterminer si une augmentation de l’impédance électrique était associée au positionnement intraneural (sous-épineural) de la pointe de l’aiguille.
Méthode
Deux mesures de l’impédance électrique ont été réalisées lors de 140 blocs nerveux périphériques. La première mesure a été prise à une distance de 0,5-1 cm du tronc nerveux (valeur de référence), et la seconde a été prise près du nerf, soit immédiatement avant l’injection d’agent anesthésique local si aucune ponction nerveuse n’était soupçonnée, soit immédiatement avant le repositionnement de l’aiguille en cas de suspicion de ponction nerveuse. La ponction nerveuse a été soupçonnée si l’une des indications suivantes était présente : douleur ou paresthésie; réactions motrices avec un courant de stimulation minimal < 0,4 mA; observation de la pointe de l’aiguille dans le nerf grâce à l’échoguidage; gonflement du nerf après injection de l’anesthésique local. Les variations d’impédance électrique ont été comparées entre les groupes sans ponction et avec suspicion de ponction.
Résultats
Une ponction nerveuse a été soupçonnée dans 21 cas. La variation médiane [quartiles] de l’impédance électrique était de +6,6 % [−20; 36 %] dans le groupe ponction soupçonnée (n = 21) et de −10,0 % [−28; 0 %] dans le groupe sans ponction (n = 119) (P = 0,02). Les valeurs absolues d’impédance électrique près du nerf étaient plus élevées dans le groupe ponction soupçonnée (15,5 kΩ [12,0; 18,0 kΩ]) que dans le groupe sans ponction (12,0 kΩ [8,9; 15,1 kΩ]) (P = 0,013). Une courbe d’efficacité de l’observateur (ROC) a été créée, et la limite d’inclusion optimale pour l’impédance était de +4,3 %.
Conclusion
Une augmentation > 4,3 % de l’impédance électrique pourrait indiquer une ponction nerveuse accidentelle pendant un bloc nerveux périphérique.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Peripheral nerve injury is a rare1,2 but serious complication of regional anesthesia. Needle penetration into a nerve is an infrequent occurrence while performing a peripheral nerve block (PNB). It does not necessarily result in fascicular damage,3,4 and the outcome is usually benign. Nevertheless, this complication remains a significant legal issue associated with regional anesthesia, with devastating consequences for the patient. Several methods are currently available to prevent nerve injury while performing PNB, including testing for paresthesia, using a peripheral nerve stimulator and/or ultrasound guidance, and monitoring the injection pressure while administering the local anesthetic. Unfortunately, no nerve localization or monitoring technique has been shown to be clearly superior for reducing the frequency of clinical injury,5 and nerve injury may occur even when these techniques are applied.6-10
Interestingly, a study using a porcine model showed that electrical impedance (EI) measured by nerve stimulators was significantly lower extraneurally than intraneurally when using ultrasound guidance.11 Electrical impedance describes tissue opposition to alternating current and depends mainly on tissue composition, primarily due to the variation in water and lipid content.12 When the tip of the insulated needle is outside the nerve, current flow spreads in all three dimensions in the tissue surrounding the nerve; therefore, EI is low. Conversely, the needle tip is isolated when it penetrates the nerve, and the low-impedance path for the electrical current is no longer available; therefore, EI is high. During PNB, nerve stimulators are designed to deliver specific calibrated electrical signals, i.e., they produce a constant current (I) regardless of variations in resistance (R) via insulated needles. Recently, nerve stimulators available in clinical practice (Stimuplex HNS 12, B. Braun Medical, Bethlehem, PA, USA) have displayed EI values in real time. Electrical impedance for pulsatile stimulation is calculated according to Ohm’s law by dividing the maximum voltage developed at the end of the current pulse (V) by the known applied current intensity (I).13
We hypothesized that intraneural needle tip placement (the epineurium is then crossed) would be associated with an increase in EI and that the EI variations could help in the diagnosis of accidental nerve puncture.
Methods
We carried out a prospective observational study in our institution (Limoges University Hospital Center, France) during May to November 2010 to assess the feasibility of using EI during nerve localization. This study was approved by the CHU de Limoges Ethics Committee (number 47-2010-05) on May 5, 2010. Since this was an observational study, the Ethics Committee also approved the authors’ proposal to obtain patient consent verbally. Patients were given an information sheet about their participation in the study.
We compared variations in EI between patients with no suspicion of intraneural puncture vs patients with suspected nerve puncture. Since we did not know the precise incidence of nerve puncture during PNB, we were unable to calculate a priori the number of patients needed to show a difference of EI between the two groups.
All patients requiring PNB could be included in our study. In addition, different types of nerve blocks were performed depending on the surgical procedure (interscalene, supraclavicular, infraclavicular, axillary, and nerve blocks in the forearm, femoral, popliteal, and tibial blocks at the ankle). Ultrasound guidance (S-Nerve, Sonosite Inc., Bothell, WA, USA) with a HFL 38x 13-6 MHz linear array probe was used for nerve or plexus localization, and only an in-plane needle approach was used. Nerve stimulation (Stimuplex HNS 12, B. Braun Medical, Bethlehem, PA, USA) was also used for all PNBs. To standardize EI measurements, the nerve stimulator was set at 1 Hz, 0.5 mA, and 0.1 msec, and if muscular twitches were obtained, the intensity of the minimal stimulating current was recorded. Only short bevelled needles were used, and length was chosen depending on block site and the patient’s morphology. The type of local anesthetic solution and the agents used for sedation were chosen by the anesthesiologist in charge of the patient. For patients with blocks involving more than one injection, we made measurements for the first injection only.
Demographic data and information about the PNB performed (type of block and local anesthetic solution used) were collected. Our primary outcome was relative EI variation. For EI measurements, we made a first measure at a distance of 0.5-1 cm from the nerve; this measurement was then used as a reference value outside the nerve. A second measurement was taken either immediately before local anesthetic injection if no nerve puncture was suspected, or immediately before repositioning the needle if nerve puncture occurred. Finally, the relative variation between the two measurements was calculated using the following formula: EI at injection – EI at distance from the nerve / EI at distance from the nerve. The criteria for nerve puncture were: pain or paresthesia in the sensory territory of the targeted nerve; motor responses with a minimal stimulating current lower than 0.4 mA; needle tip seen inside the nerve using ultrasound guidance; and/or nerve swelling after injection of local anesthetics. If at least one of the above criteria occurred, the patient was included in the “suspected nerve puncture group”. All other patients were included in the “no nerve puncture group”.
Statistical analysis
The statistical analyses were performed using R software version 2.10.1 (R foundation for statistical computing, www.r-project.org). The continuous covariates were expressed in terms of median and [quartiles], and the categorical variables were expressed in terms of number (%). A Wilcoxon paired test was used to compare EI at distance vs during injection, and a generalized linear model was used to investigate the influence of demographic covariates on relative EI. Results were expressed in terms of β (standard deviation [SD]). A Mann-Whitney test was performed to compare the median relative EI variation in the “no nerve puncture group” vs the “suspected nerve puncture group”. The P values are two sided, and 95% confidence intervals were calculated when relevant. A receiver operating characteristic curve (ROC) was constructed using Medcalc® (Mariakerke, Belgium) version 11.3.6 software to determine a threshold EI value for nerve puncture diagnosis with satisfactory sensitivity, specificity, and positive and negative predictive values.
Results
One hundred thirty-three patients participated in the study and 135 PNBs were performed. One patient received a rescue block and one patient underwent two surgeries. Five patients had two nerves blocked in the forearm with one injection for each nerve; therefore, two pairs of EI values were measured in these patients, and as a result, 140 pairs of EI values were collected.
Fifty-three (40%) women and 80 (60%) men were included in the study; only eight patients (6%) were diabetics. Demographic data are shown in Table 1. One hundred PNBs were performed on the upper limb, and 40 were performed on the lower limb (Table 1). The median relative EI variation for all patients was −8% [−28; −4%].
For all patients, EI reference values (measured 0.5-1 cm from the nerve) were extremely heterogeneous. Median EI was 14.0 kΩ and ranged from 5.2-81.3 kΩ. Furthermore, extraneural EI references were significantly higher in the popliteal fossa than in the other anatomical locations (Mann-Whitney test, P < 0.05). Median EI was less on injection (12.2 kΩ [9.0; 15.5 kΩ] vs at a distance from the nerve (14.0 kΩ [Q1; Q3: 12.0; 18.0]; P = 0.0009), Wilcoxon rank test (for dependent measures).
Generalized linear analysis showed that neither sex [male vs female, β = −0.06 (SD 0.05); P = 0.27] nor age [per year increase, β = 0.0004 (0.001); P = 0.77], nor body mass index (BMI) [per unit increase, β = −0.006 (0.006); P = 0.36], nor diabetes (no vs yes, β = 0.17 (0.10); P = 0.10] affected EI relative variation measurements.
We observed at least one suspicious sign of intraneural puncture during each of 21 nerve blocks (Table 2). Six patients experienced pain or paresthesia in the sensitive distribution of the blocked nerve during the procedure, and in 15 cases, motor responses were observed with stimulating current < 0.4 mA. Two patients had both pain and paresthesia with a current < 0.4 mA. No nerve swelling was diagnosed after injection of 1 mL of the local anesthetic solution, although we twice observed accidental intraneural needle tip penetration. No nerve puncture was suspected in the remaining 119 blocks.
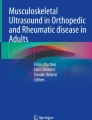
The EI variations were significantly different between the two groups. In the suspected puncture group, there was median increase of +6.6 % [−20.0; 36.0%], whereas the median EI variation was −10.0 % [−28.0; 0.0%] in the no puncture group (P = 0.02) (Fig. 1). Absolute values for EI were 15.5 kΩ [12.0; 18.0%] in the suspected puncture group and 12.0 kΩ [8.9; 15.1%] in the no puncture group (P = 0.013).

Relative electrical impedance variation (%) depending on whether a nerve puncture criterion is present (right) or not (left). The line in the rectangle represents the median; the rectangles show the quartiles, and the whiskers represent the minimum and maximum values
A ROC curve analysis was performed (Fig. 2). The area under the curve was 0.67 (95% confidence interval 0.58 to 0.75; P = 0.03). With a +4.3% threshold, the sensitivity, specificity, positive predictive values, and negative predictive values were 57%, 82%, 36%, and 92%, respectively.

Receiver operating characteristics curve (plot of sensitivity values against 1 – specificity values) for several relative electrical impedance variations
Discussion
Our study suggests that EI variations could be useful during the performance of ultrasound-guided nerve block. An increase in EI might be indicative of intraneural location, and extraneural positioning of the needle is usually associated with a decrease in EI.
Electrical impedance was first used by Thomas et al. in 1987 to identify the epidural space.14 More recently, two other studies evaluated EI variations measured by nerve stimulators. In one study, accidental vascular puncture was diagnosed,15 and in the other study, nerve puncture was detected during PNB in pigs.11 In our study, we assessed the use of EI in regional anesthesia in humans. Ultrasound evidence of intraneural puncture requires observer expertise,16 and other technologies are needed to help improve PNB safety.17,18
Our results confirm those of Tsui et al. 11 in an animal model. They found that the variation in EI displayed by the nerve stimulator is greater when the needle tip crosses the epineurium. We observed that the extraneural EI measured in our study (14.0 kΩ [12; 18 kΩ]) was lower than that reported by Chin et al. 15 [23.5 (8.3) kΩ]. One explanation for the difference could be that Chin et al. collected each measurement during supraclavicular nerve blocks, whereas we measured EI at many different body sites. The wide heterogeneity of EI values in our work (5.2-81.3 kΩ) might be explained by the various blocks performed. Indeed, a study that evaluated tissue EI along the median nerve revealed significant differences when EI was measured at the elbow vs the axilla,19 and this may be explained by differences in the distribution of muscle or fat. Electrical properties depend on the type of tissue through which the electric current travels.12 Moreover, muscles have a non-homogeneous electrical behaviour with a conductivity varying with muscle fibre orientation.20 This can explain why we observed highly variable EI values from one anatomical site to another in a same person or from one patient to another. Therefore, it is more relevant to detect relative rather than absolute values to compensate for intra-individual and interindividual sources of EI variations. We also observed that extraneural EI was higher when measured in the popliteal fossa than in other sites, probably because of the large amount of fat tissue surrounding the nerve. It is possible that EI has a better diagnostic performance when used in anatomical sites where extraneural tissue EI is low. Nevertheless, our small sample size did not allow us to verify this hypothesis. In order to establish optimal standardization of the extraneural EI measurement, it may be best to measure it in the subcutaneous fat that is present at the site of the nerve blockade.
The measurement of EI may be subject to errors because of electrical interference, a less than ideal electrical pathway through tissues, and differences between set and delivered current.21 The sources of error that can affect variations in EI measurements are not known at present.
We intended to determine a variation cut-off that would detect intraneural puncture reliably despite the small sample size in the “suspected nerve puncture” group. We focused on negative predictive value because, in our view, certainty that the needle is positioned outside the nerve is more useful than confirmation of a damaged nerve. We propose that a +4.3% cut-off is associated with a very good negative predictive value. We are aware that this is more of a theoretical value and that it is difficult to reach this value precisely in routinely practice. Nevertheless, one of our main objectives was to determine a first cut-off value for the diagnosis of intraneural injection.
Clearly, the most important limitation of our work lies in the choice of nerve puncture criteria. Since no gold standard is currently available, we relied on the criteria usually applied to suspect accidental nerve puncture during PNB. Each criterion is arguable4,16,22; but for ethical reasons, we could not perform voluntary nerve punctures, which could have reduced the variations in EI between the two groups. With our nerve puncture criteria, it is impossible to determine how often the diagnosis of nerve puncture was correct.
It was also not possible to distinguish between intra- and extrafascicular punctures. Nerve puncture does not invariably result in nerve damage, and it appears that intrafascicular injection is more deleterious than intraneural extrafascicular punctures.4 To date, no technique can convincingly make the difference. Therefore, as mentioned by Tsui et al.,11 further work should focus on differences between intra- and extrafascicular EI.
In conclusion, the present study suggests that EI measurements in regional anesthesia may be used to detect the difference between an extraneural or intraneural location and that nerve stimulators commonly used during PNB may be able to detect those differences. Thus, EI measurement may enhance PNB safety, although this needs to be confirmed by further work. We propose a relative EI cut-off of 4.3%, which is associated with a very good negative predictive value. Nevertheless, the optimal EI cut-off may depend on other factors, especially the type of block performed. We also propose that future work should focus on a single anatomical site.
References
Barrington MJ, Watts SA, Gledhill SR, et al. Preliminary results of the Australasian Regional Anaesthesia Collaboration: a prospective audit of more than 7000 peripheral nerve and plexus blocks for neurologic and other complications. Reg Anesth Pain Med 2009; 34: 534-41.
Auroy Y, Benhamou D, Bargues L, et al. Major complications of regional anesthesia in France: The SOS Regional Anesthesia Hotline Service. Anesthesiology 2002; 97: 1274-80.
Hogan QH. Pathophysiology of peripheral nerve injury during regional anesthesia. Reg Anesth Pain Med 2008; 33: 435-41.
Bigeleisen PE. Nerve puncture and apparent intraneural injection during ultrasound-guided axillary block does not invariably result in neurologic injury. Anesthesiology 2006; 105: 779-83.
Neal JM, Bernards CM, Hadzic A, et al. ASRA practice advisory on neurologic complications in regional anesthesia and pain medicine. Reg Anesth Pain Med 2008; 33: 404-15.
Tsai TP, Vuckovic I, Dilberovic F, et al. Intensity of the stimulating current may not be a reliable indicator of intraneural needle placement. Reg Anesth and Pain Med 2008; 33: 207-10.
Choyce A, Chan VW, Middleton WJ, Knight PR, Peng P, McCartney CJ. What is the relationship between paresthesia and nerve stimulation for axillary brachial plexus block? Reg Anesth Pain Med 2001; 26: 100-4.
Urmey WF, Stanton J. Inability to consistently elicit a motor response following sensory paresthesia during interscalene block administration. Anesthesiology 2002; 96: 552-4.
Cohen JM, Gray AT. Functional deficits after intraneural injection during interscalene block. Reg Anesth Pain Med 2010; 35: 397-9.
Reiss W, Kurapati S, Shariat A, Hadzic A. Nerve injury complicating ultrasound/electrostimulation-guided supraclavicular brachial plexus block. Reg Anesth Pain Med 2010; 35: 400-1.
Tsui BC, Pillay JJ, Chu KT, Dillane D. Electrical impedance to distinguish intraneural from extraneural needle placement in porcine nerves during direct exposure and ultrasound guidance. Anesthesiology 2008; 109: 479-83.
Pethig R. Dielectric properties of body tissues. Clin Phys Physiol Meas 1987; 8(Suppl A): 5-12.
Cory PC. Increased impedance on nerve stimulator display may actually reflect a decrease in total system impedance. Anesthesiology 2009; 110: 1192-4.
Thomas SP, Arandia HY, Leal JJ, Chilcoat R. Tissue electrical impedance as an aid to identification of the epidural space. Reg Anesth Pain Med 1987; 12: 169-71.
Chin J, Tsui BC. No change in impedance upon intravascular injection of D5W. Can J Anesth 2010; 57: 559-64.
Sites BD, Spence BC, Gallagher JD, Wiley CW, Bertrand ML, Blike GT. Characterizing novice behavior associated with learning ultrasound-guided peripheral regional anesthesia. Reg Anesth Pain Med 2007; 32: 107-15.
Byrne K, Tsui BC. Practical concepts in nerve stimulation: impedance and other recent advances. Int Anaesthesiol Clin 2011; 49: 81-90.
Dillane D, Tsui BC. From basic concepts to emerging technologies in regional anesthesia. Curr Opin Anaesthesiol 2010; 23: 643-9.
Sauter AR, Dodgson MS, Kalvoy H, Grimnes S, Stubhaug A, Klaastad O. Current threshold for nerve stimulation depends on electrical impedance of the tissue: a study of ultrasound-guided electrical nerve stimulation of the median nerve. Anesth Analg 2009; 108: 1338-43.
Gielen FL, Wallinga-de Jonge W, Boon KL. Electrical conductivity of skeletal muscle tissue: experimental results from different muscles in vivo. Med Biol Eng Comput 1984; 22: 569-77.
Tsai JZ, Will JA, Hubbard-Van Stelle S, et al. Error analysis of tissue resistivity measurement. IEEE Trans Biomed Eng 2002; 49: 484-94.
Bigeleisen PE, Moayeri N, Groen GJ. Extraneural versus intraneural stimulation thresholds during ultrasound-guided supraclavicular block. Anesthesiology 2009; 110: 1235-43.
Competing interests
None declared.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author contributions
Patrick Bardou, Jean-Christophe Merle, Jean-Baptiste Woillard, Nathalie Nathan-Denizot, and Pierre Beaulieu contributed to the study design. Patrick Bardou and Jean-Christophe Merle participated in conducting the study. Patrick Bardou and Jean-Baptiste Woillard contributed to the data analysis. Patrick Bardou, Nathalie Nathan-Denizot, and Pierre Beaulieu were involved in manuscript preparation.
Rights and permissions
About this article
Cite this article
Bardou, P., Merle, JC., Woillard, JB. et al. Electrical impedance to detect accidental nerve puncture during ultrasound-guided peripheral nerve blocks. Can J Anesth/J Can Anesth 60, 253–258 (2013). https://doi.org/10.1007/s12630-012-9845-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-012-9845-y