
Abstract
The introduction of ultrasound guidance has been a marked advance in the practice of regional anaesthesia, and has gained popularity as an adjunct or alternative to nerve stimulation technique. Ultrasound-guided nerve blocks consist of the identification of the target nerve, visualization of the surrounding anatomy (such as blood vessels, lymph nodes, and other important structures), needle tip, and real-time observation of the local anesthetic spread. Peripheral nerves can be identified and traced to alternative sites where local anaesthetic can be safely injected without the risk of neurovascular injury. Direct visualization of the target nerve and deposition of local anesthetic has been shown to improve block operating efficiency while decreasing placement complications and patient discomfort.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Ultrasound
- Peripheral nerves
- Musculoskeletal system
- Peripheral nerve block
- Regional anahestesia
- Nerve stimulation
- Anahestetic drugs
5.1 General Considerations
The principles underlying ultrasound (US)-guided regional anesthesia practice do not differ significantly from established practice.
The addition of US imaging poses few additional problems when organizing one’s practice and when approaching specific patients.
5.1.1 Ergonomics
When setting up a US-guided nerve block, care should be taken to ensure that the machine’s screen can be viewed without e xerting too much stress on the operator, who is normally facing the patient. Ideally, the machine’s controls should be within their reach too, as image setup is best carried during preprocedural scans, using the same approach as will be used for the block.
5.1.2 Sterility
Whether full sterile barrier precautions are needed for single-shot and/or regional catheter placement has been the object of debate and a full analysis is beyond the scope of this chapter. However, adequate precautions to prevent contamination of the equipment should always be employed.
Several approaches have been proposed to protect US transducers. Historically, these have included the creative use of sterile surgical gloves and sterile dressing. As the use of US guidance becomes standard practice in more and more institutions throughout the world, the choice not to use proper sterile sheaths and sonographic gel s eems all the more untenable.
Care should be taken to avoid (cross-)contamination of patients even before the field is prepped. Precautions should be taken when performing both diagnostic and preprocedural scans. In these cases, wound dressings can be more prac tical to use; tissue wipes soaked with specific, noncorrosive disinfectant are also available. Alcohols may gradually wear down the conducive surface of US transducers. Disinfection should include all external surfaces of the US machine; as keyboards are notoriously difficult to sanitize, it has been proposed that touchscreen interfaces may be more easily decontaminated.
5.2 Indications and Contraindications
The choice whether to implement regional anesthesia and specifically peripheral nerve blocks (PNB) into a patient’s clinical pathway will only seldom be based strictly on evidence. In fact, there are but few settings where it has been indisputably demonstrated that PNBs improve outcomes—an d, even then, the choice of the outcome variables may vary greatly depending on the setting.
Evidence-based medicine, however, is mostly based on results obtained on selected populations, by investigators employing predetermined techniques and sharing a common goal. While rigorous methodology guarantees internal validity, generalization of results depends on inclusion criteria and should always be interpreted at the population level. In other words, while evidence-based medicine is useful in guiding population-level decision -making in healthcare policy (e.g., whether to offer femoral nerve blocks to all patients undergoing total knee replacement at one’s hospital), it is not necessarily the preferred approach when discussing options with an individual patient.
Furthermore, other steps in an institution’s clinical pathway may limit the applicability of available evidence in the given context. For example, differences in mobilization policies and physical therapy availability between a randomized con trolled trial and a given institution may negate the advantages of femoral nerve blocks in terms of joint range of motion at 3 months; or again, variations in patterns of perioperative opioid use may affect the prevalence of chronic pain after surgery. To summarize, general indications to PNBs s hould always begin at the evidence base and then be adapted in the context of the individual patient.
The main purposes of a PNB may be summari zed in two items: analgesia, both intraoperative and postoperative, and anesthesia. The former term refers to the utilization of the technique as the sole anesthetic technique, as opposed to the combination of general anesthesia or central blocks as complements. While it is empirically known that many kinds of surgery may be carried out with PNBs a s the main anesthetic in the context of monitored anesthesia care (MAC) , little evidence is available to demonstrate the possible outcome differences when compared to general anesthesia or central blocks, either alone or in combinations with PNBs.
In some countries, anesthetic management may be influenced by reimbursement practices, encouraging the addition of general anesthesia or central blocks to P NBs. When this is not an issue, the need for an additional anesthetic technique should be evaluated on the basis of block effectiveness, surgical technique, patient preference, and practical considerations. However, the need for MAC (i.e., the continued presence of dedicated personnel trained in anesthesia) should never be questioned but for the simplest surgical procedures performed with distal nerve blocks.
In the setting of chronic pain medicine, PNBs can be considered to have two primary indications: pain relief in the short-to-medium term and differential diagnosis. In specific settings, results obtained after a PNB may influence subsequent management, although this is usually practical evidence. For example, significant pain relief after a suprascapular nerve block for rotator cuff syndrome may suggest that a patient will benefit from pulsed radiofrequency treatment of the nerve; absence of pain relief despite a successful blo ck (as evidenced by skin sensory testing) may, conversely, advise against such procedure. In the latter case, the pain generator could be assumed to be innervated by a different nerve. However, it is unclear whether diagnostic blocks are predictive of outcome after radiofrequency treatment in cases where the pain generator is clearly identified (e.g., intercostal nerves, knee, hip, etc.), as one should always consider the possibility of technical failure of the diagnostic block.
A search of the literature will reveal a grow ing number of case reports for niche indications fo r PNBs, including:
-
Acute limb ischemia/vasospasm
-
Limb replantation/salvage procedures
-
Chronic regional pain syndromes
The underlying theory, demonstrated in part in animal models, is that blockade of sympathetic efferents will favorably affect these c onditions.
5.3 Setting and Patient Preparation
The ideal environment for the execution of a nerve block is a preparation room, where the anesthetist can have the material and the time required for the execution of the block and where the patient can be monitored and treated in case of adverse events. However, the execution of a nerve block does not require a specific setting , as it can be performed even directly in the operating room.
Beyond the specific setting, the patient should be positioned in the most favorable posture for the execution of the block itself, as described in each chapter.
The anesthetist should ensure the patient’s monitoring (electrocardiographic trace and peripheral O2 saturation are usually enough), prepare a s terile field, and proceed with the ultrasound scan and with the nerve block.
In some cases, it may be appropriate to consider the need for a mild sedation or analgesia before the execution of the block, in order to make th e procedure easier and better tolerated by the patient.
5.4 Drug and Material Requirements
The only required materials are an ultrasound machine with a linear and a convex transducer (depending on the block, as described in each chapter), ultrasound gel, a needle whose length depends on the target depth, syringes, sterile gloves, disinfectant, and local anesthetic.
One of the most important choice in the execution of a nerve block is obviously of the local anesthetic and its concentration. This choice depends on the desired effect in terms of the type of block (anesthetic or analgesic) and in ter ms of duration of the block itself.
An in-depth dissertation on local anesthetics is not the goal of this manual; therefore we report a simple summary in Tab le 5.1.
5.5 US Guidance and Navigation Systems
The introduction of ultrasound guidance has been a marked advance in the practice of regional anesthesia and has gained popularity as an adjunct or alternative to the nerve stimulation technique . Ultrasound-guided nerve blocks consist of the identification of the target nerve, visualization of the surrounding anatomy (such as blood vessels, lymph nodes, and other important structures), needle tip, and real-time observation of the local anesthetic spread. Peripheral nerves can be identified and traced to alternative sites where local anesthetic can be safely injected without the risk of neurovascular injury. Direct visualization of the target nerve and deposition of local anesthetic have been shown to improve block operating efficiency while decreasing placement complications and patient discomfort. Variations in limb anatomy are commonly identified by ultr asonography and may, in part, explain the documented high incidence of block failure using traditional methods. Regional anesthesia performed with bedside ultrasound guidance compared to peripheral nerve stimulation has been shown to have a significant decrease in the risk of vascular puncture, an increase in the nerve block duration, and a faster onset time. Ultrasound has already transformed the practice of peripheral nerve and plexus blockade, and its wider availability is likely to ensure even greater use in the future.
For evaluation of the superficial nerves, su ch as those in the forearm, the brachial plexus, and femoral nerves, a high-frequency (10–15 MHz) linear transducer is required which provides better resolution. A lower-frequency convex probe (4–7 MHz), which provides better penetration, is recommended for deeper targets such as the sciatic nerve or for more obese patients. The availability of color flow Doppler is useful for differentiating vascular structures. N eedle visualization during US-guided regional anesthesia is likely essential for safety and efficacy.
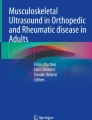
However, accurate and consistent needle tip visualization is hampered by several factors, including the difficulty of needle-beam alignment, and the poor echogenicity of commonly available block needles in the clinical setting. There are two methods of orienting the needle relative to the US beam in US-guided peripheral nerve block: the in-plane and out-of-plane approaches. In the out-of-plane needle approach , the longitudinal axis of the needle is inserted in a plane perpendicular to that of the US beam, and the needle tip crosses the plane of imaging as an echogenic dot (Fig. 5.1a, b).

(a) The needle is inserted using an out-of-plane approach. (b) It is relatively easy to confuse the shaft that appears as an echogenic dot (indicated by yellow arrow)
This approach has a shorter needle trajectory and mirrors the landmark-based technique, but with the additional benefits of ultrasound guidance. However, the block needle, usually 22 gauge and 5 cm in length, is viewed in cross section only, and the precise location of the needle tip can be uncertain. If the needle tip crosses the scan plane without recognition, it may be advanced into undesired structures. In general, the out-of-plane approach provides less-consistent needle visualization when compared to the in-plane approach and is typically used for superficial injections with minimal surrounding soft tissues. Using the in-plane approach the entire length of the needle is held within the plane of the ultrasound beam and is visible as a bright hyperechoic line (Fig. 5.2a, b). The needle can be viewed continuously throughout the procedure and the tip accurately placed while avoiding vital structures. The angle at which the needle shaft and US beam intersect (needle-beam angle) greatly affects needle visibility. Needle tip and shaft v isibility are better at larger needle-beam angles when using an in-plane needle approach; the optimal angle appears to be >55°, and a needle-beam angle close to 90° offers the best needle visibility (Fig. 5.3a, b).

(a) The needle is inserted using an in-plane approach (the needle-beam angle is almost 90°) in a shallow trajectory. (b) Both the shaft and tip (yellow arrows) are clearly visible, with maximal reflection back to the transducer

(a) The needle is inserted in a steep trajectory (small needle-beam angle). (b) The needle shaft and tip (yellow arrows) become less echogenic and are poorly visible
However, difficulties in aligning the needle and the transducer can lead to incorrect identification of the needle tip, possibly damaging structures not visible on the ultrasound screen. Additional techniques specifically developed to aid alignment of needle and probe or identification of the needle tip are now available, such as needle guides; three- and four-dimensional ultrasound; magnetism, electromagnetic, or GPS systems; optical tracking; augmented (virtual) reality; robotic assistance; and automated (computerized) needle detection.
For the fusion imaging technique, a variety of tracking methods are available, including optical, image-based, and electromagnetic tracking. Electromagnetic tracking is most widely used for US-guided interventions. There are three components of the electromagnetic tracking-based fusion imaging technique: the magnetic field generator, position sensor, and position sensor unit. The first step of image fusion is uploading the data set to be fused with real-time US to the US machine. This technique involves the co-registered display of real-time ultrasound with a reference series from another modality, such as CT or MRI. As the ultrasound exam is performed, the fusion system continuously generates reformatted planes from the reference series matching the oblique imaging planes of the ultrasound transducer.
Virtual needle tracking (navigation system) can be provided by the fusion imaging system with the use of the electromagnetic position sensor embedded in the distal tip of a needle or attached to the hilt of the needle. A needle with a position sensor at the distal tip of the needle can provide a more accurate expected electrode path than that with a position sensor attached to the hilt of the needle. US needle guidance with CT fusion assistance allows for safe and effective injection of degenerative facet joint disease in patients suffering from back pain (Fig. 5.4). This technique may be readily translated also to other a pplications in which spinal needles are used.

CT fusion-assisted US- guided injection of facet joints in patients suffering from back pain. The needle is inserted using a “navigation system” with virtual needle tracking, provided by an electromagnetic position sensor embedded in the needle tip
5.6 Interscalene Block
The brachial plexus (Fig. 5.5) that provides sensory and motor innervation to the upper limb can be blocked at four levels: at trunks level (interscalene block), at divisions level (supraclavicular block), at cords level (infraclavicular block), and at terminal branches level (axillary block).

Brachia l ple xus anatomy and blocks’ sites
Anatomy (Fig. 5.6): At this level the trunks, surrounded by a connective sheath, are located in the interscalene groove (defined by the anterior and middle scalene muscles) deep to the sternocleidomastoid muscle.

The in tersc alene groove in a trans-sectional view of the neck. TS superior trunk, TM middle trunk, TI inferior trunk, CA carotid artery, IJV internal jugular vein
Indications : Anesthesia or analgesia for shoulder surgery as this approach targets the proximal roots of the plexus (C4–C7). The more distal roots of the plexus (C8–T1) are usually spared by this approach.
Patient position : The patient is positioned supine or with the head elevated 45° with a pillow under the shoulder. The head is turned 45° to the contralateral side.
What you need: A high-frequency (10–15 MHz) linear probe and a 22G atraumatic echogenic needle, 50 mm of length. 15 mL of local anesthetic.
Sonoanatomy (Fig. 5.7): When the probe is in the right position, you can see the interscalene groove that is located under the sternocleidomastoid muscle, lateral to the carotid artery and internal jugular vein. Between the anterior and the middle scalene muscles, you can see the three trunks of the brachial plexus: they appear hypoechoic, with a round or oval cross section and with a hyperechoic labrum, aligned one above the other like a “traffic light.”

(a) Patient po sition and needle entry point. The yellow arrow shows the trajectory of “traceback method” scanning. (b) Sonoanatomy. SCM sternocleidomastoid muscle, AS anterior scalene muscle, MS middle scalene muscle, Long white arrow needle direction and target point
How to do it (Fig. 5.7): We suggest the “traceback method .” The probe is initially positioned above the clavicle to search the subclavian artery and the secondary trunk of the plexus lateral and above the artery. Afterward, the probe is withdrawn along the sternocleidomastoid muscle: the secondary trunks become primary trunks, and a transverse image of the plexus roots in the interscalene area is obtained on the lateral aspect of the neck in an axial oblique plane.
The needle is inserted in-plane with the skin entry point 1–2 cm away from the probe. The tip of the needle must be between the superior and the middle trunks of the plexus. The anesthetic spread will be inside the connective sheath surrounding the brachial plexus in order to provide an adequate anesthesia/analgesia with the lowest volume of anesthetic.
Tips and tricks: Be aware of anatomical variants of the brachial plexus . One of the most common, concerns the root of C5 that gives rise to the superior trunk. The C5 ventral ramus can pass through or upon the anterior scalene muscle, and this can be a cause of failure of the blind interscalene approach of the brachial plexus.
Before the injection of the anesthetic solution, use the power Doppler to detect vessels near the tip of the needle.
Complications : One of the most common side effects of interscalene block is hemidiaphragmatic paresis secondary to phrenic nerve palsy. Using low volume of anesthetic can mitigate it.
Unintentional epidural or spinal anesthesia and spinal cord injury are very rare complications of interscalene block.
5.7 Supraclavicular Block
Anatomy (Fig. 5.8): In the supraclavicular area , the brachial plexus (the trunks and/or their respective anterior and posterior divisions) is located lateral and posterior to the subclavian artery. They both lie over the first rib and under the clavicle.

Topogra ph y of brachial plexus in the supraclavicular area. CL clavicle, FR first rib, BP brachial plexus trunk’s divisions, SA subclavian artery. The blue box shows the echographic supraclavicular window
Indications : Surgeries of the arm, forearm, or hand.
Patient position : Supine position with a pillow under the shoulder. The head is turned 45° to the contralateral side.
What you need: A high-frequency (10–15 MHz) line ar probe and a 22G atraumatic echogenic needle, 50 mm of length. 15 mL of local anesthetic.
Sonoanatomy (Fig. 5.9): In the supraclavicular area, the plexus appears most commonly as a group of several hypoechoic structures with a round or oval cross section and with a hyperechoic labrum that has been compared to a “bunch of grapes” lateral to a round pulsatile uncompressible structure that is the subclavian artery. Under the plexus you can see a hyperechoic structure with the acoustic shadowing below the f irst rib. Over the plexus you can see a light hyperechoic line that is the superficial cervical fascia.

(a) Patien t p osition and needle entry point. Probe tilting (yellow arrows). (b) Sonoanatomy. 1st R first rib, A subclavian artery. Corner pocket (yellow dashed lines). Long white arrow needle direction and target point
How to do it (Fig. 5.9): We suggest scanning over the supraclavicular fossa in a coronal oblique plane. From medial to lateral you can find the trachea, the carotid artery, the jugular vein, and finally the subclavian artery with the plexus. Tilt the probe to check the right window.
In order to facilitate the entry of the needle, just before inserting it, move the lateral part of the probe away from the clavicle. In this way the humeral head will not be an obstacle for the physician.
The needle is inserted in-plane with the skin e ntry point 1–2 cm away from the probe.
The “corner pocket ,” the angle between the subclavian artery and the first rib, is traditionally the site of local anesthetic injection, but it has been demonstrated that a multiple injection between the plexus nerves, a so-called “targeted intra-cluster injection,” can allow a rapid onset of the block.
Tips and tricks: Be aware of intra-grape vessel of the brachial plexus, and use the power Doppler before the injection (Fig. 5.10).

Power Doppler showing an intra-grape vessel
During the injection of local anesthetic in the pocket corner, look at the movement of the subclavian artery away from the first rib to be sure to anesthetize the divisions that will generate the radial nerve.
Complications : The risk of pneumothorax is greatly reduced with the use of ultrasound-guided block. Other rare complications can be hemidiaphragmatic paresis (1%), Horner syndrome (1%), and vascular puncture (0.4%).
5.8 Infraclavicular Block
Anatomy (Fig. 5.11): In the infraclavicular area , the cords of the brachial plexus are located posterior to major and minor pectoralis muscles, around the second part of the axillary artery. The lateral cord of the plexus lies superior and lateral, the posterior cord lies posterior, and the medial cord lies posterior and medial to the axillary artery.

Anatomy of infraclavear cords of brachial plexus (arrowed). LC lateral cord, PC posterior cord, MC medial cord, CL clavicle, FR first rib, BP brachial plexus trunk’s divisions, SA subclavian artery. The blue box shows the echographic infraclavicular window
Indications: Surgeries of the a rm, forearm, or hand. This approach is the preferred one for catheter positioning thanks to better stability of the catheter.
Patient position: the patient is positioned supine with the arm on the side abducted 90°. In this way the artery becomes more superficial and more distant from the pleura, wh ile the three cords become all lateral and posterior to the artery (Fig. 5.12).

The abductio n of the arm shifts the three cords of the brachial plexus lateral and posterior to the artery MC medial cord, LC lateral cord, PC posterior cord
What you need: A high-frequency (6–13 MHz) linear probe. A 22G atraumatic echogenic needle, 80 mm of length. Local anesthetic: 30 mL.
Sonoanatomy (Fig. 5.13): In t he upper part of the screen, we can see the pectoralis muscles with their fasciae (hyperechoic lines), two vascular structures, the axillary vein (oval shape, bigger, squeezable), and the axillary artery (smaller, rou nd shape, pulsing, and incompressible). More deeply you can see the pleura and the three cords as hyperechoic structures like a “honeycomb” (Fig. 3).

(a) Patient posit ion and needle entry point, with abducted arm. (b) Sonoanatomy. MaP major pectoralis muscle, MiP minor pectoralis muscle, A axillary artery, V axillary vein, MC medial cord (yellow outlined), LC lateral cord (yellow outlined), PC posterior cord (yellow outlined), Long white arrow needle direction and target point
How to do it (Fig. 5.13): Put the pro be on the deltoid pectoral sulcus with a transverse view scanning in a parasagittal plane.
The needle is inserted in-plane with the ultrasound beam in a cephalo-to-caudad orientation and with a lateral direction to avoid the pneumothorax.
The tip of the needle must be posterior to the artery: we suggest to inject here 20 mL of local anesthetic and 10 mL during the draw ing back of the needle before crossing to deeper fascia of the pectoralis muscle.
Sometimes the cords are not v ery visible; in this case you can use ENS guide together with ultrasound guide to find the posterior cord. The anesthetic injection will produce an anechoic bubble like the artery one with the so-called “double bubble sign.”
Be aware of the possibility to find two axillary arteries or a lot of thoracic veins: in this case it is better to avoid this approach in order to avoid intravascular injection or vascular complications.
Complications: Pneumothorax remains t he most feared complication of this block. Vascular injection is also possible but rare.
5.9 Axillary Block
Anatomy (Fig. 5.14): The axillary approach to the brachial plexus targets three terminal branches of the plexus: the median, the ulnar, and the radial nerve. The musculocutaneous nerve often departs from the lateral cord in the proximal axilla and is commonly spared by the axillary approach (Fig. 1).

Anatomic slice of axillary area. Bsh biceps short-head muscle, Blh biceps long-head muscle, CBr coracobrachialis muscle, H humerus, Tm teres major muscle, Tr triceps muscle, A axillary artery, V axillary vein, MC musculocutaneous nerve, M median nerve, U ulnar nerve, R radial nerve
Indication : Axillary brachial plexus block is usually indicated for distal upper limb surgery (hand and wrist).
Patient position : The patient is positioned supine with the arm on the side abducted 90° and the elbow flexed or extended.
What you need: A high-freque ncy (6–13 MHz) linear probe. A 22G atraumatic echogenic needle, 50 mm of length. Local anesthetic: 20, 5 mL for nerve.
Sonoanatomy (Fig. 5.15): With the probe in the right position, you can see in the deeper area of the screen the humerus (a curved hyperechoic image with acoustic shadowing below it) and three muscles, the triceps (posterior), the biceps, and the coracobrachialis (anterior), that create a triangular area in which you can find th e axillary artery and the three nerves. The median nerve is commonly anteromedial to the artery, the ulnar nerve medial to the artery, and the radial nerve posteromedial to it.

(a) Patient position a nd needle entry point. (b) Ultrasound view of axillary area. A axillary artery, MC musculocutaneous nerve, M median nerve, U ulnar nerve, R radial nerve, B biceps muscle, CB coracobrachialis muscle, TeM teres major muscle, T triceps muscle, H humerus
The musculocutaneous nerve can be found in the coracobrachialis muscle or between it and the triceps muscle.
Nerves in the axilla have mixed echogenicity and a “honeycomb” appearance (representing a mixture of hypoechoic nerve fascicles and hyperechoic non neural fibers).
How to do it (Fig. 5.15): The transducer is placed along the axillary crease, perpendicular to the long axis of the arm. The needle is inserted in-plane 1 cm away from the probe.
We suggest to scan the axilla beginning from lateral to medial in order to find the best site for the block: one in which you can b lock the four nerves with a unique skin entry point.
The first nerve to be blocked is the musculocutaneous nerve; afterward, draw back the tip of the needle and go to the front of the axillary artery. When a loss of resistance is felt, you can switch on the ENS to be sure to be close to the median nerve. Afterward, draw back the tip of the needle and go under the artery; at this point the ENS will elicit the ulnar nerve. Finally put the tip of the needle at the back of the artery and find the radial nerve with the ENS. This technique is called “perineural technique ” (Fig.5.16a–c).

(a–c) The yellow arrows indicate the needle around the axillary artery (A) near to the terminal branches of the brachial plexus
Tips and tricks: The classical disposition of nerves around the axillary artery can be found in 65% of people. However you can obtain an axillary block using the so-called “perivascular technique ” putting the local anesthetic just around the artery without localizing the nerves, except for the musculocutaneous nerve.
Watch out to see the “black cloud” when you inject the local anesthetic in order to avoid intravascular injection.
Complications : The most common complica tion is axillary artery puncture or intravascular injection. Nerve injury is also possible.
5.10 Median Nerve Block
Anatomy (Fig. 5.17): Median nerve can be located just proximal to the elbow crease, medial to the brachial artery, or at the forearm among the tendons of flexor muscles.

Terminal branches of the brachial plexus in the upper limb. A axillary nerve, MC musculocutaneous nerve, M median nerve, U ulnar nerve, R radial nerve
Patient position: The patient is positioned supine with the arm on the side abducted 90° with the elbow extended.
What you need: A high-fre quency (6–13 MHz) line ar probe. A 22G atraumatic echogenic needle, 50 mm of length. 5 mL of local anesthetic solution is generally sufficient to block any of the terminal nerves individually.
Sonoanatomy (Figs. 5.18 and 5.19): You have to look for the typical “honeycomb” aspect. In distal arm, the medial nerve can be found superficially, medial to the brachial artery. Just below the median nerve, you can see the brachialis muscle and deeper the humerus.

(a) Patient position and needle entry point. (b) Sonoanatomy of median nerve in distal arm. M medial nerve close to brachial artery, B biceps muscle, T triceps muscle, Br brachialis muscle, H humerus, Long white arrow needle direction and target point

(a) Patient posit ion and needle entry point. (b) Sonoanatomy of median nerve in the forearm. M median nerve, FCR flexor carpi radialis muscle, FPL flexor pollicis longus muscle, FPD flexor profundus digitorum muscle, FSD flexor superficialis digitorum muscle, R radius, U ulna, Long white arrow needle direction and target point
In the forearm the median nerve can be found among the flexor muscles.
How to do it (Figs. 5.18 and 5.19): The transducer is placed perpendicular to the long axis of the arm. The needle is inserted in-plane.
Tips and tricks: As the nerve is always lateral to the artery, put yourself by the side of the nerve to block, in order to facilitate it and avoid arterial puncture.
Be careful to paresthesia and/or high pressure of injection that are warning signs of intraneural injection.
Complications: Arterial p u ncture and intraneural injection.
5.11 Ulnar Nerve Block
Anatomy (Fig. 5.20): The ulnar nerve is superficially located in the arm. It may be safely blocked proximal to the ulnar groove or at the forearm.

Anatomic schema of ulnar nerve at the elbow. U ulnar nerve
Patient position: The patient is position ed supine with the arm on the side abducted 90° with the elbow extended.
What you need: A high-frequency (6–13 MHz) li near probe. A 22G atraumatic echogenic needle, 50 mm of length. 5 mL of local anesthetic.
Sonoanatomy (Figs. 5.21 and 5.22): In the arm you can see the ulnar nerve superficially, above the brachialis and the triceps muscles. In the forearm, the ulnar nerve is close to the ulnar artery.

(a) Patient position and needle entry point. (b) Sonoanatomy of ulnar nerve in cubital tunnel. U ulnar nerve (outlined), ME medial epicondyle, CT cubital tunnel, Long white arrow needle direction and target point

(a) Patient position and needle entry point. (b) Sonoanatomy of ulnar nerve in distal arm. U ulnar nerve close to the ulnar artery, FSD flexor superficialis digitorum muscle, FPD flexor profundus digitorum muscle, Long white arrow needle direction and target point
How to do it (Figs. 5.21 and 5.22): The tr ansducer is placed perpendicular to the long axis of the arm to see the nerve in short axis. The needle is inserted in-plane.
For the forearm block, begin the scanni ng at the wrist and after go cephalic. The right site for the block is where the nerve runs from the artery.
Tips and tricks: As the ulnar nerve is close to the ulnar artery, use the power Doppler to detect it. Avoid to block at the wrist as the ri sk of arterial puncture or hematoma is higher. Both blockade of the ulnar nerve at the elbow (ulnar groove) is traditionally discouraged as the nerve is cir cumscribed by rigid structures (bones and ligaments) and there is the potential for entrapment.
5.12 Radial Nerve Block
Anatomy (Fig. 5.23): The radial nerve can be located in the lateral aspect of the distal part of the arm, deep to the brachialis and brachioradialis muscles and superficial to the humerus. In the forearm, the radial nerve runs laterally to the radial artery.

Anatom ic slice of distal arm. Bic biceps muscle, Br brachialis muscle, H humerus, Tr triceps muscle, R with black arrow radial nerve
Patient position: For the prox imal bl ock, the arm is adducted and the elbow is flexed 90°.
For the block at the forearm, the patient is positioned supine with the arm on the side abducted 90° with the elbow.
What you need: A high-freque ncy (6–13 MHz) linear probe. A 22G atraumatic echo genic needle, 50 mm of length. 5 mL of local anesthetic.
Sonoanatomy (Figs. 5.24 and 5.25): In the arm the radial nerve with his honeycomb aspect is between the brachialis and brachioradialis muscles. In the forearm, the radial nerve is next to the radial artery.

(a) Patient position and needle entry point. (b) Sonoanatomy of radial nerve in distal arm. R radial nerve, B brachialis muscle, T triceps muscle, H humerus, long white arrow needle direction and target point

(a) Patient position and needle entry point. (b) Sonoanatomy of radial nerve at forearm. R ulnar nerve close to the radial artery, BR brachioradialis muscle, PT pronator teres muscle, FPL flexor pollicis longus muscle, long white arrow needle direction and target point
How to do it: The transducer is pl aced perpendicular to the long axis of the arm to see the nerve in short axis. The needle is inserted in-pla ne.
For the forearm block begin the scanning at the wrist and after go cephalic. The right site for the block is where the nerve runs from the artery.
Tips and tricks: As the nerve is always lateral to the artery, put yourself by the side of the nerve to block, in order to facilitate it and avoid arterial puncture.
Be careful to the warning signs of intraneural injection: paresthesia and/or high pressure of injection.
Complications: Arterial puncture and intraneural injection.
5.13 Thoracic Paravertebral Block
Anatomy (Figs. 5.26 and 5.27 ): The paravertebral space (PVS) is a wedge-shaped area positioned between the heads and necks of the ribs. The anterolateral boundary is formed by the parietal pleura. The medial boundary is formed by the posterolateral aspect of the vertebral body, the intervertebral discs, the intervertebral foramen, the spinal nerves, and connective tissue. The posterior boundary is formed by the superior costotransverse ligament which extends from the inferior aspect of each transverse process to the superior aspect of the rib below. The superior costotransverse ligament is continuous laterally with the internal intercostal membrane, which is the aponeurosis of the internal intercostal muscle and attaches medially to the upper and lower borders of the ribs.

Para vertebr al space between the extrapleural (a) and the subendothoracic (b) spaces. 1 visceral pleura, 2 interpleural space, 3 parietal pleura, 4 endothoracic fascia. SG sympathetic ganglion, A aorta

Sche matic rep resentation of the ultrasound view of the paravertebral space in a paramedian longitudinal plane. 1 superior costotransverse ligament, 2 paravertebral space, 3 pleura
Indications : Analgesia for unilateral surgical procedures or painful conditions of the thorax and abdomen.
Patient position : Sitting position w ith neck and back flexed or prone position with a pillow under the thorax.
What you need: A high-frequency (10–15 MHz) linear probe and a 22G atraumatic echogenic needle, 50 mm of length. 10–20 mL of local anesthetic.
Sonoanatomy (Figs. 5.28 and 5.29 ): The transverse processes and ribs are visualized as hyperechoic structures with acoustic shadowing below them. The PVS appears as a wedge-shaped hypoechoic layer demarcated by the hyperechoic reflections of the pleura below and the internal intercostal membrane above.

(a) Patie nt po sition and needle entry point for paramedian sagittal approach. (b) Sonoanatomy. TP transverse process, IC intercostal muscles, P pleura, Yellow asterisk paravertebral space, White dot needle position in target point

(a) Pati ent po sition and needle entry point for transverse approach. (b) Sonoanatomy. TP transverse process, P pleura, Yellow asterisk paravertebral space, Long white arrow needle direction and target point
How to do it: There are two different a pproaches to the paravertebral space: the paramedian sagittal approach and the transverse one.
Paramedian sagittal approach (Fig. 5.28 ): The p robe is placed in a longitudinal paramedian plane between two transverse processes, 5–6 cm lateral to the midline. Both transverse processes should be visualized, with the superior costotransverse ligament and the pleura visible in between. The needle is inserted in-plane under direct visualization until it pierces the superior costotransverse ligament. When the needle tip is located immediately above the pleura, you can inject the local anesthetic. Look at the downward displacement of the pleura, indicating proper spread of the local anesthetic. The extent of local anesthetic spread should be evaluated by moving the ultrasound probe superiorly and inferiorly.
Transverse approach (Fig. 5.29 ): The probe is placed in a transverse position and is moved superiorly and inferiorly to confirm the correct position. The transverse process is visualized medially with the pleura dipping under the inferolateral aspect. The needle is inserted in-plane until the PVS; inject local anesthetic, resulting in downward displacement of the pleura, indicating proper spread of the local anesthetic.
Tips and tricks: Inject slowly the local anesthetic avoiding forceful high-pressure injection to reduce the risk of bilateral epidural spread.
Complications : Unintentional injec tion in unwanted locations (pleura, neuraxial space) resulting in pneumothorax and spinal anesthesia.
5.14 Transversus Abdominis Plane (TAP) Block
Anatomy (Fig. 5.30 ): the anterior abdominal wall is innervated by the anterior rami of the lower thoracic nerves (T7–T12) and by the first lumbar nerve (L1). The terminal branches of these somatic nerves run in a neurovascular plane between the internal oblique and the transversus abdominis muscles. This plane is c alled transversus abdominis plane (TAP).

(a) Patient position and needle entry point. (b) Sonoanatomy. EO external oblique muscle, IO internal oblique muscle, TA transverse abdominis muscle, IH iliohypogastric nerve, II ilioinguinal nerve, Long white arrow needle direction and target point
Indications : Postoperative analgesia for laparotomy, appendicectomy, abdominoplasty, open-prostatectomy, cesarean section, and laparoscopic surgery; alternative technique to epidural anesthesia/analgesia for surgery on abdomen; chronic abdominal pain.
Patient position : Supine po sition.
What you need: High-frequency (10–15 MHz) linear probe, 50–100-mm and 20–21-gauge needle; two 20-mL syringes of local anesthetic.
Sonoanatomy (Fig. 5.30 ): From the surface into the depth, the abdominal wall between the costal margin and the iliac crest is composed of these different layers: skin, subcutaneous tissue, and three muscle layers separated by hyperechoic fascia (external oblique, internal oblique, transversus abdominis), peritoneum, and abdom inal cavity with bowel.
How to do it (Fig. 5.30 ): With the transducer transverse on the abdomen, at the anterior axillary line between the costal margin and the iliac crest, move slightly caudal or cephalic to identify the three muscle layers.
Once the TAP is identified, insert the needle with the in-plane approach from medial to lateral. A “pop” may be felt when the needle tip enters the plane between two muscles. When the TAP is reached, after gentle aspiration, inject a small amount of LA to verify the position of the tip. Not infrequently, the LA will spread within, rather then between muscle bellies; when this happens, the needle should be advanced or withdrawn and a test injection performed again. When dissection of the correct plane by injectate is achieved (Fig. 4), 15–20 mL of LA (different concentration, depending on the indication) can then be administered, with frequent aspirations. The goal is to visualize the LA spread between the transversus abdominis and the internal obli que muscle plane.
Tips and tricks: Usually the appropriate depth of the ultrasound field is about 3–4 cm. In obese patients the exact identification of TAP can be challenging. In these cases remember that the internal oblique muscle is always the thickest, while the transversus abdominis the thinnest. During the LA injection, scan the abdomen caudal and cephalic to determine the extent of longitudinal spread. Make sure the transversus muscle and the underlying peritoneum and bowel are clearly identified at the bottom of the image. If prolonged analgesia is needed, consider the insertion of a catheter.
Complications : LA toxicity, intravascular injection, nerve wound, block failure, hepatic puncture, bowel wound, hematoma, and tr ansient paralysis of femoral nerve.
5.15 Rectus Sheath Block
Anatomy (Fig. 5.31 ): Innervation of the anterolateral abdominal wall arises from the anterior rami of spinal nerves from T7 to L1. They are located in the plane between the internal oblique and the transversus abdominis muscles. Tho racic nerves (T7–T11) pierce the posterior wall of the rectus sheath as anterior cutaneous branches, and they provide sensory innervation to the rectus muscle and the overlying skin. In particular, nerves T7–T9 supply the skin superior to the umbilicus, T10 the umbilicus, and T11 the skin inferior to the umbilicus.

Anatomy of rec tus muscle (Rm). 1 Site of local anesthetic injection, 2 fascia transversalis, 3 linea alba
Indication: Postoperative analgesia for umbilical hernia repair and other umbilical surgery, analgesia for the middle anterior wall from xiphoid process to the symphysis pubis.
Patient position: Supine position.
What you need: High-frequen cy (10–15 MHz) linear probe, 50–100-mm 22-gauge needle; local anesthetic 15–30 mL.
Sonoanatomy (Fig. 5.32 ): The rectus abdominis muscle is an oval-shaped structure under the superficial fascia of the abdo men. The m uscle is surrounded by an aponeurotic sheath which splits into two layers, which merge near the midline and conjoin with the contralateral fascia to form the linea alba. Color Doppler imaging may reveal small epigastric arteries deep in the muscle belly. More deeply, one can see pre-peritoneal fat, the peritoneum, and bowel.

(a) Patient posit ion and needle entry point. (b) Sonoanatomy. R: rectus muscle, Long white arrow needle direction and target point
How to do it (Fig. 5.32 ): Put the transducer transverse on abdomen lateral to the umbilicus; insert the needle with an in-plane approach with lateral to medial direction. Advance the needle until the posterior rectus sheath. Inject f irst a small amount of LA to confirm the right position of the tip. Then inject the total dose of AL (about 10–20 mL per side in adults). The goal is to visualize an adequate LA spread between rectus m uscle and posterior rectus sheath.
Tips and tricks: Use color Doppler to avoid the puncture of epigastric arteries.
If prolonged analgesia is neede d, consider the insertion of a catheter.
Complications: Rare. Bleeding, infection, LA systemic toxicity, intravascular injection, rectus sheath hematoma, perit oneal and bowel perforation.
5.16 Lumbar Plexus Block
The lumbar plexus (LP ) consists of a group of six nerves that supply the lower abdomen and lower leg. Combined with a sciatic nerve block, the lumbar plexus block can provide complete analgesia to the lower extremity. The complete lumbar plexus can be blocked from a posterior approach (also known as the psoas compartment block), and with other new ultrasound-guided approaches.
Anatomy (Fig. 5.33 ): The lumbar plex us is formed from the ventral rami of L1–L4 with variable contributions from T12 and L5 (Fig. 1). The peripheral branches of the lumbar plexus include the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, femoral, and obturator nerves. The plexus forms within the body of the psoas muscle.

Simplified schema o f lumbar plexus anatomy (posterior nerves red painted). A iliohypogastric nerve, B ilioinguinal nerve, C genitofemoral nerve, D lateral femoral cutaneous nerve, E and F branches for psoas and iliacus muscles, G femoral nerve, H accessory obturator nerve, I obturator nerve, J lumbosacral trunk
Indications : Anesthesia or analgesia fo r lower limb surgery, enclosed hip surgery, in association with proximal sciatic block.
What you need: A low-frequency (6–8 MHz) convex probe and a 22G atraumatic echogenic needle, 100 mm of length. 20–30 mL of local anesthetic.
Sonoanatomy (Figs. 5.34 and 5.35 ): The transverse processes are closely related to the plexus and therefore are used as the mai n landmark during LPB. A scan for the LPB can be performed in the transverse or longitudinal axis. The ultrasound transducer is positioned 3–4 cm lateral to the lumbar spine for either orientation.

Ultrasound anatom y of the lumbar paravertebral space using transverse oblique view. ES erectors spinae muscle, QL quadratus lumborum muscle, P psoas major muscle, LP lumbar plexus, VB vertebral body, L lamina, SP spinal process

Patient pos ition (a) and sonoanatomy (b) in Karmakar’s approach. The tip of the needle (white dots) is between the “teeth of the trident.” TP transverse process
Using a transverse oblique view, you can see lumbar plexus root just below the lamina and above the vertebral body. Quadratus lumborum muscle and psoas major muscle are lateral to the root.
Using a longitudinal view the acoustic shadow of the transverse processes has a characteristic appearance called the “trident sign .” Lumbar plexus roots look like linear hyperechoic structures between the transverse processes a bove the psoas muscle.
Patient position : The patient is placed in the lateral decubitus position with the operative side up.
How to do it: Lumbar plexus block can b e done using different techniques. We suggest two methods.
Karmakar’s approach (Fig. 5.35 ): Put the transducer longitudinally on the lumbar paravertebral region, and scan gradually from caudal to cephalad in order to find the transverse processes and the “trident sign .” Insert the needle out-of-plane.
The goal of the technique is to guide the needle between the transverse processes (between the “teeth of the trident”) of L3–L4 or L2–L3 into the posterior part of the psoas major muscle containing the roots of the lumbar plexus. Use nerve stimulation to confirm the correct position (ipsilateral quadriceps muscle contractions) before the injection of the anesthetic solution.
Shamrock’s method (Fig. 5.36 ): Another method of ultrasound-guided lumbar plexus block is scanning the patient’s flank, immediately crania l to the iliac crest, in a transverse plane and inserting the needle 4–5 cm later to the midline in-plane and perpendicular to the ultrasound beam. In this way the anatomical structures surrounding the lumbar plexus give a recognizable ultrasonographic pattern like a shamrock with three leaves. Hyperechoic round oval structures representing the nerves of the lumbar plexus are found in the medial and posterior part of the psoas muscle, typically within a distance of two centimeters from the trans verse process. The needle tip can be visualized clearly and positioned precisely beside the target nerves. Nerve stimulation with ipsilateral quadriceps muscle contractions can confirm it.

Patient pos ition (a) and sonoanatomy (b) in Shamrock’s method. P psoas muscle, ES erector spinae muscle, QL quadratus lumborum muscle, TP transverse process, L4 represents the pattern of a shamrock with three leaves. The nerve (arrowed in target point) is found in the medial and posterior part of the psoas muscle. Long white arrow needle direction and target point
Tips and Tricks: Dual guidance with neurostimulator is recommended because at such deep location nerve roots can be indistin guishable from tendons or muscle septa, in a longitudinal view.
Local anesthetic must be administered in fractionated doses of 5 mL every minute to identify LA toxicity phenomena.
Complications : Unintentional epidural or spinal anesthesia, retroperitoneal hematoma, and renal injury are the rare complications o f lumbar plexus block.
5.17 Iliohypogastric and Ilioinguinal Nerve Block
Anatomy (Fig. 5.37 ): Ilioinguinal (ILIN ) and iliohypogastric (ILHN ) nerves both emanate from the first lumbar spinal root. As they emerge from the lateral border of the psoas major, they pass obliquely across the quadratus lumborum and iliacus and finally perforate the transverse muscle above the iliac cres t. The ILHN lies medial to the ILIN. The ILHN pierces the internal oblique muscle distributing filaments to it and lies between the external and internal oblique muscles. It descends medially and caudally accompanying the spermatic cord through the subcutaneous inguinal ring. The ILHN supplies the skin over the inguinal region. The ILIN runs anteroinferiorly to the superficial inguinal ring, where it emerges to supply the skin on the superomedial aspect of the thigh.

The anatomy of ilio hypogastric (IH) and ilioinguinal (II) nerves. GF genitofemoral nerve, Gb genital branch, Fb femoral branch, P psoas muscle
Indications: Anesthesia for any somati c procedure involving the lower abdominal wall/inguinal region such as inguinal herniorrhaphy a nd for analges ia after surgical procedures using a Pfannenstiel incision. These blocks do not provide visceral anesthesia.
Patient position: Supine.
What you need: A high-frequency (10–15 MHz) linear probe, 50–80-mm and 20–21-gauge needle, 20-mL syringe, sterile gloves, disinfectant, local anesthetic 5–10 mL.
Sonoanatomy (Fig. 5.38 ): The anterior superior iliac spine (ASIS) is the standard starting positi on from which the transducer sho uld be slowly moved along the ASIS-umbilicus line. The adult ILIN can be visualized between the internal oblique and transverse or external oblique muscles and within 1–3 cm from the ASIS. The ILHN lies im mediately adjacent or somewhat medial to it.

(a) Patient position an d needle entry point. (b) Sonoanatomy. EO external oblique muscle, IO internal oblique muscle, TA transverse abdominis muscle IH iliohypogastric nerve, II ilioinguinal nerve IC Iliac Crest. Long white arrow needle direction and target point
How to do it (Fig. 5.38 ): Put the probe perpendicular to the inguinal ligament so that the lateral aspect of the probe lies on top of the iliac crest. The ASIS is the standard starting position from which the transducer was moved slowly along the ASIS-umbilicus line. Ilioinguinal and iliohypogastric nerves are sought in the fascial plane between the external oblique and internal oblique and between internal oblique and transverse abdominis muscle. The ilioinguinal nerve is usually foun d close to the iliac crest, and the iliohypogastric nerve lies medial to it.
Complications: Perforation of both the small and large bowels and creation of a pelvic hematoma have been reported after ilioingui nal/iliohypogastric blocks without ultra sound guide.
5.18 Lateral Femoral Cutaneous Nerve Block
Anatomy (Fig. 5.39 ): The lateral femoral cutaneous nerve (LFCN ), arises from the dorsal divisions of L2–L3. After emerging from the lateral border of the psoas major muscle, it courses inferiorly and laterally toward the anterior superior iliac spine (ASIS) . The nerve passes under the inguinal ligament and over the sartorius muscle into the thigh, where it divides into two branches (anterior and posterior).

Anatomy of the l ateral femoral cutaneous nerve. I iliacus muscle, S sartorius muscle, TFL tensor fasciae latae muscle
Indications: LCFN provide s sensory innervation of the lateral thigh. Anesthesia of this nerve is useful for head neck surgery in older people. It is also used in the management of meralgia paresthetica caused by the entrapment o f the nerve. The ultrasound-guided techniques showed a higher success rate because of a high variability in the course of the nerve.
Patient position: Supine positi on with the leg in a neutral position.
What you need: A high-frequency (10–15 MHz) linear probe and a reflective atraumatic 22G ultrasound needle, 50 mm of length. 4–5 mL of local anesthetic.
Sonoanatomy (Fig. 5.40): The LFCN i s identified as a hypoechoic structure generally foun ded in the interfascial plane above the sartorius muscle medially and the tensor fascia lata muscle laterally. It looks like an “eye” with a hyperechoic circle inside of an almond-shaped structure.

Sonoanato my. S sartorius muscle, TLF tensor fascia lata, LFC lateral femoral cutaneous nerve, Long white arrow needle direction and target point
How to do it (Fig. 5.41): We suggest to identify the ASIS and then move the linear probe medially and inferiorly to locate the fascia lata and the sartorius muscle. Look for the “eye sign” above the sartorius muscle. Insert the n eedle in-plane. The injection should be done below the fascia lata.

Patient position and needle entry point
Tips and tricks: Insert the needle with a shall ow angle to reach the plane just below the fascia lata immediately medial and inferior to the ASIS.
Complications: Intraneural or intravascular injection.
5.19 Femoral Nerve Block
Anatomy (Fig. 5.42): The femoral nerve is the largest branch of the lumbar plexus, arising from the second, third, and fourth lumbar nerves. The femoral nerve passes underneath the inguinal ligament into the thigh. As it passes beneath the inguinal ligament, the nerve is positioned lateral and slightly deeper than the femoral artery between the psoas and iliac muscles.

A trans-sectional v iew of the thigh showing the adductor canal. IP biceps muscle, P brachialis muscle, F femur, Fn with black arrow femoral nerve close to femoral artery and vein
Indications: Anesthesia and analg esia for anterior thigh, femur, and knee surgery.
Patient position: The patient is in su pine position with the leg slightly externally rotated.
What you need: A high-frequency (10–15 MHz) linear probe and a reflective atraumatic 22G ultrasound needle. 10–20 mL of local anesthetic.
Sonoanatomy (Fig. 5.43 ): The nerve lies about 1–2 cm lateral to the artery, positioned below fascia iliaca and lata and above the iliopsoas muscle and is contained within a triangular-shaped sheath of fascia by the ligamentum i liopectineus. The nerve itself can have a triangular or oval shape and is often not clearly visualized. Because of this, the triangle created by the femoral artery medially, fascial planes anteriorly, and the iliopsoas muscle posteriorly is used as the target for the block. The nerve becomes visualized after injection.

(a) Patient positio n and needle entry point. (b) Sonoanatomy of the inguinal area. Fn femoral nerve, PS iliopsoas muscle, PE pectineus muscle, A femoral artery, V femoral vein, F femur
How to do it (Fig. 5.43 ): The probe is placed in the inguinal crease, parallel to the inguinal l igament and transverse to femoral vein and artery with the indicator toward the patient’s right. The probe is slid medial to lateral until the femoral vessels are seen. Insert the needle in-plane (Fig. 3) until the needle tip is witnessed adjacent (either above, below, or lateral) to the nerve; after inject the anesthetic solution.
Tips and tricks: To confirm the proper needle placement, inject 1–2 mL of local anesthetic. When injection of the local anesthetic does not appear to result in a spread close to the femor al nerve, additional needle repositions and injections may be necessary.
Complications: Intraneural or intravascular injection.
5.20 Saphenous Nerve Block
Anatomy (Fig. 5.44): The saphenous nerve is the largest cutaneous branch of the femoral nerve. The saphenous nerve often lies anterior to the femoral artery as this vessel passes beneath the sartorius muscle and posterior to the aponeurotic covering of the adductor canal. It descends along the medial side of the knee posterior to the sartorius muscle. It is a sensory nerve covering the medial aspect of the calf, ankle, foot, and great toe.

A trans- sectional view of the thigh showing the adductor canal. RF rectus femoris muscle, VL vastus lateralis muscle, VI vastus intermedius muscle, VM vastus medialis muscle, SR sartorius muscle, A adductor longus muscle, S with black arrow saphenous nerve
Indications: Anesthesia and anal gesia of anterior aspect of the knee and leg.
Patient Position: Supine position with the leg externally rotated (frog position).
What you need: a high-frequency (10–15 MHz) linear probe and a reflective atraumatic 22G ultrasound needle. 5–10 mL of local anesthetic.
Sonoanatomy (Fig. 5.45 ): The adductor canal in the lower half of the thigh is cove red by the sartorial muscle in its descent laterally to medially across the anterior thigh. The sides of the triangular canal are formed by the vastus medialis laterally and adductor longus or magnus medially. The femoral artery passes beneath the muscle. The saphenous nerve is infrequently seen on the ultrasound image; however, sometimes it is visualized as a small round hyperechoic structure medial to the artery. A femoral vein accompanies the artery and saphenous nerv e, which are all typically visualized at 2–3 cm depth.

(a) Patient posit ion and needle entry point. (b) Sonoanatomy of the adductor canal. S sartorius muscle, VM vastus medialis muscle, AL adductor longus muscle, Sn saphenous nerve, A femoral artery, V femoral vein, Long white arrow needle direction and target point
How to do it— block at the adductor canal (Fig. 5.45 ): Put the probe transverse to the longitudinal axis and scan the m edial aspect of the thigh. Identify the femoral artery, the sartorius muscle, and the saphenous nerve below it. Insert the needle in-plane. The aim is to insert the needle deep to the sartorius and depositing the local anesthetic medial to the artery.
Block at tibial level (Fig. 5.46 ): Put the probe in a transverse plane at the level of tibial tuberosity; insert the needle in-plane. Here the nerv e pierces the fascia lata between the sartorius and the gracilis tendons and joins the saphenous vein. The aim is to insert the needle near the saphenous vein.

(a) Patient positio n and needle entry point. (b) Sonoanatomy of a transverse section at tibial level. S: saphenous nerve, Long white arrow needle direction and target point
Tips and tricks: Visualization of the nerve, at the abductor canal, is not necessary for this block. Administration of 5–10 mL of local anesthetic next to the artery should suffice without confirming the nerve position.
Also at the tibial level the saphenous nerve is difficult to visualize, but the block is easily performed with an ultrasound-guided peri venous injection of local anesthetic.
Complications: Intraneural or i ntravascular injection.
5.21 Obturator Nerve Block
Anatomy (Fig. 5.47 ): The obturator nerve arises from the anterior rami of the second, third, and fourth lumbar nerves. The obturator nerve then runs along the lateral wall of the lesser pelvis and extends to the anterior thigh after passing through the obturator canal. During its course, the obturator nerve divides into anterior and posterior branches that run between the pectineus and obturator externus muscles.

Schema of obtur ator nerve anatomy AB Adductor brevis, AL Adductor longus, AM Adductor magnus
Indications: Analgesia/anesthesia of th e medial aspect of thigh and knee. R elief of painful adductor muscle contractions or to prevent adduction of thigh during transurethral bladder surgery.
Patient position: The patient is in supine position. The thigh is slightly abducted and laterally rotated.
What you need: A high-frequency (10–15 MHz) li near probe and a reflec tive atraumatic 22G ultrasound needle. 3–5 mL of local anesthetic for each branch.
Sonoanatomy (Fig. 5.48 ): The two branches of the obturator nerve appear as hyperechoic lip-shaped structures contained in the fascia of adductor muscles. The anterior branch of the obturator nerve lies in a fascial layer between the pectin eus, adductor longus, and adductor brevis muscles. The posterior branch lies between the adductor brevis and the adductor magnus muscles. Often the anterior and the posterior branches of the obturator nerve are not visible like hyperechoic structures, and only the fascial planes can be distinguished.

(a) Patient position and needle entry point. (b) Sonoanatomy of medial aspect of upper thigh showing adductor longus AL, brevis AB, and magnus muscles AM in a transverse view P pettineus, OAB Obturator anterior branch, OPB Obturtor Posterior branch. Long white arrows needle direction and target points
How to do it (Fig. 5.48 ). Put the pro be horizontal, 1–3 cm inferior to the inguinal crease on the medial aspect (adductor compartment) of the thigh. Identify the three adductor muscles (pectineus, adductor longus, and brevis); insert the needle in-plane to reach the fascial plane and the anterior branch between pectineus and adductor longus and the posterior one between adductor longus and magnus.
Tips and tricks: A low-current nerve stimulation that elicits adductor muscle contraction can be used to aid localization of the obturator nerve.
When the obturator nerve branches are not visible, perform the block just putting the anesthetic solution into the appropriate i nterfascial planes.
Complications: Intraneural an d intravascular injection.
5.22 Sciatic Nerve Block
Anatomy (Fig. 5.49 ): The sciatic nerve is the largest nerve in the human body, originating from the lumbosacral plexus (L4–5 and S1–3) and providing sensory and motor innervation to the lower extremity.

Schema of sciatic nerve anatomy S sciatic nerve, T tibial nerve, GM gluteus maximus muscle, P piriformis muscle, BF Biceps femoris muscle, SM semitendinosus muscle
The sciatic nerve exits the pelvis via the greater sciatic foramen below the piriformis muscle. In the gluteal region, the sciatic nerve courses between muscle layers. The sciatic nerve anterior (deep) to the gluteus maximus muscle is found just l ateral to the origin of the biceps femoris muscle at the ischial tuberosity.
The sciatic nerve lies medial to the greater trochanter.
In the subgluteal region, the sciatic n erve is more accessible for the block, even in obese patients, because it is more superficial than in t he gluteal region and it lies within a palpable groove in this location.
Indications: With femoral nerve block for knee and lower limb surgery and foot surgery.
Patient position: The patient is in a position between the lateral decubitus and prone position (Sim’s position). The leg to be blocked is up, with the hip and knee flexed.
What you need: A low-frequency (4–6 MHz) convex probe and a reflective atraumatic 22G ultrasound needle. 15–20 mL of local anesthetic.
Sonoanatomy (Fig. 5.50 ): In the sub gluteal region, the sciatic nerve usually appears as a wedge-shaped hyperechoic structure between the two hyperechoic bony prominences of the ischial tuberosity and the greater trochanter of the femur. The sciatic nerve is located immediately deep to the gluteus muscles, superficial to the quadratus femoris muscle.

(a) Patient position and needle entry point. (b) Sonoanatomy. S sciatic nerve, GT greater trochanter, GM gluteus maximus muscle, QF quadratus femoris muscle, IT ischial tuberosity, Long white arrow needle direction and target point
How to do it (Fig. 5.50 ): For the subgluteal approach, place the probe over the subgluteal region in a transverse plane.
Move the probe from lateral (great tr ochanter area) to medial (ischial tuberos ity) until the sciatic nerve is visible in a sling between the two hyperechoic bony shadows. Insert the needle in-plane. The angle of approach of the needle is often close to perpendicular to the skin.
This makes visualization of the entire needle shaft using the in-plane approach more difficult.
Performing this block with ne rve st imulation guidance is very helpful to identify the sciatic nerve when it is not clearly visible. The goal is to see circumferential spread of hypoechoic local anesthetic solution around the nerve.
Tips and tricks: It is often easier to identify the sciatic nerve from its surrounding structures by decreasing the gain on the US machine.
As imaging of the needle tip c an be problematic for the deep location, its position is often inferred by injections of small volumes of saline solution, local anesthetic, or air.
Never inject against high resistance to injection (>15 psi) because this may signal an intraneural injection.
Complications: Intraneural in jection is the more feasible. Intravascular injection is more unlikely for the lack of adjacent vascular structures.
5.23 Popliteus Nerve Block
Anatomy (Fig. 5.51 ): Sciatic nerve, after emerging from the pelvis, travels deep in the posterior thigh. Proximal to the popliteal fossa, the sciatic nerve lies more superficial, between the long head of the biceps femoris laterally and the semimembranosus muscles medially. In this location, the nerve generally bifurcates into the common peroneal and tibial nerves. These nerves continue into the popliteal fossa where they lie superficial and lateral to the popliteal vessels. The tibial nerve provides innervation to the majority of the posterior lower extremity, knee joint, a nd plantar surface of the foot. The common peroneal nerve provides sensory innervation to the dorsal lateral foot and ankle and posterolateral portion of the distal lower extremity via its branches.

Schema o f popliteal fossa anatomy BF Biceps femoris muscle, ST Semitendinosus muscle, SM semimembranosus muscle, LG Gastrocnemius lateral head, MG Gastrocnemius medial head
Indications: Anesthesia and analgesia of a nkle and foot with saphenous nerve block.
Patient position: Prone position with a roller pillow under the ankle.
What you need: A high-frequency (10–15 MHz) linear probe and a reflective atraumatic 22G ultrasound needle. 15–20 mL of local anesthetic.
Sonoanatomy (Fig. 5.52 ): In the popliteal fos sa, at the popliteal crease, the femur is identified as characteristic hyperechoic stripe and dense posterior shadowing; the pulsatile popliteal artery and corresponding vein are located superficial and medial to the femur. At this level, the sciatic nerve has generally bifurcated into the tibial and common peroneal nerves. The tibial is found superficial and lateral to the artery. The common pe roneal nerve is found lateral to the tibial nerve at a similar depth.

(a) Patient position and needle entry point. (b) Sonoanatomy in a transverse section of popliteal region showing popliteal nerve, vein, and artery. F femur, ST semitendonosus muscle, SM semimembranosus muscle. Long white arrow needle direction and target point
How to do it (Fig. 5.52 ): The probe is pl aced transversely across the popliteal fossa at the popliteal crease. The needle is inserted in an in-plane approach from the side of the probe; it is advanced to the deep border of the sciatic nerve. The goal is to surround the nerve(s) with local anesthetic.
Tips and tricks: If nerve visualization is difficult, ask the patient to plantar flex and dorsiflex the foot. This will cause the “see-saw” sign: tibial and peroneal components move during foot movement.
If blocking the tibial and common peroneal nerves after the bifurcation, the nerve farther from the needle entry site is blocked before blocking the closer one.
Complications: Intraneur al or intrav ascular injection.
5.24 Ankle Block
Anatomy (Fig. 5.53 ): Five nerves provide sensory innervation to the foot at or below the level of the ankle . These are posterior tibial, sural, deep, and superficial peroneal nerves (terminal branches of sciatic nerve) and saphenous nerve (branch from the femoral nerve).

Schema of an kle nerves anatomy PTn posterior tibial nerve, SAn saphenous nerve, DPn deep peroneal nerve, SPn superficial peroneal nerve, SUn surak nerve. T tibia, P Fibula, EDL extensor digitorum longus muscle, TA tibial anterior muscle, FHL flexor hallucis longus, PP peroneus muscles
Indications: Acute pain management in trauma as ankle block results in anesthesi a of the entire foot. Foot surgery without the need of tourniquet and for postoperative pain relief as it causes no motor blockade of the foot.
Patient position: Supine position with a footrest underneath the calf facilitates access to the ankle, especially for the tibial and sural nerve blocks.
What you need: A small (25 mm) high-frequency (10–15 MHz) linear probe or a hockey probe and a 22–25-gauge ult rasound needle, 4–5 cm of length. 3–5 cc of local anesthetic for each nerve.
Sonoanatomy: Tibial nerve passes posterior to the medial malleolus and posterior to the posterior tibial artery at the ankle (Fig. 5.54). A transducer placed in the transverse orientation at the level of the extensor retinaculum will show the deep peroneal nerve lying immediately lateral to the artery, on the surface of the tibia (Fig. 5.55). A transducer placed transverse ly on the leg, approximately 5 cm proximal and anterior to the lateral malleolus, will identify the superficial peroneal nerve lying in the subcutaneous tissue over the fascia (Fig. 5.56). Near to the lateral malleolus, the sural nerve can be visualized as a small hyperechoic structure that is intimatel y associated with the small saphenous vein (Fig. 5.57). The saphenous nerve is a small nerve; it is best visualized 10–15 cm proximal to the medial malleolus, using the saphenous vein as a landmark (Fig. 5.58).

(a) Patient position an d needle entry point. (b) Sonoanatomy of the tibial nerve at the ankle. PTn posterior tibial nerve, A tibial artery, V tibial vein, FHL flexor hallucis longus, White dot needle target point

(a) Patient position and needle entry point. (b) Sonoanatomy. DP deep peroneal nerve, A anterior tibial artery, Long white arrow needle direction and target point

(a) Patient position and needle entry point. (b) Sonoanatomy. SP superficial peroneal nerve, F fibula, EDL extensor digitorum longus muscle, EHL Extensor hallucis longus. Long white arrow needle direction and target point

(a) Patient po sition and needle entry point. (b) Sonoanatomy. Sn sural nerve, V small saphenous vein, F fibula, T tibia. Long white arrow needle direction and target point

(a) Patient position and needle entry point. (b) Sonoanatomy. S saphenous nerve, V saphenous vein, T tibia, FDL flexor digitorum longus. Long white arrow needle direction and target point
How to do it. For all blocks put the pro be in a transverse plane. Insert the ne edle in-plane or out-of-plane.
Tips and tricks: The nerves at the ankle are so small that it is difficult to detect them. The simpler method is to look for the vessel.
Do not press the probe in order to not squeeze vessels.
Complications: Intrane ural and in travascular injection.
Suggested Readings
Beaudoin FL, Nagdev A, Merchant RC, Becker BM. Ultrasound-guided femoral nerve blocks in elderly patients with hip fractures. Am J Emerg Med. 2010;28(1):76–81.
Ben-Ari A, Moreno M, Chelly JE, Bigeleisen PE. Ultrasound-guided paravertebral block using an intercostal approach. Anesth Analg. 2009;109:1691–4.
Casati A, Baciarello M, Di Cianni S, Danelli G, De Marco G, Leone S, Rossi M, Fanelli G. Effects of ultrasound guidance on the minimal effective anaesthetic volume required to block the femoral nerve. Br J Anaesth. 2007;98:823–7.
Demirelli G, Baskan S, Karabeyoglu I, Aytac I, Ornek DH, Erdogmus A, Baydar M. Comparison of ultrasound and ultrasound plus nerve stimulator guidance axillary plexus block. J Pak Med Assoc. 2017;67(4):508–12.
Dufour E, Toussaint A, Liu N, Fischler M, Nourry G, Vercoutère M. Ultrasound-guided perineural circumferential median nerve block in carpal tunnel syndrome. Anaesthesia. 2013;68(4):434–6.
Falyar CR. Ultrasound-guided ankle blocks: a review of current practices. AANA J. 2015;83(5):357–64.
Franco CD, Williams JM. Ultrasound-guided interscalene block: reevaluation of the “stoplight” sign and clinical implications. Reg Anesth Pain Med. 2016;41(4):452–9.
Guirguis MN, Abd-Elsayed AA, Girgis G, Soliman LM. Ultrasound-guided transversus abdominis plane catheter for chronic abdominal pain. Pain Pract. 2013;13(3):235–8.
Gurnaney H, Ganesh A. Incidence and effects of unintentional intraneural injection during ultrasound-guided subgluteal sciatic nerve block. Reg Anesth Pain Med. 2013;38:72.
Hara K, Sakura S, Nomura T, Saito Y. Ultrasound guided thoracic paravertebral block in breast surgeries. Anesthesia. 2009;64:223–5.
Hara K, Sakura S, Shido A. Ultrasound-guided lateral femoral cutaneous nerve block: comparison of two techniques. Anaesth Intensive Care. 2011;39:69–72.
Henshaw DS, Kittner SL, Jaffe JD. Ultrasound-guided continuous superficial radial nerve block for complex regional pain syndrome. J Pain Palliat Care Pharmacother. 2016;30(2):118–23.
Herring AA, Stone MB. The accuracy of a handheld ultrasound machine in locating the sciatic nerve in the popliteal fossa. Reg Anesth Pain Med. 2004;29:413–6.
Herring AA, Stone MB, Fischer J, Frenkel O, Chiles K, Teismann N, Nagdev A. Ultrasound-guided distal popliteal sciatic nerve block for ED anesthesia. Am J Emerg Med. 2011;29(6):697.e3–5.
Honnannavar KA, Mudakanagoudar MS. Comparison between conventional and ultrasound-guided supraclavicular brachial plexus block in upper limb surgeries. Anesth Essays Res. 2017;11(2):467–71.
Ilfeld BM. Continuous peripheral nerve blocks: an update of the published evidence and comparison with novel, alternative analgesic modalities. Anesth Analg. 2017;124(1):308–35.
Jenstrup MT, et al. Effects of adductor-canal-blockade on pain and ambulation after total knee arthroplasty: a randomized study. ActaAnaesthesiol Scand. 2012;56(3):357–64.
Kim BG, Han JU, Song JH, Yang C, Lee BW, Baek JS. A comparison of ultrasound-guided interscalene and supraclavicular blocks for post-operative analgesia after shoulder surgery. Acta Anaesthesiol Scand. 2017;61(4):427–35.
Moritz T, Prosch H, Berzaczy D, Happak W, Lieba-Samal D, Bernathova M, Auff E, Bodner G. Common anatomical variation in patients with idiopathic meralgia paresthetica: a high resolution ultrasound case-control study. Pain Physician. 2013;16:E287–93.
Nwawka OK, Miller TT, Jawetz ST, Saboeiro GR. Ultrasound-guided perineural injection for nerve blockade: does a single-sided injection produce circumferential nerve coverage? J Clin Ultrasound. 2016;44(8):465–9.
O Riain SC, Donnell BO, Cuffe T, Harmon DC, Fraher JP, Shorten G. Thoracic paravertebral block using real-time ultrasound guidance. Anesth Analg. 2010;110:248–51.
Rahiri J, Tuhoe J, Svirskis D, Lightfoot NJ, Lirk PB, Hill AG. Systematic review of the systemic concentrations of local anaesthetic after transversus abdominis plane block and rectus sheath block. Br J Anaesth. 2017;118(4):517–26.
Redborg KE. Ultrasound improves the success rate of a tibial nerve block at the ankle. Reg Anesth Pain Med. 2009;34(3):256–60.
Shteynberg A, Riina LH, Glickman LT, Meringolo JN, Simpson RL. Ultrasound guided lateral femoral cutaneous nerve (LFCN) block: safe and simple anesthesia for harvesting skin grafts. Burns. 2013;39:146–9.
Strakowski JA. Ultrasound-guided peripheral nerve procedures. Phys Med Rehabil Clin N Am. 2016;27(3):687–715.
Tammam TF. Ultrasound-guided infragluteal sciatic nerve block: a comparison between four different techniques. Acta Anaesthesiol Scand. 2013;57:243–8.
Tumber PS, Bhatia A, Chan VW. Ultrasound-guided lateral femoral cutaneous nerve block for meralgia paresthetica. Anesth Analg. 2008;106:1021–2.
Turner AL, Stevenson MD, Cross KP. Impact of ultrasound-guided femoral nerve blocks in the pediatric emergency department. Pediatr Emerg Care. 2014;30(4):227–9.
Ueshima H, Otake H, Lin JA. Ultrasound-guided quadratus lumborum block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:2752876.
Yoshida T, Nakamoto T, Kamibayashi T. Ultrasound-guided Obturator nerve block: a focused review on anatomy and updated techniques. Biomed Res Int. 2017;2017:7023750.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Puntillo, F., Bertini, L., Bosco, M., Tedesco, M., Baciarello, M. (2018). US-Guided Nerve Blocks: Procedure Technique. In: Silvestri, E., Martino, F., Puntillo, F. (eds) Ultrasound-Guided Peripheral Nerve Blocks. Springer, Cham. https://doi.org/10.1007/978-3-319-71020-4_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-71020-4_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-71019-8
Online ISBN: 978-3-319-71020-4
eBook Packages: MedicineMedicine (R0)