
Abstract
Objective
To determine the diagnostic efficacy of comparative supine and sitting lateral radiographs in the diagnosis of incident osteoporotic vertebral fracture (OVF), 41 incident OVF in 38 patients, which had been diagnosed by magnetic resonance imaging, were evaluated.
Methods
There were 27 female and 11 male patients with the average age of 78 years (range, 54–94 years). Using lateral decubitus-position radiographs, fractures were classified into normal, wedge, biconcave, and crush types, and graded from 0 to 3. Vertebrae showing any measurable changes in the vertebral body height between supine and sitting radiographs were referred to as mobile fractures. Mobile fractures and fixed (nonmobile) fractures were compared with regard to gender and age of patients, location, fracture grade, and the presence of prevalent OVF. The Mann–Whitney U test and the Fisher’s exact probability test were used for statistical analysis.
Results
Of 41 incident OVF, 33 vertebrae (80.5%) showed dynamic mobility in supine and sitting lateral radiographs. Of nine OVF with small deformities (grade 0 or 0.5) and 19 OVF with prevalent OVF, dynamic mobility was seen in six (66.7%) and 15 (78.9%), respectively. Age was significantly higher in patients with mobile fractures than those with fixed fractures. Mobile fractures included a significantly lower percentage of thoracic vertebrae (6%) than of fixed fractures (37.5%). Seven out of eight fixed fractures (87.5%) were grade 1 or less.
Conclusions
These findings indicate that comparative supine and sitting lateral radiographs are a simple diagnostic procedure for incident OVF available in daily clinics.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Diagnosis of osteoporotic vertebral fractures (OVF) is crucial for proper treatment of acute back pain and prevention of post-fracture sequelae [1–3]. Despite current advances in diagnostic technology, conventional radiography is still the mainstay of diagnostic tools for OVF in daily clinics. In radiographs, OVF is identified on the basis of interpretation of individual radiographic findings. This causes difficulty in distinguishing incident OVF from other conditions with similar radiographic appearances such as non-fracture deformity, and normal variants, and prevalent OVF [4–7]. False-negative rates of diagnosis of incident OVF by conventional radiographs, as were reported, ranged from 27% to 48.5%, despite strict radiographic protocols with classification and semiquantification of OVF [4, 5, 7]. Although magnetic resonance imaging (MRI) and high-resolution imaging with dual X-ray absorptiometry were shown to be more promising than plain radiographs in diagnosis of incident OVF [1, 2, 4, 6, 8], they are costly and are not always immediately available.
Comparative lateral radiographs on weight-bearing positions (standing or sitting) and supine positions have been used to determine indication of percutaneous vertebroplasty for delayed union or nonunion of OVF [9–11] and also surgical indication of traumatic thoracolumbar fractures [12]. However, no studies in the English literature have yet focused on their diagnostic value for incident OVF. In the present study, we analyzed 41 incidents of OVF which had been diagnosed by MRI and assessed for dynamic mobility in supine and sitting lateral radiographs.
Materials and methods
Inclusion criteria in this study were of patients who were presented with acute low back or back pain within 14 days after onset and were diagnosed as having OVF by MRI. T1-weighted images and short tau inversion recovery (STIR) sequence images were used in MRI. Patients were examined using anteroposterior and lateral decubitus-position radiographs and also spine cross-table lateral and sitting lateral radiographs on the day of initial presentation. The radiographs were taken at a film-focus distance of 1.1 m. Between February 2007 and April 2008, 39 patients including two patients who were presented on two different occasions met the criteria. One patient who had not been able to stay in a sitting position while taking a sitting lateral radiograph was excluded.
There were 27 female and 11 male patients with the average age of 78 years (range, 54–94; Table 1). Two patients (cases 14 and 31) with OVF at 60 years old or younger had both been treated with corticosteroid for aplastic anemia and dermatomyositis, respectively. These 38 patients exhibited 41 fractures; two patients (cases 5 and 20) were presented twice on different occasions and one other patient (case 20) had a fracture involving two vertebrae. Fractures were distributed from T7 to L5 vertebrae; 5 in the thoracic spine (T7–T10), 22 in thoracolumbar junction (T11–L1), and 14 in the lumbar spine (L2–L5). Eighteen fractures were caused by a simple fall and 23 fractures occurred during daily activities. Nineteen patients showed prevalent OVF in radiographs and MRI.
Using lateral decubitus-position radiographs, fractures were classified into normal, wedge, biconcave, and crush types [13], and graded into 0 (normal), 0.5 (borderline, <20%), 1 (mild, 20–25%), 2 (moderate, 25–40%), and 3 (severe, >40% vertebral height reduction at any posterior, middle, or anterior point) [14].
Vertebral fracture mobility was determined by measuring the vertebral height to the nearest millimeter in lateral radiographs taken in the supine and sitting positions. Vertebrae showing any measurable changes in the vertebral body height between supine and sitting radiographs were referred to as mobile fractures.
Mobile fractures and fixed (nonmobile) fractures were compared with regard to gender and age of patients, location, fracture grade, and the presence of prevalent OVF. The Mann–Whitney U test was used in the analysis of interval data and the Fisher’s exact probability test was used in a 2 × 2 cross-contingency table.
Results
Of 41 incident OVF diagnosed by MRI, 33 vertebrae (80.5%) showed dynamic mobility in supine lateral and sitting lateral radiographs (Table 1). The average change in vertebral body height between supine lateral and sitting lateral radiographs was 6.1 mm (range, 2–12 mm). Radiographs of case 20 and case 27 were shown in Figs. 1, 2, 3, 4, 5, and 6, respectively, as the representative cases.

Case 20. Anteroposterior (a) and lateral decubitus-position (b) radiographs at the first presentation, showing scoliotic deformity of the L4 vertebra, wedge deformity of the L2 vertebral body, and irregularity of the anterior wall of the L3 vertebral body

Case 20. Comparative sitting (a) and supine (b) lateral radiographs taken at the first presentation revealed vertebral body mobility of L2 (3 mm) and L3 (7 mm). T1-weighed MR image (c) and STIR sequence MR image (d) showed signal changes consistent with compression fractures of L2 and L3 vertebrae. The patient was admitted to the hospital and immobilized with a Behler body cast. After 4 weeks, the cast was switched to a rigid body jacket and the patient was discharged

Case 20. One month after discharge, the patient fell down at home. The patient again was presented to the hospital with severe low back pain. Anteroposterior (a) and lateral decubitus-position (b) radiographs showed wedge deformity of the L2 and crush deformity of the L3 vertebral body. In these radiographs, new fractures were not detectable

Case 20. Comparative sitting (a) and supine (b) lateral radiographs at the second presentation then revealed an apparent vertebral body mobility of L1 (12 mm) but not of the L2 and L3 vertebrae. T1-weighed MR image (c) and STIR sequence MR image (d) confirmed fracture of the L1 vertebra in addition to the previous L2 and L3 fractures. Lack of dynamic mobility in the L2 and L3 vertebrae on the second visit indicates healing process of the L2 and L3 fractures

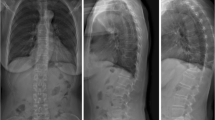
Case 27. Anteroposterior (a) and lateral decubitus-position (b) radiographs showed wedge deformity of L2, crush deformity of L3, and biconcave deformity of L4 and L5 vertebral bodies

Case 27. Sitting (a) and supine (b) lateral radiographs revealed a vertebral body mobility of L3 (5 mm) but not L2, L4, or L5 vertebrae. T1-weighed MR image (c) showed low signal intensity of L3 and L5 vertebral bodies. STIR sequence MR image showed a high signal intensity area only in L3 vertebral body, consistent with an incident compression fracture of L3 vertebra. This case illustrates the usefulness of comparative supine and sitting lateral radiographs in distinguishing incident OVF as opposed to multiple prevalent OVF
Diagnosis of incident OVF is difficult in cases where OVF exhibit small deformities or OVF coexist with prevalent OVF. In this regard, of nine OVF with small deformities (grade 0 or 0.5) and 19 OVF with prevalent OVF, dynamic mobility was seen in six (66.7%) and 15 (78.9%), respectively.
Table 2 depicts the results of comparison between 33 mobile fractures and eight fixed fractures. Age was significantly higher in patients with mobile fractures (80.4 ± 7.2) than those with fixed fractures (70.0 ± 9.2). Gender and presence of prior fracture had no significant difference between the groups. In contrast, mobile fractures included a significantly lower percentage of thoracic vertebrae (6%) than of fixed fractures (37.5%). Furthermore, seven out of eight fixed fractures (87.5%) were grade 1 or less, which was higher in percentage than mobile fractures (45.5%) with statistical significance.
Discussion
Comparative supine and sitting lateral radiographs identify incident OVF on the basis of fracture mobility. This differs in concept from conventional morphology-based fracture diagnosis. Identification of OVF by supine and sitting lateral radiographs does not require particular imaging modalities or precise morphometric assessment but simple measurement of the height of the vertebral body. In practice, this method can be as an alternative to MRI on the basis that the facilities for MRI scanning may not always be available.
Measurement of fracture mobility can be determined by flexion–extension radiographs, which have been used commonly in clinics. However, back pain during motion limits the range of flexion–extension and thus limits fracture mobility to be observed on radiographs. In fact, Hasidate et al. [15] demonstrated that the anterior wall height of fractured vertebrae was significantly larger in supine cross-table radiographs than in extension radiographs. Although back pain in patients with incident OVF can also hamper supine and sitting positioning, we encountered only one patient who was unable to sit up for the radiographs.
Morphology-based assessment of OVF has technical limitations in distinguishing OVF with no or small deformities (grade 0 or 0.5) from normal vertebrae, and incident OVF from prevalent OVF. It should be noted that 66.7% of grade 0 or 0.5 OVF were identified and 78.9% of fresh OVF could be distinguished from prevalent OVF by supine-sitting lateral radiographs.
McKiernan et al. [10] analyzed 65 OVF with a mean fracture age of 117 days by using comparative supine and standing lateral radiographs and found dynamic vertebral mobility in 35% of fractures. In the present study, mean fracture age was 5 days (range 0–14 days) and dynamic vertebral mobility was noted in 80.5% of 41 OVF. Fractures showing dynamic mobility in the study by McKiernan et al. [10] probably represent delayed union or nonunion cases.
Eight fixed fractures (false-negative cases) showed the following characteristics; (1) patients were younger than those showing mobile fractures, (2) 37.5% were thoracic spine fractures, and (3) 87.5% were grade 1 or less fractures. These findings likely reflect the instability of fractures, which is low in young patients (supposedly less osteoporotic), thoracic spine fractures, and low grade fractures. Conversely, the findings suggest that comparative supine and sitting lateral radiographs are suitable for detection of OVF in elder patients, thoracolumbar and lumbar spine fractures and those with grade 2 and 3. In this regard, 23 out of 24 fractures (95.8%) in patients aged 80 years or older showed fracture mobility in the present study.
The limitations of the present study include the small number of patients, lack of non-fracture controls, and the presence of only one examiner of the radiographs. In this regard, a simple measurement of vertebral body height decreases the concern for inter-observer discrepancy. However, the findings of this study need to be verified by larger studies.
In conclusion, this is the first report demonstrating the efficacy of comparative supine and sitting lateral radiographs for diagnosis of incident OVF. The concept of dynamic vertebral body mobility is useful in detection of incident OVF and assessment of fracture healing in addition to decision making for indication of percutaneous vertebroplasty and other surgical treatments.
References
Papaioannou A, Watts NB, Kendler DL, Yuen CK, Adachi JD, Ferko N (2002) Diagnosis and management of vertebral fractures in elderly adults. Am J Med 113(3):220–228
Grigoryan M, Guermazi A, Roemer FW, Delmas PD, Genant HK (2003) Recognizing and reporting osteoporotic vertebral fractures. Eur Spine J 12(Suppl 2):S104–S112
Ferrar L, Jiang G, Adams J, Eastell R (2005) Identification of vertebral fractures: an update. Osteoporos Int 16(7):717–728
Guermazi A, Mohr A, Grigorian M, Taouli B, Genant HK (2002) Identification of vertebral fractures in osteoporosis. Semin Musculoskelet Radiol 6(3):241–252
Binkley N, Krueger D, Gangnon R, Genant HK, Drezner MK (2005) Lateral vertebral assessment: a valuable technique to detect clinically significant vertebral fractures. Osteoporos Int 16(12):1513–1518
Link TM, Guglielmi G, van Kuijk C, Adams JE (2005) Radiologic assessment of osteoporotic vertebral fractures: diagnostic and prognostic implications. Eur Radiol 15(8):1521–1532
Ito Z, Harada A, Matsui Y, Takemura M, Wakao N, Suzuki T, Nihashi T, Kawatsu S, Shimokata H, Ishiguro N (2006) Can you diagnose for vertebral fracture correctly by plain X-ray? Osteoporos Int 17(11):1584–1591
Kanchiku T, Taguchi T, Kawai S (2003) Magnetic resonance imaging diagnosis and new classification of the osteoporotic vertebral fracture. J Orthop Sci 8(4):463–466
Faciszewski T, McKiernan F (2002) Calling all vertebral fractures classification of vertebral compression fractures: a consensus for comparison of treatment and outcome. J Bone Miner Res 17(2):185–191
McKiernan F, Faciszewski T (2003) Intravertebral clefts in osteoporotic vertebral compression fractures. Arthritis Rheum 48(5):1414–1419
McKiernan F, Jensen R, Faciszewski T (2003) The dynamic mobility of vertebral compression fractures. J Bone Miner Res 18(1):24–29
Mehta JS, Reed MR, McVie JL, Sanderson PL (2004) Weight-bearing radiographs in thoracolumbar fractures: do they influence management? Spine 29(5):564–567
Eastell R, Cedel SL, Wahner HW, Riggs BL, Melton LJ 3rd (1991) Classification of vertebral fractures. J Bone Miner Res 6(3):207–215
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8(9):1137–1148
Hashidate H, Kamimura M, Nakagawa H, Takahara K, Uchiyama S (2006) Pseudoarthrosis of vertebral fracture: radiographic and characteristic clinical features and natural history. J Orthop Sci 11(1):28–33
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kawaguchi, S., Horigome, K., Yajima, H. et al. Comparative supine-sitting lateral radiographs identifying incident osteoporotic vertebral fractures. Eur Orthop Traumatol 1, 157–162 (2011). https://doi.org/10.1007/s12570-010-0033-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12570-010-0033-7