
Abstract
Exposure to certain arsenic (As) species has been associated with increased cancer risk and a wide range of other health concerns, even at low levels. Here we used urine as a biomarker of As internal dose in a well-characterized cohort to relate diet, demographics and geography to exposure. As speciation in spot urine samples was determined for 89 participants aged ≥ 50 years from the Northern Ireland Cohort for the Longitudinal Study of Ageing (NICOLA), stratified to cover the country. Principal component analysis showed that all As species clustered together, suggesting that arsenobetaine, inorganic As (iAs) and the methylated species monomethylarsonic acid and dimethylarsinic acid forms have a common source. Seafood and alcohol consumption were positively correlated with As species, while dairy products (i.e. milk) and tap water were negatively correlated. Multiple regression analysis showed that diet explained approximately 30% of the variability in urinary iAs concentrations. Geography was not found to be a predictor of As exposure. Dairy consumption was negatively correlated and the best predictor of iAs in urine, explaining 15.9% of the variability. The majority of the variation in As biomarkers was not explained, suggesting the contribution of other sources and other non-predicted variables on As metabolism and elimination.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Human health is dependent on the quality of the food, air and water available. Long-term clinical health conditions (such as cardiovascular diseases, diabetes, neurodegenerative diseases, respiratory diseases and cancer) can be related to environmental and food exposure to toxic compounds (Wardrop and Le Blond 2015). In the case of the metalloid arsenic (As), high concentrations of As in drinking water are typically found in Bangladesh, West Bengal (India), Inner Mongolia (China), Taiwan, Argentina and Chile (Chappell et al. 2003; Wu et al. 2018). In these areas, it is well known from epidemiological studies that there is an association between inorganic As (iAs) exposure and urinary bladder, kidney and lung cancer risk (Chappell et al. 2003; IARC 2012). Although those naturally high As regions are of major concern, low–moderate chronic exposure to As have also been associated with a range of detrimental health effects, including an increased risk of skin lesions, diabetes, cardiovascular effects, neurotoxicity, lung disease, reproductive effects and cancer (WHO 2001).
Exposure to As can originate from different sources such as inhalation (Xu et al. 2013; Subhani et al. 2015), dermal (Ouypornkochagorn and Feldmann 2010), drinking water (IARC 2004; Chappell et al. 2003; Navoni et al. 2014; Diaz et al. 2015) and food (Meharg and Raab 2010; Signes-Pastor et al. 2017a). The contribution of these sources depends on As levels in each of these matrices. Food can be considered the main source of As exposure in the European Union and many other regions, where there is high percentage of population with access to treated water supplies (Meharg and Raab 2010; Signes-Pastor et al. 2017a). Rice consumption has been shown to be a concern for iAs exposure as it accumulates iAs up to concentrations tenfold higher than in other grains (Williams et al. 2006; Kordas et al. 2016; Davis et al. 2017). Dietary studies, using urine spot samples as a biomarker of As exposure, have shown that iAs in rice is both bioavailable and a dominant source in the diet (Signes-Pastor et al. 2017a; Wei et al. 2014). As species commonly found in urine include iAs, monomethylarsonic acid (MMA) and dimethylarsinic acid (DMA), both of which are human metabolites of iAs, and the non-toxic arsenobetaine (AsB), derived from seafoods (Navas-Acien et al. 2011; Popowich et al. 2016). Other dietary sources of As, and how general dietary patterns (liquid, alcohol, vitamin intake, etc.) interplay with As metabolism, the methylation of iAs to MMA and DMA, are not well understood.
This study has a developed country focus, Northern Ireland (NI), where a high percentage of people uses treated municipal water supplies with low levels of iAs (Signes-Pastor et al. 2017b) and where rice is not the dominant staple (Harrington et al. 2001). Here we evaluate the association between As exposure, nutrition and demographic variables in NI using a subset of participants aged ≥ 50 years from the Northern Ireland Cohort for the Longitudinal Study of Ageing (NICOLA). The subset was considered of settled geography since all participants were living in their own homes in NI. As has been shown to have strong environmental gradients in soils and waters over NI, as revealed through detailed sampling (at 2 km2 density) (Geological Survey Northern Ireland, GSNI 2007).
Materials and Methods
Study Population
This study was conducted in a sub-sample (n = 89) of participants from the NICOLA study who were also taking part in the NICOLA dietary validation study (NIDAS). Participants were randomly selected, aged ≥ 50 years (born on or before 30 September 1962) and living in their own homes across NI. NIDAS was primarily conducted to validate the dietary assessment methodology used in the NICOLA study. Ethical approval for both the NICOLA and NIDAS studies was obtained from the School of Medicine, Dentistry and Biomedical Sciences Research Ethics Committee, Queen’s University Belfast (Ethical Approval Numbers 15.18 and 12.23, respectively).
The inclusion criteria for this sub-sample were (a) participants in the NICOLA study, (b) participants willing to allow a researcher to visit them at their home. The exclusion criteria were (a) participants unable to provide informed consent, (b) participants with medical conditions that would limit their ability to complete the protocol. Each participant signed a written informed consent prior to participating in the study.
Spot urine samples were collected for As speciation analysis. All urine samples were stored at − 80 °C until analysis. All participants were asked to complete a 4-day food diary which involved them recording their food and drink intake over a period of 4 days (two weekdays and two weekend days). The dietary assessment and urine sampling were repeated after a period of 6 months to allow the capture of any seasonal variation in diet. Demographic data (age, gender, location of residence, level of education, smoking status and alcohol consumption) were obtained via a computer-assisted personal interview, while clinical data [weight, height, body mass index (BMI)] were obtained as part of the NICOLA health assessment (Neville et al. 2019).
As Speciation Analysis and Sample Preparation
iAs, MMA, DMA and AsB were analysed in urine by ion chromatography interfaced with inductively coupled plasma-mass spectrometry detection (IC-ICP-MS) using the method published by Signes-Pastor et al. (2017c). Briefly, chromatographic separation was performed using a Dionex IonPac™ AS7 RFIC analytical column (2 × 250 mm, Thermo Scientific) protected by a Dionex IonPac™ AG7 guard column (2 × 50 mm, Thermo Scientific) and a 12.5 min gradient mobile phase starting from 100% 20 mM ammonium carbonate (A) up to 100% 200 mM ammonium carbonate (B). Mobile phase flow rate was 0.3 mL/min. Certified standards of AsB, DMA, tetramethylarsonium (TMAO), MMA and iAs were used to determine their retention times. The concentration of As species was determined using a DMA dilution series. Seronorm™ Trace Elements Urine (Lot 0,511,545, Sero®) and Clinchek® Urine Control, for As species, level 1, were used as certified reference material (CRM) for quality control. Working standards, blank samples, urine samples and CRMs were included within each analytical run.
The urine samples were prepared by appropriate dilution and centrifuged at 4500 × g for 5 min. Supernatants were transferred to 700 μL polypropylene vials with 1% analytical grade hydrogen peroxide (30%, Analar Normapur®) to convert all arsenite (AsIII) in arsenate (AsV). As species concentrations in urine were statistically modelled with and without normalization by specific gravity (SG).
Four-Day Food Diaries
Participants recorded all food and drink consumed over two weekdays and two weekend days (four consecutive days) by reporting the frequency, amount and method of food preparation. Amounts of foods were reported in household measures (for example, one table spoon) or natural measures (for example, one slice of bread). Researchers explained the dietary assessment protocols in detail to ensure close adherence. Completed food diaries were reviewed by the researchers in order to check if any entries were unclear and to clarify the information recorded. Mean food, energy and nutrient intakes from the food diaries were calculated using a computerized food analysis database (Nutritics 2018).
Statistical Analysis
All statistical analyses were performed using SPSS version 25.0 (SPSS, Inc., Chicago, IL) and the statistical significance was defined as p < 0.05. Descriptive statistics were obtained for all variables of interest. The urinary concentrations of As species were not normally distributed with positive-skew profile and were logarithmically transformed using base-10 for analysis. All analyses were carried out using As species concentration in urine, both adjusted, or not, by SG. Analysis of variance (ANOVA) was performed to evaluate the effect of geographical location on urinary concentrations of As species. Principal component analysis (PCA) was performed with As species in urine and selected foods, drinks and nutrients in order to analyse the relationships among these variables and to identify the main dietary factors affecting As exposure. Due to the different units of measurement of variables, raw data were standardized to receive equal weight in PCA. Variables were standardized by subtracting the mean values from the raw data and dividing by the standard deviation. PCA was carried out using covariance matrix, with extraction of two components and varimax rotation with Kaiser normalization. Multiple linear regression using stepwise method was performed to predict exposure to As from demographic, clinical and dietary variables.
Results and Discussion
A total of 89 participants [n = 42 males (47.2%), n = 47 females (52.8%)] were included in the analysis, with ages ranging from 51.1 to 89.5 years (average = 65.9 years; median = 66.6 years). Demographic and clinical characteristics, including age, gender, weight, BMI, smoking status and alcohol consumption are presented in Table 1. BMI ranged from 20.9 to 43.9 kg/m2 (average = 28.5 kg/m2; median = 27.7 kg/m2) and 26.9% of participants (n = 24) had BMI > 30 kg/m2. Forty participants (44.9%) were current or previous smokers (44.9%). Alcohol was consumed by 61 participants (68.5%), with the mean consumption among consumers being 16.4 g/day (median 4.81 g/day). All participants, with the exception of two, completed the food diary. Mean food and nutrient intake are presented in Table 2. The extent and spatial distribution of the participants in the study are shown in Fig. 1.

copyright and database rights 2016. Compiled using QGIS, version 3.2.3
Map of Northern Ireland showing the extent of study area and spatial distribution of study participants (n = 89). Data presented as postcode districts. Numbers inside circles indicate that there is more than one participant per location. Data points which were close together were combined. The map presents OS, Royal Mail and National Statistics data © Crown and Royal Mail
The mean concentrations calculated for iAs, MMA, DMA and AsB in the CRMs were compared with the mean certified values in order to calculate percentage recoveries (Supplementary Material: Table S1). Recoveries of 108.3%, 87.2%, 94.7% and 86.9% resulted for iAs, MMA, DMA and AsB, respectively, for ClinChek® Control (level I). For Seronorm™ trace elements urine (lot 0,511,545), the reference values were expressed in terms of total As only. The recovery of total As was 97.6% and all experimental concentrations were within the acceptable range. The limit of detection (LOD) was for As speciation was 0.0067 μg/L, as estimated from the DMA calibration.
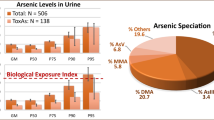
The median concentrations (5–95th percentiles) of iAs, MMA, DMA and AsB were 0.32 (0.08–0.98) µg/L, 0.31 (0.10–0.91) µg/L, 1.90 (0.58–7.35) µg/L and 2.24 (0.13–61.19) µg/L, respectively (Table 3). TMAO was below the detection limit in ~ 70% of samples. No statistical differences were found between the two urine samples collected 6 months apart, in terms of AsB, iAs, MMA, DMA (paired t-test, p > 0.05, data not shown). Therefore, the second collected urine profile of each participant was considered for further analysis. Although women have shown more efficient methylation capacity than men in previous studies (Lindberg et al. 2008; Hudgens et al. 2016; Shen et al. 2016), gender was not a significant predictor of As exposure in the current study.
As a naturally occurring element, the contribution of As exposure sources depends on the levels of As within soil, water and food. Drinking water or food originating from regions with high concentrations of As will result in a higher risk of adverse effects (Chappell et al. 2003; Wu et al. 2018). Results from a detailed geochemistry study conducted by The British Geological Surveys (BGS) indicate that the southern (South Armagh, Portaferry, Strangford and New Castle) and western (County Tyrone) regions of NI have high soil As concentrations (> 10 mg/kg) (GSNI 2007). This geochemistry data has been previously used to investigate potential associations with chronic diseases. The relationship of nephrotoxicant elements (including As) and the prevalence of chronic kidney disease (CKD) was investigated by Jackson et al. (2016). The main association with CKD was found with elevated concentrations of the essential elements zinc and calcium in stream water (Jackson et al. 2016). A potential association has also been observed between incidence of stomach cancer and high levels of As in soils in the South Armagh area of NI (McKinley et al. 2013).
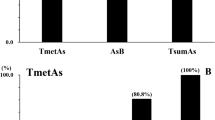
This current investigation of As exposure in NI was performed in a population that was widely distributed throughout the country (Fig. 1). The effect of geographical location was investigated by classifying participants according to their area of residence: Belfast (n = 21), West of Bann (n = 14), South Down and Armagh (n = 11), East Derry and North Antrim (n = 12), South Antrim (n = 18), North Down (n = 13). No differences were observed in terms of log10-transformed urinary concentrations of iAs, DMA or AsB across the various locations. Thus, the NI areas with high concentrations of As in soils were not reflected in terms of iAs exposure in its residents. MMA concentrations were lower in N. Down (log10: − 0.63) and in S. Antrim (log10: − 0.65) compared to Belfast (log10: − 0.38) and the West of the Bann (log10: − 0.35, p < 0.05). A marginal difference (p = 0.055) was observed for the ∑iAs + MMA + DMA, with similar profile to the one observed for MMA (Fig. 2). Since the variation in environmental As occurs at a much finer spatial scale (GSNI 2007) than the geographical distribution presented here, the observation of a geographic effect on As exposure might require a larger sample size. The education level had no effect on As exposure in the investigated population.

Effect of areas of residence in NI on As exposure. Box and whiskers plots of urinary concentration of As species normalized by specific gravity and log10-transformed for the investigated population (n = 89). Boxes range from first and third quartiles with median line. Lower and upper whiskers are minimum and maximum values, except the outliers which are represented as empty circles. One-way ANOVA (p < 0.05) was performed with LSD post hoc analysis. aDifferent from Belfast, bdifferent from E. Derry and N. Antrim, cdifferent from N. Down, ddifferent from S. Antrim
Post-industrialized cities, such as Belfast and Derry, may be expected to have higher environmental pollutant burdens, including As (Shi et al 2012; Strosnider et al. 2017). However, previous reports show higher As levels in rural residents when compared to residents from urban communities (Zailina et al. 2014; Pang et al. 2016; Zhang et al. 2018). In the current study, we found no difference in As exposure between metropolitan versus non-metropolitan areas (Greater Belfast vs. other areas, or Greater Belfast + Greater Derry vs. other areas) (Supplementary Material: Fig. S1). Indeed, the results showed that residing in a city/urban area does not add additional sources of As exposure as assayed through urinary As.
Considering the substantial number of food and nutrient variables, PCA was performed to evaluate the relationships between the dietary variables and to identify the main covariates of As exposure. Due to the different units of measurement (concentration, food/drink/nutrient intake), all variables were standardized to receive the same weight within the PCA. Two factors were generated from the PCA which accounted for 40% of the variability (Fig. 3; Supplementary Material: Table S2). Results from the PCA analysis showed that all As species clustered together, suggesting the variability in urinary concentrations of AsB and that the inorganic species have a common source. The principal component 2 separates As species, with seafood consumption being more strongly related with As species, followed by alcohol consumption. Dairy products and tap water consumption were negatively related to As species, being diametrically opposite to the As species cluster on plots of PCA1 versus PCA2. Most of the nutrients (protein, energy, vitamins B1–3, B5–7, B9, selenium, carbohydrates) were not related to As species, being orthogonal in the PCA plot. Given that food intake was observed to be a better predictor of As exposure, as opposed to nutrient intake, subsequent multiple linear regression analysis were performed using foods as potential covariates (Fig. 3). Nutrients were excluded from the regression analysis to avoid multicollinearity.

Factor loadings for PCA, including arsenic biomarkers (blue), foods (red), drinks (green) and nutrients (black). Due to the different units of measurement of variables, raw data were standardized to receive equal weight in the analysis. To standardize a variable, raw data were subtracted by the mean and then divided by the standard deviation. The concentration of arsenic species in urine was normalized by specific gravity and log-transformed
Multiple regression analysis showed that variation in urinary concentrations of iAs was explained mainly by dairy products (16.0%), alcohol (9.0%) and fortified cereals consumption (4.0%). The total contribution of these covariates explained around 30% of iAs variability. Dairy product consumption showed a negative association with As exposure, suggesting that the higher the intake the lower the iAs concentration in urine. Since the urinary concentrations of iAs species are positively correlated with the urinary flow rate (Middleton et al. 2016), urinary concentrations adjusted for SG were used for PCA or multiple linear regression analysis. All analyses were carried out using both SG-normalized or non-normalized concentrations without changing significantly the results.
DMA is the main metabolite of iAs found in urine and accounts for approximately 60–90% of ∑iAs + MMA + DMA. Therefore, the variables which contributed significantly to the association in the multiple regression analysis were relatively similar for DMA and the ∑iAs + MMA + DMA. Dairy product consumption was the main predictor of DMA and ∑iAs + MMA + DMA, explaining approximately 15% of variation for each. Beside the apparent dilution effect of dairy products, seafood was a significant source of exposure accounting for 7–8%, followed by a dilution effect of tap water which accounted for 6–7% of the total variability (Table 4).
Seafood consumption, including both shellfish, oily fish and white fish, is known to be the main source of AsB (Signes-Pastor et al. 2017a; Jones et al. 2016). AsB in urine comes only from seafood consumption (Popowich et al. 2016) in contrast to DMA which is derived from As metabolism, seafood (Jones et al. 2016) and rice consumption (Punshon et al. 2018). In the present work, seafood was the main predictor of AsB, explaining 16% of the total variation is AsB urinary levels (Table 4). Milk consumption was considered a significant predictor in the current analysis, although it only explained 4.1% of the total variation in AsB concentration. Overall, while milk and seafood consumption together explained 20% of the variation in AsB, the majority of the variation remains unexplained. Although minor, when compared to AsB, seafood consumption was also a significant predictor of DMA, and the ∑iAs + MMA + DMA, explaining approximately 7.5–8% of the total variation. Linear modelling showed that a daily increase of 100 g of seafood was associated with sixfold increase in urinary DMA concentration (Table 4). Other variables such as age, weight, BMI, smoking status or education level were not found to be predictors of iAs, DMA, MMA or AsB.
The effect of alcohol on As exposure is not clear in the literature. Some authors have shown that alcohol consumption does not effect As speciation or As methylation capacities (Hopenhayn-Rich et al. 1996; Tseng et al. 2005; Huang et al. 2008), while others found that the consumption of alcoholic beverages is related to increased levels of iAs in urine (Saoudi et al. 2012; Mori et al. 2016). Wine has been previously reported as source of exposure by the regular use of As as pesticide in vineyards in the past (Saoudi et al. 2012). We found here a positive association between alcohol consumption and urinary iAs (Fig. 3; Table 4). This association suggests inhibition of As primary methylation, since a negative correlation was observed between alcohol consumption and MMA/iAs ratio (Spearman coefficient − 0.280, p value 0.009). The linear modellings showed that an increase of 10 g/day in alcohol was associated with a 9.6% increase in urinary iAs concentration. These findings are consistent with those reported in a systematic review and meta-analysis by Shen et al. (2016) whereby primary methylation of iAs was 0.13-fold lower in alcohol drinkers compared to non-drinkers (Shen et al. 2016). Based on the present findings and on previous data (Hopenhayn-Rich et al. 1996; Tseng et al. 2005; Huang et al. 2008; Saoudi et al. 2012; Mori et al. 2016), we hypothesize that the alcohol effect on As exposure can only be observed when As exposure is relatively low and/or food is a dominant source. Beer consumption was positively associated with increased total As in urine in Japanese adults (Mori et al. 2016). Increased urinary concentrations of iAs + MMA + DMA were associated with higher wine consumption in a French cohort (Saoudi et al. 2012). Considering that similar effects are observed despite the alcoholic beverage (Saoudi et al. 2012; Mori et al. 2016), we suggest that the alcohol regulates As methylation. However, this effect is not observed at higher levels of As exposure (Hopenhayn-Rich et al. 1996; Tseng et al. 2005; Huang et al. 2008).
Drinking water is a relevant source of iAs in areas with high natural levels in public or private water supplies (Chappell et al. 2003; Kordas et al. 2016; Wei et al. 2014; Navoni et al. 2014; Diaz et al. 2015). In the City of Belfast, the concentration of iAs, DMA and TMAO in tap water ranged from 0.039–0.047 μg/L, 0.027–0.031 μg/L and 0.050–0.057 μg/L, respectively (Signes-Pastor et al. 2017b). These levels are very low compared to the parametric value of 10 µg/L for human consumption in the EU (CEU 1998). Tap water consumption showed a moderate negative correlation with urine SG (Pearson correlation coefficient − 0.462, p < 0.001). Moreover, tap water intake showed a dilution effect on urinary As excretion, either adjusting or not the urinary concentrations by SG (Supplementary Material: Fig. S2).
A similar dilution effect on As species excretion was observed for dairy products or milk consumption (Supplementary Material: Fig. S2). The average daily intake of dairy products reaches approximately 250 g (Table 2). Dairy products are generally low in iAs (Jackson et al. 2012; Sugár et al. 2013). As a result, low levels of As species can be expected in NI. In the linear models, an increase in dairy product consumption by 100 g per day was associated with a 26% decrease in iAs urinary concentration (Table 4). However, the dilution effect was not observed for the variable “water from drinks” which included water intake calculated from all drinks consumed including juices, infusions, dairy products and soft drinks. Similarly to tap water, a negative correlation was observed between “water from drinks” with the log-transformed iAs in urine normalized by SG. These findings corroborate the dilution effect of tap water on iAs levels in urine.
Results from the National Health and Nutrition Examination Survey (NHANES) and the US Department of Agriculture’s Food Intakes Converted to Retail Commodities Database (FICRCD) showed that diet accounted for 11.5% of the variation in the ∑iAs + MMA + DMA (Davis et al. 2014). In the current study, diet explained 30% of the variation for the same urine As species. Unlike previous studies where rice-based products were reported to be a major cause of As exposure (Kordas et al. 2016; Wei et al. 2014), this was not evident in NI. Rice is not a food staple in NI (18), and its consumption in the studied population was very low (Table 2). The mean consumption of rice-based products was 20.2 g/day, which is equivalent to 6.0 g of dried grains/day (Table 2). Rice consumption did not show any significant association with urinary As species in the current population.
Despite the lack of a significant association between As exposure and nutrient intake in the current study, As hepatic metabolism has previously been shown to depend on the folate cycle and methionine cycle. The levels of SAM and glutathione, which are required for the serial As methylation and reduction reactions, respectively, are regulated by methionine and folate pathways while vitamin B6 and B12 are cofactors (Kurzius-Spencer et al. 2017). A previously randomized placebo-controlled trial showed that folate supplementation resulted in increased percentage of DMA and reduced percentages of MMA and iAs (Gamble et al. 2006). In NHANES 2003–2004, dietary folate, vitamin B6 and protein intake were correlated to lower percentage iAs and higher percentage DMA, in urine (Kurzius-Spencer et al. 2017). The high consumption of meat was also associated with higher percentage DMA in urine, probably due to the higher sources of protein and methionine, which are SAM precursors (Kordas et al. 2016).
The current study has some limitations in that it is based on a limited cohort of older adults due to the strictures of NICOLA. However, this age restriction of the cohort also has advantages, in that age variability has been removed, an issue that confounds wider population studies, and due to the fact that long-term residency at their geographical location enables a more detailed examination of the influence of geography on As exposure and urinary excretion. The intra-individual variability on As kinetic disposition is likely to be higher in older adults than in young adults, due to the variable age-related reduction in renal and hepatic function, comorbidities and potential drug–As interaction. Ageing is related to physiological reduced hepatic and renal clearance, but also age-related diseases (Hilmer 2008). An older population may be more representative for the assessment of residential area effect compared to younger adults who are more likely to travel or move (Wilding et al. 2018). The present study shows that H2O, alcohol and seafood are important predictors of As levels in urine. It is, however, possible that other variables not evaluated in this work such as genetic polymorphisms related to As toxicokinetics may be important contributors and may increase the predictability of the regression models (Gribble et al. 2015).
References
C.E.U. Council Directive 98/83/EC of November 1998 on the quality of water intended for human consumption. Official Journal European Community, May 12, 1998, pp L330/32–L330/52. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:01998L0083-20151027&from=EN. Accessed 20 May 2019
Chappell WR, Abernathy CO, Calderon RL, Thomas DJ (2003) In: Chappell WR, Abernathy CO, Calderon RL, Thomas DJ (eds) Arsenic exposure and health effects V, 1st edn. Elsevier, Amsterdam, pp 3–103
Davis MA, Gilbert-Diamond D, Karagas MR, Li Z, Moore JH, Williams SM, Frost HR (2014) A dietary-wide association study (DWAS) of environmental metal exposure in US children and adults. PLoS ONE 9:e104768. https://doi.org/10.1371/journal.pone.0104768
Davis MA, Signes-Pastor AJ, Argos M, Slaughter F, Pendergrast C, Punshon T, Gossai A, Ahsan H, Karagas MR (2017) Assessment of human dietary exposure to arsenic through rice. Sci Total Environ 586:1237–1244. https://doi.org/10.1016/j.scitotenv.2017.02.119
Diaz OP, Arcos R, Tapia Y, Pastene R, Velez D, Devesa V, Montoro R, Aguilera V, Becerra M (2015) Estimation of arsenic intake from drinking water and food (raw and cooked) in a rural village of northern Chile. Urine as a biomarker of recent exposure. Int J Environ Res Public Health 12:5614–5633. https://doi.org/10.3390/ijerph120505614
Gamble MV, Liu X, Ahsan H, Pilsner JR, Ilievski V, Slavkovich V, Parvez F, Chen Y, Levy D, Factor-Litvak P, Graziano JH (2006) Folate and arsenic metabolism: a double-blind, placebo-controlled folic acid-supplementation trial in Bangladesh. Am J Clin Nutr 84:1093–1101. https://doi.org/10.1093/ajcn/84.5.1093
Geological Survey Northern Ireland, GSNI (2007) Tellus project overview. https://www.bgs.ac.uk/data/home.html?src=topNav. Accessed on 25 Sep 2018
Gribble MO, Voruganti VS, Cole SA, Haack K, Balakrishnan P, Laston SL, Tellez-Plaza M, Francesconi KA, Goessler W, Thomas DC, Gilliland F, North KE, Franceschini N, Navas-Acien A, (2015) Linkage analysis of urine arsenic species patterns in the strong heart family study. Toxicol Sci 148:89–100. https://doi.org/10.1093/toxsci/kfv164
Harrington KE, McGowan MJ, Kiely M, Robson PJ, Livingstone MB, Morrissey PA, Gibney MJ (2001) Macronutrient intakes and food sources in Irish adults: findings of the North/South Ireland Food Consumption Survey. Public Health Nutr 5A:1051–1060
Hilmer SN (2008) ADME-tox issues for the elderly. Expert Opin Drug Metab Toxicol 4:1321–1331. https://doi.org/10.1517/17425255.4.10.1321
Hopenhayn-Rich C, Biggs ML, Smith AH, Kalman DA, Moore LE (1996) Methylation study of a population environmentally exposed to arsenic in drinking water. Environ Health Perspect 104:620–628. https://doi.org/10.1289/ehp.96104620
Huang YK, Huang YL, Hsueh YM, Yang MH, Wu MM, Chen SY, Hsu LI, Chen CJ (2008) Arsenic exposure, urinary arsenic speciation, and the incidence of urothelial carcinoma: a twelve-year follow-up study. Cancer Causes Control 19:829–839. https://doi.org/10.1007/s10552-008-9146-5
Hudgens EE, Drobna Z, He B, Le XC, Styblo M, Rogers J, Thomas DJ (2016) Biological and behavioral factors modify urinary arsenic metabolic profiles in a U.S. population. Environ Health 15:62. https://doi.org/10.1186/s12940-016-0144-x.
IARC (2004) Monographs on the evaluation of carcinogenic risk to humans. Some drinking-water disinfectants and contaminants, including arsenic, vol 84. World Health Organization, Lyon
IARC (2012) Arsenic, metals, fibres and dust. Volume 100C. A review of human carcinogens. IARC monographs on the evaluation of carcinogenic risk to humans. World Health Organization, Lyon
Jackson BP, Taylor VF, Punshon T, Cottingham KL (2012) Arsenic concentration and speciation in infant formulas and first foods. Pure Appl Chem 84:215–223. https://doi.org/10.1351/PAC-CON-11-09-17
Jackson CE, McKinley JM, Ofterdinger U, Fogarty D, Atkinson PM, Palmer S (2016) Investigating relations between environmental toxins in Northern Irish soils and streams and Chronic Kidney Disease prevalence. Appl Geochem 75:236–246. https://doi.org/10.1016/j.apgeochem.2016.10.016
Jones MR, Tellez-Plaza M, Vaidya D, Grau M, Francesconi KA, Goessler W, Guallar E, Post WS, Kaufman JD, Navas-Acien A (2016) Estimation of inorganic arsenic exposure in populations with frequent seafood intake: evidence from MESA and NHANES. Am J Epidemiol 184:590–602. https://doi.org/10.1093/aje/kww097
Kordas K, Queirolo EI, Mañay N, Peregalli F, Hsiao PY, Lu Y, Vahter M (2016) Low-level arsenic exposure: nutritional and dietary predictors in first-grade Uruguayan children. Environ Res 147:16–23. https://doi.org/10.1016/j.envres.2016.01.022
Kurzius-Spencer M, da Silva V, Thomson CA, Hartz V, Hsu CH, Burgess JL, O’Rourke MK, Harris RB (2017) Nutrients in one-carbon metabolism and urinary arsenic methylation in the National Health and Nutrition Examination Survey (NHANES) 2003–2004. Sci Total Environ 607–608:381–390. https://doi.org/10.1016/j.scitotenv.2017.07.019
Lindberg AL, Ekström EC, Nermell B, Rahman M, Lönnerdal B, Persson LA, Vahter M (2008) Gender and age differences in the metabolism of inorganic arsenic in a highly exposed population in Bangladesh. Environ Res 106:110–120. https://doi.org/10.1016/j.envres.2007.08.011
McKinley JM, Ofterdinger U, Young M, Barsby A, Gavin A (2013) Investigating local relationships between trace elements in soils and cancer data. Spat Stat 5:25–41. https://doi.org/10.1016/j.spasta.2013.05.001
Meharg AA, Raab A (2010) Getting to the bottom of arsenic standards and guidelines. Environ Sci Technol 44:4395–4399. https://doi.org/10.1021/es9034304
Middleton DR, Watts MJ, Lark RM, Milne CJ, Polya DA (2016) Assessing urinary flow rate, creatinine, osmolality and other hydration adjustment methods for urinary biomonitoring using NHANES arsenic, iodine, lead and cadmium data. Environ Health 15:68. https://doi.org/10.1186/s12940-016-0152-x
Mori M, Sato T, Yoshida HY, Ohira Y, Itou Y, Shimizu S (2016) Association of beer consumption with arsenic concentration in urine: a result from a cross-sectional study of the general Japanese population. Environ Health Prev Med 21:327–333. https://doi.org/10.1007/s12199-016-0533-3
Navas-Acien A, Francesconi KA, Silbergeld EK, Guallar E (2011) Seafood intake and urine concentrations of total arsenic, dimethylarsinate and arsenobetaine in the US population. Environ Res 111:110–118. https://doi.org/10.1016/j.envres.2010.10.009
Navoni JA, De Pietri D, Olmos V, Gimenez C, Bovi Mitre G, de Titto E, Villaamil Lepori EC (2014) Human health risk assessment with spatial analysis: study of a population chronically exposed to arsenic through drinking water from Argentina. Sci Total Environ 499:166–174. https://doi.org/10.1016/j.scitotenv.2014.08.058
Neville CE, Cruise SM, Burns F (2019) The Northern Ireland Cohort for the Longitudinal Study of Ageing (NICOLA). In: Encyclopedia of gerontology and geriatrics. Springer, Cham. https://doi.org/10.1007/978-3-319-69892-2_346-1
Nutritics (2018) Research Edition (v5.02) (computer software). Nutritics, Dublin. www.nutritics.com. Accessed 4 Feb 2019
Ouypornkochagorn S, Feldmann J (2010) Dermal uptake of arsenic through human skin depends strongly on its speciation. Environ Sci Technol 44:3972–3978. https://doi.org/10.1021/es903667y
Pang Y, Peng RD, Jones MR, Francesconi KA, Goessler W, Howard BV, Umans JG, Best LG, Guallar E, Post WS, Kaufman JD, Vaidya D, Navas-Acien A (2016) Metal mixtures in urban and rural populations in the US: the Multi-Ethnic Study of Atherosclerosis and the Strong Heart Study. Environ Res 147:356–364. https://doi.org/10.1016/j.envres.2016.02.032
Popowich A, Zhang Q, Le XC (2016) Arsenobetaine: the ongoing mystery. Natl Sci Rev 3:451–458. https://doi.org/10.1093/nsr/nww061
Punshon T, Carey AM, Ricachenevsky FK, Meharg AA (2018) Elemental distribution in developing rice grains and the effect of flag-leaf arsenate exposure. Environ Exp Bot 149:51–58. https://doi.org/10.1016/j.envexpbot.2018.02.007
Saoudi A, Zeghnoun A, Bidondo ML, Garnier R, Cirimele V, Persoons R, Fréry N (2012) Urinary arsenic levels in the French adult population: the French National Nutrition and Health Study, 2006–2007. Sci Total Environ 433:206–215. https://doi.org/10.1016/j.scitotenv.2012.06.053
Shen H, Niu Q, Xu M, Rui D, Xu S, Feng G, Ding Y, Li S, Jing M (2016) Factors affecting arsenic methylation in arsenic-exposed humans: a systematic review and meta-analysis. Int J Environ Res Public Health 13:205. https://doi.org/10.3390/ijerph13020205
Shi G, Chen Z, Teng J, Bi C, Zhou D, Sun C, Li Y, Xu S (2012) Fluxes, variability and sources of cadmium, lead, arsenic and mercury in dry atmospheric depositions in urban, suburban and rural areas. Environ Res 113:28–32. https://doi.org/10.1016/j.envres.2012.01.001
Signes-Pastor AJ, Carey M, Vioque J, Navarrete-Muñoz EM, Rodríguez-Dehli C, Tardón A, Begoña-Zubero M, Santa-Marina L, Vrijheid M, Casas M, Llop S, Gonzalez-Palacios S, Meharg AA (2017a) Urinary arsenic speciation in children and pregnant women from Spain. Expo Health 9:105–111. https://doi.org/10.1007/s12403-016-0225-7
Signes-Pastor AJ, Vioque J, Navarrete-Muñoz EM, Carey M, García de la Hera MG, Sunyer J, Casas M, Riaño-Galán I, Tardón A, Llop S, Amorós R, Amiano P, Bilbao JR, Karagas MR, Meharg AA (2017b) Concentrations of urinary arsenic species in relation to rice and seafood consumption among children living in Spain. Environ Res 159:69–75. https://doi.org/10.1016/j.envres.2017.07.046
Signes-Pastor AJ, Woodside JV, McMullan P, Mullan K, Carey M, Karagas MR, Meharg AA (2017c) Levels of infants’ urinary arsenic metabolites related to formula feeding and weaning with rice products exceeding the EU inorganic arsenic standard. PLoS ONE 12:e0176923. https://doi.org/10.1371/journal.pone.0176923
Strosnider H, Kennedy C, Monti M, Yip F (2017) Rural and urban differences in air quality, 2008–2012, and community drinking water quality, 2010–2015: United States. MMWR Surveill Summ 66:1–10. https://doi.org/10.15585/mmwr.ss6613a1
Subhani M, Mustafa I, Alamdar A, Katsoyiannis IA, Ali N, Huang Q, Peng S, Shen H, Eqani SA (2015) Arsenic levels from different land-use settings in Pakistan: bio-accumulation and estimation of potential human health risk via dust exposure. Ecotoxicol Environ Saf 115:187–194. https://doi.org/10.1016/j.ecoenv.2015.02.019
Sugár E, Tatár E, Záray G, Mihucz VG (2013) Relationship between arsenic content of food and water applied for food processing. Food Chem Toxicol 62:601–608. https://doi.org/10.1016/j.fct.2013.09.028
Tseng CH, Huang YK, Huang YL, Chung CJ, Yang MH, Chen CJ, Hsueh YM (2005) Arsenic exposure, urinary arsenic speciation, and peripheral vascular disease in blackfoot disease-hyperendemic villages in Taiwan. Toxicol Appl Pharmacol 206:299–308. https://doi.org/10.1016/j.taap.2004.11.022
Wardrop NA, Le Blond JS (2015) Assessing correlations between geological hazards and health outcomes: addressing complexity in medical geology. Environ Int 84:90–93. https://doi.org/10.1016/j.envint.2015.07.016
Wei Y, Zhu J, Nguyen A (2014) Rice consumption and urinary concentrations of arsenic in US adults. Int J Environ Health Res 24:459–470. https://doi.org/10.1080/09603123.2013.857393
WHO (2001) Environmental Health Criteria 224—arsenic and arsenic compounds. International Program on Chemical Safety, Geneva
Wilding S, Martin D, Moon G (2018) Place and preference effects on the association between mental health and internal migration within Great Britain. Health Place 52:180–187. https://doi.org/10.1016/j.healthplace.2018.06.008
Williams PN, Islam MR, Adomako EE, Raab A, Hossain SA, Zhu YG, Feldmann J, Meharg AA (2006) Increase in rice grain arsenic for regions of Bangladesh irrigating paddies with elevated arsenic in groundwaters. Environ Sci Technol 40:4903–4908. https://doi.org/10.1021/es060222i
Wu F, Chi L, Ru H, Parvez F, Slavkovich V, Eunus M, Ahmed A, Islam T, Rakibuz-Zaman M, Hasan R, Sarwar G, Graziano JH, Ahsan H, Lu K, Chen Y (2018) Arsenic exposure from drinking water and urinary metabolomics: associations and long-term reproducibility in Bangladesh adults. Environ Health Perspect 126:017005. https://doi.org/10.1289/EHP1992
Xu S, Zheng N, Liu J, Wang Y, Chang S (2013) Geochemistry and health risk assessment of arsenic exposure to street dust in the zinc smelting district, Northeast China. Environ Geochem Health 35:89–99. https://doi.org/10.1007/s10653-012-9463-1
Zailina H, Najibah H, Aiezzati AN, Praveena SM, Patimah I (2014) Comparison of the health implications on the use of As and Cd contaminated water supply between urban and rural communities. Biomed Res Int 2014:797603. https://doi.org/10.1155/2014/797603
Zhang X, Wang B, Cui X, Lin C, Liu X, Ma J (2018) Total arsenic concentrations in Chinese children’s urine by different geographic locations, ages, and genders. Environ Geochem Health 40:1027–1036. https://doi.org/10.1007/s10653-017-9963-0
Acknowledgements
We are grateful to all the participants of the NICOLA, and the whole NICOLA Team, which includes nursing staff, research scientists, clerical staff, computer and laboratory technicians, managers and receptionists. The Atlantic Philanthropies, the Economic and Social Research Council, the UKCRC Centre of Excellence for Public Health Northern Ireland, the Centre for Ageing Research and Development in Ireland, the Office of the First Minister and Deputy First Minister, the Health and Social Care Research and Development Division of the Public Health Agency, the Wellcome Trust/Wolfson Foundation and Queen’s University Belfast provide core financial support for NICOLA. The authors alone are responsible for the interpretation of the data and any views or opinions presented are solely those of the authors and do not necessarily represent those of the NICOLA Study Team.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
de Moraes, N.V., Carey, M., Neville, C.E. et al. Water Dilutes and Alcohol Concentrates Urinary Arsenic Species When Food is the Dominant Source of Exposure. Expo Health 12, 699–710 (2020). https://doi.org/10.1007/s12403-019-00329-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-019-00329-5