
Abstract
The risk of urothelial carcinoma (UC) and urinary arsenic speciation have been evaluated in a few case–control studies; however, the association has not been verified in a prospective cohort study. The aim of this study was to examine the association between urinary arsenic speciation and the incidence of UC in a cohort study. A total of 1,078 residents of southwestern Taiwan were followed for an average of 12 years. A high-performance liquid chromatography/hydride generator and an atomic absorption spectrometry were used to measure urinary arsenite, arsenate, monomethylarsonic acid (MMAV), and dimethylarsinic acid (DMAV). The incidence of UC was estimated by examining the National Cancer Registry of Taiwan between January 1985 and December 2001. There were 37 newly diagnosed cases of UC during a follow-up period of 11,655 person-years. Significantly higher percentages of MMAV and lower percentages of DMAV existed among the patients with UC than among the healthy residents. After adjustment for age, gender, educational level, and smoking status, the percentage of urinary DMAV was shown to have an inverse association with the risk of UC, having a relative risk (RR) of the tertile strata of 1.0, 0.3, and 0.3, respectively (p < 0.05 for the trend test). The RR (95% confidence interval) of residents with a cumulative arsenic exposure (CAE) of ≥20 mg/l-year and a higher percentage of MMAV or a CAE of ≥20 mg/l-year and a lower percentage of DMAV was 3.7 (1.2–11.6) or 4.2 (1.3–13.4) compared to residents with a CAE of <20 mg/l-year and a lower percentage of MMAV or a CAE of <20 mg/l-year and a higher percentage of DMAV respectively. There was a significant association between inefficient arsenic methylation and the development of UC in the residents in the high CAE exposure strata in an area of southwestern Taiwan endemic for arseniasis.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Arsenic is widely distributed in nature and present in the environment mainly in the water. Inorganic arsenic (InAs) is a human bladder carcinogen [1]. Populations in southwestern Taiwan are known to have been exposed to arsenic via drinking water at levels >500 μg/l. There is accumulating evidence of an arsenic-related risk of cancer, especially involving the bladder, in the area of southwestern Taiwan with elevated arsenic levels and exposure [2–4]. Another evidence that inorganic arsenic ingested from drinking water is related to the incidence of urinary tract cancer has appeared [5, 6]. Studies from Chile and Argentina have also shown that urinary bladder cancer is associated with long-term arsenic exposure from drinking water [7–9]. All studies have relied, to one extent or another, on measurements of arsenic in water, and some also use questionnaire data.
The liver is the main organ that metabolizes inorganic arsenic. After ingestion of InAs, arsenate (AsV) is readily reduced to arsenite (AsIII) in the red blood cells [10, 11] and subsequently methylated to monomethylarsonic acid (MMAV) and dimethylarsinic acid (DMAV) in the liver [12, 13]. Approximately 60∼90% of the ingested arsenic is excreted in the urine when a mammal is exposed to a single dose of inorganic arsenic, and DMAV is the endpoint product in humans; in general, 10∼30% of InAs, 10∼20% of MMAV, and 60∼80% of DMAV are excreted in the urine, but the arsenic metabolic profile varies among different animal species [14]. Evaluation of the efficiency of arsenic methylation is mainly based on the relative amounts of the different metabolites in the urine. MMAV is less toxic than InAs, but the transient metabolic intermediate of MMAIII and DMAIII has a more toxic activity than InAs in various human cell lines [15], as well as in hamsters [16]. Further proof of MMAIII induced DNA damage mediated by reactive oxygen species was demonstrated in vitro study [17].
Previous epidemiologic evidence has suggested that patients with skin and bladder cancer have a higher percentage of InAs (%InAsV) and MMAV (%MMAV), and a lower percentage of DMAV (%DMAV) and lower primary methylation indices (PMI) than do healthy controls [18–21]. The relationship between urinary arsenic species and cancer risk has been shown in populations exposed to an extremely high dose of arsenic in those studies. A recent report has shown that inefficient arsenic methylation profiles are associated with the risk of UC in a Taiwan population exposed to arsenic at the legal limit in their water sources [22]. Similarly, in Argentina and the United States, individuals with a higher urinary %MMAV were more susceptible to arsenic-related cancer [23]. Case–control studies presented the prevalence of cancer cases which was insufficient to prove a casual relationship between urinary arsenic profiles and bladder cancer. A prospective follow-up study is therefore needed to further investigate that putative causal relationship.
A tap water supply system was installed in the endemic area of Taiwan in which blackfoot disease (BFD), a unique peripheral artery disease related to chronic arsenicalism in southwestern Taiwan since the early 1960s, but usage of the tap water supply system remained low until the early 1970s. Artesian well water was no longer used for drinking and cooking after the mid-1970s. The residents in that area had used artesian well water for more than 30 years when they were recruited to participate in the current study, and the duration of arsenic exposure may have been long enough to induce cancer. However, urinary arsenic profiles remain fairly stable over time [24], and the urinary arsenic species marker is a good index to predict the risk of arsenic-related disease [25, 26]. This is the first cohort study to document the relationship between the urinary arsenic profile and the incidence of urothelial carcinoma (UC) in the area of southwestern Taiwan endemic for arseniasis.
Materials and methods
The study area and the study cohort
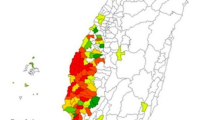
The study area included Homei, Fuhsing, and Hsinming villages in the Putai township of Chiayi County, Taiwan. Residents in this study area have the greatest prevalence of BFD in Taiwan, with a prevalence as high as 13.6% in Homei, 9.6% in Fuhsin, and 10.3% in Hsinming [27]. The method of recruitment of subjects from these areas has been reported in a previous study [28]. In brief, 2,258 residents >30 years of age were registered in the household records of the local household registration office in their respective villages. A total of 1,571 residents that lived at least 5 days per week in the study villages were eligible for participation in the study. One thousand eighty-one residents, including 468 males and 613 females, provided informed consents and thus became the study cohort. A home interview with each participant was conducted between September 1988 and June 1989. The participants were also invited, on a voluntary basis, to undergo a health examination, including a urine sample, in January and February 1989. Participants who had UC prior to January 1989 were excluded from the study and a final study cohort of 1,078 participants was followed for an average of 12 years. The Institutional Review Board of National Taiwan University approved this study.
Identification of urothelial carcinoma cases
Each participant’s unique national identification number was used to link to the computerized National Cancer Registry profiles in Taiwan for the purpose of identifying newly diagnosed cases of UC between 1 January 1989 and 31 December 2001. The National Cancer Registry system was implemented in 1978 in Taiwan and is considered to be a nationwide cancer registry system with updated, accurate, and complete information [29]. Taiwan’s cancer registry system also provides histologic data and only histologically confirmed cases of incident UC were included in the current study (ICD-9 codes 188 and 189) [30]. Twenty-two residents were identified as having a malignant neoplasm of the bladder (ICD-9 code 188), 18 residents had a malignant neoplasm of the kidney and other unspecified urinary organs (ICD-9 code 189), including the renal pelvis (ICD-9 code 189.1), the ureter (ICD-9 code 189.2), the urethra (ICD-9 code 189.3), a urinary organ of unspecified site (ICD-9 code 189.9), and 110 participants had non-urinary organ cancer. According to the International Classification of Diseases for Oncology, Third Edition, the histology of the malignant neoplasm of the bladder (21 of 22 cases) and malignant neoplasm of the kidney and other unspecified urinary organs (16 of 18 cases) was urothelial (transitional cell) carcinoma (TCC; ICD-O-3 M-codes 8120/3 and 8230/3) [31). No tissue specimens were identified as renal cell carcinoma (ICD-O-3 M-codes 8312/3 and 8260/3) in this study. Overall, 37 cases of UC and 928 cancer-free residents were analyzed in the present study.
Determination of urinary arsenic species
During the first health examination in 1989, overnight urine samples were collected from 19:00 to the first voiding the next morning. Urine samples were stored at −20°C without any additives and were retrieved for determination of the urinary arsenic species within 6 months of collection.
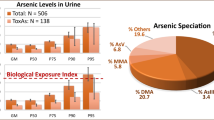
Urine was thawed at room temperature, ultrasonically mixed, and filtered through a Sep-Pak C18 column (500 mg 40 μm APD, 60 Å; JT Baker, Phillipsburg, NJ, USA). Analytical methods for AsIII, AsV, MMAV, and DMAV determinations have been reported in our previous study [32]; at the time that study was conducted, only 302 urine samples from subjects were analyzed due to budget constraints, but all of the remaining urine samples had been analyzed sequentially. The standard reference material, SRM 2670, containing 480 ± 100 μg/l of total arsenic was obtained from the National Institute of Standards and Technology (NIST; Gaithersburg, MD, USA). SRM 2670 was used as an internal standard and analyzed along with the urine samples. The mean arsenic value of SRM 2670 determined by our system was 507 ± 17 (SD) μg/l (n = 4). Recovery of AsIII, DMAV, MMAV, and AsV in each assay, ranged between 93.8 and 102.2%, with detection limits of 0.24, 0.05, 0.11, and 0.12 μg/l, respectively. The coefficient of variation was used to test the reliability and was <5% for all experiments.
The arsenic methylation indices were the percentages of respective urinary arsenic species (AsIII, AsV, MMAV, and DMAV) present in the total arsenic content, which was the sum of AsIII, AsV, MMAV, and DMAV. The PMI was defined as the ratio between MMAV and InAs (AsIII + AsV) levels, and the secondary methylation index (SMI) was defined as the ratio between DMAV and MMAV. The percentages of urinary arsenic species or the arsenic methylation index were internal dose indices of arsenic exposure in this study.
Questionnaire interview and determination of arsenic exposure
Two public health nurses carried out the standardized personal interviews between September 1988 and June 1989 based on a structured questionnaire. Information obtained from the interview included a history of high-arsenic artesian well water consumption, residential history, socioeconomic and demographic characteristics, lifestyle factors, such as alcohol consumption and cigarette smoking, as well as personal and family histories of hypertension, diabetes, and cardiovascular diseases.
Some subjects moved from one village to another and the arsenic concentration in the artesian well water of these villages was known to differ. As both the duration of exposure and arsenic level in the artesian well water may be associated with the incidence of UC, an index of cumulative arsenic exposure (CAE) was derived to reflect the overall exposure to arsenic for each subject. The detailed residential history and duration of consuming high-arsenic artesian well water were used to derive the CAE for each study subject. The CAE, expressed in milligrams per liter-years was defined as the sum of the products, which were derived by multiplying the arsenic concentration in well water (mg/l) by the duration of water consumption (years) during consecutive periods of living in different villages. The arsenic levels in artesian well water of villages where subjects had lived were obtained from previous reports carried out in the 1960s. These water samples were collected from 155 wells located in the 42 villages in the geographic areas in which BFD is endemic [33]. The arsenic level in the artesian well water in the study area has been reported to be stable in two surveys carried out by the Taiwan Provincial Institute of Environmental Sanitation [34]. The CAE index (mg/l-year) for a given subject was defined by the following formula: Σ (Ci × Di), where Ci is the median arsenic concentration of artesian well water (mg/l) in the village where the subject lived and Di is the duration in years of consumption of artesian well water while residing in the village. The average arsenic concentration in drinking water was calculated by the following formula: Σ (Ci × Di)/ΣDi. Some subjects moved into the study villages after they had lived in other areas for several years, while some others moved away for study or work for several years and returned to the study area. Because the arsenic concentration in drinking water was not available in other areas, the CAE and average arsenic concentration for a given subject was considered to be unknown if the median arsenic concentration of the artesian well water in any villages where the subject had lived during his or her lifetime was not available. The CAE and average arsenic concentration could not be calculated with precision for 254 study subjects (26.3 %) in this study. The arsenic exposure indices calculated from the questionnaire interview were used as external dose indices of arsenic exposure.
Statistical analyses
We used an indirect adjustment method to estimate the standardized incidence ratios (SIRs) [35]. This method incorporates age- and gender-specific UC incidence rates in Taiwan from 1989 to 2001 as the reference values. The expected incidence of a given cancer was calculated by summing the products of the age- and gender-specific incidence rates of cancer in the reference population and the age- and gender-specific person-years under observation in this study cohort [∑(incidence × person-years)]. The SIR was derived by dividing the observed number of incident cases by the expected number of incident cases.
The Wilcoxon Mann Whitney U test was used to analyze the differences in indices of urinary arsenic between older and younger subjects, males and females, highly educated and less educated subjects, smokers and non-smokers, alcohol consumers and non-consumers, and cases of UC and non-UC because they were not normally distributed. For comparing urinary arsenic indices among three or more groups, the urinary arsenic indices were ranked and analyzed by analysis of variance (ANOVA) followed by Scheffe’s post hoc test. Cut points for urinary arsenic indices were the median or tertiles of those indices in healthy residents separated into two or three strata, respectively. The person-years of follow-up were computed from 1 January 1989 to the date UC was diagnosed or the end of the follow-up period (31 December 2001). Cox proportional hazards models were used to evaluate associations between risk factors and the incidence of UC; the relative risks and the 95% confidence intervals (CI) were calculated by adjusting for potential confounders. The analyses were done using SAS, version 8.2.
Results
The standardized incidence ratio for UC in the area of southwestern Taiwan with increased arseniasis compared to the general population between 1989 and 2001 was 1.8 (95% CI, 1.4–2.5; p < 0.01) in this study (data not shown). The person-years and relative risk of UC, stratified by gender, educational level, cigarette smoking, alcohol consumption, and age at enrollment are shown in Table 1. The cases of UC and healthy residents were followed for 257 and 11,398 person-years, and the average follow-up periods were 6.9 and 12.28 years, respectively. An older age at enrollment was associated with an increased risk of UC.
The associations between the chronic arsenic exposure indices and the relative risk of UC are shown in Table 2. The risk of UC was significantly associated with the duration of high-arsenic artesian well water consumption and CAE after adjustment for age, gender, educational level, and cigarette smoking. However, data representing 26.3% of the subjects were unavailable for the CAE or average concentration of arsenic in the artesian well water consumption, thus their relative risk of UC was between the lowest and highest arsenic exposure levels. Unavailability of chronic arsenic exposure data for these subjects did not affect the assessment of the association between arsenic exposure and the incidence of UC, and they were excluded in the dose-response analysis.
The distribution of the urinary arsenic profile among subgroups of age, gender, educational level, cigarette smoking, alcohol consumption, chronic arsenic exposure indices, and cases of UC and controls are shown in Table 3. A higher total urinary arsenic level was observed for males compared with females, cigarette smokers compared with non-smokers, and alcohol consumers compared with non-alcohol consumers. Females or non-smokers had a lower %InAs than males or smokers. Participants with a CAE ≥ 20 mg/l-year had a lower %InAs than participants with a CAE between 1 and 20 mg/l-year. The elderly (≥ 50 years old), males, cigarette smokers, and cases of UC had a significantly higher %MMAV, a lower %DMAV, and a lower SMI than the younger (<50 years old), females, non-smokers, and healthy subjects. These results suggest that the elderly, males, cigarette smokers, or cases of UC had an inefficient methylation capacity by which to metabolize arsenic to DMAV.
Two models were used to estimate the association between arsenic methylation indices and the risk of UC (Table 4). The age, gender, educational level, and cigarette smoking status were adjusted in Model I. In addition to the risk factors of Model I, the CAE was included in Model II to adjust the long-term arsenic exposure among individuals. A high %DMAV decreased the risk of UC and demonstrated a reverse dose-response relationship between the %DMAV and the risk of UC (p trend = 0.01 in Model I and p trend = 0.01 in Model II). Arsenic methylation is a serial process; the %MMAV and %DMAV or the PMI and SMI may represent the activity of the first and second methylation phases.
Table 5 shows the effect of the urinary arsenic profile on the incidence of UC in participants with a low or high CAE. Participants with a high %MMAV or a high PMI had a significantly elevated risk of UC and those with a high % DMAV or a high SMI had a significantly decreased risk of UC when they were exposed to a high CAE (≥ 20 mg/l-year). There was no association between arsenic methylation profiles and the risk of UC when participants were exposed to a low CAE (<20 mg/l-year). These findings suggest that subjects with a low arsenic methylation capacity had an increased risk of UC when they were exposed to a high CAE. Cigarette smoking is an important risk factor for UC; we therefore compared the relative risk of UC among the arsenic methylation profile groups in smokers and non-smokers and the findings are presented in Table 6. Cigarette smoking status did not modify the arsenic methylation capacity on the risk of developing UC. The results in Tables 5 and 6 suggest the modification of the CAE was greater than cigarette smoking status on arsenic methylation profiles for risk of UC.
Discussion
Our previous studies have shown that ingestion of InAs is related to the development of cancers in areas of southwestern Taiwan which are hyperendemic for arseniasis [2, 3]. In this study area, residents began drinking artesian well water in the 1910s; a tap water system was first introduced in the 1960s and not completed until the mid-1970s. Nearly one-half of the residents are long-term consumers (>20 years) of high-arsenic artesian well water, with an average arsenic concentration of 500 μg/l or greater. Urine samples obtained from subjects in this study were collected in 1989, about 20–30 years after drinking artesian well water ceased. Thus, the population in this study was appropriate for investigating the putative association between arsenic exposure and risk of cancer. Only a minority of the population with exposure to arsenic was diagnosed with UC and this implied that individual susceptibility to the metabolism and detoxification of the ingested InAs might be central to the development of UC. Our study suggested that the risk of UC is not only related to the dosage exposure of arsenic, but also to the methylation profiles of arsenic. Subjects with inefficient arsenic metabolism (i.e., methylation of InAs to %DMAV) were shown to have a significantly increased risk for UC.
Evaluation of exposure to arsenic in drinking water is often based on the measurement of arsenic levels or a combination of information pertaining to the duration and amount of water consumed, or even biomarkers, such as urinary arsenic. The median arsenic concentration of artesian well water was used herein to calculate the CAE, which may not reflect an individual’s arsenic exposure. The CAE was combined with urinary arsenic methylation profiles to estimate the internal exposure. These profiles are good markers reflecting the metabolism of InAs ingested from drinking water [25, 26]. The study showed that urinary arsenic methylation indices were fairly stable for 8–10 months for subjects who drank water with a 20 μg/l arsenic level [36]. Subjects that discontinued drinking high arsenic-containing water and changed to consuming low-level arsenic-containing water sequentially had a decreased urinary %MMAV and an increased %DMAV [37]. The urinary %InAs, %MMAV, and %DMAV were 20, 16, and 63, respectively, in Taiwanese subjects who had no evidence of arsenic exposure (i.e., <50 μg/l) [38]. In an arsenic-affected population of northern Argentinians who were exposed to arsenic from drinking water, the urinary %InAs, %MMAV, and %DMAV were 25–49, 2–4, and 54–74, respectively [39]. In contrast, the urinary %InAs, %MMAV, and %DMAV were 7–10, 20–23, and 67–73% in the residents of the BFD endemic areas, who had ceased drinking artesian well water for 2 to 3 decades [32]. Native women from the Andes exposed to arsenic from drinking water excreted lower levels of MMAV (2.3–3.5%) in urine [40]. The large inter-individual variability in arsenic methylation ability may be due to the polymorphism of an arsenic methylation-related gene. Our previous study showed that glutathione S-transferase M1 and T1 were related to the urinary arsenic methylation profile [41]. Recent studies have also shown that polymorphism of MMAV reductase or arsenic methyltransferase are related to urinary arsenic methylation profiles [42–44]. Therefore, a substantial inter-individual variation in arsenic metabolism was found in different ethnicities, which might indicate a genetic role in the regulation of enzymes involved in the metabolism of arsenic.
The biotransformation of arsenic in humans ingesting arsenic-containing water is an important factor related to several diseases. The urinary arsenic species can provide useful insight into the arsenic methylation capacity in different animal species and humans [45]. Case–control studies in Taiwan, Argentina, and the United States have shown that higher urinary %MMAV is related to the risk of bladder cancer [18, 23]. These studies have reported that an association between urinary arsenic species and human diseases may not be causally related. Therefore, the observations might not distinguish between the impact of methylation patterns on disease and the impact of disease or disease treatment on the methylation patterns. We collected urinary samples and measured the urinary methylation pattern before the diagnoses of cancer were made to attempt to establish the relationship between the arsenic methylation pattern and the development of UC. We found that inefficient urinary arsenic methylation profiles, high %MMAV, or low %DMAV increased the incidence of UC in residents who ceased ingesting arsenic-enriched well water for >30 years.
A renewed interest in urinary metabolites has followed the identification of two novel arsenic species, MMAIII and DMAIII [15, 46, 47], which are thought to be toxic intermediates in the biotransformation of ingested InAs. It is expected that the major genotoxic and transforming agents of the uroepithelium are the trivalent metabolites of methyl-arsenical [48]. In the arsenic methylation process, MMAV must be reduced to MMAIII and methylated to DMAV. The possibility cannot be excluded that the higher MMAV in the urine is a reflection of higher MMAIII in the blood or inside the cells, where the injuries are incurred by arsenic. We also found that a high %MMAV was associated with a significantly elevated risk of UC in those subjects with a CAE ≥20 mg/l-year. It is speculated that MMAIII is a more relevant carcinogenic metabolite and urinary trivalent methylated arsenicals are dependent on a very high cumulative arsenic exposure. However, MMAIII and DMAIII are unstable and rapidly oxidize to MMAV and DMAV, respectively [49]. The detection of the transient metabolites of MMAIII and DMAIII depends on the conditions of sample storage and the concentrations in the urine, which were beyond the analytical detection at the time of this study in 1989. The levels of trivalent methylated metabolites in the urine are expected to be very low since these metabolites have short half-lives and are therefore considered not to be suitable markers for arsenic methylation at the present time [45, 50]. Urinary trivalent arsenic methylated metabolites reflect the impact on health and their measurement requires a reliable and valid method [45]. Therefore, it is difficult to use those markers to explore associations with disease. However, further investigations focusing on the associations between these highly toxic arsenic metabolic intermediates and clinical diseases are potentially meaningful.
DMAIII is rarely detected in human body fluids, but a study has provided urinary DMAIII measurements from a population exposed to high dose arsenic in drinking water [51]; however, the analytical procedure may have been flawed because 6 M hydrochloric acid was added to the reaction tube containing the urine sample, resulting in the chemical reduction of DMAV to DMAIII. Urinary DMAV is rarely oxidized from DMAIII; the majority is generated from the methylation process of arsenic. Subjects who had consumed high-arsenic artesian well water for >30 years and had high %DMAV were conferred protection from UC. Therefore, we have deduced the hypothesis that subjects with a higher %DMA have a more efficient methylation capability. The %DMAV may be influenced by seaweed intake because the arsenosugars present in the seaweed are metabolized to DMAV and excreted in the urine [52]. The data for seaweed ingestion was not available in the questionnaire in this study. However, our previous study demonstrated that the frequency of seaweed ingestion was not related to urinary DMAV [38], and this result seems contradictory to the observation from Japanese volunteers after consumption of seaweed [53]. Any variation of seaweed intake might be biased in the identification of urinary %DMAV in both cases of UC and healthy residents causing a non-differential misclassification and displacement of the relative risk toward the null.
The current study had some limitations. The relative risks should be interpreted cautiously due to the low incidence of cases of UC, resulting in inadequate statistical power. The arsenic methylation profiles were found to be constant over time, reflecting a uniform exposure via drinking water [54]. Reports about whether the arsenic methylation profile has or does not have long-term consistency are lacking. Indeed, the long-term consistency of methylation profiles is an important assumption in this article, and repeat measurements will be needed in future investigations. Nevertheless, the current study population had discontinued the consumption of high-arsenic artesian well water and a burden effect of chronic arsenic exposure must be considered. If urinary arsenic species levels decreased with time, any dilution effect would have biased our results toward the null.
This is the first perspective cohort study to evaluate the relationship between arsenic methylation patterns and the development of UC in subjects who had ever-exposure to high-level arsenic from drinking water. In summary, there was a significant association between the urinary arsenic speciation and the development of UC in high CAE exposure strata among residents in an area of southwestern Taiwan endemic for arseniasis.
Abbreviations
- UC:
-
Urothelial carcinoma
- % DMAV :
-
Percentage of DMAV
- %InAsV :
-
Percentage of InAs
- %MMAV :
-
Percentage of MMAV
- AsIII :
-
Arsenite
- AsV :
-
Arsenate
- InAs:
-
Inorganic arsenic
- BFD:
-
Blackfoot disease
- CAE:
-
Cumulative arsenic exposure
- DMAV :
-
Dimethylarsinic acid
- InAs:
-
Inorganic arsenic
- MMAV :
-
Monomethylarsonic acid
- PMI:
-
Primary methylation indices
- SIRs:
-
Standardized incidence ratios
- SMI:
-
Secondary methylation index
References
IARC (1980) Some metals and metallic compounds. International Agency for Research on Cancer, Lyon, Franch, p 325
Chen CJ, Chuang YC, Lin TM, Wu HY (1985) Malignant neoplasms among residents of a blackfoot disease-endemic area in Taiwan: high-arsenic artesian well water and cancers. Cancer Res 45:5895–5899
Chen CJ, Chen CW, Wu MM, Kuo TL (1992) Cancer potential in liver, lung, bladder and kidney due to ingested inorganic arsenic in drinking water. Br J Cancer 66:888–892
Chiou HY, Hsueh YM, Liaw KF et al (1995) Incidence of internal cancers and ingested inorganic arsenic: a seven-year follow-up study in Taiwan. Cancer Res 55:1296–1300
National Research Council (2001) Arsenic in drinking water: 2001 update. National Academy Press, Washington, DC
Tapio S, Grosche B (2006) Arsenic in the aetiology of cancer. Mutat Res -Rev Mutat Res 612:215–246
Smith AH, Goycolea M, Haque R, Biggs ML (1998) Marked increase in bladder and lung cancer mortality in a region of Northern Chile due to arsenic in drinking water. Am J Epidemiol 147:660–669
Marshall G, Ferreccio C, Yuan Y et al (2007) Fifty-year study of lung and bladder cancer mortality in Chile related to arsenic in drinking water. J Natl Cancer Inst 99:920–928
HopenhaynRich C, Biggs ML, Fuchs A et al (1996) Bladder cancer mortality associated with arsenic in drinking water in Argentina. Epidemiology 7:117–124
Vahter M (1981) Biotransformation of trivalent and pentavalent inorganic arsenic in mice and rats. Environ Res 25:286–293
Vahter M (2002) Mechanisms of arsenic biotransformation. Toxicology 181–182:211–217
Buchet JP, Lauwerys R, Roels H (1981) Comparison of the urinary excretion of arsenic metabolites after a single oral dose of sodium arsenite, monomethylarsonate, or dimethylarsinate in man. Int Arch Occup Environ Health 48:71–79
Buchet JP, Lauwerys R, Roels H (1981) Urinary excretion of inorganic arsenic and its metabolites after repeated ingestion of sodium metaarsenite by volunteers. Int Arch Occup Environ Health 48:111–118
Vahter M (1999) Methylation of inorganic arsenic in different mammalian species and population groups. Sci Progr 82:69–88
Styblo M, Del Razo LM, Vega L et al (2000) Comparative toxicity of trivalent and pentavalent inorganic and methylated arsenicals in rat and human cells. Arch Toxicol 74:289–299
Petrick JS, Jagadish B, Mash EA, Aposhian HV (2001) Monomethylarsonous acid (MMA(III)) and arsenite: LD(50) in hamsters and in vitro inhibition of pyruvate dehydrogenase. Chem Res Toxicol 14:651–656
Nesnow S, Roop BC, Lambert G et al (2002) DNA damage induced by methylated trivalent arsenicals is mediated by reactive oxygen species. Chem Res Toxicol 15:1627–1634
Chen YC, Su HJ, Guo YL et al (2003) Arsenic methylation and bladder cancer risk in Taiwan. Cancer Causes Control 14:303–310
Chen YC, Guo YL, Su HJ et al (2003) Arsenic methylation and skin cancer risk in southwestern Taiwan. J Occup Environ Med 45:241–248
Hsueh YM, Chiou HY, Huang YL et al (1997) Serum beta-carotene level, arsenic methylation capability, and incidence of skin cancer. Cancer Epidemiol Biomarkers Prev 6:589–596
Yu RC, Hsu KH, Chen CJ, Froines JR (2000) Arsenic methylation capacity and skin cancer. Cancer Epidemiol Biomarkers Prev 9:1259–1262
Pu YS, Yang SM, Huang YK et al (2007) Urinary arsenic profile affects the risk of urothelial carcinoma even at low arsenic exposure. Toxicol Appl Pharmacol 218:99–106
Steinmaus C, Bates MN, Yuan Y et al (2006) Arsenic methylation and bladder cancer risk in case–control studies in Argentina and the United States. J Occup Environ Med 48:478–488
Steinmaus C, Yuan Y, Kalman D, Atallah R, Smith AH (2005) Intra individual variability in Arsenic methylation in a U.S. population. Cancer Epidemiol Biomarkers Prev 14:919–924
Hindmarsh JT (2002) Caveats in hair analysis in chronic arsenic poisoning. Clin Biochem 35:1–11
Hughes MF (2006) Biomarkers of exposure: a case study with inorganic arsenic. Environ Health Perspect 114:1790–1796
Wu HY, Chen KP, Tseng WP, Hsu CL (1961) Epidemiologic studies on blackfoot disease: I. Prevalence and incidence of the disease by age, sex, occupation and geographical distribution. Mem College Med Natl Taiwan Univ 7:33–50
Chen CJ, Hsueh YM, Lai MS et al (1995) Increased prevalence of hypertension and long-term arsenic exposure. Hypertension 25:53–60
Chen CJ, You SL, Lin LH, Hsu WL, Yang YW (2002) Cancer epidemiology and control in Taiwan: a brief review. Jpn J Clin Oncol 32:S66–S81
US Department of Health, Human Services (2001) International classification of diseases, ninth revision, clinical modification. US Public Health Service, Washington, DC
SEER Program NCI (2001) Conversion of morphology of ICD-O-2 to ICD-O-3. In: Percy C, Fritz A, Ries L (eds) National Cancer Institute, Bethedsa, pp 1–160
Hsueh YM, Huang YL, Huang CC et al (1998) Urinary levels of inorganic and organic arsenic metabolites among residents in an arseniasis-hyperendemic area in Taiwan. J Toxicol Environ Health A 54:431–444
Kuo TL (1964) Arsenic content of artesian well water in endemic area of chronic arsenic poisoning. Rep Inst Pathol Natl Taiwan Univ 20:7–13
Lo MC, Hsen YC, Lin BK (1977) Arsenic content of underground water in Taiwan: second report. Taiwan Provincial Institute of Environmental Sanitation, Taichung
Breslow NE, Day NE (1987) Statistical methods in cancer research. vol 2. The analysis of cohort studies. International Agency for Research on Cancer, Lyon, p 120
Steinmaus C, Yuan Y, Kalman D, Atallah R, Smith AH (2005) Intraindividual variability in arsenic methylation in a U.S. population. Cancer Epidemiol Biomarkers Prev 14:919–924
Hopenhayn-Rich C, Biggs ML, Smith AH, Kalman DA, Moore LE (1996) Methylation study of a population environmentally exposed to arsenic in drinking water. Environ Health Perspect 104:620–628
Hsueh YM, Hsu MK, Chiou HY, Yang MH, Huang CC, Chen CJ (2002) Urinary arsenic speciation in subjects with or without restriction from seafood dietary intake. Toxicol Lett 133:83–91
Concha G, Nermell B, Vahter MV (1998) Metabolism of inorganic arsenic in children with chronic high arsenic exposure in northern Argentina. Environ Health Perspect 106:355–359
Vahter M, Concha G, Nermell B, Nilsson R, Dulout F, Natarajan AT (1995) A unique metabolism of inorganic arsenic in native Andean women. Eur J Pharmacol 293:455–462
Chiou HY, Hsueh YM, Hsieh LL et al (1997) Arsenic methylation capacity, body retention, and null genotypes of glutathione S-transferase M1 and T1 among current arsenic-exposed residents in Taiwan. Mutat Res -Rev Mutat Res 386:197–207
Marnell LL, Garcia-Vargas GG, Chowdhury UK et al (2003) Polymorphisms in the human monomethylarsonic acid (MMA V) reductase/hGSTO1 gene and changes in urinary arsenic profiles. Chem Res Toxicol 16:1507–1513
Schmuck EM, Board PG, Whitbread AK et al (2005) Characterization of the monomethylarsonate reductase and dehydroascorbate reductase activities of Omega class glutathione transferase variants: implications for arsenic metabolism and the age-at-onset of Alzheimer’s and Parkinson’s diseases. Pharmacogenet Genomics 15:493–501
Wood TC, Salavaggione OE, Mukherjee B et al (2006) Human arsenic methyltransferase (AS3MT) pharmacogenetics: gene resequencing and functional genomics studies. J Biol Chem 281:7364–7373
Francesconi KA, Kuehnelt D (2004) Determination of arsenic species: a critical review of methods and applications, 2000–2003. Analyst 129:373–395
Thomas DJ, Styblo M, Lin S (2001) The cellular metabolism and systemic toxicity of arsenic. Toxicol Appl Pharmacol 176:127–144
Vega L, Styblo M, Patterson R, Cullen W, Wang C, Germolec D (2001) Differential effects of trivalent and pentavalent arsenicals on cell proliferation and cytokine secretion in normal human epidermal keratinocytes. Toxicol Appl Pharmacol 172:225–232
Drobna Z, Jaspers I, Thomas DJ, Styblo M (2003) Differential activation of AP-1 in human bladder epithelial cells by inorganic and methylated arsenicals. FASEB J 17:67–69
Gong ZL, Lu XF, Cullen WR, Le XC (2001) Unstable trivalent arsenic metabolites, monomethylarsonous acid and dimethylarsinous acid. J Anal At Spectrum 16:1409–1413
Del Razo LM, Styblo M, Cullen WR, Thomas DJ (2001) Determination of trivalent methylated arsenicals in biological matrices. Toxicol Appl Pharmacol 174:282–293
Valenzuela OL, Borja-Aburto VH, Garcia-Vargas GG et al (2005) Urinary trivalent methylated arsenic species in a population chronically exposed to inorganic arsenic. Environ Health Perspect 113:250–254
Le XC, Cullen WR, Reimer KJ (1994) Human urinary arsenic excretion after one-time ingestion of seaweed, crab, and shrimp. Clin Chem 40:617–624
Ma M, Le XC (1998) Effect of arsenosugar ingestion on urinary arsenic speciation. Clin Chem 44:539–550
Steinmaus C, Yuan Y, Kalman D, Atallah R, Smith AH (2005) Intraindividual variability in arsenic methylation in a U.S. population. Cancer Epidemiol Biomarkers Prev 14:919–924
Acknowledgments
The study was supported by grants (NSC-89-2320-B038-013, NSC-89-2314-B038-049, NSC-90-2320-B-038-021, NSC91-3112-B-038-0019, NSC92-2321-B-038-004, NSC92-3112-B-038-001, NSC93-2321-B-038-012, NSC93-3112-B-038-001, NSC94-2314-B-038-023, and NSC95-2314-B-038-007) from the National Science Council, Executive Yuan, ROC.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Huang, YK., Huang, YL., Hsueh, YM. et al. Arsenic exposure, urinary arsenic speciation, and the incidence of urothelial carcinoma: a twelve-year follow-up study. Cancer Causes Control 19, 829–839 (2008). https://doi.org/10.1007/s10552-008-9146-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-008-9146-5