
Abstract
Quantitative microbial risk assessment (QMRA) is a valuable tool for estimating the burden of disease due to exposure of a particular microbial pathogen. In this study, we used the quantitative risk assessment method to calculate the burden of disease with special reference to gastroenteritis from three reference pathogens—Escherichia coli, Campylobacter, and Rotavirus in the drinking water treatment systems of Mysore Urban city, Karnataka, India. A total of 140 samples were analyzed over a period of 24 months in different seasons using standard methods. The risk burden was estimated by guidelines for drinking water quality (WHO in Campylobacter, factsheet no. 255, 2011a; Guidelines for drinking water quality, 2011b) method. The results show that the Mysore Urban population connected to the current drinking water treatment plant seems to be vulnerable to waterborne gastroenteritis diseases since the results indicate less effectiveness on pathogen removal in treatment system. The result reveals that the pathogenic E. coli disease burden from Melapura plant shows a slower level (6.74E\(-\)07) than the WHO reference (10E\(-\)06) level. The risk estimates for Campylobacter show that they slightly exceed by (2.54E\(-\)06) over the WHO guidelines. The final disease burdens (db) of Rotavirus were lower for the both the treatment plants (Melapura—4.75E\(-\)07 and Hongally—2.54E\(-\)06) compared with the WHO reference. Overall, the estimates for the annual risks of infection of E. coli and Campylobacter were in excess of the WHO guideline values. The present QMRA study is believed to be the first attempt and to be useful for the local authorities and stakeholders to evaluate the likely risk of infection and to ensure the better management of water supplies in India.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The transport of microbial pathogens to a large number of people through drinking water causing subsequent illness is well documented. The outbreak that has been reported throughout the world demonstrates that transmission of pathogens by drinking water remains a significant cause of illness. It has been proved that drinking water treatment utilities play a major role in protecting public health through the reduction of waterborne diseases. The presence of pathogens and its relative risk in a water source may remain undetected due to limitations of the commonly used monitoring techniques (Brookes et al. 2005). To ensure sufficient drinking water treatment in terms of pathogen removal at the drinking water treatment, a microbial risk assessment needs to be performed.
In developing countries, the risk assessment of microbial pathogens in drinking water has not been conclusively established. With due concern for protection of public health and to develop an alternative treatment system, and for issuing rules and regulations to ensure the quality of water that is suitable for the intended use, an effective risk assessment should be performed. The WHO advocates the use of health based water safety plans for provision of water that is safe to drink. In particular, WHO highlighted that the use of quantitative microbial risk assessment (QMRA) is a valuable tool for validation of water safety plans (Howard et al. 2006; WHO 2011a, b, 2004).
QMRA is a technique used to estimate the burden of diseases caused by individual causative agents rather than undifferentiated health effects (Haas et al. 1999; Howard et al. 2006). Exposure assessment, dose–response analysis, and risk characterization are the major tasks of QMRA as defined by Haas and Eisenberg (2001). To understand and compare the outcomes from different types stress, the method of disability-adjusted life years (DALYs) has been recommended for risk assessment (Havelaar and Melse 2003; WHO 2004).
In a developing country like India, little information is available regarding the quantitative health risk assessment in drinking water systems. Many studies have reported on microbiological quality of drinking water system in India, but the hazard identification, exposure, and health risk-associated assessments have not yet been reported. In view of this, an attempt was made to carryout microbiological hazard identification and exposure assessment in an urban drinking water system.
In this study, we tried a simplified QMRA to assess the microbial risk with reference to gastroenteritis in Mysore urban drinking water treatment system. Mysore is a city continuously facing the problem with gastroenteritis every year. The waterborne outbreak related to contaminated drinking water supply is poorly documented in this region. Hence, the present study aims to use the simplified risk assessment to estimate the disease burden with special reference to gastroenteritis from the three reference pathogens viz., E. coli, Campylobacter and Rotavirus. The risk burden was estimated by guidelines for drinking water quality—GDWQ (WHO 2004). The E. coli results were also extrapolated for other pathogenic organisms such as Campylobacter and Rotavirus due to the lack of available pathogen concentration data and barriers in laboratory analysis. Hence many authors have been implemented initial QMRA work based on the indicator organisms (Howard et al. 2006).
By means of this simplified risk assessment method, we estimated the disease burden (db)/health outcome target (HT) for Pathogenic E. coli from distribution system and also the above-mentioned reference organism in the water leaving from the plant. Our study is believed to be the first attempt to assess the health risk in Mysore urban water system, and it will be helpful for the local authorities and other stakeholders to evaluate the likely risk of infection and to ensure the better management of water supplies.
Materials and Methods
Description of the Study Area
The study was carried out in Mysore, located at 12\(^{\circ }\) 18\(^{\prime }\)N 76\(^{\circ }\) 39\(^{\prime }\)E 12.30\(^{\circ }\) N 76.65\(^{\circ }\) E, and the city has an average altitude of 770 meters (2,526 ft) in the state of Karnataka, India. Mysore Municipal City Corporation covers an area of 128.42 Square Kilometers. The current population is about 8, 87,446 people (Census 2011) and expected to be cross one million by 2015. The work was focused on the three water treatment plants and the drinking water distribution system in Mysore city.
Description of the Water Supplies and Treatments
Drinking water in Mysore has to meet the quality requirements of the regulating authorities by State and Central Governments. To ensure that this quality is achieved, the Mysore Municipal Corporation has three water treatment plants which are located in Belagola, Hongally, and Melapura. The Raw water source for the treatment plans is mainly from the River Cauvery. The raw water is treated in all water treatment plants (WTPS) by conventional water treatment method which comprises coagulation/flocculation, sedimentation, filtration, and finally followed by disinfection. These plants have the distribution mains the total length of which about 1,281 Kms, which supply 125.98 MLD from the centralized Vani Vilas Water Works. The coverage of water supply for domestic connection is about 67 % in urban limit.
Sampling and Analysis
A total of 140 (Raw water & distribution system) samples were collected and analyzed during the three seasons in the period of 2011–2013 (winter, summer, and monsoon) for microbiological parameters. A total of 72 raw water samples were collected from the water intake point nearby respective treatment plants, and 68 samples randomly were collected from the distribution system. The samples were collected in pre-sterilized bottles and subjected to investigations to analyze the microbiological parameters such as total coliform count (TCC), fecal coliform count (FCC), and E. coli, which were determined using standard methods APHA (1998).
Risk Assessment Procedure
Data used in the QMRA were taken from different sources: Vani Vilas Water Works (VVWW), Mysore, and specific water-quality assessments undertaken in 2011 and 2013 by the authors (Table 1). In this study, QMRA was performed as described by Haas et al. (1999). The disease burden was calculated following the method described in the 4th Edition of GDWQ (WHO 2011a, b) and Howard et al. (2006). The procedure for estimation is summarized in Table 2.
Selection of Reference Pathogens
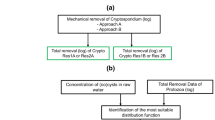
The three reference pathogens were chosen for this assessment: Pathogenic E. coli, Campylobacter and Rotavirus. The selection of reference pathogen was mainly based on the presence of an identified waterborne pathogen that occurred in India (Sharma et al. 2003; Karmakar et al. 2008; Chitambar et al. 2011; Naik and Desai 2012; Mukherjee et al. 2013). However, due to lack of specific pathogen data from the water supplies, we used indicator organisms as surrogates. The used surrogate organism was fecal coliform (E. coli was confirmed by biochemical characterization). Based on the assumption by several reports that 95 % of fecal coliforms were E. coli and 8 % of E. coli were pathogenic (Haas et al. 1999; Howard et al. 2006). In this study, the ratio used for E. coli: Pathogenic E. coli was 1: 08 (Haas et al. 1999; Howard et al. 2006); for E. coli: Campylobacter was 1: 066 (Smeets 2008; Machdar et al. 2013); and for E. coli: Rotavirus it was 1: 10\(^{-5 }\)(Mara et al. 2007; Machdar et al. 2013).The dose–response parameter used in this study was Beta Poisson model as described by Haas et al. (1999). The risk assessments were performed for all three reference pathogens collected from the water leaving the treatment plant based on the surrogate pathogen ratio. In the distribution system, the risk assessment was carried out only for pathogenic E. coli.
Pathogenic Escherichia coli
The outcomes of gastroenteritis due to pathogenic E. coli were based on the strain E. coli O157: H7. In this study, we used the data for E. coli O157: H7 due to lack of dose–response data. The outcome of disease, severity, and duration of illness due to E. coli O157: H7 were taken from Havelaar and Melse (2003) and v. According to Haas et al. (1999), the disease burden for E.coli O157:H7 can be estimated by using the dose–response data for Shigella infections. Hence, the fatality ratio for E. coli O157: H7 was considered as 0.7 % as reported by Kotloff et al. (1999) and Howard et al. (2006).
Campylobacter
Campylobacter are the most common bacteria considered as major cause of foodborne diarrheal illness in humans, which causes gastroenteritis worldwide. In developing countries, in children under the age of two years, the illness of Campylobacter was frequently reported, which also resulted in the death of children (WHO 2011a, b). For Campylobacter , the severity and duration of illness were taken from Kemmeren et al. (2006), and the fatality rate was 0.1 % with an average death at the age of 1. (Haas et al. 1999; Havelaar and Melse 2003). The outcome of gastroenteritis, severity, and duration of illness due to campylobacter were based on Kemmeren et al. (2006).
Rotavirus
Gastroenteritis due to Rotaviruses is the leading cause of life-threatening disease in developing countries. According to the study by Havelaar and Melse (2003), the case fatality rate was 0.6 % in developing countries. For this study, the fatality rate of 0.7 % has been used based on the assumption by Howard et al. (2006). The dose–response was estimated from WHO (2004), and the risk of illness from Havelaar and Melse (2003).
Calculation of DALYs
The disease burden related to gastroenteritis was calculated for each pathogen from the previous studies (Havelaar and Melse 2003; Howard et al. 2006; Machdar et al. 2013). The average life expectancy for India is 65 years (WHO 2013) which was used in the calculations. However, for lack of disease incidents and infection data for developing countries, we adopted the literature data from developed countries like Havelaar and Melse (2003). For each pathogen, the outcome of disease, severity, and duration of illness are summarized in Table 3.
Calculation of Susceptible Fraction (Exposed Population)
In this study, a comprehensive field survey was carried out to determine the water-usage pattern and the exposed population in Mysore city. The susceptible populations were calculated based on the access of domestic water supply connections in Mysore city. The city has been divided into 65 administrative wards. The existing distribution of water to the city is not uniform in all areas. The city has been divided into east zone and west zone for water supply. In east zone, 40 wards are getting daily water supply, and in west zone 25 wards are getting alternate day water supply. Based on this proportion, 56.6 % of people are getting daily water supply, and 43.4 % (City Sanitation Plan 2011) of people are getting alternate day supply of water. The daily supply of water in Melapura scheme is about 23.2 % and alternate day supply of water about 76.8 %.The daily supply of water from Hongally Scheme is about 68.2 % and alternate day supply is about 31.8 %.
In this study, the access of water supply is considered from two sources i.e., Melapura and Hongally supply scheme. The water supply from Belagola was not considered as a sustainable source of water to Mysore city. Based on the estimation, 28.3 % of connections were located in Melapura water supply scheme, and the rest 71.7 % are located in Hongally and Belagola. For the ease of calculation, we assumed that the Melapura water supply scheme provides water to 28 % and the Hongally scheme provides to 72 % of the total population. Out of 1, 42,804 connections, the domestic connection form 1,32,556 connections (Vani Vilas Water Works, Mysore). Based on the domestic connections, five persons per household were considered for the estimation of water supply coverage. The susceptible population fraction is calculated by dividing the population exposed to treated water by the total population. In the present study, 67 % of the population were considered as susceptible population.

Disease burden (db)/health outcome target (HT) for E. coli, Rotavirus and Campylobacter leaving from the treatment plants
Results and Discussion
Findings of Risk Assessment
The consistent log reduction value of 10\(^{5}\) was considered based on the reports of the published data from the conventional treatment systems (WHO 2004). Risk assessments for Pathogenic E. coli leaving from the treatment plants are shown in Table 4. WHO (2004) suggests that the reference level for tolerable risk for pathogenic E. coli is 10E\(-\)06. For the present study, data were obtained from the experimentation and from the review of the existing data. In the WHO Guidelines (WHO 2004), the unheated drinking water was set at 1 L per capita per day. In the present study, the estimated value of unheated drinking water consumption (V) was 1.025 L/day. The calculated treatment effect (PT) was 0.99999. The result of the QMRA assessment reveals that the disease burden from Melapura plant shows a lower level (6.91E\(-\)07) than the WHO reference (10E\(-\)06) level. The Hongally plant data show that the levels of risk slightly are higher (3.60E\(-\)06).
The risk estimates for Campylobacter are shown in Table 4. The QMRA results show that in Hongally Plants, they slightly exceed (2.60E\(-\)06) the WHO guidelines for health-based targets and that the Melapura is below the level of risk (4.87E\(-\)07) suggested as tolerable by WHO standards. Table 4 also shows the risk assessment of Rota Virus. The final disease burden (db) levels were low for the both treatment plants (Melapura-4.87E\(-\)07 and Hongally-2.43E\(-\)06). In case of Rotavirus, the levels of risk are lower compared with the WHO reference. The results of this study are in line with Machdar (2010) who calculated that the risk of Rotavirus infection was lower compared to those of E. coli and Campylobacter for drinking water in Nima, Ghana.
Overall, the Hongally plant slightly exceeds the reference level of risk for Pathogenic E. coli and Campylobacter (Fig. 1). It may be due to the variation in raw water quality of two plants as well as unprotected water source or inappropriate transportation to treatment plant leads increased microbial counts. In general, the pathogen concentration in treated water was well below the routine microbiological detection. By means of QMRA, it is revealed that one plant slightly exceeded the reference level of WHO. Hence, the focused importance of QMRA method is to calculate the health risk from pathogenic microorganisms with the input value of raw water pathogen concentration and treatment removal efficiency of water treatment plant.
The QMRA risk assessments for pathogenic E. coli in the distribution system are summarized in Table 5. The calculated value for risk of diarrhoeal illness given infection (P\(_{\mathrm{{ill}}/\mathrm{{inf}}}\))was 0.25.The estimated value for consumption of unheated drinking water (V) was considered as 1.025 l/day. The annualized risk assessments for Pathogenic E. coli from both distribution systems show higher value (Fig. 2) than the WHO reference level. The possible reasons of post-treatment contamination might be the old pipelines, poorly maintained distribution system (Lee and Schwab 2005), inequitable supply of water (Raju et al. 2011). The result reveals that the water supplies in distribution system are significantly more contaminated than the water leaving from the treatment plants.
The results of the present findings are in line with those of Clark et al. (1993), Geldreich (1996) and Howard et al. (2006) who state that the water quality problems are mostly associated with poor distribution systems rather than the treatment system failures. Hence, the post treatment requires the following measures like, optimization of main leak detection and repair, intensification of efforts for replacement of pipes, and periodic inspection in the distribution systems to be implemented for effective management of microbial water quality in distribution systems.

Disease burden/health outcome target for pathogenic E. coli in distribution system
From this study, it is observed that the consumers of current drinking water treatment plants of Mysore city are vulnerable to waterborne diseases due to the annual risk of infection. Due to the increase of pathogens in the water source, the post treatment will have the possibility of greater risk. Hence, it is necessary to upgrade the current treatment plant with better pathogen removal treatment technique. Detailed and continuous risk assessments on microbial pathogen are recommended in the water treatment systems of Mysore city.
Conclusions
The present study is believed to be the first attempt to estimate the disease burden from the microbial pathogens in urban water system of Mysore city. The treated water in Mysore city was found to be moderately safe in terms of microbial risk. However, post-treatment contamination was found, which indicated the problems with distribution system, thereby increasing the microbial risk of gastroenteritis even after treatment. The present model of simplified microbial risk assessment can be applied as a systemic approach by the regulatory authorities in order to control the risk posed by the examined pathogens. The present QMRA model will be improved as more data become available. For effective management of waterborne pathogens, a systematic continuous sanitation, re-creation of drinking water system, and the establishment of continuous database on drinking water quality and associated risks ares recommended.
References
APHA (American Public Health Association) (1998) Standard methods for the examination of water and wastewater, 20th edn. American Public Health Association Inc, Washington, DC
Brookes JD, Hipsey MR, Burch MD, Linden LG, Ferguson CM, Antenucci JP (2005) Relative value of surrogate indicators for detecting pathogens in lakes and reservoirs. Environ Sci Technol 39(22):8614–8621
Census India (2011) http://www.censusindia.gov.in. Accessed 18 Aug 2014
Chitambar SD, Lahon A, Tatte VS, Desai NH, Ugare MR, Kulkarni SV, Waghmare AP (2011) Occurrence of group B rotavirus infections in the outbreaks of acute gastroenteritis from western India. Indian J Med Res 134:399–400
City Sanitation Plan, Mysore (2011) http://www.indiasanitationportal.org/sites/default/files/Mysore_CSP.pdf. Accessed 19 Aug 2014
Clark RM, Goodrich JA, Wymer LJ (1993) Effect of the distribution system on drinking water quality. J Water Suppl Res Technol AQUA 42(1):30–38
Geldreich EE (1996) Microbial quality of water supply in distribution systems. Lewis Publishers, New York
Haas CN, Rose JB, Gerba CP (1999) Quantitative microbial risk assessment. Wiley, New York
Hass C, Eisenberg JNS (2001) Risk Assessment. In L. Fewtrell, J. Bartram (eds) Water Quality: Guidelines, Standards and Health; Assessment of risk and risk management for water-related infectious disease, International Water Association (IWA) on behalf of the World Health Organization, London, pp161–183
Havelaar AH, Melse JM (2003) Quantifying public health risks in the WHO guidelines for drinking-water quality: a burden of disease approach. Report 734301022/2003. RIVM, Bilthoven
Howard G, Pedley S, Tibatemwa S (2006) Quantitative microbial risk assessment to estimate health risks attributable to water supply: can the technique be applied in developing countries with limited data? J Water Health 04:49–65. http://www.who.int/mediacentre/factsheet/ts255/en http://www.who.int/gho/publications/world_health_statistics/2013/en/. 16 Aug 2014
Naik J, Desai P (2012) Detection of entero-haemorrhogic E. coli 0157:H7 and its drug resistance pattern. J Environ Res Develop 7(1):51–55
Karmakar S, Rathore Abhilakh Singh, Kadri Syed Manzoor, Dutt Som, Khare Shashi, Lal Shiv (2008) Post-earthquake outbreak of rotavirus gastroenteritis in Kashmir (India): an epidemiological analysis. Public Health 122:981–989
Kemmeren JM, Mangen MJJ, Van Duynhoven YHPT, Havelaar AH (2006) Priority setting of food borne pathogens: disease burden and costs of selection enteric pathogens. Report 330080001/2006. National Institute for Public Health and the Environment, Bilthoven
Kotloff KL, Winickoff JP, Ivanoff B, Clemens JD, Swerdlow DL, Sansonetti PJ, Adak GK, Levine MM (1999) Global burden of Shigella infections: implications for vaccine development and implementation of control strategies. Bull World Health Organ 77(8):651–666
Lee EJ, Schwab KJ (2005) Deficiencies in drinking water distribution systems in developing countries. J Water Health 3(2):109–127
Machdar EC (2010) Application of QMRA for analyzing public health risk from drinking water supply in a low income area in Accra, Ghana, Master of Sciences Thesis, UNESCO-IHE Institute for Water Education, Delft
Machdar E, van der Steen NP, Raschid-Sally L, Lens PNL (2013) Application of quantitative microbial risk assessment to analyze the public health risk from poor drinking water quality in a low income area in Accra, Ghana. Sci Total Environ 449:134–142
Mara DD, Sleig PA, Blumenthal UJ, Carr RM (2007) Health risks in wastewater irrigation: comparing estimates from quantitative microbial risk analyses and epidemiological studies. J Water Health 5(1):39–50
Mukherjee P, Ramamurthy T, Rajendran K (2013)Campylobacter jejuni in hospitalized patients with Diarrhea, Kolkata, India. Emerg Infect Dis 19(7):1155–1156
Raju NS, Roopavathi C, Ramachandra Kini K, Niranjana SR (2011) Assessment of coliform contamination in drinking water from source to point of use in Mysore city of Karnataka, India. 35\(^{th}\)WEDC, conference, Loughbourough. http://wedc.lboro.ac.uk/resources/conference/35/Raju-N-1047.pdf
Sharma S, Sachdeva P, Virdi JS (2003) Emerging waterborne pathogens. Appl Microbiol Boitechnol 61(1):424–428
Smeets PWMH (2008) Stochastic modeling of drinking water treatment in quantitative microbial risk assessment. Water Management Academic Press, Delft
WHO (2004) Guidelines for drinking-water quality, 3rd edn. World Health Organization, Geneva
WHO (2011a) Campylobacter, factsheet no. 255. WHO, Geneva. www.who.int/mediacentre/factsheets/fs255/en
WHO (2011b) Guidelines for drinking water quality, 4th edn. World Health Organization, Geneva
WHO (2013) Health statistics. http://www.who.int/gho/publications/world_health_statistics/2013/en
Acknowledgments
The authors wish to thank the Authorities of Vani Vilas Water Works, Mysore, Govt. of Karnataka for their support to carry out this study. They acknowledge the fellowship support provided by the TWAS-CAS (The World Academy of Sciences-Chinese Academy of Sciences), the Indian Council of Medical Research (ICMR), and National Natural Science Foundation of China (Project No. 51290283, 21277169) to the first author.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
George, J., An, W., Joshi, D. et al. Quantitative Microbial Risk Assessment to Estimate the Health Risk in Urban Drinking Water Systems of Mysore, Karnataka, India. Water Qual Expo Health 7, 331–338 (2015). https://doi.org/10.1007/s12403-014-0152-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-014-0152-4