
Abstract
Background
Ejection fraction (EF) reserve has been found to be a useful adjunct for identifying high risk coronary artery disease in cardiac positron emission tomography (PET). We aimed to evaluate EF reserve obtained from technetium-99m sestamibi (Tc-99m) high-efficiency (HE) SPECT.
Methods
Fifty patients (mean age 69 years) undergoing regadenoson same-day rest (8-11 mCi)/stress (32-42 mCi) Tc-99m gated HE SPECT were enrolled. Stress imaging was started 1 minute after sequential intravenous regadenoson .4 mg and Tc-99m injections, and was composed of five 2 minutes supine gated acquisitions followed by two 4 minutes supine and upright images. Ischemic total perfusion deficit (ITPD) ≥5 % was considered as significant ischemia.
Results
Significantly lower mean EF reserve was obtained in the 5th and 9th minute after regadenoson bolus in patients with significant ischemia vs patients without (5th minute: −4.2 ± 4.6% vs 1.3 ± 6.6%, P = .006; 9th minute: −2.7 ± 4.8% vs 2.0 ± 6.6%, P = .03).
Conclusions
Negative EF reserve obtained between 5th and 9th minutes of regadenoson stress demonstrated best concordance with significant ischemia and may be a promising tool for detection of transient ischemic functional changes with Tc-99m HE-SPECT.
Spanish Abstract
Antecedentes
Se ha encontrado que la reserva de la Fracción de Eyección (FE) en la tomografía de emisión de positrones cardiaca (PET, positron emission tomography por sus siglas en ingles) es una herramienta útil adicional en la identificación de pacientes con enfermedad arterial coronaria de alto riesgo. Nuestro objetivo fue evaluar la reserva de la FE obtenida por SPECT de alta eficiencia (AE) con Tecnecio-99m (Tc-99m) sestamibi.
Métodos
Cincuenta pacientes (edad promedio 69 años) a quienes se les realizo un SPECT de AE con Tc‐99m sincronizado con el electrocardiograma en un solo día reposo (8-11mCi)/estrés 32-42mCi) con regadenoson fueron incluidos La adquisición de las imágenes de estrés se inicio un minuto después de la administración secuencial intravenosa de regadenoson .4mg y Tc-99m, compuesta de 5 adquisiciones sincronizadas con el electrocardiograma de 2 minutos cada una en supino seguidas de dos adquisiciones de 4 minutos cada una en supino y sentado. Un defecto total de perfusión isquémico (DTPI) ≥5% fue considerado como isquemia significativa.
Resultados
El promedio obtenido de la Reserva de la FE fue significativamente menor en los minutos 5to y 9no posterior al bolo de regadenoson en pacientes con isquemia significativa comparados con pacientes sin isquemia (5to minuto: −4.2 ± 4.6% vs 1.3 ± 6.6%, p= 0.006; 9no minuto: −2.7 ± 4.8% vs 2.0 ± 6.6%, p = 0.03).
Conclusiones
Una Reserva de la FE negativa obtenida en los minutos 5to y 9no del estrés con regadenoson demostró una mejor concordancia con la presencia de isquemia significativa y podría ser un herramienta promisoria para la detección de cambios funcionales isquémicos transitorios con un estudio SPECT de AE con Tc-99m.
Chinese Abstract
背景
对于心脏PET显像, 射血分数 (EF) 储备 已成为评判高风险冠心病的有效辅助手段。本文旨在评价采用Tc-99m甲氧基异丁基异睛显影剂和高能SPECT测定EF储备的可行性。
方法
入选55行类伽腺苷一日法静息 (8-11mCi) /负荷 (32-42mCi) 门控高能SPECT显像的患者, 平均年龄为69岁。在连续静脉注射类伽腺苷 (0.4mg) 和Tc-99m一分钟后开始负荷图像的采集。负荷图像包括5个2分钟的仰卧位门控采集和后续2个分别为仰卧位和直立位的4分钟门控采集。总灌注缺损≧5%为显著缺血。
结果
注射类伽腺苷后, 显著缺血患者的平均EF储备在第5和第9分钟时较无缺血患者显著降低 (第5分钟: −4.2 ± 4.6% vs. 1.3 ± 6.6%, p = 0.006; 第9分钟: −2.7 ± 4.8% vs. 2.0 ± 6.6%, p=0.03)。
结论
在类伽腺苷负荷时, 第5至9分钟测得的EF储备负值与显著缺血的一致性最佳, 这很可能成为Tc-99m高能SPECT检测一过性心肌缺血伴随的心功能改变的有效手段。
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Single-photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) is a well-established non-invasive procedure for evaluation and risk stratification of patients with coronary artery disease (CAD).1 However, it has been recognized that with certain patients, SPECT MPI does not allow to detect the presence nor to estimate the extent of CAD. Indeed, the moderate to severe perfusion defects are revealed in less than half of the patients with significant left main disease.2 A number of studies have been conducted to improve the sensitivity of SPECT MPI, through the analysis of post-stress left ventricular (LV) ejection fraction (EF),3,4 post-stress wall motion abnormalities,5 and transient LV dilation,6 but these investigations have been made using conventional Anger cameras with waiting periods after stress tracer injection as long as 60 minutes. Such delayed EF measurements seem to be relatively ineffective for the detection of significant CAD, as a result of their transient nature. The ability of PET MPI to measure EF and to determine EF reserve during peak of stress using highly sensitive detectors and high-dose short-lived tracers has been reported.7 Recently, a novel high-efficiency (HE) SPECT camera with solid state cardiac-focused detectors has shown to be significantly more sensitive for the detection of cardiac activity than the conventional Anger scintillation camera,8-10 giving SPECT a “PET-like” ability to image rapidly during a peak of stress. The aim of this study was to explore the feasibility of evaluating EF reserve using HE-SPECT.
Methods
Study Population
The patients of the study were selected from consecutive subjects who were referred to clinically indicated regadenoson pharmacologic stress MPI to the Nuclear Medicine Department, Sacred Heart Medical Center, Springfield, Oregon, between August 2012 and August 2013. The selection of the patients depended on the limitations related to the scheduling of a non-routine imaging protocol, in particular the availability of the stress lab staff and nurses during the entire procedure. Fifty consecutive patients were selected for the protocol. None had any significant respiratory problems that would preclude the use of regadenoson. The study was approved by the hospital’s institutional review board, which included a waiver of informed consent.
Regadenoson Stress Protocol and Image Acquisition Sequence
Patients were instructed to discontinue any caffeine-containing products for 24 hours. Whenever possible, beta blockers and calcium-channel antagonists were terminated 48 hours before testing and nitrates at least 6 hours before testing. During the pre-imaging stress-lab evaluation and procedures, standard 12 leads for ECG monitoring and leads for image gating were applied, and a venous catheter was inserted into an antecubital vein through which the patient received a rest injection of 296-407 MBq (8-11 mCi) 99mTc-sestamibi, according to a body mass index-related dose schedule (8 mCi for BMI ≤ 25, 9 mCi for BMI range of 26-32, 10 mCi for BMI range of 33-39 and 11 mCi for BMI ≥ 40). Within 20 minutes, the patient was brought to the imaging room, equipped with an ECG/physiologic monitor, emergency cart, and oxygen source. The patient was placed in supine position in the HE-SPECT cardiac camera (D-SPECT, Spectrum Dynamics, Caesarea, Israel). Using the rest injected activity, the detector was positioned to include the entire heart image, as well as to isolate the heart from extra-cardiac activity, and a standard 6 minutes rest supine image was acquired. Approximately 30 minutes post rest injection and after obtaining baseline heart rate, blood pressure, and a 12 leads ECG, the patient, while remaining in supine position, received .4 mg of regadenoson bolus11 over 30 seconds, immediately followed by an IV bolus of 1143-1806 MBq (32-42 mCi) 99mTc-sestamibi, according to the body mass index-related dose schedule (32 mCi for BMI ≤ 25, 36 mCi for BMI range of 26-32, 40mCi for BMI range of 33-39 and 42 mCi for BMI ≥ 40). Imaging started at 1 minute post stress injection.
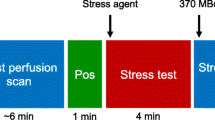
A series of five 2 minutes gated acquisitions were carried out. Between each subsequent acquisition, there was approximately 2 minutes delay, which corresponds to the technical time currently required for the system to fully complete one acquisition and start the next one. These 2-minute acquisitions are denoted by their starting time after injection in the following: 1, 5, 9, 13, and 17 minutes. After the 2-minute acquisition, a standard supine 4-minute acquisition (at 21st minute) followed by a standard 4-minute upright acquisition was completed (Figure 1). There was no repositioning of the patient or camera detector during the entire sequence of supine imaging. Heart rate, blood pressure, and ECG were monitored and recorded during the imaging protocol and 10 minutes after. The entire clinical stress protocol was performed in a standard manner by the stress laboratory staff that could terminate the study at any time if deemed necessary.

Technetium-99m sestamibi rest—early/late stress protocol. Red arrows indicate timing of rest and stress tracer and regadenoson injection. Blue boxes indicate timing of rest and consecutive early and late stress acquisitions. Note that the first acquisition (1 minute post injection) has been discarded for further analysis due to poor image quality
High-Efficiency SPECT Scanner, Scanning Methods, and Image Processing
The HE-SPECT system (D-SPECT, Spectrum Dynamics, Caesarea, Israel) uses nine collimated, pixilated cadmium zinc telluride (CZT) detector columns, mounted vertically in 90° geometry.12,13 Each of the columns consists of 1024 (16 × 64), 5-mm-thick CZT elements (2.46 × 2.46 mm2). Square-hole tungsten collimators are fitted to each of the detectors, with the size of the collimator holes matching the dimensions of the detector elements. Scintigraphic data are acquired by the detector columns rotating in synchrony, focusing on the region of interest (the heart), and are saved in list-mode along with R-wave markers. Before imaging, the detector was positioned parallel to the patient’s chest, and care was taken to align the heart to the center of the field of view. Each image set was acquired with 120 projections per detector. Transaxial images were then generated by using proprietary Broadview reconstruction algorithm (Spectrum Dynamics), based on the maximum likelihood expectation maximization method.12 Images were reoriented into short-axis and vertical and horizontal long-axis slices using standard software (QPS/QGS, Cedars-Sinai Medical Center, Los Angeles, California).
All image contours were reviewed by an experienced technologist and a nuclear cardiologist and were individually adjusted if required. Since manual correction resulted in a fixed valve plane contour, it was then necessary to correct all gated images including the standard rest and stress images for the purpose of comparison. This approach prevented us from a possible bias, which could occur if uncorrected contours were compared to user-corrected contours. Therefore, the correction rates for stress and rest scans and for early and delayed scans were approximately the same. The contour correction was kept as similar as possible for all the standard and serial 2-minute images within a patient study.
Automated Quantification of Perfusion and Function and Visual Assessment
QPS software computed total perfusion deficit (TPD) score by integrating the hypoperfusion severities below normal limits in polar map coordinates.14 Normal limits threshold was defined as 3.0 mean absolute deviations (approximately equivalent to 2.5 standard deviations) for each polar map sample. Ischemic TPD (ITPD) was calculated as the absolute difference between TPD at stress, taken from the last 2-minute supine acquisition (at 17th minute) and rest TPD,15,16 and was expressed as a percentage (%). Stress EF and rest EF were quantified separately for each acquisition using standard QGS software with 16 frames per cardiac cycle. EF reserve was calculated as the absolute difference between stress EF and rest EF for each acquisition. For further analysis, the patients were categorized retrospectively into two groups depending on their ITPD (5% cut-off). Significant ischemia was considered as ITPD ≥5%.
Image quality was assessed by experienced imaging cardiologists and was scored using four categories (excellent/good, fair, poor, uninterpretable). Extra-cardiac activity was scored using three categories (none, low, high).
Statistical Analysis
Statistical analyses were performed using STATA software (version 12, StataCorp LP). All continuous variables were described as mean ± SD. Student two-sample t-test was used to compare differences for continuous variables. Chi-square test was used to compare differences across subgroups for categorical variables. Two-sample Wilcoxon rank-sum (Mann-Whitney) test was used to compare differences between the ischemic and non-ischemic patient groups (as defined below). A 2-tailed P < .05 was considered statistically significant.
Results
Baseline clinical characteristics of studied patients are presented in Table 1. Overall, 22 patients (44%) had stress TPD = 0 %; stress TPD >0 % was seen in 28 patients. 40 patients did not have significant ischemia (ITPD <5%), and 10 patients had significant ischemia (ITPD ≥5%). Gated resting EF <50% was recorded in 14 patients (28%).
Assessment of Image Quality
Low myocardial tracer activity, residual ventricular blood pool activity, and high interfering hepatic activity in the initial acquisition started 1 minute after tracer injection were noticed. Such poor quality precluded the use of this acquisition for further accurate quantitative perfusion and functional analysis. Thus, the images from the 2nd minute acquisition have been discarded.
However, the subsequent 2-minute early acquisitions and the 4-minute standard supine acquisition showed improved (at least a fair) image quality, except for only two early stress acquisitions where an excess of extra-cardiac (abdominal) activity was observed. Namely, the acquisitions started at 5th, 9th, 13th, 17th, and 21st minutes have been considered for analysis, as shown in Figures 1 and 2. The grades of quality of stress and rest acquisitions are shown in Table 2. It is noteworthy that, despite beginning stress imaging 5 minutes after regadenoson/tracer injection, 96% of the stress images demonstrated good, excellent, or fair quality, allowing a confident clinical reading. Clinical example of poor quality 1st minute stress acquisition is depicted in Figure 3a. The examples of good image quality in the 5th and 9th minute stress acquisitions are presented in Figure 3b, c, respectively, but some mild degree of residual extra-cardiac activity is still seen. Similarly to the standard rest acquisitions, 98% of early stress images demonstrated none or low grades of extra-cardiac activity (Table 2). The overall image quality and level of extra-cardiac activity were similar in both analyzed subgroups.

Comparison of mean ejection fraction reserve (EFR) obtained from early and late consecutive acquisitions between ITPD ≥5% group (red line) and ITPD <5% group (blue dotted line). Significant difference at 5th and 9th minutes between the two subgroups was observed. Small bars indicate standard deviation. ITPD ischemic total perfusion deficit



Stress and rest gated images (short axis, vertical long axis, and horizontal long axis) in the same patient at different acquisition times. A First gated acquisition (starting at 1 minute post injection): increased right ventricular uptake and extra-cardiac activity in gated stress acquisition and no right ventricular uptake/extra-cardiac activity in standard gated rest acquisition. B Good-quality early 5th minute gated stress acquisition and standard rest acquisition with no longer increased right ventricular uptake/extra-cardiac activity in stress images. Anterior and septal reversible perfusion defects are clearly seen at that time but were not seen in the first acquisition shown in panel (A). C Good-quality 9th minute gated stress acquisition and standard rest acquisition with no increased right ventricular uptake/extra-cardiac activity in stress images. Anterior and septal reversible perfusion defects are clearly seen similar to (B). Some degree of residual extra-cardiac activity is still seen at the 5th and 9th minute images
Quantitative Results
Overall, in this study, the manual correction for all acquisitions was required in approximately 48% of the patients. It was applied in 7/10 of abnormal (ITPD ≥5%) and 18/40 of normal (ITPD <5%) patients. This is a much higher rate than in usual practice; however, in this study, if just one file required correction for a given patient, all studies had to be corrected for that patient. No difference in mean rest TPD in ITPD ≥5% group vs ITPD <5% group (5.1 ± 6.4 vs 4.8 ± 6.0, P = .9) was observed. However, significantly higher mean values of stress TPD in ITPD ≥5% group vs ITPD <5% group (13.9 ± 4.6% vs 5.1 ± 6.4%, P = .0002) were seen. Similarly, significantly higher mean ITPD values in ITPD ≥5% group vs ITPD <5% group (9.5 ± 2.6% vs 1.2 ± 1.5%, P < .0001) were monitored.
Comparison of stress EF between the subgroups is shown in Table 3. The trend for lower mean EF values in the first two acquisitions (5th and 9th minute) was seen. Comparison of mean EF reserve between the two groups during all consecutive acquisitions is depicted in Figure 2. In the ITPD ≥5% group, mean EF reserve was negative through all acquisitions (from −4.2% in 5th minute to −1.5% in 21st minute). In contrast, the ITPD <5% group demonstrated positive mean EF reserve through all acquisitions. Moreover, in the ITPD <5% group, mean EF reserve was higher during the first two acquisitions (5th and 9th minute) as compared to the three later ones (Figure 2). In the first two early acquisitions (5th and 9th minute), significantly lower mean EF reserve (P = .006 and P = .03) was observed in the ITPD ≥5% group as compared to the ITPD <5% group (Figure 2). Regarding the later acquisitions (13th, 17th, and 21st minute), the ITPD ≥5% group showed lower mean EF reserve, but these results were not statistically significant as compared to second subgroup. Individual per-patient EF reserve values at 5th and 21st minutes are depicted in Figure 4. In the group with ITPD ≥5%, 7 patients out of 10 demonstrated a negative EF reserve at both 5th and 21st minute. In the group with ITPD <5%, 33 out of 40 patients had a positive EF reserve at both 5th and 21st minute.

Individual EF reserve responses for the 50 patients, corresponding to the 5th and 21st minute acquisitions. Red lines correspond to the ITPD ≥5% group (n = 10). Blue lines correspond to ITPD <5% group (n = 40)
Discussion
To the best of our knowledge, this is the first study evaluating feasibility of EF reserve quantification obtained from early gated acquisitions using Tc-99m HE-SPECT MPI. The main discovery in our study is that the EF reserve obtained from early gated acquisitions (obtain 5 and 9 minutes after injection) showed concordance with significant myocardial ischemia, while later acquisitions (at 13th, 17th and 21st minute) or standard HE-SPECT gated acquisitions did not. According to our findings, the time range period (5 to 9 minutes after injection) should be considered in further studies for the detection of early ischemic functional changes after regadenoson stress. This timing appears to be in accordance with regadenoson pharmacodynamics11 where the vasodilatation effect starts 3 minutes after injection, peaking at 5 minutes, and fading slowly during the next 10 minutes. Another important finding needs to be noted: the later acquisitions (started at, 17th, and 21st minute) failed to show significant correlation between ischemia and EF reserve. Based on our observations, we considered the practical inexpediency of performing multiple 2 minute-long gated acquisitions as it was done in the present study. We would therefore recommend performing a single 2 minute-long gated acquisition at 5th minute or potentially even earlier after regadenoson bolus covering the peak of activity.
Another noteworthy finding was the good image quality with low or no extra-cardiac tracer activity as early as 5 minutes after Tc-99m injection as well as in later subsequent gated acquisitions. This observation appeared to be in accordance with a previous study17 with the same HE-SPECT camera but with a different (dual isotope) MPI protocol. This was explained by the fact that early post-injection imaging with HE-SPECT camera may be completed rapidly before extra-cardiac radioactivity has reached maximum. However, our observations contradict another study,18 where different type of CZT camera was used, that showed that resting Tc-99m images acquired in the 0 to 8 minutes range period were predominantly uninterpretable due to either increased blood pool uptake or perfusion defects. In that study, the images acquired in the 8th to 12th minute range were interpretable and compared to the conventional images obtained 60 minutes after injection.
Despite the fact that the mean body mass index of the studied population was 31 kg/m2, (mild to moderate obesity), the image quality for early gated images in obese patients was also found to be good. High diagnostic accuracy and image quality of HE-SPECT in obese population has been recently reported.19
First attempts to detect early ischemic functional abnormalities in nuclear cardiology were done with 82-Rb PET, when the usefulness of EF reserve assessment was demonstrated.7,20,21 High EF reserve was shown to have excellent negative predictive value in exclusion of severe CAD during dipyridamole stress 82-Rb PET MPI.7 In a study of EF reserve during regadenoson 82-Rb PET, MPI is inversely related to the magnitude of reversibility and myocardial jeopardy, increasing from rest to stress in the normal MPI but not in the abnormal studies.20 The prognostic value of negative EF reserve to predict cardiac events and all-cause mortality has also been suggested.21 Due to i) high cost and unavailability of PET in many nuclear labs and ii) growing availability of new generation SPECT cameras,22 our study of HE-SPECT might have significant practical repercussions. In particular, it is in agreement with results of PET studies,7,20 showing that severe ischemia is associated with negative EF reserve. According to our results, HE-SPECT appears to be a useful diagnostic tool for the evaluation of peak stress functional gated parameters similar to 82Rb PET MPI. Furthermore, as it is routinely done with PET, the feasibility of myocardial blood flow measurements with HE-SPECT has been recently shown.23 Therefore, it is possible that the same early imaging could be used to measure both myocardial flow and EF reserve.
This feasibility study has several limitations. The data were obtained in a single center and with one particular type of equipment. The study sample was small, especially for patients with significant ischemia, but nevertheless, the results were shown to be statistically significant. Due to these limitations, we were not able to perform separate analysis for female or obese patients. No angiographic or clinical end-points correlation of negative EF reserve was evaluated. The timing of the acquisition was perhaps not optimal and could explain a modest EF decrease. It is possible that a slightly earlier acquisition, as compared to the 5th minute post stress acquisition used in this study, would allow an even better differentiation of EF reserve. However, image quality may be an issue, and thus, further studies are required to determine the optimal imaging time. Additionally, in current implementation of the software, any manual correction of the valve constraints resulted in a user-defined fixed valve plane position. It was therefore necessary to correct all gated images including the rest and stress (at all time points) images for purposes of serial comparison for patients in which some correction was required in even one study. This approach, however, prevented us from a possible bias where uncorrected contours were compared to user-corrected contours (with no valve motion). Further studies are likely warranted with alternative segmentation approaches. Currently, cardiac 82Rb PET MPI stress acquisitions start as early as 30 seconds after regadenoson stress bolus.21 Larger studies with coronary angiographic correlation and comparison to cardiac PET imaging are needed for further evaluation of the usefulness of EF reserve with HE-SPECT.
New Knowledge Gained
It is feasible to evaluate EF reserve using HE-SPECT during peak of regadenoson stress as early as 5 minutes after Tc-99m injection. Since the negative EF reserve correlated with significant ischemia, it would be helpful to acquire the gated images as early as 5 minutes after injection in order detect transient ischemic functional changes.
Conclusions
We have demonstrated the feasibility of early EF reserve measurement with HE-SPECT. Negative EF reserve obtained between 5th and 9th minutes of regadenoson stress demonstrated best concordance with significant ischemia and could be a promising clinical tool for detection of early ischemic functional changes with Tc-99m HE-SPECT.
Abbreviations
- SPECT:
-
Single-photon emission computed tomography
- MPI:
-
Myocardial perfusion imaging
- CAD:
-
Coronary artery disease
- LV:
-
Left ventricular
- EF:
-
Ejection fraction
- PET:
-
Positron emission tomography
- HE:
-
High-efficiency
- CZT:
-
Cadmium-zinc-telluride
- TPD:
-
Total perfusion deficit
- ITPD:
-
Ischemic total perfusion deficit
- SD:
-
Standard deviation
References
Holly TA, Abbott BG, Al-Mallah M, Calnon DA, Cohen MC, DiFilippo FP, et al. Single photon-emission computed tomography. J Nucl Cardiol 2010;5:941-73.
Berman DS, Kang X, Slomka PJ, Gerlach J, de Yang L, Hayes SW, et al. Underestimation of extent of ischemia by gated SPECT myocardial perfusion imaging in patients with left main coronary artery disease. J Nucl Cardiol 2007;4:521-8.
Lima RS, Watson DD, Goode AR, Siadaty MS, Ragosta M, Beller GA, Samady H. Incremental value of combined perfusion and function over perfusion alone by gated SPECT myocardial perfusion imaging for detection of severe three-vessel coronary artery disease. J Am Coll Cardiol 2003;1:64-70.
Sharir T, Germano G, Kavanagh PB, Lai S, Cohen I, Lewin HC, et al. Incremental prognostic value of post-stress left ventricular ejection fraction and volume by gated myocardial perfusion single photon emission computed tomography. Circulation 1999;10:1035-42.
Sharir T, Bacher-Stier C, Dhar S, Lewin HC, Miranda R, Friedman JD, et al. Identification of severe and extensive coronary artery disease by postexercise regional wall motion abnormalities in Tc-99m sestamibi gated single-photon emission computed tomography. Am J Cardiol 2000;11:1171-5.
Abidov A, Bax JJ, Hayes SW, Cohen I, Nishina H, Yoda S, et al. Integration of automatically measured transient ischemic dilation ratio into interpretation of adenosine stress myocardial perfusion SPECT for detection of severe and extensive CAD. J Nucl Med 2004;12:1999-2007.
Dorbala S, Vangala D, Sampson U, Limaye A, Kwong R, Di Carli MF. Value of vasodilator left ventricular ejection fraction reserve in evaluating the magnitude of myocardium at risk and the extent of angiographic coronary artery disease: an 82Rb PET/CT study. J Nucl Med 2007;3:349-58.
Imbert L, Poussier S, Franken PR, Songy B, Verger A, Morel O, et al. Compared performance of high-sensitivity cameras dedicated to myocardial perfusion SPECT: A comprehensive analysis of phantom and human images. J Nucl Med 2012;12:1897-903.
Sharir T, Slomka PJ, Hayes SW, DiCarli MF, Ziffer JA, Martin WH, et al. Multicenter trial of high-speed vs conventional single-photon emission computed tomography imaging: Quantitative results of myocardial perfusion and left ventricular function. J Am Coll Cardiol 2010;18:1965-74.
Erlandsson K, Kacperski K, van Gramberg D, Hutton BF. Performance evaluation of D-SPECT: a novel SPECT system for nuclear cardiology. Phys Med Biol 2009;9:2635-49.
Iskandrian AE, Bateman TM, Belardinelli L, Blackburn B, Cerqueira MD, Hendel RC, et al. ADVANCE MPI Investigators. Adenosine vs regadenoson comparative evaluation in myocardial perfusion imaging: Results of the ADVANCE phase 3 multicenter international trials. J Nucl Cardiol 2007;5:645-58.
Sharir T, Ben-Haim S, Merzon K, Prochorov V, Dickman D, Ben-Haim S, Berman DS. High-speed myocardial perfusion imaging. Initial clinical comparison with conventional dual detector Anger camera imaging. J Am Coll Cardiol Imaging 2008;1:156-63.
Patton J, Berman DS, Slomka P. Recent technological advances in nuclear cardiology. J Nucl Cardiol 2007;14:433-54.
Slomka PJ, Nishina H, Berman DS, Akincioglu C, Abidov A, Friedman JD, et al. Automated quantification of myocardial perfusion SPECT using simplified normal limits. J Nucl Cardiol 2005;1:66-77.
Xu Y, Kavanagh P, Fish M, Gerlach J, Ramesh A, Lemley M, et al. Automated quality control for segmentation of myocardial perfusion SPECT. J Nucl Med 2009;9:1418-26.
Nishina H, Slomka PJ, Abidov A, Yoda S, Akincioglu C, Kang X, et al. Combined supine and prone quantitative myocardial perfusion SPECT: method development and clinical validation in patients with no known coronary artery disease. J Nucl Med 2006;1:51-8.
Berman DS, Kang X, Tamarappoo B, Wolak A, Hayes SW, Nakazato R, et al. Stress thallium-201/rest technetium-99m sequential dual isotope high-speed myocardial perfusion imaging. JACC Cardiovasc Imaging 2009;3:273-82.
Askew JW, Miller TD, Ruter RL, Jordan LG, Hodge DO, Gibbons RJ, O’Connor MK. Early image acquisition using a solid-state cardiac camera for fast myocardial perfusion imaging. J Nucl Cardiol 2011;5:840-6.
Nakazato R, Slomka PJ, Fish M, Schwartz RG, Hayes SW, Thomson LE, et al. Quantitative high-efficiency cadmium-zinc-telluride SPECT with dedicated parallel-hole collimation system in obese patients: Results of a multi-center study. J Nucl Cardiol 2014;2:266-75.
Hsiao E, Ali B, Blankstein R, Skali H, Ali T, Bruyere J Jr, et al. Detection of obstructive coronary artery disease using regadenoson stress and 82Rb PET/CT myocardial perfusion imaging. J Nucl Med 2013;10:1748-54.
Dorbala S, Hachamovitch R, Curillova Z, Thomas D, Vangala D, Kwong RY, Di Carli MF. Incremental prognostic value of gated Rb-82 positron emission tomography myocardial perfusion imaging over clinical variables and rest EF. JACC Cardiovasc Imaging 2009;7:846-54.
Slomka PJ, Berman DS, Germano G. New cardiac cameras: Single-photon emission CT and PET. Semin Nucl Med 2014;4:232-51.
Ben-Haim S, Murthy VL, Breault C, Allie R, Sitek A, Roth N, Fantony J, et al. Quantification of myocardial perfusion reserve using dynamic SPECT imaging in humans: A feasibility study. J Nucl Med 2013;6:873-9.
Acknowledgment
This research was supported in part by Grant R01HL089765 from the National Heart, Lung, and Blood Institute/National Institutes of Health (NHLBI/NIH) (PI: Piotr Slomka). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NHLBI/NIH. Yafim Brodov, MD, PhD is a Michael Kogan Save a Heart Foundation fellow in Cardiac Imaging and Nuclear Cardiology, Cedars-Sinai Medical Center, Los Angeles, California.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Drs Piotr Slomka, Guido Germano, and Daniel Berman receive royalties from the QPS software employed in the study for the quantification of perfusion. Dr Mathews Fish is a medical consultant for Spectrum Dynamics. All others disclose no current conflict of interest.
Additional information
JNC thanks Dr. E. Alexanderson, UNAM, Mexico, for providing the Spanish abstract, and Weihua Zhou, PhD, University of Southern Mississippi, USA, for providing the Chinese abstract. An audio interview between Dr. Slomka and the editor-in-chief, Dr. Iskandrian, discussing the article can be found as Electronic Supplementary Material at SpringerLink.
See related editorial, doi:10.1007/s12350-016-0570-8.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Brodov, Y., Fish, M., Rubeaux, M. et al. Quantitation of left ventricular ejection fraction reserve from early gated regadenoson stress Tc-99m high-efficiency SPECT. J. Nucl. Cardiol. 23, 1251–1261 (2016). https://doi.org/10.1007/s12350-016-0519-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-016-0519-y