
Abstract
Background
Cardiac CT is a non-invasive modality with the ability to estimate LVEF. However, given its limited temporal resolution and radiation, there has been initial resistance to use CT to measure LVEF. Developing an accurate, fast, low radiation dose protocol is desirable.
Objective
The objective of this study is to demonstrate that a ‘low radiation dose’ 64 slice cardiac computed tomography (CT) protocol is feasible and can accurately measure left ventricular ejection fraction (LVEF) while delivering a radiation dose lower than radionuclide angiography (RNA).
Methods
Patients undergoing RNA were prospectively screened and enrolled to undergo a ‘low-dose’ 64 slice CT LVEF protocol. LVEF measures, duration of each study and radiation dose between CT and RNA were compared.
Results
A total of 77 patients (mean age = 61.8 ± 12.2 years and 58 men) were analyzed. The mean LVEF measured by CT and RNA were 41.9 ± 15.2% and 39.4 ± 13.9%, respectively, (P = 0.154) with a good correlation (r = 0.863). Bland-Altman plot revealed a good agreement between the CT and RNA LVEF (mean difference of −2.4). There was good agreement between CT LVEF and RNA for identifying patients with LVEF ≤30% (kappa = 0.693) and LVEF ≥50% (kappa = 0.749). The mean dose estimated effective dose for CT and RNA were 4.7 ± 1.6 and 9.5 ± 1.0 mSv, respectively. The mean CT LVEF imaging duration (4:32 ± 3:05 minutes) was significantly shorter than the RNA image acquisition time (9:05 ± 2:36 minutes; p < 0.001).
Conclusion
The results of our study suggest that low-dose CT LVEF protocol is feasible, accurate, and fast while delivering a lower radiation dose than traditional RNA.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Left ventricular ejection fraction (LVEF) has been demonstrated to have prognostic value in numerous cardiac conditions and is often used to guide medical and device therapy.1-9 Recent guidelines have identified patients with LVEF ≤30% who may benefit from primary prevention using devices such as implantable cardioverter defibrillators (ICD) and cardiac resynchronization therapy (CRT).10 Thus the accurate measure of LVEF is extremely desirable. Cardiac CT is a non-invasive modality with the ability to estimate LVEF with prognostic value incremental to coronary artery disease (CAD) severity.11 Studies have demonstrated good correlation between CT and echocardiography,12-16 biplane cine-ventriculography,13 gated myocardial perfusion imaging,17,18 and radionuclide LV angiography (RNA).19 However, given its limited temporal resolution and radiation, there has been initial resistance to use CT to measure LVEF.
The objective of this study is to demonstrate that a relatively ‘low radiation dose’ 64 slice cardiac CT protocol is feasible and can accurately measure LVEF while delivering a radiation dose lower than RNA.
Methods
Between June 2012 and August 2013, patients undergoing radionuclide angiography (RNA) for assessment of LVEF were prospectively screened and enrolled. On the same day as their RNA, eligible candidates underwent a ‘low-dose’ CT LVEF protocol. Patients with renal dysfunction (GFR <45 mL/minutes), atrial arrhythmias, and allergy to iodinated contrast agents were excluded. The study was approved by the Institutional Human Research Ethics Board and all patients provided written informed consent.
CT LVEF Protocol
Image acquisition was performed without metoprolol, diltiazem, or nitroglycerin to ensure that the test was feasible and was not limited by heart rate. A bi-phasic timing bolus was used to measure transit time11,20 and CT LVEF image acquisition was performed using a tri-phasic intravenous contrast administration protocol. The volume and rate of contrast were individualized according to scan time and patient body habitus.11,20 Retrospective ECG-gated data sets were acquired with the GE Volume CT (GE, Milwaukee, Wisconsin) with 64 × 0.625 mm slice collimation and a gantry rotation of 350 ms (mA = 200-300, kV = 80-100) without ECG-gated X-ray tube modulation. Pitch (0.16-0.24) was individualized according to heart rate. Data sets were reconstructed using 10 phases (5-95%) with 1.25 mm slice collimation and an increment of 1.25 mm.
CTA Image Analysis
ECG-gated CT images were post-processed, using the GE Advantage Volume Share Workstation (GE, Milwaukee, Wisconsin) and the Aquarius iNtuition (TeraRecon San Mateo, California), by expert observers blinded to all clinical data and RNA results. Using a semi-automated volumetric algorithm (Advantage Workstation, Ejection Fraction), LV volumes were measured at end-diastole and end-systole, and LVEF was calculated.11,21,22
Radionuclide Angiography
RNA was performed using the local clinical protocol using the ‘modified in-vivo method’.23 In brief, equilibrium planar RNA with Tc-99m-labeled red blood cells was performed with a small field-of-view Siemens ZLC gamma camera and a low-energy all-purpose collimator.24 Gated acquisition was performed for 24 frames per cardiac cycle with a beat rejection window of 10%. Scans were acquired in the best septal left anterior oblique view and a minimum of six million counts were acquired. Calculations of LVEF and LV volumes were performed twice using FUGA software (version 4.7, HERMES Medical Solutions, Stockholm, Sweden) and the mean LVEF and LV volumes were used for analysis.24-26
Statistical Analysis
Statistical analyses were performed using SAS (version 9.2, SAS Institute Inc., Cary, NC), and statistical significance was defined as P < 0.05. Continuous variables are presented as means with standard deviations and median with interquartile range (IQR), and categorical variables are presented as frequencies with percentages. To compare patient characteristics, Wilcoxon rank-sum test was used to compare continuous variables and Fisher’s exact test was used for categorical variables. Kappa analysis was used to assess the agreement of LVEF categories. The inter-observer reliability for measures of LVEF and volumes were assessed using intra-class correlation coefficients (ICC) and the Bland-Altman plot was also used to assess agreement and potential biases.
Results
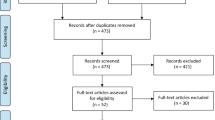
A total of 78 patients presenting for RNA imaging to assess LVEF were recruited for same day CT LVEF imaging. 77 (99%) patients had CT LVEF imaging the same day as the RNA, but 1 patient, due to time restraints, elected to return 4 days later for CT LVEF imaging. One patient was excluded from analysis for missing CT image data, therefore, the final analysis comprised 77 patients (mean age = 61.8 ± 12.2 years and 58 men) (Table 1).
Measured Left Ventricular Ejection Fraction
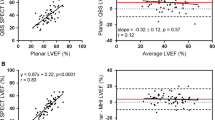
The mean LVEF measured by CT and RNA were 41.9 ± 15.2% and 39.4 ± 13.9%, respectively (P = 0.154) with a good correlation (r = 0.863) (Fig. 1). Bland-Altman plot revealed a good agreement between the CT and RNA LVEF (mean difference of −2.4; Fig. 2). The kappa agreement between CT and RNA for patients with LVEF ≤30%, 30-49%, and ≥50% was good (kappa = 0.658), and the kappa agreement for patients with LVEF ≤30% and LVEF ≥50% were 0.693 and 0.749, respectively (Table 2). 44 (57%) patients had CT and RNA LVEF measurements within 5% of each other and 64 (83%) patients were within 10%.

Correlation between LVEF measured by RNA and CT

Bland-Altman plot of the difference in mean LVEF percent between RNA and CT methods
Acknowledging the temporal resolution of CT, a subanalysis was performed in the 30 patients with HR >60 bpm. The mean LVEF measured by CT and RNA were 40.4 ± 18.2% and 38.1 ± 15.3%, respectively (P = 0.301) (Table 3) with a good correlation (r = 0.844) (Fig. 3).

Correlation between LVEF measured by RNA and CT in subjects with CT heart rates >60 (r = 0.844)
Radiation Exposure
The mean mA and kVp used for CT LVEF were 295.4 ± 14.5 and 87.5 ± 9.8, respectively (Table 4). The mean dose length product of CT LVEF was 335.7 ± 114.3 mGy*cm with an estimated effective dose of 4.7 ± 1.6 mSv. With RNA, the mean administered pertechnetate dose was 1358.7 ± 148.8 MBq with an estimated effective dose of 9.5 ± 1.0 mSv (Table 4).
Image Acquisition
The mean heart rate at the time of CT LVEF imaging was 60.2 ± 14.7 bpm and the mean contrast volume used for CT LVEF was 94.1 ± 5.5 mL (Table 4).
Imaging duration was measured using both imaging modalities (Table 4). The mean CT LVEF imaging time (duration between initial scout to final retrospective ECG-gated image acquisition) (4:32 ± 3:05 minutes) was significantly shorter than both the RNA image acquisition time (9:05 ± 2:36 minutes; P < 0.001) and the total duration of the RNA study (stannous injection to completion of image acquisition) (85:39 ± 23:44 minutes; P < 0.001).
Variability in LVEF Measures
The inter-observer variability of CT LVEF was 0.94 (0.91-0.96). RNA LVEF was measured twice using automated and semi-automated method and the variability between the two measures was 0.99 (0.98-0.99).
Discussion
Our study explores a protocol, using existing 64-slice single-source CT, which minimizes radiation while maintaining diagnostic accuracy. The results of our study suggest that low-dose CT LVEF protocol is feasible, accurate, and fast while delivering a lower radiation dose than traditional RNA.
Left ventricular ejection fraction (LVEF) is important in determining the prognosis of many cardiac conditions and its measurement is often used as a guide for medical and device therapy.1-9 Decisions to initiate specific cardiac medications in patients with congestive heart failure (CHF) are based upon LVEF and symptoms. The continuation of chemotherapy, in cancer patients, is often determined by stability in LVEF. LVEF measures are important to the decision-making for CABG and cardiac valve surgery. Recent guidelines have identified patients with LVEF ≤30% and 35% benefit from primary prevention using devices such as implantable cardioverter defibrillators (ICD) and cardiac resynchronization therapy (CRT).10 Thus the accurate assessment of LVEF is extremely important to patient care. Due to the increasing demand to assess LVEF for clinical decision-making, safe, accurate, and accessible non-invasive methods are being sought.
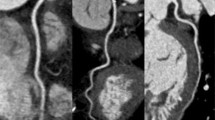
We observed that our CT volumes were smaller than those obtained with RNA. This is likely explained by overlapping vascular structures. Since RNA images were obtained in the left anterior oblique position, counts from the vascular structures such as the left atrium and aorta would have been included, thereby increasing end-systolic and end-diastolic volumes (Fig. 4).

3D-volume rendered image of the left ventricle, left atrium, and aorta in LAO 45° and left lateral positions (A, B). Left lateral view demonstrating vascular structures (left atrium and aorta) that would contribute to the RNA counts using a region of interest in the LAO 45° position (C, D)
Methods for Assessing Left Ventricular Ejection Fraction
Currently, cardiac magnetic resonance imaging (CMR) and radionuclide angiography (RNA) are considered the most accurate measures of LVEF. However, access to CMR can be limited and potentially costly. Though RNA is more available, it requires the administration of a radiotracer that exposes patients to 8-10 mSv of ionizing radiation. This becomes a concern when patients require repeat studies for monitoring or changes in clinical status.
Echocardiography is equally accessible as RNA, however, studies have demonstrated inaccuracies in echocardiographic LVEF measurements, which may be related to extrapolation of volumes using 2-dimensional measures, poor acoustic windows, and local expertise.
The radiation exposure of CT using a retrospective ECG-gated image acquisition protocol (10-15 mSv) has limited its widespread acceptance. If a new CT protocol could be developed to minimize radiation exposure, lower than that of RNA, then CT may be a viable modality for measuring LVEF when echocardiography or CMR are not immediately available. However, efforts made to reduce patient radiation exposure will result in the inability to assess the coronary arteries. Future advances in both hardware and software may facilitate low radiation dose studies while maintaining sufficient CT image quality to evaluate for LVEF and CAD. Although we would not advocate that this new technique be used routinely, we demonstrate that it is a viable option for measuring LVEF especially when other modalities are unavailable, not feasible or inconclusive.
Limitations
This is a single centre study using a single-source 64-slice CT. Although our results require confirmation using newer technologies, one would anticipate similar or better results. The need for contrast is another potential limitation of this technique; our results cannot be extrapolated to all patient populations. Due to the risk of acute contrast-induced kidney injury, patients with low GFR were excluded from the study. Such patients may be best studied using modalities which would minimize this renal risk. However, some studies have demonstrated that the risks of contrast may be small.27 Similarly, patients with atrial fibrillation may not be routine CT LVEF candidates but would be dependent upon available CT technology. Although the temporal resolution of CT is limited, our study purposely did not use acute b-blocker for heart rate control. The subanalysis of patients with HR >60 demonstrated that the agreement between RNA and CT LVEF was still very good. In addition, this study assesses accuracy and not test-retest repeatability. Future studies are still needed to demonstrate the reproducibility of CT LVEF measures.
New Knowledge Gained
This study demonstrates that a new “low radiation dose” 64-slice CT protocol can accurately measure LVEF while delivering less radiation than RNA. Thus, it is a potential option for assessing heart function when other traditional modalities may not be available or feasible.
Conclusions
The results of our study suggest that a low-dose CT LVEF protocol is feasible, fast, yields similar results as RNA and can be performed with a lower radiation dose than traditional RNA.
References
Sanz G, Castaner A, Betriu A, Magrina J, Roig E, Coll S, et al. Determinants of prognosis in survivors of myocardial infarction. N Engl J Med 1982;306:1065-70.
Taylor GJ, Humphries JO, Mellits ED, Pitt B, Schulze RA, Griffith LS, et al. Predictors of clinical course, coronary anatomy and left ventricular function after recovery from acute myocardial infarction. Circulation 1980;62:960-70.
White HD, Norris RM, Brown MA, Brandt PWT, Whitlock RML, Wild CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation 1987;76:44-51.
Eagle KA, Guyton RA, Davidoff R, Edwards FH, Ewy GA, Gardner TJ, et al. ACC/AHA 2004 Guideline Update for Coronary Artery Bypass Graft Surgery: Summary Article: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). J Am Coll Cardiol 2004;44:1146-54.
Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M, et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J Am Coll Cardiol 2006;48:e247-346.
Strickberger SA, Benson DW, Biaggioni I, Callans DJ, Cohen MI, Ellenbogen KA, et al. AHA/ACCF Scientific Statement on the Evaluation of Syncope: From the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; and the American College of Cardiology Foundation In Collaboration With the Heart Rhythm Society. J Am Coll Cardiol 2006;47:473-84.
Hunt SA. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol 2005;46:e1-82.
McAlister FA, Ezekowitz J, Hooton N, Vandermeer B, Spooner C, Dryden DM, et al. Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction: A systematic review. JAMA 2007;297:2502-14.
Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr Faxon DP, Freed MD, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;52:e1-148.
Russo AM, Stainback RF, Bailey SR, Epstein AE, Heidenreich PA, Jessup M, et al. ACCF/HRS/AHA/ASE/HFSA/SCAI/SCCT/SCMR 2013 Appropriate Use Criteria for Implantable Cardioverter-Defibrillators and Cardiac Resynchronization Therapy: A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Heart Rhythm Society, American Heart Association, American Society of Echocardiography, Heart Failure Society of America, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 2013;61:1318-68.
Chow BJW, Wells GA, Chen L, Yam Y, Galiwango P, Abraham A, et al. Prognostic value of 64-slice cardiac computed tomography: Severity of coronary artery disease, coronary atherosclerosis and left ventricular ejection fraction. J Am Coll Cardiol 2010;55:1017-28.
Butler J, Shapiro MD, Jassal D, Neilan T, Nichols J, Ferencik M, et al. Comparison of multidetector computed tomography and two-dimensional transthoracic echocardiography for left ventricular assessment in patients with heart failure. Am J Cardiol 2007;99:247-9.
Dewey M, Muller M, Eddicks S, Schnapauff D, Teige F, Rutsch W, et al. Evaluation of global and regional left ventricular function with 16-slice computed tomography, biplane cineventriculography, and two-dimensional transthoracic echocardiography: Comparison with magnetic resonance imaging. J Am Coll Cardiol 2006;48:2034-44.
Henneman MM, Schuijf JD, Jukema JW, Holman ER, Lamb HJ, de Roos A, et al. Assessment of global and regional left ventricular function and volumes with 64-slice MSCT: A comparison with 2D echocardiography. J Nucl Cardiol 2006;13:480-7.
Schuijf JD, Bax JJ, Jukema JW, Lamb HJ, Salm LP, de Roos A, et al. Assessment of left ventricular volumes and ejection fraction with 16-slice multi-slice computed tomography; comparison with 2D-echocardiography. Int J Cardiol 2007;116:201-5.
Sugeng L, Mor-Avi V, Weinert L, Niel J, Ebner C, Steringer-Mascherbauer R, et al. Quantitative assessment of left ventricular size and function: Side-by-side comparison of real-time three-dimensional echocardiography and computed tomography with magnetic resonance reference. Circulation 2006;114:654-61.
Schepis T, Gaemperli O, Koepfli P, Valenta I, Strobel K, Brunner A, et al. Comparison of 64-Slice CT with Gated SPECT for Evaluation of Left Ventricular Function. J Nucl Med 2006;47:1288-94.
Henneman MM, Schuijf JD, Jukema JW, Lamb HJ, de Roos A, Dibbets P, et al. Comprehensive cardiac assessment with multislice computed tomography: Evaluation of left ventricular function and perfusion in addition to coronary anatomy in patients with previous myocardial infarction. Heart 2006;92:1779-83.
Kim IJ, Choo KS, Lee JS, Kim SJ, Kim JH, Kim YK, et al. Comparison of gated blood pool SPECT and multi-detector row computed tomography for measurements of left ventricular volumes and ejection fraction in patients with atypical chest pain: Validation with radionuclide ventriculography. Cardiology 2007;107:8-16.
Chow BJW, Abraham A, Wells GA, Chen L, Ruddy TD, Yam Y, et al. Diagnostic accuracy and impact of computed tomographic coronary angiography on utilization of invasive coronary angiography. Circ Cardiovasc Imaging 2009;2:16-23.
Abbara S, Chow BJW, Pena AJ, Cury RC, Hoffmann U, Nieman K, et al. Assessment of left ventricular function with 16- and 64- slice multi-detector computed tomography. Eur J Radiol 2008;67:481-6.
Lin FY, Devereux RB, Roman MJ, Meng J, Jow VM, Jacobs A, et al. Cardiac chamber volumes, function, and mass as determined by 64-multidetector row computed tomography: Mean values among healthy adults free of hypertension and obesity. JACC Cardiovasc Imaging 2008;1:782-6.
Beck-da-Silva L, De Bold A, Davies RA, Chow BJW, Ruddy TD, Fraser M, et al. Effect of bisoprolol on right ventricular function and brain natriuretic peptide in patients with heart failure. Congest Heart Fail 2004;10:127-32.
American Society of Nuclear Cardiology. Updated imaging guidelines for nuclear cardiology procedures, part 1. J Nucl Cardiol 2001;8:G5-58.
Chow BJW, Abunassar JG, Ascah K, deKemp R, DaSilva J, Mesana T, et al. Effects of mitral valve surgery on myocardial energetics in patients with severe mitral regurgitation. Circ Cardiovasc Imaging 2010;3:308-13.
Massardo T, Gal RA, Grenier RP, Schmidt DH. Left ventricular volume calculation using a count-based ratio method applied to multigated radionucide angiography. J Nucl Med 1990;31:450-6.
McDonald RJ, McDonald JS, Carter RE, Hartman RP, Katzberg RW, Kallmes DF, et al. Intravenous contrast material exposure is not an independent risk factor for dialysis or mortality. Radiology 2014;273:714-25.
Acknowledgments
Benjamin Chow is supported by the Saul and Edna Goldfarb Chair in Cardiac Imaging and receives research support from GE Healthcare and educational support from TeraRecon Inc. The study was funded in part by the UOHIAMO Innovations Fund.
Disclosures
No other authors have conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
See related editorial, doi:10.1007/s12350-015-0183-7.
Rights and permissions
About this article

Cite this article
Yang, Y., Yam, Y., Chen, L. et al. Assessment of left ventricular ejection fraction using low radiation dose computed tomography. J. Nucl. Cardiol. 23, 414–421 (2016). https://doi.org/10.1007/s12350-015-0123-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-015-0123-6