
Abstract
Background
Recent advances in nuclear myocardial perfusion imaging (MPI) have made it possible to develop a dual-isotope protocol for high-speed acquisition with image quality and radiation delivery comparable to that obtained with conventional single isotope protocols. So far, no study has compared dual-isotope high-speed MPI to invasive coronary angiography (ICA) in a large cohort using a Cadmium-zinc-telluride SPECT system.
Methods
Over a 1-year period (May 2011 to April 2012), 1366 patients underwent dual-isotope high-speed MPI. Patients with ICA within 3 months after dual-isotope high-speed MPI were included together with patients with a low likelihood of coronary artery disease (CAD) in order to assess normalcy rate. Global summed stress score (SSS) and summed rest score (SRS) were calculated, and ICA results were analyzed independently. The main end point was a patient-based assessment of the diagnostic performance of dual-isotope high-speed MPI in detecting or ruling out significant CAD (>70% reduction in lumen diameter).
Results
Inclusion criteria were fulfilled for 214 patients (143 men; age 60 ± 14 years; ICA, n = 104; low likelihood for CAD, n = 110). An exercise stress test was performed in 62% of patients and a pharmacological stress test was performed with either dipyridamole (32%) or dobutamine (6%). Average examination duration was 22.4 ± 4.5 minutes. Mean SSS, SRS, and SDS were 8.0 ± 4.9, 3.1 ± 4.3, and 5.0 ± 3.2, respectively. Prevalence of angiographic CAD was 75%. ICA detected stenosis in the left main trunk, left anterior descending artery, left circumflex artery, and right coronary artery in 4, 33, 31, and 42 patients, respectively. Sensitivity of dual-isotope high-speed MPI was 94%, normalcy rate was 92%, and accuracy was 83% for detecting CAD.
Conclusion
Dual-isotope high-speed MPI is reliable at detecting or ruling out CAD. NCT01785589
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cadmium-zinc-telluride (CZT) technology is a powerful new addition to the arsenal of cardiac nuclear medicine with recent clinical validation studies showing reductions in scan time1 and in the dose of radiation delivered2 without any loss in myocardial perfusion imaging quality in comparison with standard dual-detector cameras.3
The increased photon-counting sensitivity of this type of camera can be used to investigate novel protocols that may offer advantages over standard myocardial perfusion imaging (MPI) protocols. Berman et al, using a gamma D-SPECT camera, showed that a stress thallium-201/rest technetium-99m protocol with high-speed SPECT MPI combines the superiority of thallium-201 for stress imaging and that of technetium-99m agents for rest imaging.4 Therefore, the use of dual-isotope imaging is promising as it combines thallium-201 with technetium-99m agents for optimal image resolution and a simultaneous assessment of viability.
The evidence shows that nuclear medicine is highly effective in the diagnosis of coronary artery disease.5 Many studies have compared the performance of standard dual-detector cameras with invasive coronary angiography (ICA). Fiechter et al reported the first validation of ultrafast dedicated cardiac gamma camera with CZT in comparison with ICA. However, this study was conducted using a novel hybrid SPECT/CT device and a technetium-99m-tetrofosmin pharmacological stress/rest examination,6 whereas stress thallium-201/rest technetium-99m sequential dual-isotope high-speed MPI has not yet been validated in comparison with ICA in a specific study using a Discovery NM 530c camera (DNM).
Therefore, the present study reports the first validation of a high-speed dual-isotope protocol for myocardial perfusion imaging using ICA as the standard of reference.
Methods
Study Population
Patients admitted to the University Hospital of Grenoble for MPI prescribed in accordance with Appropriate Use Criteria for Cardiac Radionuclide Imaging7 were evaluated over a year from May 2011 to April 2012. Patients with acute or recent ST-segment elevation myocardial infarction (MI), unstable angina within 3 months, coronary artery bypass grafting (CABG) surgery, non-ischaemic cardiomyopathy, and severely reduced left ventricular systolic function (EF <35%) were excluded. CAD detection using the new CZT camera with stress thallium-201/Rest technetium-99m-sestamibi DI-HS-MPI was compared with ICA. A total of 1,336 successive patients with a dual-isotope high-speed MPI evaluation were considered for inclusion into this study. Among these, patients who had undergone both dual-isotope high-speed MPI and ICA within 3 months after MPI were analyzed. In addition, patients with low likelihood of CAD (<10%) were also included into this study in order to determine the normalcy rate of this new device using the dual-isotope high-speed MPI protocol. The inclusions to determine the normalcy rate were specific of design study. All were, without history of cardiac disease, and all had been recruited among volunteers who wanted to benefit from a cardiac evaluation. Written informed consent was obtained from all patients for use of their clinical and imaging data for research purposes as approved by the Institutional Review Board. The ClinicalTrials.gov identifier for this study was NCT01785589.
Imaging and Stress Protocols
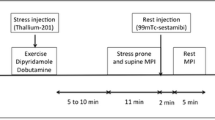
Dual-isotope high-speed MPI was performed as previously described.4 Briefly, patients were instructed to discontinue beta-blocker drugs and calcium antagonists 48 hours before testing and nitrate 24 hours before testing. A bicycle exercise stress test (stepwise increments of 25 W every 2 minutes) was performed with an injection of thallium-201 at peak stress. Exercise was continued at the same effort level for an additional 60 seconds and was eventually stopped after a 6 minutes recovery period at low resistance. A horizontal or down-sloping ST-segment depression ≥1 mm or up-sloping ≥1.5 mm was considered positive for ischemia. For dipyridamole stress testing, patients were told to avoid caffeine-containing products for 24 hours before the test. Dipyridamole (0.56 mg/kg) was infused over 4 minutes, and thallium-201 was injected between minutes 6 and minute 8 after the beginning of dipyridamole infusion. When neither exercise testing nor dipyridamole could be used, patients were given a dobutamine stress test. Intravenous dobutamine was administered at incremental doses of 5, 10, 15, 20, 25, 30, and 40 μg/kg/minutes at 3 minutes intervals. Therefore, at peak stress, patients were injected with thallium-201. Five-to-10 minutes after stress a 5-minutes supine acquisition was performed followed by a 5-minutes prone acquisition. Subsequently, technetium-99m-sestamibi was injected, and 2 minutes later a single 5-minutes rest acquisition was performed. Acquisition time was established on previous results in 38 patients, which compared performance of CZT scan to classic acquisition time of anger camera (unpublished results). The ultrafast protocol used is shown in Figure 1. During stress acquisition, patients were imaged in supine and prone positions with their arms positioned over their head. The rest acquisition was only acquired in supine position. The gated SPECT studies were performed at rest in the supine position. Injected activity (IA) was adjusted for patient weight. For weights of <80 kg/80-100 kg/>100 kg, thallium-201 IAs were 74/92/111 MBq and technetium-99m-sestamibi IAs were 300/370/450 MBq, respectively. The effective dose was calculated using ICRP 1038,9 tissue weighting factors and assumptions on the biodistribution data based on data from Krahwinkel et al and Thomas et al for thallium-201.10,11

Study protocol
CZT Camera
Ultrafast imaging was performed using a Discovery NM 530c camera (DNM, GE Healthcare) fitted with a multi-pinhole collimator and 19 stationary CZT detectors allowing the simultaneous acquisition of 19 cardiac views. Each detector consists of 32 × 32 pixelated CZT elements. All stress and rest acquisition were preceded by thorough positioning of the heart within the center of the field-of-view utilizing the real-time persistence imaging tool.
Analysis of Perfusion Images and Image Quality
Stress and rest perfusion images of high-speed SPECT were semi-quantitatively scored using a 17-segment model of the left ventricle and a 5-point scale (0 = normal, 1 = equivocal, 2 = moderate, 3 = severely reduced radiotracer uptake, and 4 = no detectable uptake) by two experienced nuclear cardiologists (AC, DF) blinded to clinical and ICA data. Discordant findings were resolved by consensus. Global summed stress score (SSS), summed rest score (SRS), and summed difference score (SDS) were calculated for the 17 segments in the stress and rest images, respectively. Scans were considered as normal when SSS was <4. Perfusion defects were assigned to coronary territories using the American Heart Association coronary arterial segment model.12 By comparing supine and prone images, defects that changed their location were considered to artifactual, while defects remaining fixed were considered to true perfusion defects. The whole of high-speed SPECT images (supine and prone imaging at stress and imaging at rest) were scored by AC and DF for image quality using a 4-point scale: 1 = excellent, 2 = good, 3 = acceptable, and 4 = unacceptable. Furthermore, in order to assess the variability of measurements (using the SSS), 20 randomly selected patients with dual-isotope high-speed MPI were evaluated twice in a random order by the same observer for intra-observer variability, and by two different observers for inter-observer variability.
Coronary Angiography
Selective conventional coronary angiography was performed using standard techniques (Philips Allura Xper FD10, Philips Healthcare). All patients were evaluated using quantitative coronary angiography (QCA [Vepro Computersysteme GmbH]) by two cardiologists (GB, EV) blinded to clinical data and the DI-HS-MPI results. Discordant findings were resolved by consensus. The standard 15-segment American Heart Association classification system was used. All coronary artery stenoses were graded in at least two orthogonal views, and the measurement was made in the projection showing the highest degree of stenosis. Significant obstructive CAD was defined by the presence of a stenosis ≥70% in one or more of the three-epicardial vessels or ≥50% in the left main coronary artery.
Normalcy Rate
The pre-scan likelihood of CAD was based on age, sex, symptoms, risk factors, and the results of the subject’s stress electrocardiogram.13 Normalcy rate was assessed in patients with a pre-scan likelihood of CAD of less than 10% by experienced nuclear cardiologists (AC, DF) blinded to clinical data. Discordant findings were resolved by consensus.
Statistical Analysis
Statistical analysis was conducted using SPSS® version 15.0 software (SPSS Inc., Chicago, Illinois, USA). All continuous variables are expressed as mean ± standard deviation. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for MPI with respect to CAD detection. Dual-isotope high-speed MPI quantification variability was quantified by computing the intra-class correlation coefficient (ICC). Inter-observer reliability for SSS measurement was assessed using two-way random single-measure ICC analysis.
Results
Population Characteristics
Clinical characteristics are listed in Table 1. For the ICA population, mean age was 65 ± 12 years [34-88] and 70% were men. The main cardiovascular risk factors were hypertension and dyslipidemia. Fifty one percent of patients presented with previously known CAD. Dual-isotope high-speed MPI was mainly performed in symptomatic patients (95%) presenting with typical angina pectoris, atypical chest pain, or dyspnea, but also in asymptomatic patients either for evaluation prior to vascular surgery (3%) or because of an elevated CAD risk (2%). Exercise testing was performed in 65 patients (62%), whereas pharmacological stress testing with dipyridamole or dobutamine was performed in 33 (32%) and 6 (6%) patients, respectively. Four patients presented left bundle branch block (LBBB) and 5 patients had a pacemaker. The mean injected dose of thallium-201 during stress was 82 ± 19 MBq (range 68-115 MBq) and the mean injected dose of technetium-99m-sestamibi at rest was 314 ± 41 MBq (range 265-457 MBq). The DI-HS-MPI protocol was completed in 22.4 ± 4.5 minutes [18-27]. One hundred percent of the MPI were ranked as being of either good or excellent in quality. In addition, intra-observer and inter-observer reproducibilities were high for SSS: ICC = 0.97 [95% CI 0.92-0.98] and 0.92 [95% CI 0.82-0.97], respectively. Mean SSS, SRS, and SDS were 8.0 ± 4.9, 3.1 ± 4.3, and 5.0 ± 3.2, respectively. Seventeen patients had a normal scan, whereas MPI was found to be mildly, moderately, or severely abnormal in 42, 30, and 15 patients, respectively. Among these abnormal scans, 35 patients presented entirely reversible ischemia and 52 patients had both reversible ischemia and fixed hypoperfusion. Finally, dual-isotope high-speed MPI was found to be normal in 101 out of 110 patients with a low (<10%) likelihood of CAD (normalcy rate = 92%). Clinical characteristics are listed in Table 2.
According to ICA, the prevalence of CAD was 75%. Among the 78 patients with CAD, 49 (63%) had single-vessel disease, 24 (31%) had 2-vessel disease, and 5 (6%) had 3-vessel disease. Among the 75 patients with single or 2-vessel disease, 33 showed significant stenosis of the left anterior descending (LAD) artery, 31 had significant stenosis of the left circumflex artery (LCx), 42 had significant stenosis of the right coronary artery (RCA), and 4 had significant coronary stenosis in the left main coronary artery.
Comparison Between Dual-Isotope High-Speed MPI and ICA
Diagnostic performance of dual-isotope high-speed MPI over ICA for the detection of CAD in the per-patient analysis was: sensitivity 94%; specificity 50%; PPV 85%; NPV 76%; and accuracy 83% (Figure 2). ROC curve analysis was performed using SSS from the quantitative assessment of stress perfusion (Figure 3). The area under the curve for SSS, SRS, and SDS with dual-isotope high-speed MPI were 0.88 (95% CI 0.80-0.96), 0.67 (95% CI 0.56-0.78), and 0.81 (95% CI 0.72-0.90), respectively. Figure 4 shows a typical inferior perfusion defect at stress using the dual-isotope high-speed MPI protocol in a 53-year-old man with significant stenosis of the right coronary artery as determined by ICA. According to stenosis distribution, AUCs were 0.88, 0.87, and 0.90 for the LAD, LCx, and RCA, respectively (Figure 5). The estimated radiation dose for dual-isotope high-speed MPI was of 12.0 ± 0.9 mSv.

DI-HS-MPI in the diagnosis of significant obstructive coronary artery stenosis. The numbers of true positives, false positives, true negatives, and false negatives were 74, 13, 13, and 4, respectively

ROC curve derived from combined supine and prone summed stress scores (SSS), summed rest scores (SRS), and summed difference scores (SDS)

Dual-isotope high-speed myocardial perfusion imaging (left panel) showing inferior ischemia and corresponding invasive coronary angiography showing stenosis of the right coronary artery (right panel)

ROC curves for the per-vessel qualitative analysis of DI-HS-MPI. For each SSS cut-off point, the curves represent the pair of sensitivity-specificity values
Discussion
This study investigates for the first time the accuracy of a dual stress thallium-rest technetium-99m Sequential DI-HS-MPI using a DNM SPECT system for the detection of CAD assessed by invasive coronary angiography. Dual-isotope high-speed MPI demonstrated high sensitivity and accuracy for the detection of CAD and significant time gain.
The possibility of performing a dual-isotope thallium-201 stress/rest technetium-99m protocol using a conventional three-detector Anger camera was proposed in 2008 by Steele et al14 However, cameras based on CZT detector technology such as the D-SPECT and the DNM recently became available with improved characteristics over standard cameras. D-SPECT and DNM have more detectors and each is more efficient, making it possible to return to dual-isotope protocols.
A first successful translation of dual-isotope protocol to this new generation of camera has been reported by Berman et al who used a gamma D-SPECT camera.4 Here we show that this type of protocol can be performed with the second CZT camera, the DNM. Like Berman et al, we show that immediate imaging after rest technetium-99m tracer injection is possible and offers high image quality without significant hepatic interference using the DNM camera, as previously reported with the D-SPECT camera.
The use of a dual-isotope protocol affords several advantages. Thallium-201 is the most appropriate tracer for myocardial perfusion, with a first pass extraction fraction of 85%.15,16 In comparison with sestamibi or tetrofosmin, this enhances the detection of mild coronary stenosis. In comparison, sestamibi is a less efficient tracer for stress imaging (extraction fraction: 65%) although it has been shown to be suitable for determining myocardial viability at rest.17 Reduced imaging time presents several advantages. In addition to reducing patient discomfort, sources of error associated with separate image acquisitions are reduced, and it makes it possible to record in both the supine and the prone positions: this helps when it comes to distinguishing a true perfusion defect from an artifact due to attenuation or patient motion. Moreover, the design of the DNM camera is compatible with a real prone position, unlike with the D-SPECT camera. Thallium stress imaging must be performed quite rapidly following injection in order to prevent redistribution. Consequently, considering the dual-isotope protocol acquisition time, stress tests can be performed every 25 minutes. Therefore, the protocol successfully reduced the length of the procedure for patients, but also required a specific organization inside the nuclear medicine department.
Other studies aimed at comparing CZT SPECT MPI to coronary angiography have been reported before,6,18-24 but the present study investigates for the first time the use of a dual-isotope protocol in a cohort using a DNM SPECT system. Nakazato et al performed dual-isotope Stress thallium-201-rest technetium-99m-sestamibi on patients who underwent diagnostic ICA within 6 months. However, the dual-isotope protocol was only carried out in a subgroup of 17 patients out of a cohort of 142 and a D-SPECT camera was used19 so it is difficult to assess the real performance of dual-isotope protocols from this data. It is difficult to compare the results of these studies because of differences in inclusion and exclusion criteria as well as in the prevalence of CAD. However, the overall performance for detection of CAD in the present study was similar to that reported by others using single isotope protocols in comparison with coronary angiography.6,18-24 The low specificity that was observed in this study is probably due to the study design and the high prevalence of CAD. Referral bias (i.e., performing coronary angiography based on clinical indication and selected patients rather than based on the sole MPI results) is known to significantly alter specificity of MPI, with values as low as 37% as reported by Duvall et al20 This limitation is countered by use of the normalcy rate. A high rate of false-positive results can also be explained by two others elements. Although the level of concordance between conventional SPECT and invasive fractional flow reserve (FFR) measurement has been studied, the level of concordance between FFR and CZT-based SPECT is not yet well known. Moreover, the improved spatial resolution of CZT detectors together with the use of thallium-201 during stress might result in improved visualization of perfusion defects due to endothelial dysfunction without any significant CAD by IA. Indeed, myocardial ischaemia may occur in the absence of overt atherosclerotic diseases in the epicardial coronary vessels demonstrable by coronary angiography. Myocardial ischaemia in these settings is often associated with abnormalities of the coronary microcirculation. These elements might in turn further affect the specificity of this device. Further studies including the measurement of FFR, coronary flow reserve and index of coronary microcirculation dysfunction will be necessary to complete dual-isotope protocol data. The other element is that DNM system acquires MPI without movement of the detectors and reduction of artifacts due to patient motion during acquisition should result in higher values for specificity (fewer false positives). However, recent work shows that the relatively few number of detector places higher demands on requirements for precise positioning of the heart within the center of the field-of-view. A suboptimal patient positioning leads count loss and false positive myocardial perfusion SPECT studies.25 So, for example, protocol could be improved by placing point source markers on the patient’s skin to facilitate repositioning. Because DNM has this limit, it could be even more desirable to avoid repositioning the patient between stress and rest, and others studies will be necessary to determined the real source of the benefit offered by prone imaging. Probably to minimizing the repositioning and patient motion problems, simultaneous multi-isotope is the better solution. However, CZT-systems have ever demonstrated the capability to simultaneously image thallium-201 and technetium-99m in clinical application to MPI, which had been shown with gamma cameras equipped with sodium iodide detectors and Multi-Pinhole SPECT system.14 This technical limitation is due to spectral distortion when CZT is pixelated into a rectangular grid to create high resolution large area detectors for medical imaging. The gaps that are created between the CZT pixel elements provide an edge region in which incident photons do not completely interact resulting in “spectral down-shifting” of the energy detected from these partially interacted primary photons. This phenomenon is also termed charge sharing.26 This makes difficult to perform scatter and cross talk correction to separate thallium-201 and technetium-99m peak.
It is worth noting that the AUC of 0.88 found for the population as a whole did not vary according to the territory of stenosis: this can be attributed to the reduction of attenuation artifacts and improved spatial resolution for the LCx and RCA territories. The performance of dual-isotope high-speed MPI in the diagnosis of CAD has been evaluated in the present study. Nevertheless, further studies will be required to assess the long-term prognostic value of this new modality in a large population. Because CZT cameras have been designed to provide better spatial resolution and sensitivity than the Anger camera, such studies will be needed to confirm previously reported prognostic data27 as well as to investigate the usefulness of dual-isotope protocols.
Clinical Implication
Dual-isotope high-speed MPI affords rapid, reliable evaluation of myocardial ischemia with both prone and supine post-stress images acquired in less than 30 minutes. Fast, reliable examination techniques are of particular relevance in the chest pain unit. Current guidelines recommend nuclear imaging in patients with acute chest pain, no ischemic ECG changes and negative peak troponin levels.28 In this context, normal coronary computed tomography angiography (CCTA) could exclude CAD29 but, although this examination provides anatomical information, it does not detect ischemia. The evaluation of ischemia directly impacts on medical care and provides additive prognostic value.27 In consequence, the increasing availability of CZT cameras will provide important ischemia-related prognostic information.
Limitations
The study was conducted at a single site and the sample size was relatively small. High prevalence of angiographic CAD has biased the results in favor of the technique being analyzed. The principal limit of our study is the impact of verification bias on our results. Indeed, 84% of the population had abnormal images, which results in marked inflation of the derived values for sensitivity and accuracy, since the number of true positive tests will greatly exceed the number of both true negative and false negative test results. Coronary angiograms were performed for clinical indications on selected patients rather than on all patients. Hence, as in other studies, the normalcy rate determined from patients with a low probability of CAD was found to be high. However, this is the first clinical study with largest cohort, which compares Stress thallium-201/Rest technetium-99m Sequential dual-isotope high-speed MPI vs ICA for detection of CAD. Our study highlights the value of assessing the performance of dual-isotope high-speed MPI in current clinical practice. A large number of intermediate-to-high-risk stable patients were included in agreement with current guidelines; neither patients with a history of CAD or left bundle branch block nor those with an implanted pacemaker were excluded. We show that dual-isotope high-speed MPI is reliable at detecting or ruling out CAD. In our study, coronary angiography was used as the gold standard but the correlation between anatomical stenosis and myocardial ischemia has been reported as being imperfect.30 Another limitation was the fact that the present study focused on ischemia and left ventricular ejection fraction at stress was not determined. The early injection of MIBI after stress without the use of nitrates could be associated to an underestimation of myocardial viability. Probably, the usefulness of dual-isotope protocols with CZT camera to investigate viability must be validated in comparison to gold-standard test for viability.
It is desirable to develop new protocols for high efficiency cameras. However, the goal should be not only a fast test but also a safe and low radiation test. Indeed, protocols can be developed which take longer but in which the overall dose delivered is lower, rather than an ultra-fast protocol as described in this study.21 The new CZT gamma cameras should thus make it possible to match the protocol used to the patient’s morphology and the clinical picture to deliver the lowest possible dose of radiation in line with international recommendations.31 Our protocol could be tailored to a pre-specified group of patients in whom benefit exceeds the risk (such as older patients with known CAD). Moreover, optimization is possible with reviewed of stress images prior to technetium-99m injection. If normal, less radiation and a shorter test could be offered.
New Knowledge Gained
This is the first clinical study, which compares stress thallium-201/rest technetium-99m sequential dual-isotope high-speed MPI vs ICA for detection of CAD. Dual-isotope high-speed MPI showed high sensitivity and accuracy with a far shorter imaging time. The limits of the protocol were also shown with low specificity and radiation exposure not optimal. But our study is a step toward better utilization of DNM system.
Conclusion
Dual-isotope high-speed MPI is reliable at detecting or ruling out CAD.
References
Herzog BA, Buechel RR, Katz R, Brueckner M, Husmann L, Burger IA, et al. Nuclear myocardial perfusion imaging with a cadmium-zinc-telluride detector technique: Optimized protocol for scan time reduction. J Nucl Med 2010;51:46-51.
Nkoulou R, Pazhenkottil AP, Kuest SM, Ghadri JR, Wolfrum M, Husmann L, et al. Semiconductor detectors allow low-dose-low-dose 1-day SPECT myocardial perfusion imaging. J Nucl Med 2011;52:1204-9.
Esteves FP, Raggi P, Folks RD, Keidar Z, Askew JW, Rispler S, et al. Novel solid-state-detector dedicated cardiac camera for fast myocardial perfusion imaging: Multicenter comparison with standard dual detector cameras. J Nucl Cardiol 2009;16:927-34.
Berman DS, Kang X, Tamarappoo B, Wolak A, Hayes SW, Nakazato R, et al. Stress thallium-201/rest technetium-99m sequential dual isotope high-speed myocardial perfusion imaging. JACC Cardiovasc Imaging 2009;2:273-82.
Underwood SR, Anagnostopoulos C, Cerqueira M, Ell PJ, Flint EJ, Harbinson M, et al. Myocardial perfusion scintigraphy: The evidence. Eur J Nucl Med Mol Imaging 2004;31:261-91.
Fiechter M, Ghadri JR, Kuest SM, Pazhenkottil AP, Wolfrum M, Nkoulou RN, et al. Nuclear myocardial perfusion imaging with a novel cadmium-zinc-telluride detector SPECT/CT device: First validation versus invasive coronary angiography. Eur J Nucl Med Mol Imaging 2011;38:2025-30.
Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin RE, Pellikka PA, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 Appropriate use criteria for cardiac radionuclide imaging: A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. J Am Coll Cardiol 2009;53:2201-29.
Valentin J. Radiation dose to patients from radiopharmaceuticals (addendum 2 to ICRP publication 53) ICRP publication 80. Ann ICRP 1998;28:1-126.
Radiation dose to patients from radiopharmaceuticals. A report of a Task Group of Committees 2 and 3 of the International Commission on Radiological Protection. Addendum 5 to ICRP Publication 53 (2001). http://www.icrp.org/docs/Add_5-7_to_P53.pdf. Accessed 8 Aug 2008.
Krahwinkel W, Herzog H, Feinendegen LE. Pharmacokinetics of thallium-201 in normal individuals after routine myocardial scintigraphy. J Nucl Med 1988;29:1582-6.
Thomas SR, Stabin MG, Castronovo FP. Radiation-absorbed dose from 201Tl-thallous chloride. J Nucl Med 2005;46:502-8.
Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002;105:539-42.
Gibbons RJ, Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, Froelicher VF, et al. ACC/AHA 2002 guideline update for exercise testing: Summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the Exercise Testing Guidelines). J Am Coll Cardiol 1997;2002(40):1531-40.
Steele PP, Kirch DL, Koss JE. Comparison of simultaneous dual-isotope multipinhole SPECT with rotational SPECT in a group of patients with coronary artery disease. J Nucl Med 2008;49:1080-9.
Salerno M, Beller GA. Noninvasive assessment of myocardial perfusion. Circ Cardiovasc Imaging 2009;2:412-24.
Leppo JA, Meerdink DJ. Comparison of the myocardial uptake of a technetium-labeled isonitrile analogue and thallium. Circ Res 1989;65:632-9.
Udelson JE, Coleman PS, Metherall J, Pandian NG, Gomez AR, Griffith JL, et al. Predicting recovery of severe regional ventricular dysfunction. Comparison of resting scintigraphy with 201Tl and 99mTc-sestamibi. Circulation 1994;89:2552-61.
Duvall WL, Sweeny JM, Croft LB, Ginsberg E, Guma KA, Henzlova MJ. Reduced stress dose with rapid acquisition CZT SPECT MPI in a non-obese clinical population: Comparison to coronary angiography. J Nucl Cardiol 2012;19:19-27.
Nakazato R, Tamarappoo BK, Kang X, Wolak A, Kite F, Hayes SW, et al. Quantitative upright-supine high-speed SPECT myocardial perfusion imaging for detection of coronary artery disease: Correlation with invasive coronary angiography. J Nucl Med 2010;51:1724-31.
Duvall WL, Sweeny JM, Croft LB, Barghash MH, Kulkarni NK, Guma KA, et al. Comparison of high efficiency CZT SPECT MPI to coronary angiography. J Nucl Cardiol 2011;18:595-604.
Gimelli A, Bottai M, Genovesi D, Giorgetti A, Di Martino F, Marzullo P. High diagnostic accuracy of low-dose gated-SPECT with solid-state ultrafast detectors: Preliminary clinical results. Eur J Nucl Med Mol Imaging 2012;39:83-90.
Neill J, Prvulovich EM, Fish MB, Berman DS, Slomka PJ, Sharir T, et al. Initial multicentre experience of high-speed myocardial perfusion imaging: Comparison between high-speed and conventional single-photon emission computed tomography with angiographic validation. Eur J Nucl Med Mol Imaging 2013;40:1084-94.
Gimelli A, Bottai M, Quaranta A, Giorgetti A, Genovesi D, Marzullo P. Gender differences in the evaluation of coronary artery disease with a cadmium-zinc telluride camera. Eur J Nucl Med Mol Imaging 2013;40:1542-8.
Duvall WL, Slomka PJ, Gerlach JR, Sweeny JM, Baber U, Croft LB, et al. High-efficiency SPECT MPI: Comparison of automated quantification, visual interpretation, and coronary angiography. J Nucl Cardiol 2013;20:763-73.
Hindorf C, Oddstig J, Hedeer F, Hansson MJ, Jögi J, Engblom H. Importance of correct patient positioning in myocardial perfusion SPECT when using a CZT camera. J Nucl Cardiol 2014;21:695-702.
Kim JC, Anderson S, Kaye W, Zhang F, Zhu Y, Kaye SJ, et al. Charge sharing in common-grid pixelated CdZnTe detectors. Nucl Instrum Methods Phys Res A 2011;654:233-43.
Machecourt J, Longère P, Fagret D, Vanzetto G, Wolf JE, Polidori C, et al. Prognostic value of thallium-201 single-photon emission computed tomographic myocardial perfusion imaging according to extent of myocardial defect. Study in 1,926 patients with follow-up at 33 months. J Am Coll Cardiol 1994;23:1096-106.
Jneid H, Anderson JL, Wright RS, Adams CD, Bridges CR, Casey DE Jr, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non-ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update): A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2012;60:645-81.
Hoffmann U, Bamberg F, Chae CU, Nichols JH, Rogers IS, Seneviratne SK, et al. Coronary computed tomography angiography for early triage of patients with acute chest pain: The ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trial. J Am Coll Cardiol 2009;53:1642-50.
Tonino PA, Fearon WF, De Bruyne B, Oldroyd KG, Leesar MA, Ver Lee PN, et al. Angiographic versus functional severity of coronary artery stenoses in the FAME study fractional flow reserve versus angiography in multivessel evaluation. J Am Coll Cardiol 2010;55:2816-21.
Cerqueira MD, Allman KC, Ficaro EP, Hansen CL, Nichols KJ, Thompson RC, et al. Recommendations for reducing radiation exposure in myocardial perfusion imaging. J Nucl Cardiol 2010;17:709-18.
Conflict of interest
The authors have indicated that they have no financial conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Barone-Rochette, G., Leclere, M., Calizzano, A. et al. Stress thallium-201/rest technetium-99m sequential dual-isotope high-speed myocardial perfusion imaging validation versus invasive coronary angiography. J. Nucl. Cardiol. 22, 513–522 (2015). https://doi.org/10.1007/s12350-014-0016-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-014-0016-0