
Abstract
New roles have been discovered for the adipose mass/tissue of obese subjects linked to the production of different cytokines, leptin and oxidative stress, all together playing a crucial role in developing obesity, insulin resistance, metabolic syndrome, and the pathogenesis of various diseases. Inflammatory status and plasma oxidative stress have been reported as also characterizing a new metabolic condition known as normal-weight obese (NWO) syndrome observed in women with normal index but fat mass (FM) >30%. The aim of the present study was to investigate in NWO women, compared with preobese-obese (OB) and control normal weight (NW) subjects, the occurrence of DNA damage, particularly oxidative DNA damage, by using different Comet assay versions. Our goal was to find out some possible new early hallmarks of obesity. We observed above all increase in DNA damage both in OB and NWO women, compared with NW subjects, underlining DNA to be involved in oxidative stress related to metabolic abnormalities occurring in obesity. In addition, the use of either pH >13 versus pH 12.1 alkaline Comet assay versions or pH 12.1 in presence of Fpg enzyme versus pH 12.1 alone, allow us to draw attention to two possible new early differentiated hallmarks: first, alkali labile sites higher in OB compared to NWO; second, 8-oxo-dG level slightly higher in NWO than in OB women. These preliminary results encourage planning broad cohort studies in order to verify and validate these hypothesized predictive/prognostic new hallmarks.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In recent years the adipose tissue, due to its pleiotropic functions, has assumed a constantly growing metabolic relevance. It is being recognized not only as a depot for energy storage, but a kind of endocrine secretory organ, adipose organ, releasing bioactive substances, so-called adipokines or adipocytokines, with a crucial role in controlling both energy intake and expenditure as well as insulin sensitivity [1, 2]. The adipocytes, by means of numerous secretory products, link obesity to severe metabolic disorders, including “insulin resistance” disease, diabetes mellitus, hyper-lipidemia, cardiovascular diseases and cancer initiation/progression [3–6]. The increase of adipocytokines and pro-inflammatory factors, such as tumour necrosis factor (TNF-α), interleukins IL-1α,β, IL6, IL10 and IL15 [6–8], and promotion of chronic oxidative stress (ROS and RNS) with an increase in mitochondrial dysfunction and deregulation of redox-regulating enzymes, have been indeed demonstrated to play a crucial role in the onset of the major obesity-related co-morbidities [9–15].
Recently some authors [16, 17] have identified and studied in women with normal weight and body mass index, but fat mass (FM) >30%, a new so-called normal-weight obese (NWO) syndrome, in which the concentrations of plasma pro-inflammatory cytokine and oxidative stress markers were higher than in non-obese women.
Nevertheless, the pathogenesis of obesity and its link with oxidative stress, as cornerstone of the obesity-related metabolic mechanism, remain controversial [18] and additional data may be useful also to find new early hallmarks.
Daily a variety of endogenous, exogenous or environmental factors including lifestyle, exercise and diet, induce cellular oxidative stress with formation of ROS/RNS, in turn damaging vital cellular macromolecules, lipids, proteins and genomic/mitochondrial DNA, mainly considered elective targets of the radical species [15, 19]. This insult can modify the structural properties of DNA, inducing mismatched base pairs, base adducts and cross-links formation, deamination, base deletions causing apurinic/apyrimidinic (AP-alkali-labile sites) sites, single-strand breaks (SSBs), and double-strand breaks (DSBs). The most abundant ROS-induced DNA lesion is the highly mutagenic 8-OHdG, whose estimated steady-state is about 103 per cell/per day in normal tissues and up to 105 lesions per cell/per day in cancer tissues, therefore widely used as biomarker of oxidative stress and carcinogenesis [20–23].
As consequence it is important to investigate the presence of oxidative DNA damage in obese people in whom the presence of oxidative stress has been widely demonstrated [16–18], in order to discover new early biomarkers/indicators of pre-obesity/obesity condition and to design preventive interventions according to individual behaviours and life histories. Among the different approaches used to study DNA damage, the single cell gel electrophoresis (Comet assay) assay is a technically simple and fast method to quantify, both in vivo and in vitro, different types and levels of DNA damage in single cells [23–26] and in particular early damage to genomic DNA. Comet assay is different from other experimental approaches, usually capable of detecting DNA damage at a late stage of the disease, e.g. chromosome aberrations and micronucleus or TUNEL test and others methods [27].
The present research was designed to examine the occurrence of different types of DNA damage in blood cells of NWO and OB women, compared with control non-obese (NW). Different versions of Comet assay were used to identify the presence of alkali labile sites (alkaline pH >13 buffer vs. pH 12.1 buffer) and/or oxidative DNA damage (Fpg-modified version) [27–29].
Methods
Subject characteristics
The study was performed on three groups (20 subjects per group) of white Italian women, aged 25–35: control healthy non-obese (normal weight and BMI <25 kg/m2), NWO (normal weight, BMI < 25 kg/m2; FM% > 30%) and OB (BMI >25 kg/m2; FM% >30%), previously selected as in the study of Di Rienzo et al. [17].
All of the women signed an informed consensus form to participate in the study approved by the medical Ethical Committee of “Tor Vergata” University of Rome, Italy.
Cellular system
Venus heparinised whole blood cells, mainly representative of the body status, were chosen to avoid any DNA damage related to the separation of cellular types [30].
Comet assay
Blood heparinised samples (50 μl) taken from each donor were added to 950 μl of solution A (Ca2+/Mg2+-free HBSS, 20 mM EDTA, 10% DMSO, pH 7.5–7.7). The suspension was maintained at 4 °C for up to 1 h and centrifuged at 600×g 10 min; the pellet, after washing in PBS1X, was aliquoted (10 μl containing 1–1.5 × 105 cells) and stored at −80 °C for up to 10 days.
Standard Comet assay was performed utilizing Trevigen (Trevigen Inc., Gaithersburg, USA) pre-treated slides. For each group the aliquots of blood cells were embedded in 45 μl of low melting agarose (stabilized at 40 °C), dropped on the slides and maintained at 4 °C for 20 min. Then all the gel-supporting slides were immersed in lysis buffer (2.5 NaCl, 100 mM Na2EDTA, 1% Triton X100, 1% N-laurosyl sarcosine, 10% DMSO, pH = 10) for 1 h at 4 °C, in order to leave gel-embedded DNA in the form of nucleoids. DNA unwinding was left for 20 min in fresh electrophoresis buffer A (300 mM NaOH, 1 mM Na2EDTA, pH = 13.1), afterwards, alkaline version of Comet assay was performed by submarine electrophoresis in the same re-circulating pH 13.1 buffer A at 0.7 V/cm for 20 min and constant temp. (4 °C), as already reported [26]. The standard pH 13.1 alkaline version values subtracted from alkaline pH 12.1 version values, allow measurement of alkali-labile site-induced breaks.
The analysis of 8-OHdG was performed using an Fpg FLARE™ assay kit (Trevigen Inc., Gaithersburg, USA), according to the protocol provided by the manufacturer. Cell suspension (45 μl of agarose-embedded whole blood cells) was dropped on two different slides, marked a and b, respectively. After 20 min at 4 °C, slides were immersed in a pre-chilled lyses solution (provided with the FLARETM assay kit), at 4 °C for 60 min. According to manufacturer instructions, after lysis, the samples were incubated with 100 μl of either Fpg-enzyme (a), previously diluted to 1:40 with REC dilution buffer, or enzyme buffer alone (b), and then placed in a chamber at 37 °C for 45 min. After lysis and removal of proteins the “naked DNA” (or nucleoid) is in an ideal state for bacterial DNA repair enzyme attack, useful to mainly recognize and measure the sites corresponding to guanine oxidized bases. After being immersed twice for 15 min in pre-chilled alkaline electrophoresis solution (0.3 M NaOH, 1 mM Na2EDTA; pH 12.1), the slides were electrophoresed at 0.7 V/cm for 20 min.
The samples, regardless of the electrophoresis conditions, after the neutralisation treatment were 70% ethanol dried and stained with SYBER GREEN (Trevigen kit) according to protocol suggestions. One hundred nucleoids per sample (50 for each of the two replicate slides) were randomly analysed using the Leica epifluorescence microscope; the analysis did not include the lateral parts of the gel, the edges, superimposed comets and comets without distinct head (“clouds”, “hedgehogs”, or “ghost cells”). All the operations were kept in the dark.
The most important steps of different Comet assay versions were developed according to “reference conditions” suggested by Collins et al. [31]. The DNA damage was quantified by CASP free software utilizing as values the percentage of fragmented DNA in the tail of comet (%TDNA). In addition, in order to relate DNA damage to break frequencies the %TDNA values were converted in DNA break/109 Da/Gy standard units obtained through an indirect calibration according to Collins et al. [31], considering DNA breaking ability of X-rays that is known in terms of DNA break/109 Da/Gy [29]. In the case of 8-OHdG measurement the %TDNA data were expressed also as number of oxidized bases, breaks/106 bp (altered bases/106 unaltered bases) [29].
The data are averaged from three different experiments in which each sample was processed in duplicate.
Statistical analysis
Results were expressed as media values ± SEM. Differences in %TDNA between control and OB or control and NWO subjects were assessed by Student’s t test and chi-square test. Differences in %TDNA between Fpg and buffer-treated samples were tested using the Mann–Whitney U test.
Results
For each group examined, the values obtained from the samples tested by standard alkaline pH >13 Comet assay, compared with the data obtained from the same samples examined by the pH 12.1 buffer version of the assay are reported in Table 1. The results clearly evidence a significant increase in DNA damage in both NWO and OB, with respect to the control, the damage being moderately higher in OB than in NWO, at least when alkaline pH 13.1 electrophoresis data were examined. For each group, the comparative analysis of the data, enables us to highlight the presence of alkali-labile sites that are measurable mainly by pH >13 version. In fact, we did not observe significant difference, under our experimental conditions, both in NWO and control NW samples, among the values obtained after alkaline pH 13.1 and pH 12.1 electrophoresis. Conversely, in OB subjects an increase in DNA damage was evident after pH 13.1 standard alkaline electrophoresis with respect to the %TDNA measured after pH 12.1 electrophoresis, focusing on a possible main presence of alkali labile sites in these individuals.
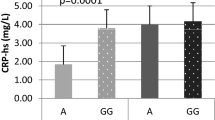
In Table 2 are reported the results of the oxidative DNA damage measured, as level of 8-OHdG, in blood cells added either with Trevigen kit supplied enzyme buffer or with DNA repair Fpg enzyme and processed with pH 12.1 alkaline buffer.
The %TDNA of Fpg enzyme-treated samples with respect to the enzyme buffer treated alone are representative, in each group of samples, of the level of 8-OHdG, the principal substrate of Fpg.
The results obtained by the Fpg-modified version of the Comet assay show an increase in the level of 8-OHdG both in NWO and OB individuals, compared to the NW. The oxidative DNA damage was slightly higher in NWO than in OB subjects.
In addition, in Tables 1 and 2 the data expressed as frequency of breaks/109 Da, on one hand confirm the growing trend in DNA damage from NWO to OB, with respect to NW and, on the other hand, reinforce the concept of a highest damage, measured by pH >13 versus pH 12.1 electrophoresis buffer, in OB with respect to NWO.
In the case of base oxidation measurement (Table 2) the data expressed also as number of oxidized bases, breaks/106 bp or altered bases/106 unaltered bases [29], point out the increase in Fpg sites in NWO with respect to OB.
Discussion
Recent dramatic changes in the dietary habits, physical activities and lifestyle of American and European people, has led to a growth in the prevalence of being overweight in comparison to just a few decades ago, increasing, as consequence, the interest in evolutionary models of human obesity. The importance of the “energy gap”, as the difference in the amount of consumed/expended calories, in influencing obesity, as well as the involvement of inflammation and oxidative stress in obesity and in the newly classified NWO syndrome have been widely discussed [11, 14, 16, 17, 32]. So, a fundamental role has been attributed to hyperglycemia, mitochondrial dysfunction, deregulation of redox-regulating enzymes [12–15, 19], even if the effects of the possible oxidative stress contributors may be different depending on the degree of obesity and of individual physical and metabolic conditions [33].
In particular, Musaad and Haynes [5] have suggested the existence, in obese subjects, of an inflammation–oxidative stress vicious circle in which oxidative stress increases the production of adipocytokine promoting inflammation. Coppak et al. [7] have suggested that the presence of excessive adiposity per se is a source of increased oxidative stress, as adipocytes and pre-adipocytes markedly produce inflammatory adipocytokines, which stimulate ROS/RNS production and up-regulate the activity of oxidant generating enzymes. Recently, some authors [16, 17] have reported in NWO, rather than in OB women, the presence of an elevated plasma cytokine level accompanied by an increase in some markers of oxidative stress, stressing that the vicious circle could be initiated in NWO before the onset of metabolic syndrome. However, in studying the sequence of events linking oxidative stress and obesity, hoping to discover new predictive biomarkers or prognostic indicators, little attention was paid to oxidants-induced DNA damage.
The hydroxyl radical produced by various oxidative mechanisms, attacks genomic and mitochondrial DNA strands, leading to the generation of a diversity of oxidation products. The interaction of OH· with nucleobases of DNA strand, such as guanine, lead to formation of 8-OHdG, the most abundant base oxidation product found in DNA, usually considered as pre-mutagenic insult [23, 27], and contributing, as a vicious circle, greatly in promoting/exacerbating different types of oxidative stress-related diseases, such as aging, malignant tumours and neurodegenerative diseases [9–12, 14, 15, 23]. The 8-OHdG lesion is one of the most important injury detected by the Fpg protein and the most commonly used biomarker for oxidative DNA. The lesion may be measured also by high-pressure liquid chromatography (HPLC) coupled to electrochemical detection, but the measurement by Fpg-modified Comet assay is currently utilized and considered as a precise, easy, economical and practicable method, compared to other approaches; also considering the little chance for spurious oxidation of guanine to occur in Comet assay [27, 29, 35].
A relationship between increased fat mass and DNA damage has been verified in dogs [34] and in a population from Pakistan too. This points out the need to develop therapeutic strategies aimed at reducing oxidative stress in obesity-predisposed subjects before they arise in the metabolic syndrome [36].
Our work, for the first time to our knowledge, investigates the relationship between obesity and different types of DNA damage in NWO and OB using different Comet assay versions as valid approaches to discriminate among several DNA lesions including SSBs, DSBs, adducts formation and alkali-labile sites (AP sites), and, in particular, based on early DNA damage [25, 27]. In a previous study Demirbag et al. [37] using alkaline Comet assay have demonstrated an increase in DNA damage in obese patients with respect to non-obese ones, stating that the obesity may be considered as a risk factor independent of DNA damage. Our results above all confirm the existence of an increase in DNA damage in both NWO and OB women, with respect to control subjects, probably sustained by inflammatory status too. The observed moderate increase in site alkali labile sites in the OB group compared to NWO women (pH 13.1 buffer electrophoresis vs. pH 12.1), as reported in Table 1, could be linked to the exacerbated oxidative stress and inflammatory conditions present in OB, preobese–obese subjects. The additional AP sites, generated by the OB metabolic abnormalities may represent an early DNA damage in a pre-metabolic syndrome condition; in addition it must be considered that AP, if not repaired, may be converted into highly damaging DSBs [25, 27].
In particular, the increase in 8-OHdG level also when expressed as altered bases/106 unaltered bases, 8-OHdG/106 dG, in NWO and OB with respect to NW and particularly in NWO with respect to OB, allows us to confirm the involvement of DNA molecules as target of the oxidative insult, and to hypothesize that the oxidative level of DNA damage in NWO could be taken into account as a hallmark predictive of obesity in the presence of low or normal BMI.
The data we reported support the results of Di Renzo et al. [17], indicating that the inflammatory and concomitant oxidative stress conditions present in NWO and OB may be considered responsible for DNA damage. In addition, we theorize that: (1) the presence of augmented AP sites in OB women, with respect to NWO, could be considered as a prognostic differential indicator between the two conditions, NWO and OB; (2) the presence of oxidative DNA damage in NWO could be considered an early event in promoting obesity and metabolic syndrome in the presence of low levels of BMI.
Our data put forward the importance to monitor the redox status and suggest a change in lifestyle and eating habits in NWO individuals other than OB, in order to counteract the rising damage [17, 38]. In fact, it cannot be excluded that the presence of oxidative stress in NWO and OB could also result from an imbalance between endogenous production of ROS/NOS and reduced intake of dietary antioxidants, as notoriously obese individuals have a lower intake of phytochemical-rich foods, lower levels of plasma dietary antioxidants (β-carotene, vitamins E and C) and of trace minerals (co-factors for antioxidant enzymes zinc, selenium), when compared with non-obese persons [38, 39].
It is clear however, that to strengthen our assumptions about biomarkers and apply them as tools in risk assessment of differently caused diseases, board cohort studies and proper validation, involving different laboratories having the same goal in mind, are required.
References
Cinti S (2005) The adipose organ. Prostaglandin Leukot Essent Fatty Acids 73:9–15
Galic S, Oakhill JS, Steinberg GR (2010) Adipose tissue as an endocrine organ. Mol Cell Endocrinol 316:129–139
Gunter MJ, Leitzmann MF (2006) Obesity and colorectal cancer: epidemiology, mechanisms and candidate genes. J Nutr Biochem 17:145–156
O’Rourke RW (2009) Molecular mechanisms of obesity and diabetes: at the intersection of weight regulation, inflammation, and glucose homeostasis. World J Surg 33:2007–2013
Musaad S, Haynes EN (2007) Biomarkers of obesity and subsequent cardiovascular events. Epidemiol Rev 29:98–114
Zulet MA, Puchau B, Navarro C, Martí A, Martínez JA (2007) Inflammatory biomarkers: the link between obesity and associated pathologies. Nutr Hosp 22:511–527
Coppak SW (2001) Pro-inflammatory cytokines and adipose tissue. Proc Nutr Soc 60:349–356
Bassols J, Moreno-Navarrete JM, Ortega F, Ricart W, Fernandez-Real JM (2010) LIGHT is associated with hypertriglyceridemia in obese subjects and increased cytokine secretion from cultured human adipocytes. Int J Obes 34:146–156
Urukawa H, Katsuki A, Sumida Y, Gabazza EC, Murashima S, Morioka K, Maruyama N, Kitagawa N, Tanaka T, Hori Y, Nakatani K, Yano Y, Adachi Y (2003) Oxidative stress is associated with adiposity and insulin resistance in men. J Clin Endocrinol Metab 88:4673–4676
Higdon JV, Frei B (2003) Obesity and oxidative stress: a direct link to CVD? Arterioscler Thromb Vasc Biol 23:365–367
Furukawa S, Fujita T, Shimabukuro M, Iwaki M, Yamada Y, Nakajima Y, Nakayama O, Makishima M, Matsuda M, Shimomura I (2004) Increased oxidative stress in obesity and its impact on metabolic syndrome. J Clin Invest 114:1752–1761
Parra MD, Martínez de Morentin BE, Martínez JA (2005) Postprandial insulin response and mitochondrial oxidation in obese men nutritionally treated to lose weight. Eur J Clin Nutr 59:334–340
Vincent HK, Taylor AG (2006) Biomarkers and potential mechanisms of obesity-induced oxidant stress in humans. Int. J. Obes. (Lond) 30:400–418
Park J, Chung JJ, Kim JB (2007) New evaluations of redox regulating system in adipose tissue of obesity. Diabetes Res Clin Pract 77:11–16
Pagel-Langenickel I, Bao J, Pang L, Sack MN (2010) The role of mitochondria in the pathophysiology of skeletal muscle insulin resistance. Endocr Rev 31:25–51
De Lorenzo A, Del Gobbo V, Premrov MG et al (2007) Normal weight obese syndrome: early inflammation? Am J. Clin. Nutr 85:40–45
Di Renzo L, Galvano F, Orlandi C, Bianchi A, Di Giacomo C, La Fauci L, Acquaviva R, De Lorenzo A (2010) Oxidative stress in normal-weight obese syndrome. Obesity (Silver Spring) 25:1–6
Khan NI, Naz L, Yasmeen G (2006) Obesity: an independent risk factor for systemic oxidative stress. Pak J Pharm Sci 19:62–65
Shlomai J (2010) Redox control of protein–DNA interactions: from molecular mechanisms to significance in signal transduction, gene expression and DNA replication. Antioxid Redox Signal 13(9):1429–1476
Ohshima H, Sawa T, Akaike T (2006) 8-nitroguanine, a product of nitrative DNA damage caused by reactive nitrogen species: formation, occurrence, and implications in inflammation and carcinogenesis. Antioxid Redox Signal 8:1033–1045
Lindahl T (1993) Instability and decay of the primary structure of DNA. Nature 362:709–771
van Loon B, Markkanen E, Hübscher U (2010) Oxygen as a friend and enemy: how to combat the mutational potential of 8-oxo-guanine. DNA Repair 9:604–616
Valavanidis A, Vlachogianni T, Fiotakis C (2009) 8-Hydroxy-2′deoxyguanosine (8-OHdG): a critical biomarker of oxidative stress and carcinogenesis. J. Environ Sci Health Part C 27:120–139
Singh NP, McCoy MT, Tice RR, Schneider EL (1988) A simple technique for quantitation of low levels of DNA damage in individual cells. Exp Cell Res 175:184–191
Tice RR, Agurell E, Anderson D, Burlison B, Hartmann A, Kobayashi H, Miyamae Y, Rojas E, Ryu J-C, Sasaki YF (2000) Single cell gel/comet assay: guidelines for in vitro and an in vivo genetic toxicological testing. Environ Mol Mutagen 35:206–222
Renis M, Calandra L, Scifo C, Tomasello B, Cardile V, Vanella L, Bei R, La Fauci L, Galvano F (2008) Response of cell cycle/stress-related protein expression and DNA damage upon treatment of CaCo2 cells with anthocyanins. Br J Nutr 100:27–35
Zhiping L, Lee JM (2001) Isolation of mature spinal motor neurons and single-cell analysis using the comet assay of early low-level DNA damage induced in vitro and in vivo. J Histochem Cytochem 49:957–972
Gedik CM, Collins A, ESCODD (European Standards Committee on Oxidative DNA Damage) (2005) Establishing the background level of base oxidation in human lymphocyte DNA: results of an interlaboratory validation study. FASEB J 19:82–84
Griffiths HR, Moller L, Bartosz G et al (2002) Biomarkers. Mol Aspects Med 23:101–208
Cheng-Hung C, Miao-Lin Hu (2004) Use of whole blood directly for single cell gel electrophoresis (comet) assay in vivo and white blood cells for in vitro assay. Mutat Res 564:75–82
Collins A,R, Dusinska M, Gedik C,M, Stetina R (1996) Oxidative damage to DNA: do we have a reliable biomarker? Environ Health Perspect 104:465–469
Hill JO, Peters JC, Wyatt HR (2009) Using the energy gap to address obesity: a commentary. J. Am. Diet Assoc 109:1848–1853
Well JCK (2009) Thrift: a guide to thrifty genes, thrifty phenotypes and thrifty norms. Int J Obes 33:1331–1338
Cline MG, Lauten S, Cox S, Bartges JW (2009) The relationship between obesity and markers of oxidative stress in dog. J. Anim. Physiol. Anim. Nutr 93:141–142
Collins AR, Cadet J, Möller L, Poulsen HE, Viña J (2004) Are we sure we know how to measure 8-oxo-7,8-dihydroguanine in DNA from human cells? Arch Biochem Biophys 423:57–65
Bukhari SA, Rajoka MI, Nagra SA, Rehman ZU (2010) Plasma homocysteine and DNA damage profiles in normal and obese subjects in the Pakistani population. Mol Biol Rep 37:289–295
Demirbag R, Yilmaz R, Gur M, Kocyigit A, Celik H, Guzel S, Selek S (2005) Lymphocyte DNA damage in patients with acute coronary syndrome and its relationship with severity of acute coronary syndrome. Mutat Res 570:197–203
Banfi G, Iorio EL, Corsi MM (2008) Oxidative stress, free radicals and bone remodeling. Clin Chem Lab Med 46:1550–1555
Vincent HK, Bourguignon CM, Taylor AG (2010) Relationship of the dietary phytochemical index to weight gain, oxidative stress and inflammation in overweight young adults. J Hum Nutr Diet 23:20–29
Acknowledgments
This study was supported by PRA, Progetti Ateneo, grants of Vanella-Renis 2008.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s12349-010-0048-1
About this article
Cite this article
Tomasello, B., Malfa, G., Galvano, F. et al. DNA damage in normal-weight obese syndrome measured by Comet assay. Mediterr J Nutr Metab 4, 99–104 (2011). https://doi.org/10.1007/s12349-010-0035-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12349-010-0035-6