
Abstract
Essential tremor (ET) is the most common pathological tremor disorder in the world, and post-mortem evidence has shown that the cerebellum is the most consistent area of pathology in ET. In the last few years, advanced neuroimaging has tried to confirm this evidence. The aim of the present review is to discuss to what extent the evidence provided by this field of study may be generalised. We performed a systematic literature search combining the terms ET with the following keywords: MRI, VBM, MRS, DTI, fMRI, PET and SPECT. We summarised and discussed each study and placed the results in the context of existing knowledge regarding the cerebellar involvement in ET. A total of 51 neuroimaging studies met our search criteria, roughly divided into 19 structural and 32 functional studies. Despite clinical and methodological differences, both functional and structural imaging studies showed similar findings but without defining a clear topography of neurodegeneration. Indeed, the vast majority of studies found functional and structural abnormalities in several parts of the anterior and posterior cerebellar lobules, but it remains to be established to what degree these neural changes contribute to clinical symptoms of ET. Currently, advanced neuroimaging has confirmed the involvement of the cerebellum in pathophysiological processes of ET, although a high variability in results persists. For this reason, the translation of this knowledge into daily clinical practice is again partially limited, although new advanced multivariate neuroimaging approaches (machine-learning) are proving interesting changes of perspective.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the last 10 years, advanced neuroimaging has provided strong insight into the pathophysiology of several neurological disorders, while concerning essential tremor (ET) there is still conflicting evidence, despite being one of the most prevalent movement disorders. Indeed, up to 5 % of individuals above the age of 65 years are coping with ET [1]. Part of this variability is dependent upon clinical knowledge about this disorder [2]. Clinical diagnosis has been developed over the years, yet the exact clinical definition of ET is still being debated. For instance, current clinical diagnosis based on the consensus statement of the Movement Disorder Society typically has an estimated error margin of 37 % for false positives [2]. Moreover, ET was, until recently, viewed as a purely motor disorder, but a plethora of epidemiological and neurophysiological studies published in the last 10 years have definitively demonstrated that ET is linked to additional cognitive deficits [3].
For this reason, the first consequence of this clinical variability in the expression of the disease is that the pathophysiology of ET is only partially understood. However, in recent years, as a result of systematic post-mortem examinations, our knowledge of the pathophysiology of this disease has grown substantially. What has been clearly demonstrated [4] is that identifiable structural changes (i.e. Purkinje cell loss, Lewy bodies) have been observed in the brains of ET patients and that these changes are not uniform and seem to follow several patterns, specifically localising into the cerebellum itself. The hypothesis that ET could depend upon cerebellar dysfunctions has initially derived from a series of clinical observations and electrophysiological experiments [5], and then supported by evidences from our group, which demonstrated in vivo, for the first time, the presence of cerebellar neurodegeneration [6].
Overall, in the last 20 years, a number of structural and functional neuroimaging studies have accumulated. Our aim is to review these studies from a neuroimaging perspective, trying to create a topographical cerebellar map of neural changes described in these studies and to determine whether results of imaging studies are congruent with recent post-mortem studies.
Structural Neuroimaging
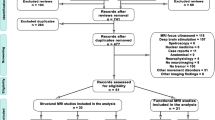
Overall, 19 magnetic resonance imaging (MRI) studies are grouped under the umbrella of structural imaging (MRI) (see Fig. 1; Tables 1 and 2). The most employed neuroimaging morphological metrics were related to changes in (a) volume or (b) diffusivity of water. The voxel-based morphometry (VBM) and the manual/automated volumetry belong to the first category. VBM is a morphological approach that performs a voxel-wise statistical analysis of the brain volume related to the grey matter (GM) and white matter (WM) tissues; however, these are relative measures and not absolute volumes. Alternatively, manual/automatic volumetry are quantitative measurements of the entire volume of distinct brain regions defined a priori (region-of-interest (ROI) analysis). The second group of techniques is mainly characterised by diffusion imaging. Diffusion-weighted imaging (DWI) and the diffusion tensor imaging (DTI; a more recent development of DWI) provide quantitative parameters that reflect microscopic aspects of the tissue damage (demyelination, microtubule breakdown, axonal loss). In tissues such as brain GM, where the measured apparent diffusivity of water is largely independent of the orientation of the tissue (i.e. isotropic), it is usually sufficient to characterise the diffusion characteristics with a single apparent diffusion coefficient (ADC). Otherwise, in anisotropic media, such as WM, where the measured diffusivity is known to depend upon the orientation of the tissue, other metrics are generally employed in order to characterise the orientation-dependent water mobility in these tissues. In particular, fractional anisotropy (FA) is a summary measure of microstructural integrity, highly sensitive to microstructural changes, but less specific to the type of change. Mean diffusivity (MD) is an inverse measure of the membrane density (independent of tissue directionality), very similar for both GM and WM. MD is sensitive to cellularity, edema and necrosis. Radial diffusivity (RD) increases in WM with de- or dys-myelination and changes in the axonal diameters or density may also influence RD. Finally, the axial diffusivity (AD) tends to be variable in WM changes and pathology. In axonal injury AD decreases, while the AD of WM tracts increase with brain maturation.

Spatial location of the structural and functional brain abnormalities in essential tremor (ET) patients relative to healthy controls (HC). Evidence for grey/white matters abnormalities in ET patients relative to controls in voxel-based morphometry (VBM; red circle) and diffusion imaging techniques (DTI; green triangle) studies. Moreover, functional pathological changes as defined by magnetic resonance spectroscopy (MRS; sky blue cross), functional magnetic resonance imaging (fMRI; blue rumble) positron emission tomography or single-photon emission computed tomography (PET-SPECT; yellow, circle). From this topographical analysis were excluded studies using global a priori ROIs (e.g. the entire cerebellum [9]) or those that did not report local maxima of significant difference at a cluster level. The location of neuroimaging results was projected onto Schmahmann’s MRI human atlas [75]
Structural abnormalities of both GM/WM in the cerebellum of ET patients are the most prevalent findings in all structural neuroimaging studies [6–17], although other brain regions have been shown to be implicated in ET in varying degrees (e.g. fronto-temporal cortex) [9–19]. Historically, the first structural MRI study investigating the presence of GM changes in ET did not describe cerebellar abnormalities. In fact, using VBM, Daniels et al. [20] did not find volumetric loss in their ET cohort when compared with age-gender-matched controls even considering uncorrected statistical threshold. In contrast, when ET patients were grouped according to the tremor type (ET patients with intentional and postural tremor in comparison to those having postural tremor alone), only ET patients with both intentional and postural tremor exhibited an unexpected expansion of GM bilaterally in the superior temporal gyrus with respect to controls. Similarly, the first diffusion imaging study in ET [21] found no cerebellar abnormalities in ET patients.
After this preliminary evidence, our group, by using three distinct volumetric approaches (VBM, automated and manual volumetry) described, for the first time, the presence of cerebellar abnormalities in a sample of 50 patients with ET [6, 7]. However, the damage of the cerebellum was only detected in patients with tremor of the hands and head but not in those who presented hand tremor alone. More specifically, we found volumetric abnormalities in the vermis and lobule IV of the cerebellum of ET patients with both hand and head tremor and only a non-significant trend for a global cerebellar volume loss in those patients with hand tremors in isolation. Our findings can be explained by the somatotopic organisation of the cerebellum in which the head and neck are represented in the midline portion of the anterior lobe (mainly vermis and lobule IV–V), whereas the hands and legs are located in the paravermis and the cerebellar hemispheres [22]. This preliminary hypothesis has been subsequently confirmed by a post-mortem study, in which Louis et al. [23] described the presence of axonal torpedoes in the cerebellar vermis of ET patients who presented tremors of the neck, voice and jaw.
Four subsequent VBM studies demonstrated the presence of cerebellar neural loss in ET patients, although more widespread neurodegenerative processes extending to other cortical and subcortical regions were reported [10, 11, 15, 17]. In particular, WM and GM changes have been reported in almost all brain, including the midbrain, the occipital, temporal and parieto-prefrontal regions.
Taken together, these VBM findings (only two of nine studies did not report significant changes [20, 24]) revealing the presence of neurodegenerative processes in the cerebellum of ET patients, can be observed when DTI studies are reviewed. Indeed, a part from the first DTI study published in the 2007, discussed above [21], where authors did not find WM change in the cerebellum, the vast majority of other studies carried out in ET patients found microstructural changes in the cerebellar WM. Shin et al. [9] were the first authors to report reduced FA in ET patients. They studied ten ET patients and found a widespread neuronal WM degeneration in the cerebellum, brainstem and cerebral hemispheres. Three subsequent DTI studies [8, 12, 13] confirmed the involvement of the cerebellum and in particular of the cerebellar peduncles, thalamus and dentate nucleus, although another study [18] also reported GM degeneration within the red nucleus. On the contrary, one recent study (where a very small sample size was investigated) did not find differences in the cerebellum between ET patients and HC [14], although a significant alteration of the superior cerebellar peduncle was detected in ET patients who underwent thalamotomy.
Using a multivariate classification approach, DTI measures were also used to distinguish between patients with different movement disorders such as Parkinson’s disease (PD), atypical Parkinsonism and ET [16]. The authors demonstrated that when DTI measures of the basal ganglia and cerebellum was employed, it was possible to accurately classify patients diagnosed with PD, from those with atypical Parkinsonism, and ET.
In conclusion, the neurodegenerative hypothesis of cerebellar cortex in ET patients has been demonstrated either by in vivo structural imaging studies or by post-mortem study [23]. However, neurodegenerative processes may also be explained by the presence of iron accumulation as already demonstrated in Alzheimer’s disease and Parkinson’s disease. Indeed, using quantitative T2*-relaxometry sequence, which is able to determine brain iron concentration in the brain, our group [25] described, for the first time, abnormal iron concentration in the dentate nucleus of 24 ET patients compared with controls (Table 1).
Magnetic Resonance Spectroscopy
The presence of neural injury and loss in the cerebellum of ET has also been confirmed by magnetic resonance spectroscopy (MRS) studies (Table 2). MRS measures in vivo level of various cellular metabolites such as N-acetylaspartate (NAA), creatine (Cr) or choline (Cho). NAA is known to be a marker of neuronal integrity, and thus a reduction in NAA is suggestive of neuronal damage and/or neuronal dysfunction and/or neuronal loss. To date, only two MRS studies [26, 27] have provided evidence of cerebellar involvement defined by means of NAA reduction (Table 2). Furthermore, Louis et al. [26] showed an inverse association between cerebellar-cortical NAA/Cr ratio and the dominant arm tremor severity. However, these promising findings have not been replicated in a third study [28] where authors focused exclusively on metabolic abnormalities of the thalamus, without providing additional evidence on the cerebellar neurodegenerative model of ET.
Functional Imaging in ET
The neurofunctional correlates of ET may be investigated using blood oxygenation level-dependent (BOLD) or regional cerebral blood flow (rCBF)/glucose metabolism/binding. The vast majority of studies used BOLD sequence during functional magnetic resonance (fMRI) acquisition for evaluating pathophysiological correlates of motor symptoms in ET patients. However, this specific field of study was started with the employment of positron emission tomography (PET) and single-photon emission computed tomography (SPECT), which were, instead, used to evaluate neurofunctional alterations in ET brain useful to enhance diagnostic accuracy. Indeed, PET and SPECT imaging are the most sensitive techniques for an early diagnosis of parkinsonian syndromes due to the employment of ligands that report nigrostriatal dopaminergic function. Post-mortem studies have shown a severe reduction of presynaptic cocaine-binding dopamine receptors associated with dopamine transporter (DaT) in patients with PD [29]. Consequently, DaT selective radiotracers have been developed by using analogues of cocaine, of which iodine 123 (123I)-β CIT (2 β-carbomethoxy-3β-(4-iodophenyl) tropane) and 123I-ioflupane (N-fluoropropyl-ß CIT or FP-CIT) are the most widely used. Therefore, DaT-SPECT imaging enables differentiation of neurodegenerative causes of parkinsonism, where typically patients have abnormal scans, from other movement or tremor disorders where typically the DaT-SPECT study is normal [30]. Otherwise, the 18F-DOPA is a PET tracer for imaging of the substantia nigra, following in vivo the pathway of dopamine. This is a valuable functional technique that provides an indirect measure of nigrostriatal neuron attenuation through evaluation of presynaptic dopa decarboxylase activity and intravesicular dopamine storage. Even if SPECT and PET depict different metabolic pathways, they present similar features in terms of biodistribution in the brain, since both radiopharmaceuticals are evident in the brain only in the structures of basal ganglia. For this reason, the vast majority of this field of study is dedicated to evaluate the presence of altered striatal dopaminergic uptake in ET patients compared with PD and controls. However, the basal ganglia are not often primarily associated with tremor generation in essential tremor [31–34]. Of consequence, the majority of DaT-SPECT and DOPA-PET studies looking into the basal ganglia found no dopaminergic deficits in essential tremor [35–44]. However, some authors reported mild reduction in striatal dopamine transporter binding in ET compared with controls and less severe compared with PD patients [45, 46].
The neuroimaging literature interested to evaluate the pathophysiological mechanisms underlying ET started in 1990 with the employment of rCBF. Overall, the most consistent finding throughout all these kind of studies was the increased cerebellar activity during posture and rest (Table 3). In the first pilot study, Colebatch and collaborators [47] investigated a small sample (n = 4) of ET patients and controls while participants held a specific posture (arms outstretched) that is typically known to trigger the tremor in ET patients. Comparing this postural to a non-postural resting condition, these authors found enhanced blood flow in the sensory-motor and pre-motor cortices controlaterally to the side of the tremor, and in the bilateral cerebellar hemispheres of ET patients relative to controls. These authors concluded that the cerebellar overactivity observed in ET was directly associated with the generation of the postural tremor and that this reflected neurophysiological “oscillations” within the cerebellar-olivary pathways. Evidence provided by this study was further confirmed by Hallett and Dubinsky [48], who suggested the involvement of the inferior olivary nuclei and the thalamus in the generation of ET. Three subsequent PET studies [49–51] confirmed the role of the cerebellum, describing increased bilateral activations in ET patients relative to controls during a simple motor task (e.g. holding a posture). Moreover, comparing brain activations of ET patients to those of patients with a different form of tremor (writing tremor) and controls, it has been found that the overactivity of the cerebellum was also related to the occurrence of both types of tremor in general. Interestingly, an additional PET experiment [52] explored the effects of alcohol, a common substance known to reduce the tremor in ET, on brain responses measured in ET patients and controls. Similar to the previously discussed findings, ET patients showed, relative to controls, increased bilateral cerebellar activation including the vermis before alcohol ingestion. Of note, however, the administration of ethanol led to bilateral decreases of the cerebellar blood flow in both ET patients and controls, and to increased regional cerebral blood flow in the inferior olivary nuclei of ET patients alone (not in controls). Given the intense anatomical connections between the olivary nuclei and the cerebellum, these data suggest that the pharmacological mechanisms of ethanol-induced suppression of tremor in ET are complex and may depend on the functional interactions within specific circuits rather than on the activity of isolated brain regions. More recently, a PET study [53] using a specific GABA-ergic radioligand has provided further insights into the neurobiological mechanisms of ET and has reinvigorated the hypothesis that the GABA system plays a critical role in mediating the functional impairments observed in the motor cortical-cerebellar pathways of ET patients. In particular, a reduced GABA-ergic function was found in the cerebellum, ventrolateral thalamus and lateral pre-motor cortex of ET patients compared to controls. Finally, one study using SPECT to determine rCBF in rest confirmed increased bilateral cerebellar activity [54].
fMRI is a useful and non-invasive tool to reveal the locus of brain abnormalities. The signal changes seen during fMRI studies depend on the BOLD response, which reflect an indirect measurement of neural activity (Table 4). The first fMRI study in ET realm was performed by Bucher et al. [55], who studied unilateral postural tremor in 12 ET patients with ET, mimicked postural tremor in 15 control subjects, and passive wrist oscillation in both groups. During postural tremor, ET patients showed increased activity of the well-known tremor network (cerebello-thalamo-cortical) [31]. Since tremor is the most important clinical characteristic of ET, one recent task-based fMRI study investigated pathophysiological mechanisms of tremor during goal-directed motor task (grip force task that elicits tremor) [56]. Starting from the well-known assumption that patients with ET have increased oscillations in the 0–3- and 3–8-Hz bands during goal-directed motor task, they demonstrated that patients with ET have increased brain activity in the motor cortex and supplementary motor area compared with HC. This activity correlated positively with 3–8 Hz force oscillations, while brain activity in cerebellar lobules I–V was reduced in ET compared with HC and correlated negatively with 0–3 Hz force oscillations. This study provides new evidence that in ET 3–8 Hz force oscillations relate to hyperactivity in the motor cortex, 0–3 Hz force oscillations relate to hypoactivity in the cerebellum and cerebellar-cortical functional connectivity is impaired. These results were consistent with the theory of a central neuronal oscillator involved in tremor genesis [57] rather than a unique structure, such as the cerebellum.
This latter explanation is the main interpretation of two very recent task-based fMRI studies. The first study [24], during continuous writing of “8” with the right dominant hand, showed a higher BOLD response in HC with respect to ET patients in the cerebellum and other brain areas pertaining to the cerebello-thalamo-cortical circuit. Moreover, these authors also studied potential differences related to the presence (ET + R) or absence (ET − R) of resting tremor, showing higher activation of the precentral gyrus bilaterally, right superior and inferior frontal gyri, left postcentral gyrus, superior and inferior parietal gyri, middle temporal and supramarginal gyri, cerebellum and internal globus pallidus in ET-R compared with ET + R patients. These observations confirmed the dysfunction of the cerebello-thalamo-cortical network in patients with ET. The second study by Buijink et al. [58] showed reduced activations in widespread regions of the cerebellum and the parietal and frontal cortices in ET compared with HC during the finger-tapping task. Additionally, reduced activation was observed in the inferior olive nuclei and left dentate nucleus, and a positive correlation between tremor score and activation of both dentate nuclei was found. These authors suggested that dysfunctions of the cerebellar cortex in ET might lead to altered dentate nucleus functioning, subsequently causing functional changes in areas outside the cerebellum.
The two fMRI studies described above are grouped under the term “task-related activity” characterised by the fact that ET patients had to perform motor tasks during scanner sessions. However, brain activity may be also investigated and quantified when the brain is at rest. Indeed resting-state fMRI (RS-fMRI) is a non-invasive technique that is based on the spontaneous fluctuation of the BOLD signal in fMRI. The RS-fMRI observes the brain’s functional change without requiring an overt task performance or stimulation, thus avoiding the inherent shortcomings of the task-designed fMRI [59]. The RS-fMRI, as well as functional connectivity measurements, has been applied to the studies of brain dysfunction in movement disorders and neurodegenerative diseases. Unlike fMRI-task, which only focuses on a single functional system at a time, the RS-fMRI provides brain functional connectivity or functional network information that will be valuable for simultaneously studying the mechanisms of motor and non-motor functional deficits in ET patients. In this field of study (Table 4), Fang et al. [60–62] provided fundamental new advancements in understanding the presence of pathological functional connectivity in brain networks of ET patients. They found that the abnormal functional connectivity was mostly located in the “tremor network” as well as in the non-motor cortices (including prefrontal, parietal and insular lobes), proposing that the disruption of local functional communication in the cerebello-thalamo cortical motor pathway is involved in tremor generation and propagation of ET, while the abnormal functional connectivity in the prefrontal, parietal and insular lobes may take responsibility for the non-motor symptoms (e.g. cognitive, psychiatric and sensory deficits).
The presence of abnormalities in brain networks outside the motor circuit highlights the need to extend functional neuroimaging studies beyond the pathophysiological mechanisms of motor symptoms (e.g. postural tremor) in ET, addressing the neural basis of other non-motor symptoms, such as cognitive impairment. In particular, the notion that ET is a pure motor condition has been challenged by a series of recent neuropsychological and epidemiological studies [3]. This research has revealed a broad spectrum of mild cognitive deficits characterising ET patients, including attention, language and working memory impairments. Furthermore, epidemiological observations have begun to show that ET patients are at a significantly higher risk of developing dementia at an earlier age than would be expected. This demonstrates that the cognitive dysfunctions that lead to dementia in ET could be intrinsically linked to specific disease mechanisms rather than simply reflecting the effect of ageing. This hypothesis has been supported in a series of VBM and DTI studies made by Bhalsing et al. [17, 19] who demonstrated that ET patients with cognitive impairment are characterised by a more widespread neurodegeneration involving mainly the frontal cortex. Our laboratory realised the first fMRI studies, which concentrated on cognitive functioning in ET [63, 64]. We demonstrated that despite similar performances between patients and HC, during a verbal working memory task, ET patients showed increased cerebellar activation compared to controls [64]. In addition, an increased activity in the parieto-prefrontal network [63] was obtained using the Stroop task in cognitively preserved ET patients suggesting that despite an intact cognitive profile, patients require additional neural demands to reach similar performance of HC.
Discussion
Figure 1 shows topographical maps of neural abnormalities detected in ET using either structural or functional imaging data. What immediately captures our attention is the diffuse presence of alterations in the cerebellar regions thus making uncertain the delineation of cerebellar-related ET neurodegenerative processes. Indeed, diffuse neural changes have been described in several cerebellar regions, including motor (from lobule I–V) and cognitive lobules (from lobule VI–IX, including crus I–II) but a precise investigation of the eventual relationship between specific areas of the cerebellum and the clinical phenotypes is still lacking. It remains to be determined in which degree cerebellar abnormalities of the motor lobules are mainly responsible of the classic motor features of ET patients and how different cognitive deficits are associated with the disintegrity of the cognitive posterior cerebellar lobules.
The Neural Basis of Motor Dysfunctions
Considering genesis of motor dysfunctions in ET, functional MRI studies have consistently demonstrated that dysfunctions within cortical-cerebellar pathways are primarily involved in the pathogenesis of the motor dysfunctions in ET and have begun to provide a clearer picture of the possible underlying mechanisms (e.g. GABA-ergic dysfunctions). Moreover, with respect to structural studies, functional imaging studies showed more consistent relationship between abnormalities in the activity of the cerebellar cortex and clinical scales (i.e. tremor severity) [26, 56, 58, 60–62].
However, an unresolved question is whether in EP patients the tremor originates in the cerebellum and is subsequently mediated by other structures within the “tremor network” or whether a concerted disruption in connectivity between several brain structures causes ET-related symptoms [33]. Given the ambiguous picture emerging from this review, we can suggest that neuroimaging studies support the hypothesis that the tremor origin in a neural loop where the cerebellum is a critical hub. Of note, Novellino et al. [25] found pathological brain accumulation in the dentate nucleus, whereas Nicoletti et al. [8] described microstructural changes of the superior cerebellar peduncle fibre tracts, which receive input from the dentate nucleus and send output to the red nucleus, thus suggesting that the dentatorubro-olivary tract may be involved in the genesis of tremor. Other studies, instead, described microstructural abnormalities in the inferior cerebellar peduncle [12] or in other cortical-cerebellar tracts [9, 13]. Similarly, some functional studies confirmed the presence of neural changes in specific brain regions involved in the well-known “tremor network” [31] such as the dentate nucleus, inferior olive nuclei and red nucleus [49–52, 55, 58]. In summary, structural and functional neuroimaging studies demonstrated that widespread disintegrity of cortical-cerebellar tracts is common and likely underlies tremor generation [33].
The Neural Basis of Cognitive Dysfunctions
The pathophysiology of cognitive deficits in ET remains largely unclear and underexplored. Until now, only three fMRI [62–64] and two structural neuroimaging studies [17, 19] explicitly investigated this fundamental topic. Different theories have been formulated to explain non-motor deficits in ET, including the hypothesis that cognitive abnormalities may depend upon mechanisms similar to those reported in AD or PD. Alternatively, it has been proposed that the cognitive impairment in ET may be driven by the cerebellum, similarly to that previously hypothesised for the tremor [65, 66]. Overall, there is consistent evidence from research in patients with focal lesions (strokes or tumours) and from functional neuroimaging in healthy subjects that specific regions of the cerebellum (posterior lobules) are critically involved in a variety of high-level cognitive functions such as working memory and attention [67]. We have therefore recently tested the hypothesis that the deficits in the working memory in ET may depend on abnormalities of cognitive cortical-cerebellar loops [63, 64]. Indeed, we have revealed greater cerebellar response in the crus I and lobule VI of ET patients while they executed a working memory task with high attention demand [64]. These cerebellar overactivations were interpreted as compensatory responses because the behavioural performances of ET patients were comparable with those of sex-, age- and education-matched controls. They also displayed altered functional connectivity between crus I/lobule VI and regions implicated in focusing attention (executive control circuit including dorsolateral prefrontal cortex, inferior parietal lobule, thalamus). These findings were modulated by the variability in neuropsychological measures: patients with low cognitive scores displayed reduced connectivity between crus I/lobule VI and the dorsolateral prefrontal cortex. Crus I/lobule VI are parts of the posterior lobule of the cerebellum that have been implicated in a wide range of cognitive functions, including language, visuospatial skills and working memory [68]. The main current hypothesis regarding the function of crus I/lobule VI was that this region would support a specific component of working memory that is called the “articulatory loop”. This cognitive process is used to “mentally” refresh the content of working memory throughout a sub-vocal rehearsal that prevents the decaying of memory traces. Enhanced cerebellar responses in ET patients would therefore reflect an increased effort to rehearse the stimuli that need to be kept in memory.
Apart from our fMRI studies, only three further neuroimaging papers directly investigated the impact of cognitive profile in ET patients. Bhalsing et al. [17, 19] used VBM and DTI to evaluate the neural basis of cognitive deficits in ET patients. First of all, Bhalsing et al. [17], evaluating cognitively impaired ET patients, reported reduced GM volumes in the anterior and posterior cerebellar lobules; however, using DTI, Bhalsing et al. [17] did not confirm the presence of anatomical changes in the cerebellar WM [18]. When neuropsychological deficits were correlated with GM and WM measurements of integrity, these authors found that working memory scores correlated with increased GM volume and negatively with mean diffusivity of the posterior cerebellar cortex. Finally, Fang et al. [62], using RS-functional connectivity demonstrated the presence of abnormal changes within the cerebellum network and between the cerebellum network and the anterior and posterior default mode networks. All these changes were correlated with cognitive behaviour. With this in mind, the authors proposed that the posterior default mode network is a key hub for balancing the cerebellum network and default mode network responsible for cognitive modulation in ET patients.
In summary, although the neurocognitive profile of ET has received lesser attention than the neural basis of motor symptoms, these preliminary findings would seem to suggest that cognitive impairment in ET is not primary driven by the cerebellum deficits but by a concerted disruption in connectivity between several brain structures that might cause ET-related cognitive symptoms, similarly to that proposed for motor symptoms.
Limitations
As widely reported in other recent reviews [31–34], the inconsistencies amongst neuroimaging findings might be dependent upon several methodological limitations that need to be summarised:
-
1.
Sample size: one main limitation of this field of study is the small sample size employed in several studies. In particular, all PET studies [47–53] as well as some structural studies [14, 15], enrolled groups of less than ten individuals, thus drastically impacting the possibility of making general inferences.
-
2.
Age: the mean age of ET patients investigated in almost all studies ranged from 53 to 70 years, whereas others reported younger cases (e.g. 38 [11], 40.7 [13] and 45 years [17, 19].
-
3.
Gender: although the majority of the studies reported a balanced gender distribution, three studies employed a cohort that was mostly comprised of females (e.g. 8F/10M, [21]; 8F/6M, [16]; 8F/6M [31]). This is not in line with those reported in several epidemiological studies [1], which demonstrated that ET has a higher prevalence amongst men.
-
4.
Disease duration: a wide variability in the disease duration is also noted amongst studies, with some reporting up to 10 years of disease duration (e.g. [9, 13, 17, 18, 24, 60]) and others with up to 20 years of clinical history (e.g. [6–8, 16, 53]).
-
5.
Whole brain vs. ROI analysis: another discrepancy in the structural neuroimaging literature of ET patients could be ascribed to methodological differences. For instance, some studies employed a voxel-based approach that investigated the morphological differences in the whole brain, while others used a priori ROIs (e.g. [8, 12, 13, 16, 18, 21]). Generally, voxel-based and manual/automatic ROIs volumetric studies are often not directly comparable and several contradictory findings have been reported [69, 70]. Voxel-based approaches could be generally influenced by several methodological issues, such as degree of smoothing, differences in registration and choice of normalisation template [70]. On the other hand, manual/automatic ROI volumetry is a quantitative research tool that captures a real physical quantity that could not reach the specificity of small changes (voxel-level).
-
6.
Cognitive impairment: The vast majority of neuroimaging studies, investigating the neural basis of motor symptoms, have not taken into account the influence of cognitive impairments as confounding factor [71]. For this reason, it is possible to hypothesise that some of the findings (e.g. the atrophy of the frontal and temporal cortices as described by Shin et al. [9], Benito-Leon et al. [10], Bagepally et al. [11] and Klein et al. [12]) may depend upon neurodegenerative processes associated with cognitive deficits per se rather than motor symptoms.
-
7.
Motion artefacts: It is important to highlight that MRI-based methods have intrinsic limitations when applied to patients with ET, namely the contamination of imaging data due to motion artefacts. Moreover, the tremor by itself could introduce confounding factors (i.e. uncontrolled body motion) during task-designed fMRI experiment influencing imaging quality and motor or cognitive performance itself.
-
8.
Clinical phenotypes: Last but not least, some inconsistencies reported in the neuroimaging literature might be dependent upon the different ET-related clinical phenotypes enrolled in these studies: (a) ET patients with or without resting tremor [24], (b) ET patients with dystonia [72], (c) ET patients with or without head tremor [8, 9], (d) ET patients with postural tremor or postural and intentional tremor [20] and, finally, (6) patients with or without a family history of ET; all these ET-related clinical expressions may influence image analysis and interpretation.
Conclusions and Future Remarks
In this review, we provide support to the hypothesis that the cerebellum is a key region involved in the pathogenesis of motor and non-motor symptoms associated with ET, although its exact role in ET-related pathophysiological mechanisms remains to be ascertained. In fact, it still remains to be determined whether the cerebellum is globally abnormal in ET and whether it is possible to define a topographical distribution inside the cerebellum of ET-related motor and cognitive symptoms.
For this reason, the first remark for the future is that neuroimaging studies applied on ET have to adopt more clinically and methodologically stringent criteria in order to reduce the intrinsic variability of this neurological disorder. This new era of studies will greatly advance the refinement of the current taxonomy of ET and will reveal whether this disorder is constituted by a continuum of associated disturbances or whether it is more appropriate to define ET as a heterogeneous disorder constituted by separate clinical entities. Indeed, the aim of advanced neuroimaging applied in clinical realms is to lower the margin of error in diagnosing ET by gaining insight into underlying brain pathology. Presently, neuroimaging of ET has a lower potential translation in daily clinical practice.
With this in mind, we conclude our review presenting a new revolutionary advanced neuroimaging approach based on machine learning. Historically, neuroimaging has been applied in clinical realms using a classical univariate approach that allows only to find differences between patients and controls at a group level, thus with a very limited translation to an individual diagnosis in a clinical setting. For this reason, a considerable effort has been put into the development of alternative approaches to the analyses of neuroimaging data. Indeed, in the last 5 years, there here has been a growing interest within the neuroimaging community toward alternative approaches to the analyses of neuroimaging data by considering multivariate pattern analysis, including machine-learning algorithms [73]. Due to their multivariate properties, machine-learning techniques are able to automatically extract multiple sources of information from functional or structural image sets without requiring a priori hypotheses of where this information may be coded in the images. The aim of this method is to classify individual structural or functional brain images by maximising the distance between groups of images. Several studies have assessed the reliability of these techniques, e.g. for the automated diagnosis of the Alzheimer’s disease with respect to mild cognitive impairment patients [50] demonstrating their high translational potential into clinical practice.
Recently, our group has applied this approach on ET patients for the first time [74]. Combining anatomical information, voxel-by-voxel, coming from volumetric and DTI data, an automated computer-based classification algorithm was able to distinguish patients who had tremor-dominant PD from those who had ET associated with rest tremor, with an accuracy of 100 %. Although further validation are needed, this study provided preliminary evidence demonstrating that this advanced neuroimaging approach might be used for the differentiation, at the individual level, of patients who have clinically indistinguishable phenotypes, thus representing a valid tool in everyday clinical diagnoses.
References
Louis ED, Ferreira JJ. How common is the most common adult movement disorder? Update on the worldwide prevalence of essential tremor. Mov Disord. 2010;25:534–41.
Jain S, Se L, Louis ED. Common misdiagnosis of a common neurological disorder: how are we misdiagnosing essential tremor? Arch Neurol. 2006;63:1100–4.
Bermejo-Pareja F, Puertas-Martín V. Cognitive features of essential tremor: a review of the clinical aspects and possible mechanistic underpinnings. Tremor Other Hyperkinet Mov (NY) 2012;2. pii: 02-74-541-1.
Louis ED. Essential tremor: evolving clinicopathological concepts in an era of intensive post-mortem enquiry. Lancet Neurol. 2010;9(6):613–22.
Deuschl G, Elble R. Essential tremor—neurodegenerative or nondegenerative disease towards a working definition of ET. Mov Disord. 2009;24(14):2033–41.
Quattrone A, Cerasa A, Messina D, Nicoletti G, Hagberg GE, Lemieux L, et al. Essential head tremor is associated with cerebellar vermis atrophy: a volumetric and voxel-based morphometry MR imaging study. AJNR Am J Neuroradiol. 2008;29(9):1692–7.
Cerasa A, Messina D, Nicoletti G, Novellino F, Lanza P, Condino F, et al. Cerebellar atrophy in essential tremor using an automated segmentation method. AJNR Am J Neuroradiol. 2009;30(6):1240–3.
Nicoletti G, Manners D, Novellino F, Condino F, Malucelli E, Barbiroli B, et al. Diffusion tensor MRI changes in cerebellar structures of patients with familial essential tremor. Neurology. 2010;74(12):988–94.
Shin DH, Han BS, Kim HS, Lee PH. Diffusion tensor imaging in patients with essential tremor. AJNR Am J Neuroradiol. 2008;29(1):151–3.
Benito-León J, Alvarez-Linera J, Hernández-Tamames JA, Alonso-Navarro H, Jiménez-Jiménez FJ, Louis ED. Brain structural changes in essential tremor: voxel-based morphometry at 3-Tesla. J Neurol Sci. 2009;287(1–2):138–42.
Bagepally BS, Bhatt MD, Chandran V, Saini J, Bharath RD, Vasudev M, et al. Decrease in cerebral and cerebellar gray matter in essential tremor: a voxel-based morphometric analysis under 3T MRI. J Neuroimaging. 2012;22(3):275–8.
Klein JC, Lorenz B, Kang JS, Baudrexel S, Seifried C, van de Loo S, et al. Diffusion tensor imaging of white matter involvement in essential tremor. Hum Brain Mapp. 2011;32(6):896–904.
Saini J, Bagepally BS, Bhatt MD, Chandran V, Bharath RD, Prasad C, et al. Diffusion tensor imaging: tract based spatial statistics study in essential tremor. Parkinsonism Relat Disord. 2012;18(5):477–82.
Buijink AW, Caan MW, Tijssen MA, Hoogduin JM, Maurits NM, van Rootselaar AF. Decreased cerebellar fiber density in cortical myoclonic tremor but not in essential tremor. Cerebellum. 2013;12(2):199–204.
Lin CH, Chen CM, Lu MK, Tsai CH, Chiou JC, Liao JR, et al. VBM reveals brain volume differences between Parkinson’s disease and essential tremor patients. Front Hum Neurosci. 2013;14:7–247.
Prodoehl J, Li H, Planetta PJ, Goetz CG, Shannon KM, Tangonan R, et al. Diffusion tensor imaging of Parkinson’s disease, atypical parkinsonism, and essential tremor. Mov Disord. 2013;28(13):1816–22.
Bhalsing KS, Upadhyay N, Kumar KJ, Saini J, Yadav R, Gupta AK, et al. Association between cortical volume loss and cognitive impairments in essential tremor. Eur J Neurol. 2014;21(6):874–83.
Jia L, Jia-Lin S, Qin D, Qing L, Yan Z. A diffusion tensor imaging study in essential tremor. J Neuroimaging. 2011;21(4):370–4.
Bhalsing KS, Kumar KJ, Saini J, Yadav R, Gupta AK, Pal PK. White matter correlates of cognitive impairment in essential tremor. AJNR Am J Neuroradiol. 2015;36(3):448–5.
Daniels C, Peller M, Wolff S, Alfke K, Witt K, Gaser C, et al. Voxel-based morphometry shows no decreases in cerebellar gray matter volume in essential tremor. Neurology. 2006;67(8):1452–6.
Martinelli P, Rizzo G, Manners D, Tonon C, Pizza F, Testa C, et al. Diffusion-weighted imaging study of patients with essential tremor. Mov Disord. 2007;22(8):1182–5.
Manni E, Petrosini L. A century of cerebellar somatotopy: a debated representation. Nat Rev Neurosci. 2004;5:241–9.
Louis ED, Faust PL, Ma KJ, Yu M, Cortes E, Vonsattel JP. Torpedoes in the cerebellar vermis in essential tremor cases vs. controls. Cerebellum. 2011;10:812–9.
Nicoletti V, Cecchi P, Frosini D, Pesaresi I, Fabbri S, Diciotti S, et al. Morphometric and functional MRI changes in essential tremor with and without resting tremor. J Neurol. 2015;262(3):719–28.
Novellino F, Cherubini A, Chiriaco C, Morelli M, Salsone M, Arabia G, et al. Brain iron deposition in essential tremor: a quantitative 3-Tesla magnetic resonance imaging study. Mov Disord. 2013;28(2):196–200.
Louis ED, Shungu DC, Chan S, Mao X, Jurewicz EC, Watner D. Metabolic abnormality in the cerebellum in patients with essential tremor: a proton magnetic resonance spectroscopic imaging study. Neurosci Lett. 2002;333(1):17–20.
Pagan FL, Butman JA, Dambrosia JM, Hallett M. Evaluation of essential tremor with multi-voxel magnetic resonance spectroscopy. Neurology. 2003;60(8):1344–7.
Kendi AT, Tan FU, Kendi M, Erdal HH, Tellioglu S. Magnetic resonance spectroscopy of the thalamus in essential tremor patients. J Neuroimaging. 2005;15(4):362–6.
Kaufman MJ, Madras BK. Severe depletion of cocaine recognition sites associated with the dopamine transporter in Parkinson’s diseased striatum. Synapse. 1991;9:43–9.
Booth TC, Nathan M, Waldman AD, Quigley AM, Schapira AH, Buscombe J. The role of functional dopamine-transporter SPECT imaging in parkinsonian syndromes, part 1. AJNR Am J Neuroradiol. 2015;36(2):229–35.
Hallett M. Tremor: pathophysiology. Parkinsonism Relat Disord. 2014;20 Suppl 1:S118–22.
Sharifi S, Nederveen AJ, Booij J, van Rootselaar AF. Neuroimaging essentials in essential tremor: a systematic review. Neuroimage Clin. 2014;5:217–31.
Klaming R, Annese J. Functional anatomy of essential tremor: lessons from neuroimaging. AJNR Am J Neuroradiol. 2014;35(8):1450–7.
Bhalsing KS, Saini J, Pal PK. Understanding the pathophysiology of essential tremor through advanced neuroimaging: a review. J Neurol Sci. 2013;335(1–2):9–13.
Breit S, Reimold M, Reischl G, Klockgether T, Wüllner U. [(11)C]d-threo-methylphenidate PET in patients with Parkinson’s disease and essential tremor. J Neural Transm. 2006;113(2):187–93.
Brooks DJ, Playford ED, Ibanez V, Sawle GV, Thompson PD, Findley LJ, et al. Isolated tremor and disruption of the nigrostriatal dopaminergic system: an 18F-dopa PET study. Neurology. 1992;42(8):1554–60.
Antonini A, Moresco RM, Gobbo C, De Notaris R, Panzacchi A, Barone P, et al. The status of dopamine nerve terminals in Parkinson’s disease and essential tremor: a PET study with the tracer [11-C]FE-CIT. Neurol Sci. 2001;22(1):47–8.
Doepp F, Plotkin M, Siegel L, Kivi A, Gruber D, Lobsien E, et al. Brain parenchyma sonography and 123I-FP-CIT SPECT in Parkinson’s disease and essential tremor. Mov Disord. 2008;23(3):405–10.
Wang J, Jiang YP, Liu XD, Chen ZP, Yang LQ, Liu CJ, et al. 99mTc-TRODAT-1 SPECT study in early Parkinson’s disease and essential tremor. Acta Neurol Scand. 2005;112(6):380–5.
Asenbaum S, Pirker W, Angelberger P, Bencsits G, Pruckmayer M, Brücke T. [123I]beta-CIT and SPECT in essential tremor and Parkinson’s disease. J Neural Transm. 1998;105(10–12):1213–28.
Benamer TS, Patterson J, Grosset DG, Booij J, de Bruin K, van Royen E, et al. Accurate differentiation of parkinsonism and essential tremor using visual assessment of [123I]-FP-CIT SPECT imaging: the [123I]-FP-CIT study group. Mov Disord. 2000;15(3):503–10.
Di Giuda D, Camardese G, Bentivoglio AR, Cocciolillo F, Guidubaldi A, Pucci L, et al. Dopaminergic dysfunction and psychiatric symptoms in movement disorders: a 123I-FP-CIT SPECT study. Eur J Nucl Med Mol Imaging. 2012;39(12):1937–48.
Isaias IU, Marotta G, Hirano S, Canesi M, Benti R, Righini A, et al. Imaging essential tremor. Mov Disord. 2010;25(6):679–86.
Roselli F, Pisciotta NM, Pennelli M, Aniello MS, Gigante A, De Caro MF, et al. Midbrain SERT in degenerative parkinsonisms: a 123I-FP-CIT SPECT study. Mov Disord. 2010;25(12):1853–9.
Gerasimou G, Costa DC, Papanastasiou E, Bostanjiopoulou S, Arnaoutoglou M, Moralidis E, et al. SPECT study with I-123-Ioflupane (DaTSCAN) in patients with essential tremor. Is there any correlation with Parkinson’s disease? Ann Nucl Med. 2012;26(4):337–44.
Isaias IU, Canesi M, Benti R, Gerundini P, Cilia R, Pezzoli G, et al. Striatal dopamine transporter abnormalities in patients with essential tremor. Nucl Med Commun. 2008;29(4):349–53.
Colebatch JG, Findley LJ, Frackowiak RS, Marsden CD, Brooks DJ. Preliminary report: activation of the cerebellum in essential tremor. Lancet. 1990;336(8722):1028–30.
Hallett M, Dubinsky RM. Glucose metabolism in the brain of patients with essential tremor. J Neurol Sci. 1993;114(1):45–8.
Wills AJ, Jenkins IH, Thompson PD, Findley LJ, Brooks DJ. Red nuclear and cerebellar but no olivary activation associated with essential tremor: a positron emission tomographic study. Ann Neurol. 1994;36:636–42.
Jenkins IH, Bain PG, Colebatch JG, Thompson PD, Findley LJ, Frackowiak RS, et al. A positron emission tomography study of essential tremor: evidence for overactivity of cerebellar connections. Ann Neurol. 1993;34:82–90.
Wills AJ, Jenkins IH, Thompson PD, Findley LJ, Brooks DJ. A positron emission tomography study of cerebral activation associated with essential and writing tremor. Arch Neurol. 1995;52:299–305.
Boecker H, Wills AJ, Ceballos-Baumann A, Samuel M, Thompson PD, Findley LJ, et al. The effect of ethanol on alcohol-responsive essential tremor: a positron emission tomography study. Ann Neurol. 1996;39:650–8.
Boecker H, Weindl A, Brooks DJ, Ceballos-Baumann AO, Liedtke C, Miederer M, et al. GABAergic dysfunction in essential tremor: an 11C-flumazenil PET study. J Nucl Med. 2010;51:1030–5.
Czarnecki K, Jones DT, Burnett MS, Mullan B, Matsumoto JY. SPECT perfusion patterns distinguish psychogenic from essential tremor. Parkinsonism Relat Disord. 2011;17(5):328–32.
Bucher SF, Seelos KC, Dodel RC, Reiser M, Oertel WH. Activation mapping in essential tremor with functional magnetic resonance imaging. Ann Neurol. 1997;41:32–40.
Neely KA, Kurani AS, Shukla P, Planetta PJ, Wagle Shukla A, Goldman JG, et al. Functional brain activity relates to 0–3 and 3–8 Hz force oscillations in essential tremor. Cereb Cortex. 2015;25(11):4191–202.
Raethjen J, Deuschl G. The oscillating central network of essential tremor. Clin Neurophysiol. 2012;123:61–4.
Buijink AW, Broersma M, van der Stouwe AM, van Wingen GA, Groot PF, Speelman JD, et al. Rhythmic finger tapping reveals cerebellar dysfunction in essential tremor. Parkinsonism Relat Disord. 2015;21(4):383–8.
Deco G, Jirsa VK, McIntosh AR. Emerging concepts for the dynamical organization of resting-state activity in the brain. Nat Rev Neurosci. 2011;12(1):43–56.
Fang W, Lv F, Luo T, Cheng O, Liao W, Sheng K, et al. Abnormal regional homogeneity in patients with essential tremor revealed by resting-state functional MRI. PLoS One. 2013;8(7):e69199.
Fang W, Chen H, Wang H, Zhang H, Puneet M, Liu M, et al. Essential tremor is associated with disruption of functional connectivity in the ventral intermediate nucleus-motor cortex-cerebellum circuit. Hum Brain Mapp. 2015. doi:10.1002/hbm.23024.
Fang W, Chen H, Wang H, Zhang H, Liu M, Puneet M, et al. Multiple resting-state networks are associated with tremors and cognitive features in essential tremor. Mov Disord. 2015. doi:10.1002/mds.26375.
Cerasa A, Passamonti L, Novellino F, Salsone M, Gioia MC, Morelli M, et al. Fronto-parietal overactivation in patients with essential tremor during Stroop task. Neuroreport. 2010;21:148–51.
Passamonti L, Novellino F, Cerasa A, Chiriaco C, Rocca F, Matina MS, et al. Altered cortical-cerebellar circuits during verbal working memory in essential tremor. Brain. 2011;134:2274–86.
Janicki SC, Cosentino S, Louis ED. The cognitive side of essential tremor: what are the therapeutic implications? Ther Adv Neurol Disord. 2013;6(6):353–68.
Passamonti L, Cerasa A, Quattrone A. Neuroimaging of essential tremor: what is the evidence for cerebellar involvement? Tremor Other Hyperkinet Mov (N Y). 2012;2. pii: 02-67-421-3.
Tedesco AM, Chiricozzi FR, Clausi S, Lupo M, Molinari M, Leggio MG. The cerebellar cognitive profile. Brain. 2011;134(Pt 12):3672–86.
Stoodley CJ, Schmahmann JD. Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuroimage. 2009;44:489–501.
Cerasa A, Quattrone A, Gioia MC, Magariello A, Muglia M, Assogna F, et al. MAO A VNTR polymorphism and amygdala volume in healthy subjects. Psychiatry Res. 2011;191(2):87–9.
Eckert MA, Tenforde A, Galaburda AM, et al. To modulate or not to modulate: differing results in uniquely shaped Williams syndrome brains. Neuroimage. 2006;32:1001–7.
Thawani SP, Schupf N, Louis ED. Essential tremor is associated with dementia: prospective population-based study in New York. Neurology. 2009;73:621–5.
Cerasa A, Nisticò R, Salsone M, Bono F, Salvino D, Morelli M, et al. Neuroanatomical correlates of dystonic tremor: a cross-sectional study. Parkinsonism Relat Disord. 2014;20(3):314–7.
Orrù G, Pettersson-Yeo W, Marquand AF, Sartori G, Mechelli A. Using support vector machine to identify imaging biomarkers of neurological and psychiatric disease: a critical review. Neurosci Biobehav Rev. 2012;36(4):1140–5.
Cherubini A, Nisticó R, Novellino F, Salsone M, Nigro S, Donzuso G, et al. Magnetic resonance support vector machine discriminates essential tremor with rest tremor from tremor-dominant Parkinson disease. Mov Disord. 2014;29(9):1216–9.
Schmahmann JD, Doyon J, Toga A, Petrides M, Evans A. MRI Atlas of the Human Cerebellum. San Diego: Academic; 2000.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
None of the authors has any conflict of interest to disclose.
Rights and permissions
About this article

Cite this article
Cerasa, A., Quattrone, A. Linking Essential Tremor to the Cerebellum—Neuroimaging Evidence. Cerebellum 15, 263–275 (2016). https://doi.org/10.1007/s12311-015-0739-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12311-015-0739-8